
Abstract
Background
Whole health is a holistic approach encompassing integrative medicine, emotional, and spiritual health and is critical to improving health outcomes among individuals with multimorbidity.
Objective
To examine the prevalence of Whole Health activities and the association of multimorbidity and Whole Health activities using nationally representative datasets.
Methods
As no single dataset has information on Whole Health self-care activities, data from the 2017 National Health Interview Survey (n = 25 134) was used to measure participants’ mind-body therapy usage, sleep, mental health, and physical activity. We used the 2017 Behavioral Risk Factor Surveillance System (n = 347 029) to assess regular vegetable and/or fruit consumption.
Results
A significantly lower percentage of adults with multimorbidity had adequate sleep (58.2%vs.67.1%), no psychological distress (71.8%vs.82.1%), adequate physical activity (48.2%vs.62.1%), and regular vegetable and/or fruit consumption (54.2%vs.56.6%) compared to those without multimorbidity. Although lower percentages of adults with multimorbidity utilized mind-body therapies (22.9%vs.25.2%), the association was reversed when adjusted for socioeconomic factors. In the fully adjusted models, adults with multimorbidity were more likely to use mind-body therapies (AOR = 1.19, 95%CI = 1.09, 1.31). Furthermore, when adjusting for other independent variables, the associations of multimorbidity with sleep, psychological distress, and diet were exacerbated, and the association of multimorbidity with physical activity was attenuated.
Conclusion
Adults with multimorbidity were less likely to engage in most of the Whole Health activities except mind-body therapies compared to the no multimorbidity group. Findings suggest that adjustment for other factors such as age and socioeconomic status changed the magnitude and direction of the association of multimorbidity with Whole Health activities.
Introduction
Multimorbidity, the concurrent presence of 2 or more chronic conditions, is a global concern for prevention and management, as multimorbidity is associated with health decline and mortality. 1 The prevalence of multimorbidity in the U.S. is approximately 1 in 4 U.S. adults. 1 For individuals with multimorbidity, the implementation of disease-specific guidelines to improve health has fallen short. Clinical guidelines and quality standards derived from clinical trials have limited relevance for those with multimorbidity because trials typically exclude individuals with multiple chronic conditions. 2 For individuals with multiple conditions, challenges exist to implementing evidence-based practices due to the proliferation of the standard of care for each disease. 3 Health systems, providers, patients, government agencies, and other stakeholders are working towards more sustainable models of care.
One of the sustainable care models that may improve health among those with multimorbidity is the Whole Health perspective. The Whole Health perspective not only focuses on singular, specific diseases and disease guidelines but also on “what matters to the person.” The Whole Health model is based on the Institute of Medicine and the World Health Organization (WHO) standards, in which balanced health involves health and healing approaches to mental and emotional; physical and structural; nutritional and chemical; environmental, and spiritual aspects of care. 4
Individuals from various backgrounds and disciplines such as pharmacists, psychologists, social workers, clinicians, chaplains, physical assistants, complementary health practitioners, and many others, have contributed to the evolution of the Whole Health Model. 5 There are different versions of the Whole Health approach from the National Institute of Whole Health (NIWH), 6 the National Center for Complementary and Integrative Health (NCCIH), 4 the Veterans Health Administration (VA), 7 the Whole Health Institute, 8 and TakeCare 9 that extended the NIWH model. However, all these versions have some common elements such as person-centeredness, disease-agnostic holistic approach, integration of traditional and complementary therapies; self-care as a pillar of health and well-being; the role of social determinants of health (SDoH), and care supported by health systems, programs, and policies.5-9
It is essential to have an evidence-based approach for Whole Health practices to contain costs, coordinate care, satisfy the patients, and improve outcomes, 10 specifically among those with multimorbidity. 11 There is some evidence that Whole Health activities that intersect self-care activities and integrated care with both conventional and complementary medicine can improve clinical outcomes, 12 decrease costs, 13 well-being of employees, 13 patient satisfaction, 13 physical and emotional health, 12 and employment. 12
For many health conditions, self-care in terms of Whole Health activities can play a significant role in primary, secondary, and tertiary prevention activities. 14 All types of prevention activities can succeed if the 5 critical activities of self-care are practiced. These activities are (1) the power of mind, (mind-body therapies), (2) recharge (adequate sleep), (3) mental health (no or low psychological distress), (4) moving the body (adequate physical activity), and (5) nutrition (regular vegetable and/or fruit consumption). 15
The growing burden of multimorbidity coupled with information technology has propelled individuals towards high-value practices such as Whole Health activities. 16 However, limited literature is available on the prevalence of Whole Health activities, specifically among individuals with multimorbidity who need it the most. We acknowledge that there have been studies on the reciprocal relationships of individual activities such as sleep, 17 physical activity,18,19 diet, 20 and psychological distress 21 with incident multimorbidity and the association of type of multimorbidity on use of alternative and complementary medicine including mind-body therapies. 22 However, studies on the prevalence rates of all Whole Health activities among those with multimorbidity are sparse. Therefore, this research aimed to examine the prevalence of Whole Health activities and the association of multimorbidity and Whole Health activities among adults in the U.S. using nationally representative datasets.
Methods
Study Design and Data Sources
We used a cross-sectional design and analyzed data on adults aged 18 or older from 2 nationally representative health surveys. As no 1 health survey collected information on all 5 self-care activities of the Whole Health model, we used the 2017 National Health Interview Survey (NHIS) to measure the prevalence of mind-body therapies, adequate sleep, psychological stress, and physical activity, and the 2017 Behavioral Risk Factor Surveillance System (BRFSS) to assess regular vegetable and/or fruit consumption. We selected 2017 because it represented the most recent available data on Whole Health self-care activities.
We harmonized measures in the 2 datasets, and variables were recoded to have the same categories or levels between the NHIS and the BRFSS. The study samples were restricted to adults without missing data on Whole Health self-care activities and multimorbidity variables and without missing age (BRFSS 2017). The analytical samples comprised 25, 133 adults from the NHIS and 343 341 adults from the BRFSS, representing about 231.8 million and 183 million adults, respectively.
Measures
Dependent Variables
NHIS-2017 - Mind-body therapies (Yes/No)
Adults who practiced mantra, mindfulness, and spiritual meditation 23 or meditation through Yoga, Tai chi, Qigong, or guided imagery during the past 12 months were considered to use mind-body therapies.
NHIS 2017 - Adequate Sleep (Yes/No)
We defined adequate sleep using the duration of sleep based on the consensus statement of the American Academy of Sleep Medicine and Sleep Research Society. 24 Based on the question “On average, how many hours of sleep do you get in a 24-hour period?”, we classified adults with at least 7 hours of sleep per night as having adequate sleep.
NHIS 2017 - Adequate Physical Activity (Yes/No)
Adequate physical activity was derived from questions about frequency, duration, and intensity of leisure time physical activity and strength training reported weekly. Using the 2008 Physical Activity Guidelines for Americans, 25 adults with at least 150 minutes of moderate-intensity activity per week or who engaged in muscle-strengthening activities at least 2 times per week were considered to have adequate physical activity. 26
NHIS 2017 – Low or No Psychological Distress (Yes/No)
A person’s mental health was measured by the Kessler Psychological Distress Scale (K6). The K6 consists of 6 questions on nervousness, hopelessness, worthlessness, restless/fidgety, sadness not able to be alleviated, and struggling in effort during the past 30 days. 27 Each question is scored from 0 (None of the time) to 4 (All of the time) and the sum of these scores range from 0 to 24. Based on a study that validated a sub-threshold cut point for moderate distress, we classified adults with scores less than 5 as having low psychological distress. 28
BRFSS 2017 - Regular vegetable and/or fruit consumption (Yes/No)
As of 2017, BRFSS now asks 6 questions as part of their dietary module. 29 These questions ask how frequently a respondent consumed different types of fruits and/or vegetables in the previous 30 days. In the absence of more comprehensive dietary questions, this study defined individuals with “regular vegetable and/or fruit consumption” as those who had at least 1 fruit and vegetable per day in the past 30 days.
Key Independent Variable: Multimorbidity (Yes/No)
This article defined multimorbidity as the co-occurrence of 2 or more chronic conditions in a single individual. 30 Multimorbidity was measured with an indicator variable 1 representing the presence of multimorbidity and 0 representing no multimorbidity. Adults with 2 or more of the following chronic conditions in BRFSS and NHIS (arthritis, asthma, cancer, chronic kidney disease, chronic obstructive pulmonary disease, diabetes, hyperlipidemia, hypertension, heart disease, and stroke) were classified as having multimorbidity. These chronic conditions were based on the availability of data as well as the framework for managing multiple chronic conditions for research, program, and policy. 31
Other Explanatory Variables
For adjusted analyses, we controlled for biologic factors, socioeconomic factors, and lifestyle factors. Biological factors included: sex (male/female); age in years (18-39, 40-49, 50-64, 65+); and race/ethnicity (White, African American, Hispanic/Latino, Other). Socioeconomic factors included: education (less than high school, high school, some college, college); health insurance status (yes, no); poverty relative to the federal poverty line (FPL) for NHIS (<100% FPL, 100-200% FPL, 200-400% FPL, >400% FPL); and annual household income for BRFSS (less than $10k, $10k-25k, $25-75k, >$75k). Social support included marital status (married, never married, divorced/widowed/separated). Lastly, lifestyle factors included obesity (under/normal weight, overweight, obese); smoking status (current, former, never); and alcohol use, which differed between surveys. For NHIS, alcohol use was measured as former, current, or never, whereas for BRFSS, it was measured as heavy drinking, moderate drinking, or no drinking. We also included a variable for the respondent’s region (Northeast, Midwest, South, West). We included a missing indicator for variables with missing data. Although missing data were included in the analysis, we did not present them in tables.
Statistical Analyses
Statistically significant group differences in Whole Health self-care activities by multimorbidity status were tested with Rao-Scott chi-square tests. Adjusted relationships of multimorbidity with Whole Health activities were tested with separate multivariable logistic regressions on each of the Whole Health activities. In these logistic regressions, we controlled for age, sex, race/ethnicity, education, income, health insurance, obesity, smoking, and region. We conducted the regression analysis using multiple models to examine changes in the association of multimorbidity with Whole Health activities. The first model included only multimorbidity (Yes/No) as an independent variable. In the second model, we adjusted for multimorbidity, sex, age, race and ethnicity, education, and poverty status. The third model was fully adjusted for multimorbidity, sex, age, race and ethnicity, education, poverty status, health insurance, marital status, body mass index, current smoking, alcohol use, and region.
To account for the complex survey design of the NHIS, we used SAS survey procedures with clustering, strata, and weights. 32 Statistical analysis with BRFSS used the final weights provided in the dataset to generalize from the sample to the population. 33
Results
Description of Selected Characteristics of Respondents. Adults (age ≥ 18 Years). National Health Interview Survey (NHIS) 2017 and Behavioral Risk Factor Surveillance System (BRFSS) 2017.

Based on 25 133 adult respondents (age 18 years or older) from the National Health Interview Survey and 343 341 adult respondents from the Behavioral Risk Factor Surveillance System. Due to missing data in BRFSS 2017 (Race and Ethnicity, Marital status, Education, and health insurance) and NHIS 2017 (Marital status, Education, and health insurance), the percentages may not total 100%.
Div/Sep/Wid: Divorced/Separated/Widowed; FPL: Federal Poverty Line; N: Unweighted number of individuals in a category. Wt. %: Weighted; HS: High school.
Multimorbidity and Whole Health Activities
Prevalence of Whole Health Activities by Multimorbidity Status. Among Adults (age ≥ 18 years). National Health Interview Survey (NHIS) 2017 and Behavioral Risk Factor Surveillance System (BRFSS) 2017.

Based on 25 133 adult respondents (age 18 years or older) from NHIS and 343 341 adult respondents from the BRFSS. Mind-body therapies, low or no psychological distress, adequate sleep, adequate physical activity, and the number of Whole Health self-care activities were measured using NHIS 2017, and regular vegetable and/or fruit consumption was measured using BRFSS 2017. Statistical significance is based on Rao-Scott Chi-square tests.
N: Unweighted number of individuals in a category. Wt. %: Weighted column percent.
Odds Ratios and 95% Confidence Intervals (CI). From Separate Logistic Regressions on Whole Health Activities. Adults (age ≥ 18 years). National Health Interview Survey (NHIS) 2017 and Behavioral Risk Factor Surveillance System (BRFSS) 2017.
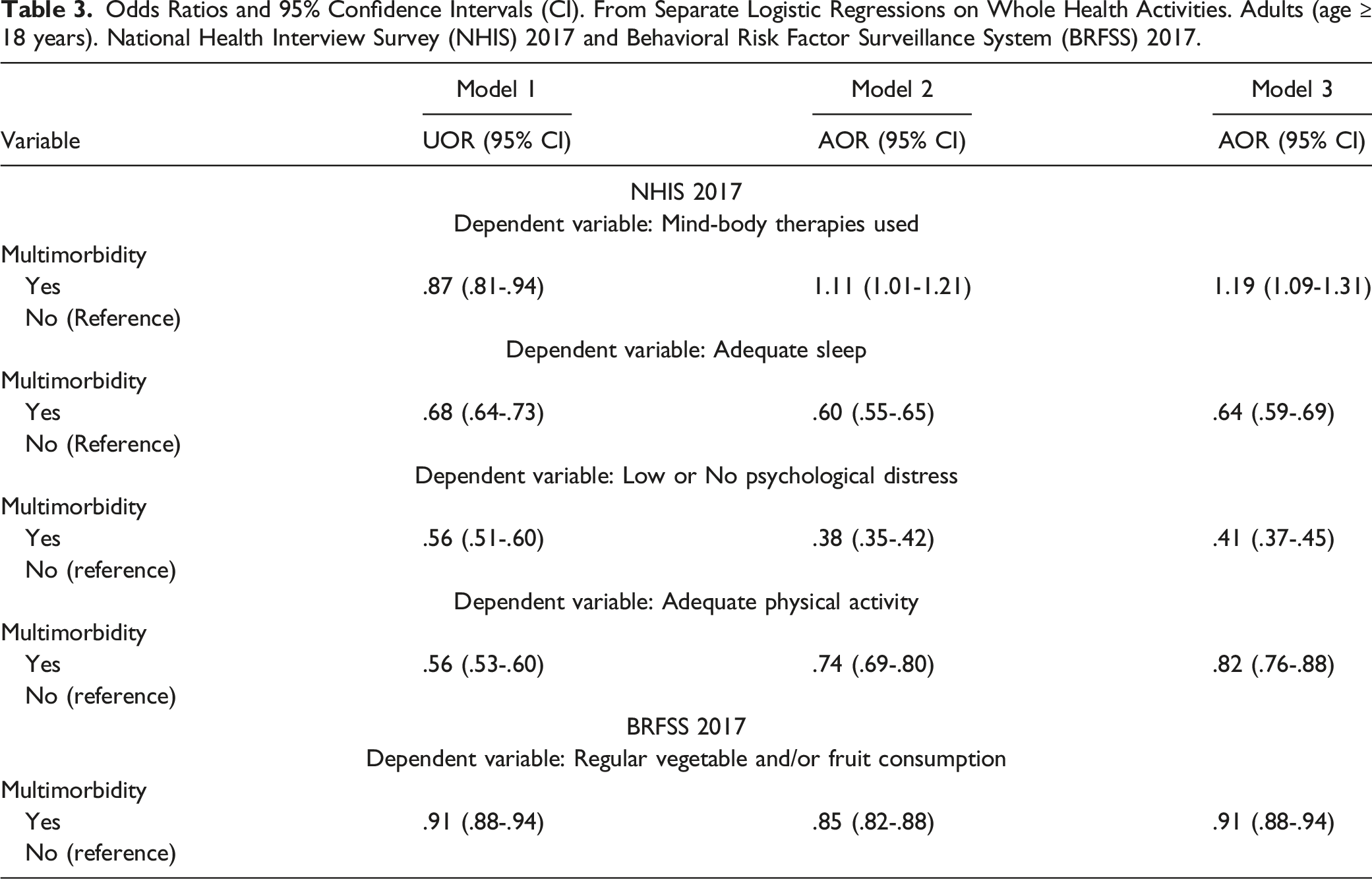
Fully adjusted multivariable regression analyses in Table 3 revealed similar results for adequate sleep (AOR = .64, 95% CI = .59-.69), no or low psychological distress (AOR = .41, 95% CI = .37-.45), adequate physical activity (AOR = .82, 95% CI .76-.88), and regular vegetable and/or fruit consumption (AOR = .91, 95% CI = .88-.94). However, the adults with multimorbidity had higher odds of mind-body therapy use in the fully adjusted model (AOR = 1.19, 95% CI = 1.09, 1.31). An examination of model 2 suggests that adjustment for education reversed the association, and adults with multimorbidity were more likely to use mind-body therapies (AOR = 1.11, 95% CI 1.01-1.21).
Discussion
The power of Whole Health activities in terms of self-care as 1 of the pillars of a Whole Health model has been well documented in the scientific literature. 34 In this article, we examined the prevalence and association of multimorbidity with Whole Health activities as part of a Whole Health model. The prevalence rates found in our study were consistent with those from prior published studies that have separately analyzed self-care activities. For example, Malecki et al, described that physical inactivity in the United States ranges from 17.3% to 47.7%, 35 while the CDC states 31.6% of adults get insufficient sleep according to NHIS data from 2011-2014. 36
In fully adjusted analyses, adults with multimorbidity were found to have lower odds of Whole Health activities compared to the no multimorbidity group except for mind-body therapies. Our study findings also highlight how the adjustment of other independent variables changed the strength and directions of associations of multimorbidity with the type of Whole Health activities. For example, adjusting for age and socioeconomic status, the association of multimorbidity with sleep, psychological distress, and diet was exacerbated. However, the same factors attenuated the association of multimorbidity with physical activity and changed the direction of the association with mind-body therapies. These findings suggest that socioeconomic factors differentially contribute to the association of multimorbidity with Whole Health activities. Therefore, programs and policies promoting Whole Health activities must consider these nuanced relationships.
Our study results with respect to psychological distress are consistent with global studies in which multimorbidity has been found to be associated with psychological symptoms in 42 countries. 37 Although the causal pathways connecting multimorbidity to psychological stress are complex with numerous interacting factors such as lifestyle choices, and genetic, environmental, social, and behavioral factors, 38 our findings suggest monitoring mental health below the threshold for mental health disorders offers potential opportunities for early prevention. 39 In this context, the healthcare systems can provide support services to mitigate the effects of stress among adults with multimorbidity.
Our study found that those with multimorbidity were less likely to engage in recommended physical activities, even though associations with exercise and improvement of life expectancy in those with multimorbidity have been documented. 40 It is possible that pain and functional limitations may limit the participation of adults with multimorbidity in physical activities.41,42 Low-impact activities such as water-based programs or stationary biking, or meditation-based activities such as yoga and Tai Chi are physical interventions that can be recommended for patients with chronic conditions if their abilities and conditions allow. 43
Inadequate sleep has been linked to the development of chronic conditions such as diabetes, hypertension, and heart disease. 44 Moderate-severe sleep disturbances have also been associated with a higher speed of chronic disease accumulation, regardless of confounders. 45 A low percentage of adults with multimorbidity in our study had adequate sleep, similar to results found in prior studies. Additionally, dietary intake is central to overall health, and in our study, a lower proportion of adults with multimorbidity were less likely to report having regular vegetable and/or fruit consumption. Our findings are consistent with a cross-sectional study conducted by Dekker et al., 46 where it was noted that higher adherence to a dietary pattern characterized by high intakes of meats, alcohol, potato, and also a “snack pattern” was associated with an increased prevalence of multimorbidity. Diet and sleep are closely related as studies have observed consistent associations with short sleep duration, higher caloric intake, higher absolute intake of fat, lower fruit intake, and lower quality diets. Therefore, Whole Health promotion strategies targeted at improving dietary intake and implementing cognitive behavioral therapy to help with insomnia should be considered in those with multimorbidity.
Previous research has documented a wide range of barriers to Whole Health activities among adults with multimorbidity. 47 These barriers suggest a multitiered and comprehensive approach such as the 1 proposed by the VA, where a health system provides comprehensive support based on an individual’s values, needs, and goals to promote Whole Health activities. 7 The comprehensive approach utilizes patient engagement support through education, wellness programs, and clinical care. 7
Regarding study strengths, we used nationally representative data sets to analyze a comprehensive list of factors associated with Whole Health. This study also adds to the limited body of evidence on the direct analysis and prevalence of Whole Health activities. Those with multimorbidity had lower odds of adequate sleep, physical activity, regular consumption of vegetables and/or fruits, utilization of mind-body therapies, and low or no psychological distress. As published literature suggests that multimorbidity is associated with unfavorable clinical outcomes, integration and improvement of Whole Health activities for the prevention and management of multimorbidity may be beneficial.
Our study did have some notable limitations. This was a cross-sectional study design in which self-reported data is subject to recall data. A noteworthy finding is that we needed to analyze 2 different datasets to estimate the state of Whole Health self-care among adults in the U.S. Widespread adoption of the Whole Health model will require scientific evidence on its beneficial effects. Building such an evidence base is not possible without data on standardized measures of Whole Health. Unfortunately, beginning in 2019, NHIS has also moved away from collecting information on some of these measures every year. For example, data on psychological distress will be collected once in 3 years - 2019, 2022, and 2025. Thus, our findings suggest that research efforts and investment need to be made to collect nationally representative data on all Whole Health measures during the same time period. We support a call to action for collecting standardized Whole Health measures in datasets sponsored by federal agencies.
Conclusion
Approximately one in 3 adults had multimorbidity. Adults with multimorbidity were less likely to report Whole Health activities, suggesting a system of support that moves away from a disease orientation to health promotion is needed. In addition, no 1 dataset collected information on all 5 activities of Whole Health activities during the same year. Therefore, we suggest collection of standardized measures on Whole Health activities for healthcare research, programs, and policies.
Based on 25 133 adult respondents (age 18 years or older) from the NHIS 2017 and 343 341 adult respondents from the BRFSS 2017. Model 1 adjusted only for multimorbidity variable. Model 2 adjusted for multimorbidity, sex, age, race and ethnicity, education, and poverty status. Model 3 is fully adjusted for multimorbidity, sex, age, race and ethnicity, education, poverty status, health insurance, marital status, body mass index, current smoking, alcohol use, and region.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: National Institute on Minority Health and Health Disparities, 5U54MD006882-10; National Institutes of Health, 1OT2OD032581-01 and National Institute of General Medical Sciences, 5U54GM104942-07.