
Abstract
Background
Preventing Loss of Independence through Exercise (PLIÉ) is an in-person group mind-body movement program for people across the spectrum of cognitive decline and care partners (CPs).
Objective
This study developed and refined an online version called Moving Together and tested feasibility and satisfaction with an online delivery.
Methods
In Phase 1, we used qualitative methods to determine which elements of the in-person program were essential to retain for the online version and adaptations that would be needed to support the user experience. In Phase 2, we created a prototype of the online program and iteratively refined it based on user feedback. In Phase 3, we assessed feasibility of online delivery based on class attendance and program completion; we assessed satisfaction and participant-reported outcomes using a post-program evaluation survey with quantitative and qualitative components.
Results
Phase 1 findings from 27 participants (14 PLWD, 13 CPs) revealed three key considerations related to online delivery of PLIÉ: technology use, social connection as a primary motivator, and physical safety concerns. Phase 2 iterative testing among 25 participants (14 PLWD, 11 CPs) resulted in key refinements to program delivery and instructional elements; Phase 3 pilot testing included 39 participants (12 PLWD, 15 CPs, 12 MCI) who attended 75 ± 29% of 24 classes; 77% completed the 12-week program, of whom 96% rated it as excellent or good. Participant-reported outcomes included improvements in social connection, emotional well-being, physical function, cognitive function and present-centered body awareness. PLWD or MCI also reported improvements in self-concept, and CPs reported improvements in caregiving self-efficacy. The primary challenges were related to participant navigation of technology.
Conclusion
The Moving Together online program is feasible for PLWD or MCI and CPs with participants reporting high satisfaction and positive outcomes across multiple domains. Providing individual technology support is critical for the success of livestreamed, online interventions for dementia.
Keywords
Background
The number of individuals affected by cognitive impairment is large and growing. Approximately 12% of people aged 65 years or older report subjective cognitive decline (SCD), and 20% are living with mild cognitive impairment (MCI).1,2 Both SCD and MCI are associated with an increased risk of developing Alzheimer’s disease or related dementias (ADRD), which currently affects 6.5 million people in the U.S. (∼12% of older adults) and 50 million people worldwide.3,4 In addition, more than 16 million family caregivers provide unpaid care for people living with dementia (PLWD) and about half of people living in the community with advanced dementia receive paid care.3,5
Although current pharmacological treatments for dementia are associated with small symptomatic relief for some patients, these therapies ultimately lack neuroprotective effects, do not alter the disease course, and do not improve quality of life.6-8 In contrast, systematic reviews and meta-analyses of randomized controlled trials have shown that non-pharmacologic and behavioral interventions improve a wide range of outcomes in PLWD or MCI.9-12 In addition, multidomain interventions have been found to improve multiple outcomes and enhance quality of life (QOL) among individuals living with dementia. 13
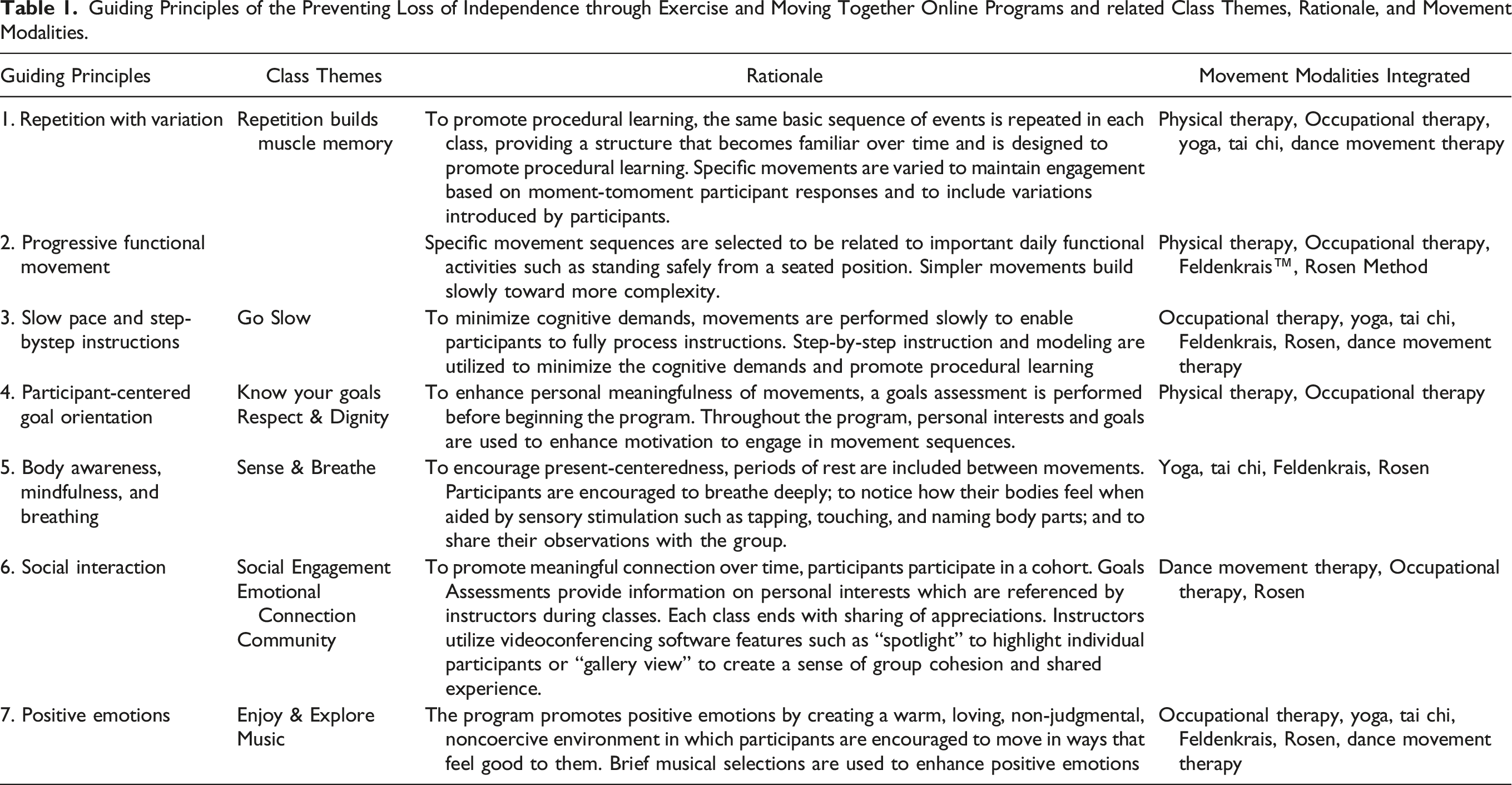
Guiding Principles of the Preventing Loss of Independence through Exercise and Moving Together Online Programs and related Class Themes, Rationale, and Movement Modalities.
Our studies have found that PLIÉ participants with MCI or mild to moderate dementia experience physical, psychological, social and cognitive benefits.15-17 We also created Paired PLIÉ, which was adapted for in-person groups of people with MCI or dementia and care partners (paid or unpaid) participating together as dyads and incorporated movements performed together as dyads. PLIÉ participants reported similar improvements in physical, psychological, social, and cognitive domains, as well as benefits for care partners.18,19 Despite the benefits reported with our in-person programs, participants also described a variety of barriers and challenges, such as difficulty with transportation and securing a suitable space for in-person classes. 19
Objective
To address logistical barriers and participant burden with traveling to the in-person PLIÉ program, the goals of this study were to develop and refine an online version called Moving Together and test its feasibility and acceptability among people across the spectrum of cognitive decline, including those with and without care partners.
Methods
Overview of Study Design
This study was performed in three phases (Figure 1). In Phase 1, we determined which elements of the in-person PLIÉ program were essential to retain for the online version and adaptations that would be needed to support the user experience. In Phase 2, we created a prototype of the online program and iteratively refined it based on user feedback. In Phase 3, we assessed feasibility, satisfaction and participant-reported outcomes associated with online delivery of Moving Together. This study was approved by the Institutional Review Board (IRB) at the University of California, San Francisco. The IRB included a waiver of informed consent for analysis of data collected for Moving Together ongoing quality improvement processes. Study design and phases.
Phase 1. Development of Moving Together Online program
Goal
The goal of Phase 1 was to determine which elements of the in-person program were most important to retain and identify adaptations needed for the online version.
Participants
We invited all individuals who had completed our previous research studies of in-person PLIÉ programs15,16,19 and agreed to be contacted for future research to participate in 90-minute, in-home interviews about their experiences with use of electronic devices and with PLIÉ. Details of eligibility criteria and cognitive screeners used in prior studies are included in Supplemental File 1). Class instructors were invited to participate in separate interviews about their experiences with technology and teaching the PLIÉ classes. All participants were age 18 years or older and fluent in English.
Data Collection
We performed semi-structured interviews and used human-centered design (HCD) to inform development of the Moving Together class format and online user interface. HCD, involving potential end-users in all phases of design and testing, is increasingly recommended for developing health-related technology that will be effective for older adults.20-22 HCD can maximize usability, satisfaction and outcomes using a flexible, user-centric, iterative approach. Semi-structured interviews and observations focused on participants’ use of technology and electronic devices in their home (e.g., computer, smart phone), experiences with the in-person PLIÉ programs, and feedback on the proposed online intervention. Using HCD best-practices, we video-recorded interviews and observations, with one interviewer leading discussion and a second taking detailed notes. Interviewers debriefed after each session to discuss observations and wrote an interview summary. Exygy, a digital design and technology firm, assisted with the HCD process and conducted semi-structured interviews with 4 PLIÉ instructors to learn their perspectives on key considerations for adapting the in-person program to an online setting.
Data Analysis
Data gathered from interviews and observations were analyzed using a ‘sticky note’ process to facilitate data organization, content analysis, and synthesis. 23 First, all team members who had participated in one or more interview (author initials) were provided with a sticky note pad and asked to write down their takeaways or key observations. The team then worked collaboratively to group the sticky notes into domains by participant type (i.e., person living with cognitive impairment, care partner, instructor), which were then distilled into key insights. Key insights were used to create a User Profile that illustrated the goals, concerns, motivations and needs of a typical participant, which served as a guide as we designed the user flow and process for the online program. In addition, we created a detailed Journey Map of the existing in-person class experience to identify periods of especially high and low motivation related to attending the in-person classes for both participants and instructors.
Results
Thirty-one individuals (10 married/partnered couples, 3 parent/child dyads, 1 person living alone with mild dementia, 4 instructors) participated in the interviews. We identified three key issues related to online delivery of PLIÉ: technology use, social connection as a primary motivator, and physical safety concerns.
Technology Use
We observed a contradiction between the way many people described their technology aptitude (‘we are not very tech savvy’) and their actual technology use. Most participants regularly and successfully used multiple devices in their daily lives such as a smart phone, camera, smart TV, laptop and/or desktop computers, e-readers, and tablets. Many also had devices in their homes that had been purchased or received as gifts that were not used due to a wide variety of reasons (e.g., obsolete technology, level of complexity, lack of interest). Participants rarely used a full feature-set of any device and often used workarounds such as notes and other paper-based reminders to help them recall passwords and instructions. Willingness to try to use new devices was most often driven by a specific need such as sharing family photos or use of banking services. When facing technical difficulty, participants most often assumed that they were somehow at fault.
Social Connection
Participants consistently reported that the social element of the in-person programs was a critical motivator for attending despite the challenges and numerous logistical challenges with attending in-person classes (e.g., dressing, eating, and managing transportation and parking). Specifically, socialization and the ability to connect in a meaningful way with others in similar situations were key aspects of the in-person program identified as essential to maintain in an online setting.
Safety
Participant safety was a commonly cited concern of all instructors, given the indirect nature of online instruction. Instructors emphasized the need to assess participants’ home environment and to incorporate verbal reminders to caution participants against overexertion, overextension, or loss of balance.
Based on these findings, we designed the initial online prototype to address barriers to technology use, maintain the social component of PLIÉ, and maximize participant safety. Key features included: (1) using familiar devices in participants’ homes to minimize the need for new technology and tapping into existing behavior patterns; (2) offering livestreaming, interactive group classes instead of pre-recorded videos to provide real-time instruction and feedback, and support feelings of social connection; (3) providing technology support and participant outreach to minimize technology hurdles and facilitate engagement; and (4) incorporating a home safety and set up assessment (See Figure 2) Comparison of in-person and online program components.
Phase 2. Refinement of Moving Together Content and Delivery
Goal
The goal of Phase 2 was to refine the prototype online Moving Together program through iterative testing. We conducted four 12-week cycles of testing (cohort-based 1-hour classes twice per week) with former participants of the in-person classes and naïve participants between February 2019 and April 2020.
Participants
In addition to overall eligibility criteria specified above, Phase 2 inclusion criteria also included willingness to participate in online classes during specified days/times. Exclusion criteria for PLWD and CPs included: wheelchair user; medical condition, physical limitation, visual or hearing impairment or psychiatric condition that could affect ability to participate; lack of memory loss diagnosis; or moderate/severe dementia severity. New participants were recruited through local caregiver support groups and social media postings. Participants from prior in-person programs were also invited to enrol in the online program. Potential Phase 2 participants completed an eligibility screen by telephone with a research assistant. Cognitive impairment was assessed using the Quick Dementia Rating Scale (Galvin, 2015) (6.5 to 12.5 inclusive based on CP report). Eligible and interested individuals received a consent form via mail or email; we obtained consent via videoconference by first reviewing the consent form and answering questions, followed by the PLWD and CP signing the consent form and returning it in a pre-paid envelope. For participants from our previous research studies, if the PLWD had previously been found to lack capacity, we requested verbal assent and asked their legally authorized representative to sign on their behalf. For new participants or those with unknown capacity to consent, we asked a series of yes/no questions to assess their understanding of study procedures, risks and benefits. A total of 25 individuals (14 PLWD, 11 CPs) enrolled and participated in one of the four 12-week online group classes. We did not systematically collect demographic data on these individuals.
Intervention Components
Technology and Safety Assessment
Prior to the first class, a Community Support Coordinator conducted a technology and safety assessment either in participants’ homes or via videoconferencing. This included assessing and testing of in-home devices and providing guidance on using the video-conferencing application. For example, some participants required HDMI cords and/or adaptors specific to their personal computer to connect it to their TV for optimal viewing on a larger screen; others required a stand for a personal tablet if a larger screen was not available. In addition, participants’ home setup included the selection of a stable chair without wheels and identifying a location with enough space to move safely and freely with as much of a full-body view on the screen as possible (Figure 3). Home set-up image included in Welcome Kit showing ideal distance (5-8 feet) between chair without wheels and camera.
Goals Assessment
The Moving Together team then conducted an assessment to gain information to personalize instruction and facilitate social connection. This assessment included questions about participants’ background, dyad relationship (if applicable), interests and hobbies, music preferences, and functional limitations, similar to the in-person program. (See Supplemental File 2 for Goals Assessment questions).
Welcome Kit
Participants received a ‘Welcome Kit’ that included a home setup guide, a booklet with weekly class themes, movement instructions for some of the basic movement sequences which was accompanied by photos, and sensory stimulation balls. If necessary, this kit included any technical equipment (e.g., cords or other adaptors) needed based on the earlier technology assessment.
Online Classes
Participants enrolled in cohorts to engage in the full series of 24 classes over 12 weeks. Online classes were limited to a maximum of 9 ‘windows’ on the screen, allowing for up to 8 pairs per group in addition to the instructor.
Class Content
Similar to the in-person program, the Moving Together Guiding Principles and class themes are based on the in-person PLIÉ programs (Table 1). To foster social connection and ensure everyone was welcomed and acknowledged, the instructor opened the online classroom 15 minutes prior to the start of class and checked in with each participant individually or in dyads as they arrived. Each 60-minute class then began with participants seated. Then the instructor led participants into present moment body awareness through movements that involve gently tapping all major body parts (including hands, arms, thighs, legs, feet, belly, back, neck, and head) and arm movements combined with deep breathing (e.g., raising arms overhead while inhaling and vocalizing while exhaling). The goal of these movement sequences is to bring participants into awareness of their bodies and breathing in the present moment, and to create a calming ritual that is repeated at the beginning and end of each class. Next, the instructor led participants through movement sequences tailored to meet the needs of the group and designed to gradually and methodically increase their functional capacity over the course of the 12-week program. The various movement sequences were performed seated, standing, and paired (e.g., PLWD and CP together) and focused on functional movements designed to support activities of daily activities, such as increasing range of motion, reaching, turning, transferring between sitting and standing, and balancing while standing and walking. Methodical, step-by-step instructions and an errorless learning process were used to ensure that all participants experience feelings of success. Mindful rests were incorporated throughout the class during which participants were encouraged to notice bodily sensations in the present moment. Finally, each class ended with a repetition of the opening sequence of present moment body awareness and breathing movements, and participants were invited to share appreciations and reflections on what brings them happiness and joy. The goal in this section of the program is to facilitate positive emotions and feelings of social connection. Personally meaningful music also is incorporated to further support positive emotions and feelings of connection.
Instructors
Instructors for the online program (n = 2) were Certified Feldenkrais Practitioners each with 10 or more years of private practice movement instruction and 5 or more years previous experience teaching in-person PLIÉ in research settings.
Data Collection and Analysis
Over the course of four 12-week online group classes, we refined program delivery, content, technology support, and engagement strategies. The first two group classes focused primarily on technology and audio-visual quality. We tested off-the-shelf audio-video conference tools including the browser-based platform TokBox and Zoom (both browser-based and app). We also assessed participants’ challenges in navigating their existing devices and ability to access the classes online. The second two groups focused primarily on identification and refinement of content and instructional elements for the online setting. Following each class, the instructors debriefed with the Community Support Coordinator and the study team to determine specific adjustments and refinements needed for the next class.
Key Refinements to Moving Together Online
Technology
The series of four 12-week classes provided opportunities to test and make key refinements in the use of technology and audio-visual quality. These included: providing real-time personalized technology support for participants prior to and during classes; instructors’ use of Bluetooth headsets to optimize audio quality; and incorporating music (e.g., genres or specific songs participants identified during Goals Assessments) through the video conferencing software. For example, when using TokBox, instructors played music through speakers physically located in their room; when using Zoom, the instructors used a music streaming app to share the audio via computer sound directly through the Zoom application screen sharing function. To enhance participant experience and ability to clearly see the instructors, we increased visual contrast through the instructors wearing bright, solid-colored clothing and shoes in front of neutral backgrounds. To support participant attendance, we incorporated class reminder emails the day before each class with the link and instructions for logging in; if participants did not log in on time, we called them on the phone.
Instructional Strategies
Key refinements to instructional elements for the online setting included: increased attention to participants’ subtle cues such as facial expressions, gestures, and interactions between dyads; conversational adaptations and coaching based primarily on visual cues; and use of videoconferencing software Spotlight and Gallery view features. At the beginning of the class series, the instructor asked each person to introduce themselves while the instructor used the video conferencing Spotlight tool focus the group’s visual attention onto the participant or dyad who was sharing. Each week, the instructors presented a discussion topic based on the program principles (Table 1) followed by one or two questions designed to prompt reflection and sharing. During this sharing, the instructor used the Gallery View to offer a group experience and used the Spotlight tool to highlight each dyad as they were sharing. During the movement sequences, the instructor used the Spotlight view on themselves to and focus the participant’s attention on the movement instruction while at the same time the instructor maintained the Gallery View to observe the participant’s movements closely. At the beginning of class, during class rest periods, and during the closing portion when sharing appreciations, the instructors used the Gallery View so the class participants could see each other and share their reflections while the instructor inquired about the participant’s experiences, listened carefully, and validated responses by repeating the response to acknowledge having heard the participant and ensuring that the group could hear each participant’s contributions.
Phase 3: Feasibility and Satisfaction with Online Delivery
Goal
The goal of Phase 3 was to assess feasibility and satisfaction of the refined online Moving Together program. We conducted four 12-week groups (cohort-based 1-hour classes twice per week) using the Zoom videoconferencing platform at the onset of the COVID-19 pandemic between April to July 2020.
Participants
We first invited people who had participated in Phases 1 and 2 Phase 2 followed by people with mild cognitive impairment who had recently completed a neuroimaging study of the in-person program. 16 Finally, we recruited additional dyads who had not previously been exposed to the online program using the same eligibility criteria and recruitment methods as Phase 2.
Data Collection
We assessed feasibility based on attendance documented immediately after class by instructors and program completion. To assess satisfaction and participant-reported outcomes, we sent a “class experience” survey to all Phase 3 participants who completed the 12-week program. Participants each received an email with a link to the self-administered online survey; CPs were asked to help PLWD complete the survey if needed. The survey included ratings of the program overall (4-point Likert scale [poor to excellent]; likelihood of recommending to others on a scale from 0 to 10); specific aspects of class experience (six items scored on a 4-point Likert scale [rarely/never to mostly/always]. In addition to these scales, participants completed a series of open-ended questions that asked about changes noticed in self and others they attributed to Moving Together and for feedback on what they liked the most and least about the online classes, particularly given that the classes were offered during the COVID-19 shelter-in-place orders (see Supplemental File 3 for class experience items and open-ended questions.) We also measured social isolation using the 4-item PROMIS v2.0 social isolation scale (response categories were modified to be consistent with the “class experience” scale).
Analysis
For feasibility, we calculated the mean (standard deviation, SD) percent of classes attended and the proportion of participants who completed the program. For satisfaction and participant-reported outcomes, we calculated the percent of responses for each survey item that were “good” or “excellent” for the overall rating, 8 to 10 on the scale for likelihood of recommending to others, “often/mostly/always” for positive items and “never/rarely” for negative items. We also calculated summary scores for class experience items and social isolation, and we converted the raw social isolation summary score to a scaled T score (mean 50, SD 10). 24
We analyzed open-ended survey data using directed content analysis, a hybrid approach utilizing both deductive and inductive coding. 25 Responses to each survey item were exported to Microsoft Excel. First, using a previously established coding scheme for qualitative analysis of PLIÉ trial data, 18 one study team member AL manually applied the following a priori codes to open-ended survey responses: physical function, cognitive function, emotional wellbeing, social connection. FMN then reviewed the coded data for accuracy, identified new concepts that did not fall into a predetermined category (e.g., present-moment body awareness), and applied inductive codes. We discussed findings with the larger study team and reached consensus on a primary code for each open-ended response and interpretation.
Results
Feasibility
Moving Together Online Class Participants, Phase 3.

Satisfaction
Moving Together Online Class Experience & PROMIS Social Isolation Ratings, Phase 3.

aData missing as follows: Recommend to others (1 PLWD, 1 CP); I feel that my problems are not unique (1 PLWD, 1 CP); I feel that people barely know me (1 PLWD); I feel that people are around me but not with me (1 PLWD).
Participant-Reported Outcomes
Participant feedback related to Moving Together impact on quality-of-life domains, Phase 3

Physical Function
Responses related to physical function focused on the impact of functional movements learned during the classes on PLWD/MCI sense of balance, strength, range of motion, and reflexes. One person with MCI explained how they ‘learned about balance [and] working with gravity’; another noted they are ‘getting more range of motion in my shoulders and lower back.’ A care partner commented how ‘…squeezing and bouncing the ball has really helped [my spouse’s] reflexes. I could never throw anything at him as he wouldn't even attempt to catch it. Now here comes keys, empty rolls of toilet paper, etc. He loves the challenge and 95% of the time he catches them. Before he wouldn't try!’ Participants reported additional physical benefits such as increased energy, relaxation, and decreased pain.
Cognitive Function
Participants described improvements in aspects of cognitive function, specifically mental clarity and learning for PLWD and MCI. For example, a person with MCI said that after the classes, ‘Usually my mind feels somehow clearer, more focused.’ One care partner noted how their spouse, ‘Seemed enlivened by the challenge of learning new things.’
Emotional Well-Being
PLWD and MCI described how participating in the online classes provided an opportunity for relaxation and improved their mood. CP responses focused on how the classes helped them to relax and manage stress. For example, one CP said, ‘I felt more relaxed and focused after the class. I was always frazzled beforehand. Stopping and taking care of myself through the exercises helped me feel more balanced or centered afterwards and through the rest of the day.’
Social Connection
Social isolation scores overall suggested relatively low levels of isolation during the classes, with mean (SD) standardized scores of 39 (6) compared to normative values of 50 (10) (Table 3). However, feelings of social isolation seemed to be slightly higher in PLWD (42 [7]) than people with MCI (38 [6]) or CPs (36 [3]). For example, 71% (n = 5) of PLWD said they sometimes (n = 4) or mostly/always (n = 1) felt that ‘people barely know me’ during the classes. On the other hand, 100% (n = 7) said they rarely/never ‘felt left out.’
Open-ended responses from PLWD, CP, and MCI illustrated how participating in the online classes enhanced social connection and fostered intimacy and ‘camaraderie’ with others in the group over time (see Table 4). For example, one PLWD said, ‘As it went on, I noticed we became closer.’ A care partner wrote: ‘We seemed happier and more connected towards the end. . . more like a family, inquiring about each other’s lives.’
Although responses highlighted an increased sense of social connection and shared experience, one participant with MCI who had attended in-person classes prior to COVID-19 reflected on the limitations of the online format: ‘I am much quieter. This is due to the [online] platform. In the classroom, the interchange was much freer and responsive. The [online] format is one-person-at-a-time and I tend to remain silent as opposed to the classroom setting.’
Self-Concept for PLWD and MCI
Participants noted positive impacts on self-concept including self-esteem, feeling useful, and presentation of self. For example, a participant with MCI explained how they developed ‘More patience and empathy with what my body can do. Less immediate shame and more confidence. Awesome! A miracle!’ One care partner expressed that ‘[Dementia] can become a silent disease. You have really helped him to see his importance.’ Some participants with dementia and MCI noted how they ‘Enjoyed interacting with others in the same boat’ and highlighted how interacting with other people with cognitive impairment was a positive experience.
Caregiving Self-Efficacy
Care partners described the impact of participating in Moving Together online on their comfort and confidence with aspects of caregiving. For example, a CP explained how they became more flexible in their caregiving approach: ‘I’m more comfortable letting [him] do as little or as much as he chooses and do things his own way, even though he isn't following instructions.’ Moving Together also provided respite and a form of present-centered self-care for CPs. ‘This is something I can participate in with my husband who has been diagnosed with Alzheimer’s. Once you get over the newness or fear of not doing a good or right job (which there is no right or wrong) you have a wonderful tension-free relaxed hour where I forget all my problems and new challenges dealing with his disease.’
Finding Purpose and Improved Relationships
Care partners also explained how participating in Moving Together online helped to provide meaning to their role. One CP wrote that ‘The classes were really special for me. They gave me a greater purpose and a positive way to participate with family, my mom, my in-laws, and even my sister’s and husband’s family as they were invited to attend.’ Others described how their relationship with their spouse with dementia improved: ‘We talk more about how we are doing.’
Present-Moment Body Awareness
PLWD and MCI described how they were more aware of their breath both during and after the online classes. One person said, ‘I find that I am more conscious of my breathing patterns.’ Another explained how they were ‘Developing [a] habit of returning to breath. Am I breathing? Breathing fully?’ In addition to increased breath awareness, a care partner said, ‘I liked having the opportunity in the middle of the day to pause and listen to myself,’ highlighting how the classes provided the opportunity to experience present-moment awareness.
Motivators for Participation During COVID-19 Pandemic
Participant responses to open-ended questions about what they ‘liked most’ about the classes highlighted four areas that enhanced overall experience and motivated attendance: social connection, physical aspects, quality of instructors, and online access to the classes. One PLWD shared how they ‘want to continue participating in the Moving Together classes, especially because I am no longer able to attend the dementia day program.’ CPs highlighted how Moving Together online was a ‘life-line’ that provided a safe activity during the COVID-19 pandemic and shelter-in-place orders. One CP reflected on how if Moving Together had not been available online, their spouse ‘. . . may have gone in a shell, not tried anything new, not had anything to look forward to and I may have thrown up my hands and sent him off. . . Not much is offered to Alzheimer’s patients, and you have really helped him become a much more positive person.’ Notably, there were no safety-related adverse events reported by participants related to participation in the online program.
In addition to having a safe activity during the coronavirus pandemic, responses from participants with MCI focused on how the online program ‘help[ed] with the monotony’ of being home. As one participant explained, ‘Having the class twice a week helps give our week some shape, because [shelter-in-place] means that all days look alike. Class means it's either Tuesday or Thursday.’
Suggestions for Program Improvement
Feedback on the least liked aspects of the online classes focused on technology challenges (e.g., audio quality, bandwidth) and inherent limitations of an online vs in-person setting. For example, one PLWD who had previously attended in person noted that ‘We did not have extra time to go interact with other participants and the instructor.’ Feedback on least liked aspects reflected the mix of participants with varied levels of physical and cognitive capacity. For example, some participants expressed a desire for more physically challenging exercises: ‘My spouse and I have often wished that the exercises could involve more strenuous activities - but we do understand that the group has a variety of abilities.’
Discussion
In this study, we found that the online Moving Together program—a theoretically informed, evidence-based, mind-body group movement program for people living with cognitive impairment or dementia and care partners—was feasible and satisfying for participants. Online delivery was feasible, with 77% completion and 75% attendance rates. Participants reported high satisfaction; 96% of participants rated the program as excellent or good and 88% were highly likely to recommend the program to others. These findings suggest that online, livestreaming multimodal programs can provide engaging activity for people living with cognitive impairment and their CPs.
We also found that participants reported positive outcomes across multiple quality of life domains: physical function, cognitive function, emotional wellbeing, and social connection. PLWD/MCI experienced improvements in self-concept/acceptance and CPs reported improvements in caregiving efficacy. These findings are in concordance with previous research pointing toward the combined physical, cognitive, and psychosocial benefits of multimodal interventions.12,26,27 While video-based interventions for older adults that combine both physical and social components have been studied less than those focused on physical activity alone, 28 our study demonstrates the feasibility and potential benefits of an online intervention that enhances social connection among PLWD, MCI and CPs while simultaneously improving physical function. Socialization is a motivating factor for older adults’ participation in community-based activities; 29 our findings suggest that technology can be used to enhance social connection rather than replacing it and that leveraging social connection can increase engagement among PLWD and MCI in an online setting.
Existing online interventions for dementia largely target caregivers individually and without PLWD and focus primarily on psychoeducation30,31 emotion regulation and mental health,32,33 and social support.30,34 Findings from our study suggest that participating in the online program as a shared experience allowed care partners to find a greater sense of purpose and connection with their loved one, leading to increased caregiving self-efficacy. Furthermore, all participant types reported an enhanced sense of present-moment body awareness, a concept which is not typically assessed as part of dementia quality-of-life measures.
In addition to our main findings, our study adds to the knowledge on the design and delivery of online interventions for people with dementia. Specifically, we demonstrate the effectiveness of using human-centered design for translating the evidence-based in-person programs to an online format designed for the specific needs of PLWD and MCI. Although user-centered design is increasingly utilized to develop health technology and online interventions for older adults,28,35 these methods are used less frequently among PLWD/MCI. By engaging PLWD and CPs in an iterative design process, we were able to identify the key elements critical to effective program delivery and real-time support necessary to engage this audience.
Strengths and Limitations
Our results should be interpreted with several limitations in mind. First, our study included participants who may not be representative of people with dementia or cognitive impairment in the general population, particularly as older adults who utilize technology are more likely to have higher levels of educational attainment and affluence. Access to the Moving Together online program was limited to individuals with internet connectivity and video-enabled devices larger than a smartphone, and by extension might exclude other determinants of digital inequality, including age, education, income, gender, language, housing and/or generational status. A strength of this study is inclusion of participants with a mix of dementia types and severity in addition to dyads of PLWD/MCI and CPs. Compared to the in-person trials, which had a small number of adverse events, there were no observed or reported adverse events related to the online program.
Half of the participants in our study had prior exposure to either the in-person program or Phase 1 online program development/testing; choosing to continue in an online format may have contributed to satisfaction levels. However, we found no meaningful differences in survey scores or patterns in qualitative feedback between prior or naïve participants. As Phase 3 classes occurred during the early part of the coronavirus pandemic when there were limited options for activities outside the home environment and widespread isolation from usual social support networks, this shared experience potentially influenced the value and meaning of the program independent from prior exposure. This study used self-report measures and open-ended responses to assess participants’ experience. While the social isolation measure is validated and widely used, 24 responses may be subject to recall, social desirability, or expectancy biases, particularly after participation in a 12-week program. Future research should consider using objective behavioral assessment or video analysis to assess change in physical function, social engagement, and other outcomes. Another limitation is the lack of a control group, although the primary aim of this pilot study was to evaluate feasibility of online delivery of PLIÉ to inform future larger-scale studies.
Conclusions
Our findings demonstrate the feasibility and acceptability of a livestreaming, mind-body group movement program for people across the spectrum of cognitive decline and their care partners and provide preliminary support for improved outcomes across multiple quality-of-life domains. In sum, the results suggest that participants found the Moving Together online program to be accessible and beneficial. We found that involving people with dementia and cognitive impairment and their care partners in human-centered design processes is an effective strategy to develop and tailor interactive online interventions for this population. Future studies should investigate the efficacy of multimodal online interventions to improve multiple quality-of-life outcomes for MCI/PLWD/CPs in larger scale trials with long-term follow up.
Supplemental Material
Supplemental Material - Adaptation of an In-Person Mind-Body Movement Program for People with Cognitive Impairment or Dementia and Care Partners for Online Delivery: Feasibility, Satisfaction and Participant-Reported Outcomes
Supplemental Material for Adaptation of an In-Person Mind-Body Movement Program for People with Cognitive Impairment or Dementia and Care Partners for Online Delivery: Feasibility, Satisfaction and Participant-Reported Outcomes by Francesca M. Nicosia, PhD, C-IAYT, Jennifer A. Lee, GCFP, Margaret A. Chesney, PhD, Cynthia Benjamin, MBA, MS, Amanda N. Lee, MS, Wolf Mehling, MD, Rebecca L. Sudore, MD, and Deborah E. Barnes, PhD, MPH in Global Advances in Integrative Medicine and Health
Footnotes
Acknowledgments
We would like to acknowledge Exygy for assistance with the Human Centered Design process including conducting Phase 2 interviews and creation of the Journey Map. A de-identified data set will be available upon request by contacting the corresponding author once all primary analyses and reports have been completed. This study was not pre-registered.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Ms. Benjamin is CEO of Together Senior Health, which is commercializing Moving Together. Ms. A. Lee is a former employee of Together Senior Health. Ms. J. Lee is a current employee of Together Senior Health. Dr. Barnes is Chief Science Advisor for Together Senior Health. Dr. Mehling and Dr. Chesney are co-inventors of PLIÉ and Paired PLIÉ and have the potential to earn royalties. Dr. Nicosia and Dr. Sudore have no conflicts of interest to declare.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by a Small Business Innovation Research (SBIR) grant from the National Institutes of Health (R44 AG059520).
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.