
Abstract
Background
The majority of children who survive a brain tumor suffer from late effects. Physical activity can have a positive impact on physical fitness and mitigate late effects. Despite this, survivors are less physically active than their peers. The aim of the study was to explore healthcare staff's experiences of promoting physical activity for these children.
Method
A qualitative design was used with semi-structured online focus group interviews with 24 experienced healthcare staff from all of Sweden's pediatric oncology centers. The interviews were analyzed with inductive content analysis.
Results
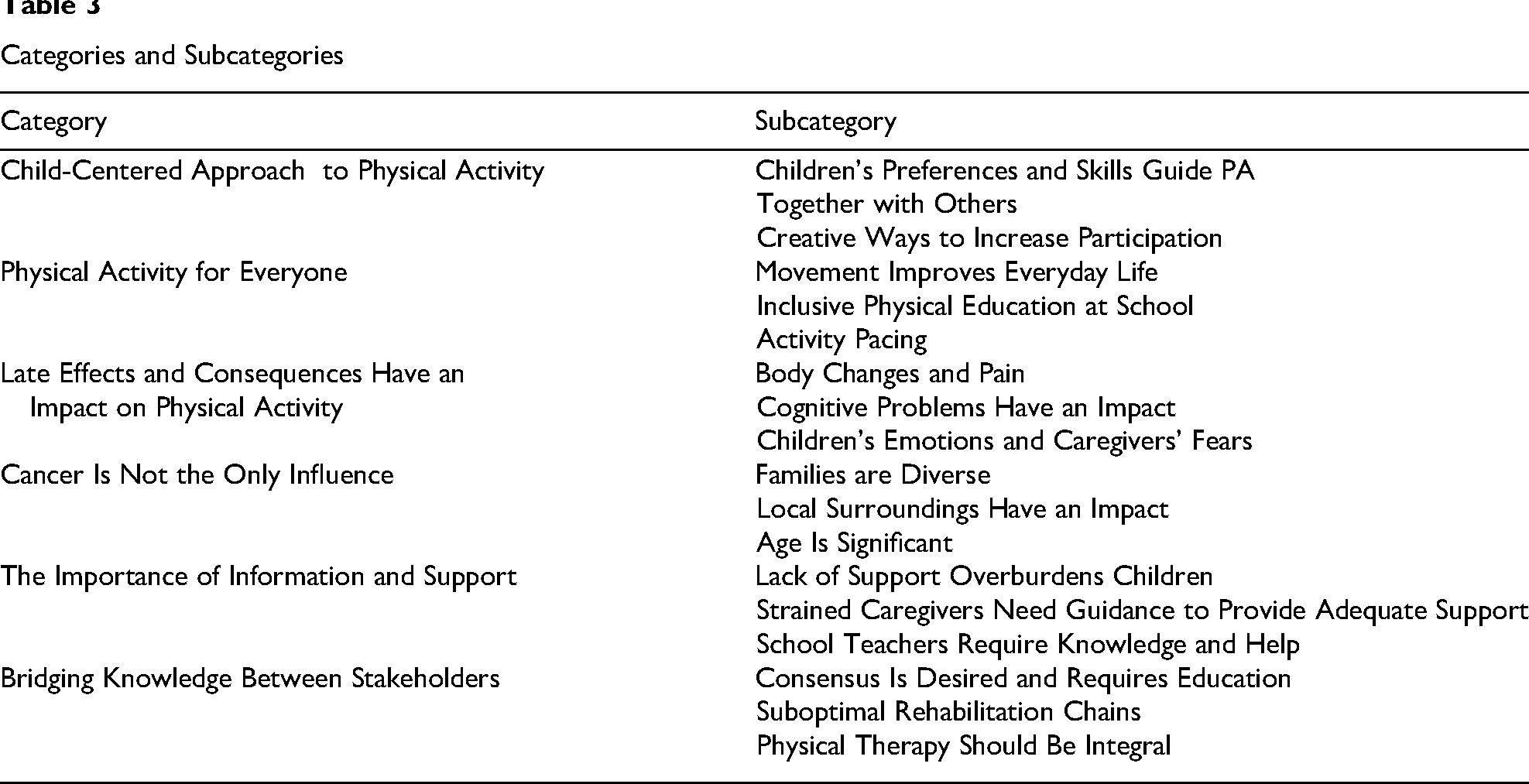
Six main categories were identified: (a) child-centered approach to physical activity; (b) physical activity is for everyone; (c) late effects and consequences have an impact on physical activity; (d) cancer is not the only influence; (e) the importance of information and support; and (f) bridging knowledge between stakeholders.
Discussion
The healthcare staff discussed the complexity of late effects, in particular fatigue, as a barrier to physical activity. The social component of doing activities together with peers was highlighted, and group activities were suggested. The value of involving children in decision-making and letting them choose a fun activity was stressed. In conclusion, the health care staff emphasized that physical activity interventions for children who survived a brain tumor should be joyful, individually tailored, and child-centered to enhance motivation and adherence. However, less significance was put on the amount of physical activity necessary to improve physical fitness.
Introduction
Children who survive brain tumors often suffer from impairments due to the tumor itself and treatments (Krull et al., 2018; Nicklin et al., 2019). Common treatments for brain tumors can potentially cause acute and late side effects, some of which appear and worsen years after treatment ends and can potentially become lifelong (Bhakta et al., 2017; Roddy & Mueller, 2016). Childhood brain tumor survivors have the highest risk of profound late effects among all childhood cancer survivors (Otth et al., 2022; Roddy & Mueller, 2016), such as cognitive impairment, cancer-related fatigue, depressive symptoms (Brinkman et al., 2016; Cheung et al., 2019; Pancaldi et al., 2023; Robinson et al., 2010; van Deuren et al., 2020), physical impairments such as impaired balance (Piscione et al., 2014; Varedi et al., 2021), endocrine and metabolic issues, cardiovascular diseases, and stroke (Gunn et al., 2015; Gupta & Jalali, 2017; King et al., 2017; Sun et al., 2020).
Childhood cancer survivors show low physical activity (PA) and high levels of sedentary behavior (Götte et al., 2023; Roussenq et al., 2022), which makes this a main target for rehabilitation from cancer to return to an active everyday life. Increased PA is associated with less cancer-related fatigue (Van Dijk-Lokkart et al., 2019) and may improve cognitive function (Bernal et al., 2023), motor function, cardiovascular health (Sharma et al., 2021; Wogksch et al., 2021), and bone mineral density (Rapti et al., 2023).
The World Health Organization (WHO) recommends that all children aged 5-17 should engage in at least an average of 60 minutes per day of moderate-to-vigorous intensity (mostly aerobic) PA, across the week. Three days per week, vigorous-intensity aerobic activities, as well as muscle- and bone-strengthening activities, should be incorporated. Reducing sedentary time, especially recreational screen time, is also recommended. PA and reducing sedentary time are important, even for children who have survived cancer. It is advised to begin at each child's individual level of PA and gradually increase the frequency, intensity, and duration over time (WHO, 2020). The International Pediatric Oncology Exercise Guidelines published in 2021 recommend PA as a safe and beneficial practice for children with cancer and survivors (Wurz et al., 2021). Nevertheless, PA may be limited by sequelae of cancer and its treatment (Antwi et al., 2019).
There is a scarcity of studies on which factors may hinder and promote PA for children who have survived a brain tumor, and these factors may differ from those associated with other cancer diagnoses. Healthcare staff within pediatric oncology have unique insights into and experience of the practical challenges and enablers of encouraging PA. Identifying, understanding, and addressing these challenges and areas for improvement provides prospects for creating effective PA interventions. The study aimed to explore healthcare staff's experiences of promoting and encouraging children who have survived a brain tumor to be physically active after completing active medical treatment.
Method
Design
The study used a qualitative design, collected data via group interviews, and adhered to the Consolidated Criteria for Reporting Qualitative Research (COREQ Tong et al., 2007).
Setting, Recruitment, and Participants
There are six pediatric oncology centers in Sweden; each center has consultant nurses for children with brain tumors who will keep in contact with the child and family during and after the completion of medical treatment. Their role is to provide continuity and support for families. They raise concerns and identify children and families who require additional support for different concerns, including PA challenges. The consultant nurse is a vital link between families, healthcare, and schools. Other oncology center staff include oncologists, psychologists, physical therapists (PTs), occupational therapists, dietitians, and hospital educators.
The inclusion criteria were healthcare staff with experience of working with children with brain tumors and encouraging PA. Participants were recruited through convenience sampling (Leedy & Ormrod, 2013). An invitation email was sent to 53 healthcare staff from all of Sweden's six oncology centers, four rehabilitation centers, and five local hospitals. Twelve did not reply, and 13 declined participation because they did not fulfill the inclusion criteria. Primary consent was obtained from 28 healthcare staff with various occupations (to achieve diverse perspectives); however, due to time constraints, four later rejected participation. Sweden is a small country with approximately 10 million inhabitants. Consequently, Sweden's oncology field is limited, and some of the participants had been briefly encountered by the researchers in other contexts. For details on the 24 participants, see Table 1.
Demographic Information of Participants (N = 24)
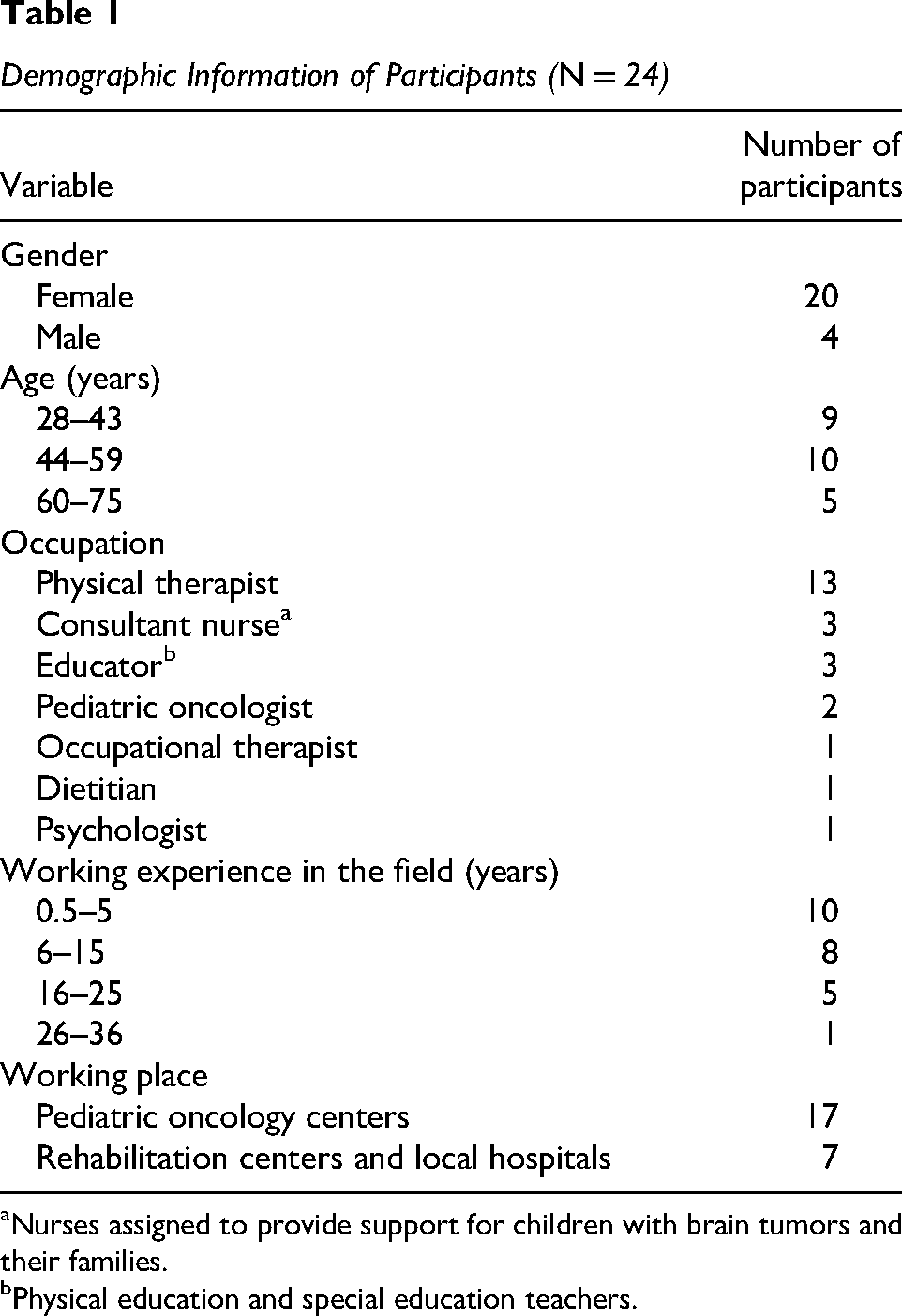
Nurses assigned to provide support for children with brain tumors and their families.
Physical education and special education teachers.
Data Collection
A semi-structured interview guide (see Supplemental File 1) with open-ended questions (developed by Å.P.D., S.F.-H., and H.I.) was used. The interview guide was pilot-tested with two healthcare professionals, and questions were raised about the definition of PA. A clear definition of PA was therefore provided during focus group interviews. The definition used for PA was all bodily movement that increases the heart rate, including play and daily activities, that is, not necessarily sports activities. The data obtained from the pilot-tested interviews were not included in the analysis.
The interview focused on participants’ experiences of encouraging PA for children who have had a brain tumor and perceptions about challenging and facilitating factors for being physically active, with an emphasis on the time after the end of active medical treatment when the child had returned home to their everyday life. Participants were asked to think freely and give suggestions for interventions to increase PA for these children. Five focus group interviews took place from May to June 2023, involving a total of 24 participants, with group sizes ranging from three to seven. The average duration of the interviews was 60 min. The focus group interviews were recorded using the digital platform Zoom. Å.P.D. moderated, while S.F.-H. assisted and took field notes. Ground rules were communicated, and participants were asked to respect each other's views and speak one at a time (Krueger & Casey, 2015). They were also requested not to name or give specific information about children in a way that could reveal their identities. Some participants may be less vocal in focus group interviews, affecting data collection. To address this, the moderator and assistant encouraged active contributions from all participants. The interviews were conducted in Swedish.
Data Analysis
The interviews were transcribed verbatim. Consistency between transcripts and audio recordings was checked, audio files were listened to, and the transcripts were read several times. Data were analyzed using qualitative content analysis, following the methodology described by Graneheim et al. (2017), Graneheim and Lundman (2004), and Lindgren et al. (2020). The process started by extracting meaning units of analytic relevance for the study's aim. This was done independently by Å.P.D. and S.F.-H., and meaning units were compared. The text was then condensed without changing the core content. The meaning units were then labeled with codes by Å.P.D., with guidance from S.F.-H. The codes with similar characteristics were grouped into subcategories, and subcategories with similar underlying content formed categories. The process was not linear; it moved back and forth within the text, modifying subcategories and categories until an enhanced level of interpretation was reached (Å.P.D., S.F.-H., and H.I.). In the final step, the analysis was discussed among all the authors and refined until consensus on categorization was reached. Reflexivity was a continuous process throughout the study. The researchers were critically reflecting on their roles, preconceptions, and potential impact on data collection, analysis, and interpretation.
Å.P.D. is a PhD student and a PT with clinical experience of working with children with brain tumors and has received formal training in qualitative research. S.F.-H. is a PT with a specialization in pediatric physical therapy; H.I. is a PT in cancer rehabilitation; G.L. is a pediatric oncologist; and PÅ is a PT with extensive knowledge of behavioral medicine. All co-authors have extensive knowledge and experience in qualitative methodology. Examples of analysis are shown in Table 2, and to strengthen analysis, illustrative quotations are presented in the results section (Graneheim et al., 2017; Graneheim & Lundman, 2004). A professional English language editor translated the quotations into English to prevent misinterpretations, and Grammarly has been used for language polishing.
Examples of the Analytical Process
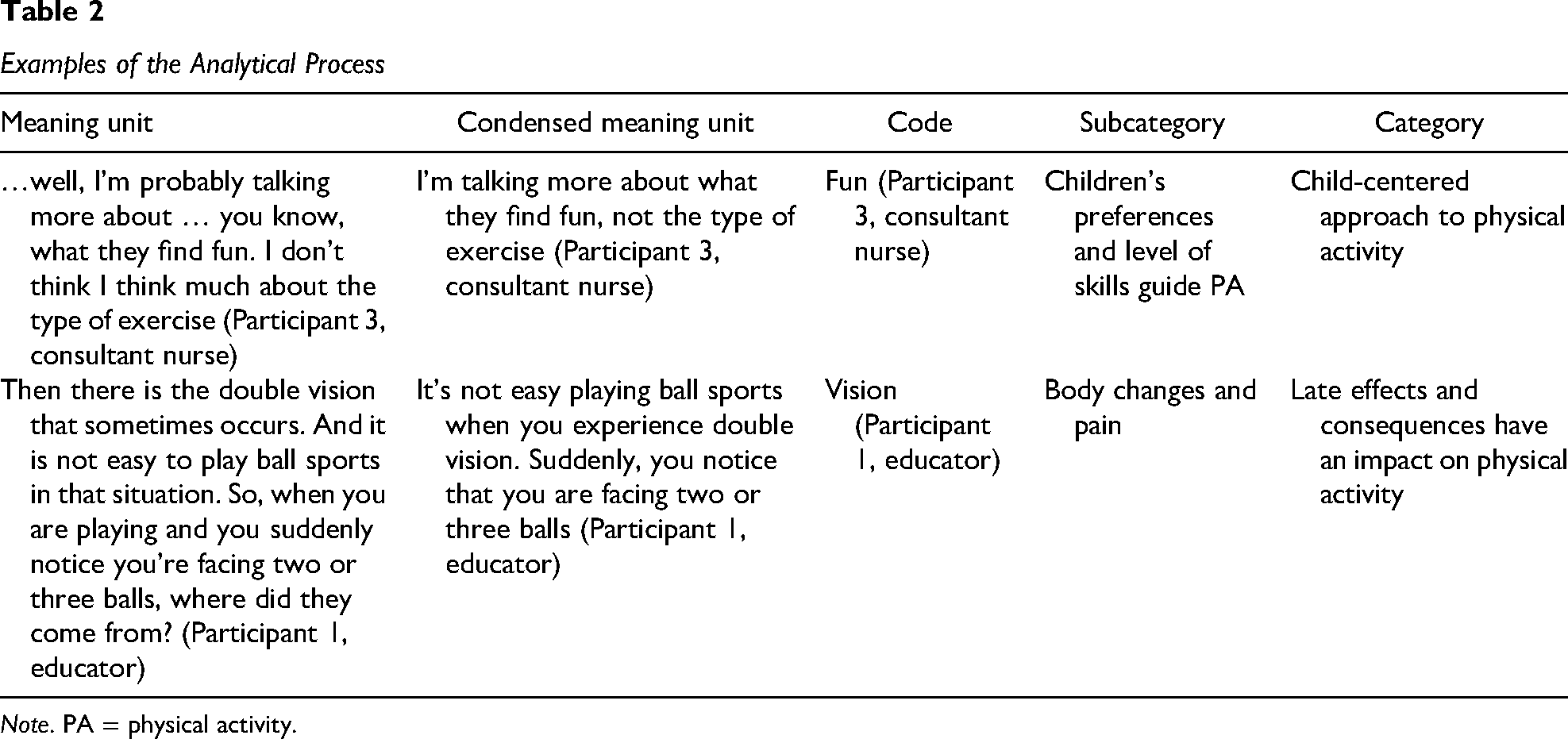
Note. PA = physical activity.
Ethics
The participants received oral and written study information, including the voluntary nature of the study and their right to withdraw without any further obligation, information about legal rights according to the EU's General Data Protection Regulation 2016/679 (Regulation 2016/679, 2016), and an assurance of confidentiality when presenting the results. Written consent was obtained from participants prior to the interviews, and additional verbal consent was obtained immediately before the audio recording began. A positive advisory opinion was given by the Swedish Ethical Review Authority (Dnr 2023-01585-01).
Results
Categories and Subcategories
Child-Centered Approach to Physical Activity
Participants emphasized the importance of a child-centered approach to PA, where children feel capable, are involved in decision-making, and can have fun. The category includes three subcategories: Children's Preferences and Skills Guide PA, Together With Others, and Creative Ways to Increase Participation.
Children's Preferences and Skills Guide PA
Focusing on children's interests when recommending PA has great value, as the most important thing is the child's own enjoyment. Participants expressed that children's age, motor skills, balance, and fatigue could influence recommendations for PA. They agreed that it was challenging to find and recommend activities that elevate the heart rate, especially in the event of impaired balance and fatigue. Involving children in decision-making and letting them list fun activities that they enjoyed was proposed: “Let the child be involved in decision-making themselves, build on what brings them joy” (Participant 2, consultant nurse). Encouraging them to explore new activities was also mentioned: “I recommend physical activities that the child is interested in. That's the most important thing. If the child has no interests, we try to find one” (Participant 4, PT).
Together With Others
The participants emphasized the benefits of involving peers; enjoyable activities in a group may increase motivation and the likelihood of adhering to PA: “It's easier to feel motivated to get going, and harder to say no, when you’re a part of a group” (Participant 12, PT). Group training with children with similar difficulties (but not necessarily with a cancer diagnosis) was suggested. Online groups were also mentioned as an option. Classmates and school activities were noted as one way to increase PA: “It is possible to encourage children to become more physically active and engaged through various school activities” (Participant 2, consultant nurse). The participants emphasized that group activities foster social interactions: “If you exercise with someone else, it's easier to get going, and it can have spin-off effects for other things as well. They have missed out so much on their social development, and they need to practice social skills” (Participant 6, psychologist).
Creative Ways to Increase Participation
The participants provided innovative ideas for promoting PA. Camps offering education about and opportunities to try out different types of PA and social interactions were recommended. Therapy dogs and horseback riding in groups were proposed as a fun way to be active: “Care dogs, therapy dogs, and horses. Pets and animals are generally beneficial. It doesn’t suit everyone, but it adds several dimensions” (Participant 3, consultant nurse). The participants pointed out how role models, social media, and influencers could motivate children. Involvement and support for the whole family to engage in PA were emphasized: “Family interventions. Screen out families that are inactive and find enjoyable physical activities for them to participate in together…” (Participant 2, consultant nurse).
Physical Activity for Everyone
The category includes three subcategories: Movement Improves Everyday Life, Inclusive Physical Education at School, and Activity Pacing. The participants stated that PA should be for every child, including those with cancer, and highlighted the many benefits of being active. They stressed the importance of establishing routines for everyday movement, pointed out how physical education (PE) could be challenging at school, and mentioned the relevance of activity pacing to make energy last throughout the day.
Movement Improves Everyday Life
Participants emphasized that “every movement counts” and that PA has physical, psychological, cognitive, and social benefits. It does not have to be a sports activity, and being outdoors benefits spontaneous movement. Early attention to regular PA after cancer may offer signals of hope for the future, and participants stressed the importance of its integration into daily life: “I believe in addressing it [physical activity] early, right from the onset of illness. (…) It's about looking ahead and giving the child hope through training, that it is rehabilitation right from the start” (Participant 3, consultant nurse). Another frequently discussed topic was reducing sedentary screen time: “Getting back to everyday habits and routines is crucial, so sometimes I just want to throw away their iPad…” (Participant 6, psychologist).
Inclusive Physical Education at School
Children in need of special care have the legal right to receive reasonable accommodations at school in all subjects, and the participants noted a scarcity of such accommodations in PE for cancer survivors. Adapting to cognitive and physical impairments, modifying the environment, and providing tailored instructions can be challenging for teachers. The Swedish Education Act allows for exceptions in grading due to disability, providing children with a chance to pass PE even if they cannot fully participate in, for example, the mandatory 200-m swimming test. Some participants viewed the exception clause as positive, while others raised concerns: “The special provision can be misused. It can be a hindrance to physical activity. Instead of the teacher adapting the physical activity, the student might end up … sitting on the bench…” (Participant 4, PT). Positive examples of when PE worked well were also discussed: “When things have gone well in physical education at school, it's because there has been an emphasis on always having alternative activities available in the gym hall. This has made the child want to participate” (Participant 15, educator).
Activity Pacing
Participants highlighted the possibility of using PA as an energy boost at school, but limited energy must always be taken into consideration: “You need to look at the whole picture, not just the physical activity, but also include other aspects as well, to ensure that there is enough energy for everything needed throughout the day” (Participant 2, consultant nurse). They mentioned activity pacing, emphasizing the importance of alternating between activity and rest throughout the day. They suggested that having an activity schedule might help maintain endurance and prioritize putting energy into the right things: “brief activities with breaks in between so that they can cope with the entire day, rather than ‘putting the pedal to the metal’ in the morning and then feeling drained for the rest of the day and the evening” (Participant 12, PT).
Late Effects and Consequences Have an Impact on Physical Activity
According to the participants, sequelae and late effects affect children's PA levels and sedentary behavior and have an impact on daily life, school, and self-perception. The consequences are not restricted to the child alone; the new situation also affects the caregivers. The category includes three subcategories: Body Changes and Pain, Cognitive Problems Have an Impact, and Children's Emotions and Caregivers’ Fears.
Body Changes and Pain
Children's decreased physical functions, affected neurological function, motor skills, vision, and body changes were discussed as barriers to PA: “Impaired balance and coordination make it difficult to be physically active” (Participant 2, consultant nurse). The changed body is another challenge, “It's quite common for teenagers to find it challenging to exercise. They feel, ‘This isn’t my body because it's different now’” (Participant 21, PT). Participants discussed how pain could be both a late effect and a consequence of inactivity and how pain could hinder PA and contribute to fatigue: “Most I have met have various pain conditions in their bodies, either as a result of treatment and medication, but also simply because they are inactive” (Participant 20, PT). Inactivity leads to reduced cardiorespiratory fitness and low stamina, further complicating PA: “It's a prolonged fatigue resembling poor cardiorespiratory fitness. It's not just weak legs; the overall fitness level is low” (Participant 4, PT).
Cognitive Problems Have an Impact
The mental fatigue of not having enough energy to last through the day was described as affecting the child's life and contributing to a lower PA level: “Tiredness and fatigue contribute to sedentary behavior” (Participant 2, consultant nurse); “And above all, cognitive difficulties make it hard to keep up with social interactions or with friends. It's more exhausting and harder; all of this contributes to more sedentary behavior” (Participant 3, consultant nurse). Struggling with academic skills, interpreting social interaction, and lost initiative and drive might lead to falling out of social context and abandoning previously enjoyed activities: “Many quit their team or their activity and end up socially excluded” (Participant 4, PT).
Children's Emotions and Caregivers’ Fears
The participants raised concerns about the children's emotional well-being, expressing worries about changed self-image and identifying as ill, even years after treatment. Challenges related to appearance may affect PA levels: “Their appearance can also pose challenges; they might not find it as easy to go to public places … such as swimming pools or take part in those kinds of [activities]” (Participant 21, PT). One oncologist mentioned, “The questions I get are ‘What am I not allowed to do?’ instead of ‘What am I allowed to do?’ So, for me, it's about reducing anxiety; you are not made of glass” (Participant 11, oncologist). Participants also described how caregivers could, with good intentions, react with overprotectiveness due to anxiety about their child falling and getting hurt: Parents might fear letting their child be active because they are worried they might fall, hit their heads, or hurt themselves. Even if it has been a year or a couple of years since surgery and everything looks healed, I find that for some there is a barrier, that they prevent the child from moving around freely. (Participant 5, PT)
Cancer Is Not the Only Influence
Factors such as family, environment, and age greatly affect children's activity levels. The category includes three subcategories: Families Are Diverse, Local Surroundings Have an Impact, and Age Is Significant.
Families Are Diverse
Culture, family habits, and routines have a significant impact on children's PA levels, according to the participants. Families may develop a habit of inactivity during treatment. Also, knowledge about and attitudes to PA differ between families: “…this is quite simply a family matter as well. It depends on the family they grow up in, their habits, and how things are. And it's not that easy. Unfortunately, not all families are particularly physically active…” (Participant 15, educator). The participants described how caregivers expressed feelings of loneliness and struggle when seeking support and help for their child's PA. They noted a risk of unequal access to support for PA due to families’ varying ability to assert themselves: If we are to provide equitable care, we need to be there for those who cannot manage this on their own. But even the strong ones [parents] have been very critical about feeling that they’ve been alone in this and have to seek [help with physical activity] themselves … which is challenging for them … they would have needed, like, a coach/support to help them incorporate it into daily life. (Participant 6, psychologist)
Local Surroundings Have an Impact
The surrounding environment also has an impact on the child's PA. Larger cities offer more accessible and diverse PA activities and rehabilitation services: “Where you live affects the options [for activities]” (Participant 24, PT). The children's circumstances at school can also vary; at some schools, PE could be reduced or removed in favor of other subjects: “So, then we think, if we get rid of PE, then they will have the energy to participate a bit in lessons” (Participant 7, PT).
Age Is Significant
Participants described how age could have an impact on PA. Younger children tend to be more active and might still play in the schoolyard, whereas older children are less active: “Younger children may find it easier to return to physical activity because they naturally play in a different way; the schoolyard play is still there” (Participant 22, educator). Additionally, children who attend sports clubs might have increased expectations placed on them with age: “The older you get, the harder it is to stay in the club; the training is tougher … Have you had [a brain tumor] and not optimal balance and stamina? Yes, then it's difficult to remain in that world” (Participant 13, PT).
The Importance of Information and Support
The participants stressed a substantial need for information and support for children, caregivers, and school teachers, which could have an impact on children's PA levels. The category includes three subcategories: Lack of Support Overburdens Children, Strained Caregivers Need Guidance to Provide Adequate Support, and School Teachers Require Knowledge and Help.
Lack of Support Overburdens Children
The participants agreed that children lack structured support in rehabilitation, school, and free time and that a heavy burden of responsibility rested on the children themselves: “One major challenge is that a great deal of responsibility is placed on the children and teenagers themselves. That there is a lack of help and support. We don’t really have any structured support” (Participant 21, PT). Support in PA was regarded as integral to addressing children's questions; it also reduces fear and anxiety, empowering them to understand their capability to move without harm. Children alone cannot be responsible for being active: “There's a need for some kind of coach, a fitness coach or a PT. You can’t just put a [training program] in someone's lap … that's not enough … it won’t happen” (Participant 6, psychologist).
Strained Caregivers Need Guidance to Provide Adequate Support
The participants described how caregivers often experience exhaustion after the child's period of illness. Parents are tired and drained, and struggle to support and place reasonable demands on their children: “The parents we see at the follow-up clinics often actually crash after the treatment. They don’t feel well afterwards, many of them are on sick leave, they can’t cope” (Participant 17, oncologist). The participants expressed the need for support for adults in order to empower them to support their children: “Parental support can help children become more physically active. It's an extremely challenging situation for all families, especially for those where there might be some shortcomings” (Participant 4, PT).
School Teachers Require Knowledge and Help
The participants acknowledged that teachers, especially PE teachers, are unsupported by healthcare systems when it comes to PA for children who have had a brain tumor: “…support in how … physical education teachers, in how they can adapt physical education. It can also be hard to know what is needed to do it well” (Participant 22, educator).
Teachers want support, and one approach discussed was to have specially trained PE teachers or to have PTs at the school: “I think it would be beneficial to have a contact person, such as a PT, within the student health services…” (Participant 23, PT).
Bridging Knowledge Between Stakeholders
Shared fundamental knowledge within the care system about the benefits of PA and the urgency of an improved rehabilitation chain with follow-ups was seen as crucial. The category includes three subcategories: Consensus Is Desired and Requires Education, Suboptimal Rehabilitation Chains, and Physical Therapy Should Be Integral.
Consensus Is Desired and Requires Education
Participants expressed that healthcare staff's limited knowledge requires continuous education through training sessions, online courses, and written materials on the benefits of PA. Consensus on PA recommendations was stressed, as well as having the doctor endorse the message: “To have a consensus and convey the same message across all healthcare professionals is useful. … Sometimes it could be … uncertainty. … That the doctor explicitly expresses that physical activity is good” (Participant 23, PT). The importance of documenting that PA is encouraged in the medical record was also discussed to promote consistency among staff: “I don’t feel very confident about what I can encourage freely, especially if there are doubts from the parents. So, I would appreciate it if there was a note in the medical records stating that this is encouraged” (Participant 16, dietitian).
The discussion also emphasized the importance of consensus on the content of information materials about PA. However, it was noted that there was a shortage of such materials to provide to families: “I don’t have any information material to hand out. We tell people to be physically active, but we don’t specify how much. Healthcare providers need to clarify this; it feels like a responsibility we have” (Participant 18, consultant nurse).
Suboptimal Rehabilitation Chains
The participants emphasized that PA should be a central and natural part of the entire rehabilitation process, beginning with the hospital diagnosis and continuing into school, including goals and follow-ups regarding PA: They come once a year for check-ups (…) we don’t have any rehabilitation plans in which goals and sub-goals and so on are set for physical activity. … So, this … might perhaps encourage them to be more active, too. If goals and sub-goals were set and followed up on. (Participant 2, consultant nurse)
They highlighted that communication between different stakeholders was crucial and that there was room for improvement. Knowledge needs to be shared so that the next care provider feels confident and secure about what to recommend: It’s important that the transitions are more seamless. We have tried to clarify and improve communication so that the rehab chain can start early. The more knowledge and information you get, the more confident you become in supporting the families. (Participant 19, PT)
Physical Therapy Should Be Integral
PTs are not always integral to the oncology team, which was considered substandard. Participants emphasized the importance of PTs in terms of providing age-appropriate activities and gradually increasing PA. Follow-up clinics often lack PTs, resulting in more general questions about PA from doctors or nurses. One of the consultant nurses said, “I feel that we don’t talk much about physical activity. It's just on a surface level, like a checklist during the visit. ‘Do you engage in any physical activity?’ We don’t delve into the details” (Participant 18, consultant nurse). Another consultant nurse said, “I generally encourage physical activity. When it comes to more specific details about types of exercise and so on, I believe that's something PTs and occupational therapists do, as they have the expertise” (Participant 2, consultant nurse). Across all focus groups, the importance of physical therapy was discussed.
Discussion
When the participants discussed PA promotion for children who have had a brain tumor, they stressed that early attention to PA should begin upon diagnosis, right from the onset, as it represents wellness and signals hope for the future. The importance of listening to, and involving, children in decision-making processes was highlighted. This helps empower children, ensure their voices are heard and considered, and foster a sense of control and agency. This aspect is crucial from an ethical standpoint and is supported by Article 12 of the United Nations Convention on the Rights of the Child. Children have the right to express their views on all issues affecting them. Their opinions should be considered with regard to their age and maturity (United Nations, 1989). Participants accentuated that children's motivation and adherence to daily PA could be increased when the activity is fun and ideally done together with peers to encourage social interactions. They also described the value of allowing children to choose a PA they enjoy, letting them list activities, and supporting them in exploring different activities. The enjoyment factor has been highlighted as a significant facilitator for participating in PA among children with disabilities (Rosenbaum & Gorter, 2012; Rosenbaum, 2022), among childhood cancer survivors (Mizrahi et al., 2020), and among children in general (Bajamal et al., 2024; Biddle et al., 2011). Many of the experiences from the participants harmonize with theories that describe psychological processes and motivation, such as Bandura's social cognitive theory (SCT; Bandura, 1977, 1986) and Deci and Ryan's self-determination theory (SDT) (Deci & Ryan, 1980, 2000). SCT emphasizes how individuals learn through observing, imitating, and modeling others’ behavior and emotions within a social context. A central concept in this theory is self-efficacy, the belief in one's ability to succeed with a specific task, which in turn affects one's motivation (Bandura, 1997). SDT emphasizes three fundamental needs for motivation and well-being: autonomy, competence, and relatedness (Ryan & Deci, 2000). When children feel they belong and are supported by others, feeling relatedness, their motivation to participate in PA increases (Ryan & Deci, 2000), while empowering children to make choices supports their autonomy and intrinsic motivation (Deci & Ryan, 1980). Thus, tailored challenges and adaptations to current skill levels can help children succeed and feel more competent and included, thereby boosting their intrinsic motivation (Ryan & Deci, 2020). This approach also relates to Bandura's principle of mastery experiences, where successful completion of a task strengthens self-efficacy and makes individuals more likely to attempt future challenges (Bandura, 1997).
The participants expressed that many children face social challenges, experience feelings of exclusion, and struggle with social interactions. This is consistent with previous studies of children after brain tumors (Aalykkja et al., 2023; Schulte et al., 2019). Social support from friends has been shown to positively predict PA for children in the general population (Hu et al., 2021) and for children during and after cancer treatment (Kappelmann et al., 2023). When the participants were encouraged to suggest ways to promote more engaging PA, they recommended group activities, educational and activity camps, and family-based interventions. In a systematic review of camps for childhood cancer survivors and their families, all articles reported positive outcomes in facilitating social skills, self-esteem, and PA levels (Kelada et al., 2020). This supports the benefit of engaging in PA activities with others, which aligns with previous research (Adamovich et al., 2024). The participants also suggested outdoor activities, as they had noted that children are often more physically active outdoors, an experience that aligns with a previous study showing that cancer survivors exercised at a higher intensity outdoors than indoors (Miller et al., 2021).
The participants repeatedly mentioned the magnitude of late effects (e.g., fatigue, cognitive problems, pain, and motor and balance impairments) and the impact on PA levels, sedentary behavior, and family and social matters that could occur and persist years after treatment. Previous studies have also reported these challenges (Antwi et al., 2019; Gupta & Jalali, 2017; Larsen et al., 2023). Interestingly, participants highlighted that pain could be a hindrance to PA but, at the same time, that inactivity could lead to pain and that pain and fatigue were often interconnected. This illustrates the complexity of symptoms. In a review of long-term cancer survivors, pain was associated with brain tumor survivors, female gender, and fatigue (Reinfjell & Zeltzer, 2020). The participants also noted that children may experience pain in multiple areas of the body, not just headaches, which is consistent with prior research on adolescents and young adult brain tumor survivors (Recklitis et al., 2019).
Moreover, participants discussed how body image can affect children's PA behavior. Weight gain and perceiving one's body as overweight are associated with being less physically active among adolescents in the general population (Karchynskaya et al., 2022) and among childhood cancer survivors (Larsen et al., 2023). Adolescent girls who have survived a brain tumor are particularly at risk of negative body image concerns (Belle et al., 2022). Challenges related to body image, cognitive impairments, pain, and fatigue are all crucial to consider. It is not only motor and balance issues that need to be accounted for when deciding what type of support and PA the child needs. The main barrier to PA participation was considered to be fatigue, which aligns with previous studies (Adamovich et al., 2024; Larsen et al., 2023; Mizrahi et al., 2020). Interestingly, participants noted that poor cardiorespiratory fitness can sometimes resemble fatigue. This suggests a need for more education about the concept of fatigue and highlighting its multifaceted nature. Cardiorespiratory fitness is an essential marker of physical and mental health in youth (Raghuveer et al., 2020). It refers to the efficiency of the circulatory and respiratory systems in supplying oxygen to muscles during PA and for muscles to use that oxygen for energy production (Armstrong, 2019). PA with elevated heart rate is crucial for improving cardiorespiratory fitness (Cao et al., 2019). Participants described this as challenging to identify and recommend activities that raise the heart rate. However, they simultaneously raised concerns that the children might become fatigued by doing PA that is too intense. This has also been described in a study of PA-promoting behavior among healthcare staff, in which staff mainly recommend mild to moderate PA due to concerns about overexertion (Haussmann et al., 2018).
The participants mentioned the concept of activity pacing, which involves drawing up a schedule that regulates and alternates activity and rest throughout the day to conserve energy (Antcliff et al., 2017; Nielson et al., 2013). Prior research on children with cancer and survivors has addressed similar strategies (Larsen et al., 2022; L’Hotta et al., 2023). Activity pacing might definitely be beneficial, but it is worth discussing which activities to choose during the day. At school, it might be tempting to prioritize theoretical classes and skip PE. However, childhood cancer survivors and their caregivers have reported PA at school to be highly valued and that PA with peers gave a sense of belonging. PE teachers’ attitudes were seen as essential for survivors’ ability to participate in PE (Larsen et al., 2023). The challenge of inclusive adaptations in PE versus limited resources was discussed by the participants, who noted that there may be insufficient support at schools for children with special needs. The challenges and consequences of late effects, such as fatigue and cognitive issues, are so significant that they might overshadow the importance of muscle- and bone-strengthening activities and disregard the relevance of cardiorespiratory fitness.
Prior research has addressed caregivers’ distress related to their child's disabilities and chronic health conditions following a brain tumor (Buchbinder et al., 2017). The participants emphasized the importance of supporting strained, overwhelmed caregivers to empower them to support their children. One thing caregivers need is adequate information about the misconceptions that PA could worsen fatigue (Cheung et al., 2021; Larsen et al., 2023), all in order to avoid well-intentioned limitations on a child's activity. Previous research has also highlighted the issue of fear of injury as a barrier to PA (Cheung et al., 2021; Ross et al., 2018). These misconceptions and fears are troublesome, as PA has been shown to potentially mitigate symptoms such as fatigue (Rapti et al., 2023). Therefore, there is a great need for education and information about fatigue and PA, not only for the child and the family but also for schools (Jess et al., 2023).
Furthermore, the participants described how habits, routines, lifestyles, support, and knowledge about PA differ among families, which also aligns with previous research (Shabanian et al., 2023). Participants highlighted a potential risk of unequal rehabilitation based on families’ assertiveness and varying abilities to seek help. Caregivers influence children's PA behavior through role modeling and support (Bandura, 1986; Su et al., 2022). The participants described how families could develop sedentary behavior, whereby children were stuck in a habit of excessive screen time from the time when they were ill. A recent study on childhood cancer survivors who were now adults found that their PA levels were still influenced by their family habits, role models, and social support during childhood (Jess et al., 2023). This supports the importance of family-centered care for children with cancer.
In the present study, as in previous studies (Haussmann et al., 2018; Shabanian et al., 2023), healthcare staff expressed a lack of in-depth knowledge about PA for survivors. They wanted more education regarding PA, both for themselves and for other healthcare staff who come into contact with these children. They suggested additional PA information, lectures, training sessions, and written materials. The participants emphasized the importance of PTs who can provide and prescribe tailored PA for children who have had a brain tumor based on individuals’ abilities and interests.
Communication between healthcare, families, and schools is also something crucial (Grandinette, 2014; Jess et al., 2023; Young et al., 2022). Within the Swedish care system, consultant nurses play a key role as they provide information and support in the child's school. They can refer to another profession, that is, PTs, who can give more tailored advice for schools regarding PA. School is a major and important part of children's daily lives and can serve as a platform for increased PA. Improved interdisciplinary collaboration could be beneficial for PA to become a given part of the rehabilitation of children after brain tumor; however, the forms for that need to be developed and evaluated in future studies.
The recurrent theme in all focus group interviews for this study was the emphasis on enjoyable and social activities. However, a sole focus on enjoyment may lead to missed opportunities to improve cardiorespiratory fitness, muscle strength, and bone health, as well as the potential to reduce fatigue through PA. These beneficial effects of PA might not have been adequately disseminated to children who have had a brain tumor, their caregivers, healthcare providers, schools, and other stakeholders. Combining enjoyment and PA components, along with social aspects, is both feasible and essential for achieving optimal outcomes in interventions.
Strengths and Limitations
The study's primary strength was the participation of experienced healthcare staff from all childhood oncology centers in Sweden. Online focus groups remove geographical distances. In focus groups, new perspectives that might otherwise have been latent in one-to-one interviews can appear (Katz-Buonincontro & Nezu, 2022). The group size ranged from three to seven participants, based on recommendations for online focus groups (Krueger & Casey, 2015), as moderating larger groups online can be more challenging (Katz-Buonincontro & Nezu, 2022). The semi-structured interview questions were pilot-tested to verify clarity (Krueger & Casey, 2015); this proved valuable, as a description of the term “physical activity” was requested. COREQ was followed to achieve transparent and rigorous reporting, enhancing the study's credibility, reproducibility, and overall quality (Tong et al., 2007). Participants did not review transcribed interviews, which may have compromised accuracy (Birt et al., 2016). Modifying or removing statements from one participant in a focus group can impact the entire outcome, as others react to and build on what has been discussed. Therefore, participant validation was not utilized in this study. To enable the reader to make transferability judgments (Lincoln & Guba, 1985), the healthcare staff's background and context are described, balancing the risk of disclosure of participants’ identity, given that Sweden's pediatric oncology field is small. The majority of participants were PTs, probably due to the inclusion criterion that required experience in encouragement of PA. This could have restricted the variety of perspectives and may also partly limit transferability to other professions. However, regardless of the profession and experiences, there was a great agreement on PA in the focus group discussions.
The analysis was conducted inductively, following the methodology described by Graneheim et al. (2017), Graneheim and Lundman (2004), and Lindgren et al. (2020). This method was chosen to ensure an openness to the empirical data and to reduce the risk of preconceived interpretations and biases. Investigator triangulation (Polit & Beck, 2013) was used to reach a consensus during the analysis.
Conclusion
The healthcare staff acknowledged that PA interventions for children who have survived a brain tumor should be fun, individually tailored, and child-centered to enhance motivation and adherence. The benefits of group activities and family-centered interventions were highlighted. Less focus was placed on the PA's intensity and frequency necessary for improving cardiorespiratory fitness and physical function. When developing PA interventions, these findings are crucial to consider. Interventions should incorporate both physical and social aspects to achieve optimal outcomes.
Clinical Implications
Healthcare staff need comprehensive education in PA to provide individualized, evidence-based recommendations for children who have had a brain tumor. This education should address PA's physical, psychological, cognitive, and social aspects, as well as strategies to motivate PA and address barriers. Interventions should incorporate activities that elevate heart rate, strengthen muscles and bone, and are enjoyable, ideally with social engagement. It is essential to start at the child's current level and gradually increase the amount and intensity of PA. Inactivity is often a family matter, where family interventions with education and support are needed to encourage PA. Attention should be given to effective communication and coordination among stakeholders in order to facilitate and support the child's PA.
Supplemental Material
sj-docx-1-jpo-10.1177_27527530251356250 - Supplemental material for Fun Leads the Way—Healthcare Staff's Experiences of Promoting Physical Activity Among Children Who Survived a Brain Tumor: A Qualitative Study
Supplemental material, sj-docx-1-jpo-10.1177_27527530251356250 for Fun Leads the Way—Healthcare Staff's Experiences of Promoting Physical Activity Among Children Who Survived a Brain Tumor: A Qualitative Study by Åsa Persson Dobruna, Helena Igelström, Pernilla Åsenlöf, Gustaf Ljungman and Sara Frygner-Holm in Journal of Pediatric Hematology/Oncology Nursing
Footnotes
Acknowledgments
The authors would like to thank the healthcare staff who participated in the focus group interviews.
Funding
The authors disclose the following financial support: the Swedish Childhood Cancer Fund (Grant No. KP2021-0015).
Declaration of Conflicting Interests
The authors declare no potential conflicts of interest with respect to the research, authorship, or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.