
Abstract
Introduction
When a child is diagnosed with cancer, life is turned upside down and the whole family is affected. Earlier strategies that parents used for managing life are no longer applicable. The child's well-being and functioning are closely connected to that of the parents. Parents and children ask for, and need, psychosocial support through the illness trajectory (Fratantoni et al., 2022; Jaaniste et al., 2022; Lin et al., 2020; Wiener et al., 2015). Children diagnosed with cancer experience challenging feelings, such as being alone and isolated and not being able to live their ordinary life because they are under attack from the cancer. To help the child deal with these emotions, and to prevent such feelings, it is important to listen to their story, provide age-adapted information about illness-related issues, and involve them in decisions regarding their illness (Darcy et al., 2019). Parenting a severely ill child is associated with several challenges and distress, for example, having huge responsibility for the ill child's needs and symptom management (Carlsson et al., 2019) while at the same time maintaining a mutual and respectful relationship with the other parent and the family as a whole. Parents often protect each other from their own psychological and emotional needs (Lewandowska, 2022; Lövgren et al., 2020). Siblings are frequently described as standing in the shadow of the needs of their ill brother or sister and having an increased risk of psychosocial problems, such as difficulties expressing and showing their feelings (Haukeland et al., 2021; Long et al., 2018; Wawrzynski et al., 2022). Open communication within the family has been shown to protect all family members from psychosocial distress (Carlsen et al., 2019; Long et al., 2018).
International guidelines for psychosocial support in pediatric oncology have been developed based on the psychosocial needs of families (Wiener et al., 2015, 2020). The family's health can be maintained and supported when interventions encompass each individual family member, as well as the family as a unit (Mooney-Doyle et al., 2021). However, there are few family-based psychosocial interventions in pediatric oncology that approach the family as a system which have been scientifically evaluated. Even fewer family-based interventions have been evaluated long-term (Enskär et al., 2015; Mooney-Doyle et al., 2021; Steele et al., 2015).
To address this gap, a family intervention, the family talk intervention (FTI), originally developed for use in psychiatric contexts (Beardslee, 2002; Pihkala et al., 2012a), was pilot-tested in pediatric oncology during 2018–2019. FTI is a psychosocial family-based intervention, also called Beardslee's family intervention, which is manual-based and includes the whole family. The primary goals of FTI are to promote resilience by facilitating family communication, support parenting, and making the children's needs visible (Beardslee, 2009). It involves six meetings where parents and children, alone or together, participate in the program at different time points, with follow-ups as required (Figure 1). FTI has an eclectic approach which includes psycho-educative, narrative, and dialogical ways of working. The psycho-educative element focuses on increased knowledge about the illness and related subjects. The narrative element involves the family's own stories and is central in FTI; the family members share their stories with each other and create a joint family history. This dialogical way of working focuses on making problematic situations visible by allowing the children's voices to be heard, sharing experiences within the family, and highlighting the different perspectives of all family members.
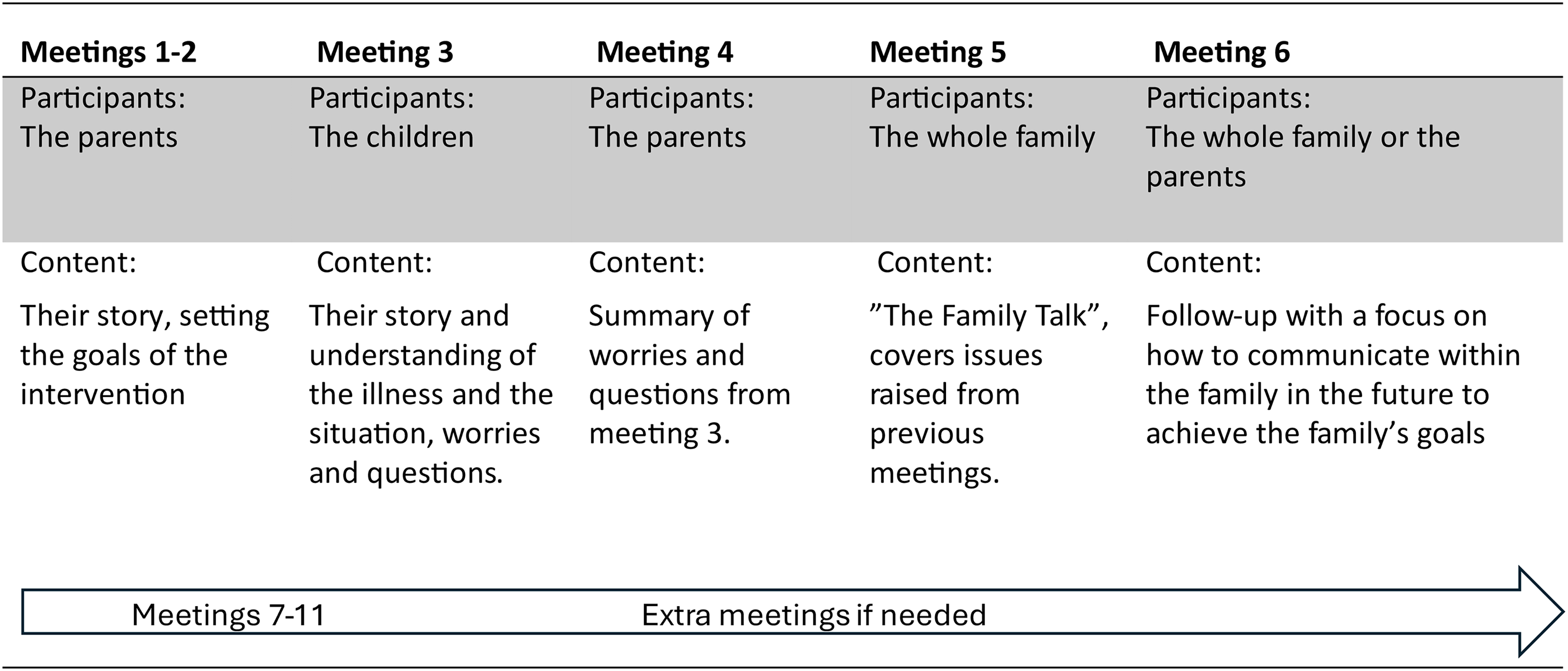
Overview of the Meetings in the Family Talk Intervention.
The pilot study of FTI in pediatric oncology showed positive results (Lövgren et al., 2022), both regarding feasibility and potential effects (Ayoub et al., 2024; Eklund & Lövgren, 2022). Parents reported that FTI helped to support their relationship through the opportunities for communication that the intervention provided. Parents and children also reported that FTI facilitated family bonding and togetherness (Ayoub et al., 2024; Eklund & Lövgren, 2022; Ivéus et al., 2022).
However, no long-term follow-up of FTI has been conducted. This study, therefore, aims to explore the parents’ experiences of what they have retained from their participation in FTI 4–5 years earlier.
Method
Design
This qualitative study involves follow-up interviews conducted 4–5 years after a complex intervention (FTI) with parents who participated in a pilot study in pediatric oncology (Lövgren et al., 2019).
Study Population
Interviews were conducted with parents who were recruited from the FTI pilot study performed in September 2018–August 2019 at one pediatric oncology center in Sweden. FTI was then led by two FTI-educated healthcare professionals, one hospital social worker, and one deacon, with extensive experience of working with families with a severely ill family member. Inclusion criteria for participating in the pilot study of FTI were that at least 2–3 months had passed since the ill child's diagnosis or relapse. Another inclusion criterion was that the participants understood and spoke Swedish. On completion of the pilot study, parents from 26 families were asked, if they consented, to be contacted in the future regarding a follow-up study. In spring 2023, we reached out to the parents from 20 families who had consented, asking if they wanted to participate in follow-up interviews. Verbal information about the follow-up study was provided and written information was sent. Thirty parents (16 mothers and 14 fathers) from 18 families consented to participate. Two families declined with no further explanation. In five of the families, their child had died during the years following their participation in FTI (Table 1).
Demographic Characteristics in the Pilot Study and the Follow-Up Study 4–5 Years Later
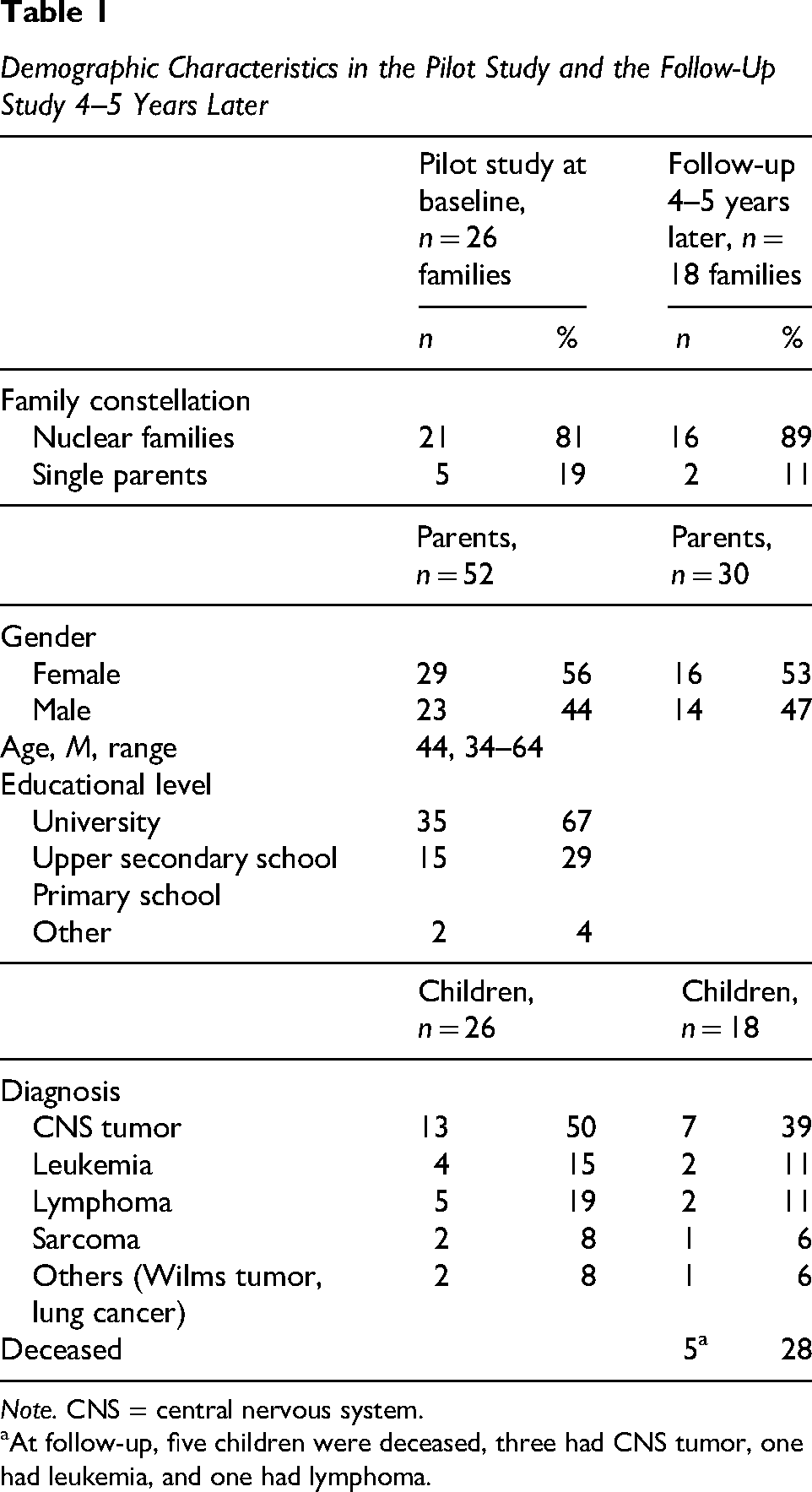
Note. CNS = central nervous system.
At follow-up, five children were deceased, three had CNS tumor, one had leukemia, and one had lymphoma.
Data Collection
The interviews were carried out between March and June 2023 and were conducted by two female research group members (the first author and a research assistant), both with extensive experience in working with families affected by severe illness. The format or location was chosen by the parents (16 by video conference and two face-to-face at the parents’ home). Thirteen dyad interviews and five single interviews were conducted. A semi-structured interview guide was used, previously used in another long-term follow-up of FTI in another care context (Bergersen et al., 2024). The first question in the interview guide involved what parents remembered from taking part in FTI 4–5 years earlier. Thereafter, the focus was on whether FTI was still useful in their everyday lives. The interviews lasted 24−75 min (M = 41 min) and were recorded and transcribed verbatim.
Data Analysis
Conventional content analysis was used based on Hsieh and Shannon's approach (Hsieh & Shannon, 2005). The transcripts were first read by the first author to gain a sense of the whole. Next, meaning units were derived from the transcripts, relating to the study aim regarding parents’ experiences of retention after their participation in FTI. Next, the meaning units were condensed and coded keeping close to the text to capture the parents’ statements. The meaning units and codes were jointly checked by all authors, so no essential information was missing. Thereafter, the codes were discussed by all authors and further discussions were held between the first and last authors to search for similarities, differences, and patterns, according to how the codes were connected to each other. All stages were transparently presented so that all authors could follow the process. Categories were then constructed from the codes and the categories were then jointly discussed by all authors until the final result was reached.
Results
Of 18 families, 13 reported long-term retention and application of the strategies they learned during the FTI intervention, which they still referred to as helpful. Parents from the other five families found it hard to distinguish the support they had received from FTI from the support given by others after their participation. However, all families found that FTI was a valuable psychosocial support they got in a difficult time in their life. The parents’ experiences of what they had retained from their participation in FTI after 4–5 years are presented below in four categories. The categories described a range of different dimensions concerning retention after FTI: (a) sharing thoughts and emotions reduced the burden of stressful situations, (b) learned strategies put the spotlight on the children, (c) long-term empowered by the validation, and (d) a springboard to managing new challenges in life.
Sharing Thoughts and Emotions Reduced the Burden of Stressful Situations
The parents described that during FTI, the family were supported to constructively share their thoughts and feelings, which has had long-term positive effects on the relationships within the family. For example, the parents described how unknown thoughts that the other parent had revealed during FTI were a key factor for understanding each other's reactions to and interpretations of illness-related information. They also described that they understood other family member's different reactions and interpretations of situations better and that this still motivated them to continue sharing their thoughts and feelings with each other.
Parents also expressed that during FTI, they had learned several strategies that helped them to manage the overwhelming emotions that come from living with a severely ill child. For example, during FTI, parents realized that it was not helpful to try to protect the other parent from their worries: “You don’t have to protect each other, because when you do, you don’t help each other.” And it was like, those two sentences, that's really something I took away from this and we have used this a lot and as a kind of way to dare to talk to each other and not think that you should protect each other when it's hard. (Father, Family 31)
By becoming more aware of the value of sharing they felt it became easier to address previous incidents and “taboo-related” issues, such as imagining their child's imminent death or planning the funeral with the other parent, something they didn’t dare raise before their participation in FTI. The increased parental openness that was initiated when FTI was still ongoing remained, according to the parents. Parents also described it as something that reduced the burden of uncertainty and stress related to living with a child with cancer.
Furthermore, parents described that they had learned several communication strategies during FTI. They reflected that they still used these strategies, which enabled them to share thoughts and emotions with the other parent, contributing to a respectful understanding of each other for a long time after FTI. These strategies included an agreement to let the other parent speak without interruption, to take one thing at the time, and not to judge or value what comes up. The strategies also included how to ask the other parent questions, which had led to an open climate even when addressing issues outside the cancer experience.
Learned Strategies Put the Spotlight on the Children
Parents described that they mainly agreed to participate in FTI because of their worries about their children and that it was ground-breaking to involve the children in the psychosocial support. They pointed out that learning strategies for how to reach the children was the most important achievement within their participation, since they felt that they hadn’t previously known how to reach out to them. Parents claimed that they still applied strategies that they had been introduced to during FTI, for example, how to initiate daily conversations or regular family meetings with the children by asking questions about their thoughts and feelings and paying attention to what the child says. Parents reminded each other of the importance of having family meetings, which had been introduced during their participation in FTI, since these helped each family member share their experiences. The family meetings had resulted in the dialogue within the family becoming more democratic. Parents pointed out that they had been worried about the siblings since they tend to get forgotten or had become invisible in the family during their brother's or sister's illness.
However, parents perceived that these family meetings gave the siblings agency and an arena where they could express their feelings of being unequal and of anger. This was still something that parents used to help the siblings to express themselves. Parents reported that after FTI, they had increased their knowledge and awareness of the siblings’ situation. They had incorporated this into daily life and still actively put the spotlight on the siblings in everyday conversations. Parents described that the strategies they learned during FTI contributed to them, as parents and in their parenthood: we got, like, a methodology, or we started working with family meetings. And we still do, [laughs] or at least it's a concept that still exists in our family, they don’t happen very regularly, but there is a dialogue about a democratic way of running things in the family … the siblings constantly end up in situations where they are forced to adapt to one thing or another and it just turns out the way it does … important for the siblings who have experienced a lot of unfairness … and anger connected to this, that this might have diminished a little by being able to … being able to talk about things. (Mother, Family 35)
Parents stated how before FTI they had been worried about saying the wrong things to their children, but after FTI they had become more confident about what to say and how to express things. This was because of the deeper understanding and new perspectives gained, based on the knowledge they had received in FTI, concerning how children can react with thoughts, feelings, and worries in stressful situations. They described that before FTI, they had found it difficult to cope with siblings voicing their fears and had become angry with the siblings for what they had said to the ill child: “I hope you don’t die,” she [sibling] said to Y [the sick child]. And we got so mad at her. To understand that it was what she hoped and felt and that it was okay. But then we got really angry with her because Y [the sick child] got really sad and it's difficult with the children. So it was that there were no taboos, get rid of them, that was very important. (Father, Family 31)
This new knowledge about children's reactions in difficult situations has helped them to be more open, tolerant, and forgiving toward the siblings even after FTI. They currently have a greater understanding and can meet the sibling where he or she is.
Moreover, parents expressed that, during FTI, they had learned to separate their own worries from the ill child's. Before it was hard for them to understand how much the ill child wanted to talk and had tried to talk a bit too often in relation to the ill child's needs. Parents described how they found out that their ill child did not want to talk about the illness all the time. The parents reported that they learned to use a special code word or sentence when the ill child wanted to talk about her/his worries or about relapse; this code word or sentence was still being used by the family. This had led to an increased respect for the ill child's wishes and sense of control when the child wanted to talk about illness-related issues, which also has contributed to a reduced uncertainty for the parents on how to address these issues.
Long-Term Empowerment Through Validation
Parents described that the different types of validation they gained from the interventionists during FTI still helped them in everyday life. Parents expressed that the stressful situation of having a child with cancer made them feel inadequate as parents, and not being able to be there for the siblings. Their participation in FTI helped them gain knowledge that made them feel more confident in their parenthood. For example, from feedback they learned that their children were open with them about their thoughts and feelings, which had contributed to a perception of being a good enough parent and knowledge that their child knew they were loved. Parents expressed that the interventionists had validated them and made them aware of their strengths as parents, such as being good at keeping the talking going, and this contributed to a more open family climate. This strengthened the parents and made them feel more confident about being good at something. Parents described that this validation encouraged them to be a role model for their children and for them to be open about their thoughts and feelings and this has helped to maintain an openness in the family. Parents also perceived that their children became more confident about being open with their own feelings and thoughts, which was also noted between the siblings: but if it has been the support program, yes, it has been, based on the way you and I have chosen to act, I think we have also influenced the children, yes, about the importance of talking … she [interventionist] just that, she raised awareness, like: “But you are a talkative family, continue with that,” like: “It will do some good.” I still think that … I have still carried with me the fact that … she said: “You talk a lot, you talk with each other, we kind of see your children and siblings talking to each other, you and X (the father) are talking, keep it up.” So that it is something that I have so concretely carried with me that I felt: “No, we are good at this and we will just carry on like this.” (Bereaved Mother, Family 39)
During FTI, parents had been encouraged to consider and acknowledge their own individual strengths and needs, which they still tried to do when facing new difficulties or situations. The confirmation they had received when taking part in FTI still gave them confidence when dealing with the burdensome reality of living with a severely ill child. The parents described the importance of taking care of themselves and their basic needs to function as a person. The validation they had received from the interventionists still gave them strength to cope. For years, they were informal caregivers to children suffering from brain tumor, all while carrying the heavy burden of both existential and physical strain. Bereaved parents described that the confirmation they received from the interventionist during FTI still gave them a sense of relief: Maybe not what was actually good about the support program, but the fear of how bad it would have been without it. “Would we not have talked with each other at all? Would we have gone around with this bomb inside us? Would we have turned in on ourselves, would we have been broken? What would have happened without the support program?” … then there is less of a risk of having problems later on after this support and I’m active in processing the grief or my feelings. (Bereaved Father, Family 39)
The parents drew strength from knowing they had done everything possible during FTI, as a prevention for their future psychological health. They addressed issues during FTI that they had previously avoided. These included differing views on managing their ill child's condition or the child's imminent death when a cure was no longer an option. They also confronted the stressful arguments that had created distance between them. By doing so, they felt they had prepared themselves to maintain better psychosocial well-being moving forward.
A Springboard to Managing New Challenges in Life
Parents described that their experiences from FTI contributed to insights into what might be helpful in difficult situations. They stated that when they faced new challenges in life, for example, new illnesses in the family, they found it easier to handle them after their participation in FTI: It's basic, if you are going to talk about things, give each thing time, don’t always discuss everything, but first see what it is. Structure is helpful when you have been through things that you are not used to handling. Keep in mind that talking is a good way forward if you get stuck. We’ve not become stuck after that (FTI). (Father, Family 36)
Parents also gave examples of how, after such a positive experience with FTI, they can support their relatives with advice when facing difficulties. Inspired by FTI, parents reported being more open and likely to share their feelings with others outside of the family than before participation. They described FTI as a springboard that created a new openness to participate in contexts where sharing the most painful thoughts and feelings with others in the same situation could be facilitated.
Furthermore, parents perceived that their child/children became more confident and learned to talk about new worries and issues he/she had to deal with after FTI: And then I think that what we did with the Interventionists probably helped Y [the sick child] to be able to tell us about things, because Y [the sick child] came to you and said: “I think I have compulsive behavior, dad,” and then Y [the sick child] started telling me about things. (Mother, Family 31)
This had helped both the ill children and siblings to raise questions about psychosocial issues that they needed professional help with after their participation in FTI.
Discussion
This is the first study that explores parents’ long-term retention of FTI in pediatric oncology care. Findings show that parents still use strategies gained from taking part in FTI 4–5 years earlier, that is, strategies that help them to continue to share their thoughts and emotions, and to maintain an open communication within the family. Parents perceived that the open communication helped to reduce stress in the family and put the spotlight on the children. The family's participation in FTI was a springboard that contributed to a willingness to participate in new support contexts, that is, peer support outside the hospital with other bereaved parents where the most difficult feelings and emotions could be shared.
The parents’ experiences of FTI in this study are similar to the experiences described immediately after the completion of FTI in pediatric oncology, such as maintaining a healthy couple relationship and an increased togetherness through open communication within the family when living with a child who has cancer (Ayoub et al., 2024; Holm et al., 2023).
Similar results have also been reported from FTI in other caregiving contexts, for example when a parent has an affective illness (Pihkala et al., 2012a, 2012b) or when a parent is dying, where FTI contributed to reduced anxiety and fewer family conflicts (Alvariza et al., 2021; Eklund et al., 2020). Findings in this study demonstrate that a psychosocial program, such as FTI, can promote parents’ feelings of resilience, since the parents reported still using several strategies that they had learned in FTI. Resilience involves a robustness within the person and, since it is not a trait, is something that a person can improve (Lundman et al., 2007; Rutter, 2012) when facing challenging and demanding life issues. One interpretation, based on the results in this study, is that parents might have increased this robustness through the new strategies they gained in FTI. For example, parents reported a deeper understanding of their own needs, but also an increased insight into the other parent's and the children's needs, and how to respond to them. The parents gave examples of how they could more easily meet new challenging situations after their participation. An intervention aiming to promote resilience, such as FTI, might start a process that enhances the ability to manage new difficulties that a person can face in the future.
As described in the results, parents emphasized how, after the child received a cancer diagnosis, they were left alone without support regarding how to reach their children. It is a unique finding that the parents in this study learned strategies, through FTI, to be able to reach out to and include the sibling as well as to the ill child, since the siblings are often described as having their needs and thoughts hidden in the shadow of the ill child's. Furthermore, in accordance with the UN's Convention on the Rights of the Child (UNCRC; UNICEF, 2024), a child needs an environment that facilitates the expression of their thoughts and emotions, coupled with the presence of someone who intentionally creates this space and engages in active, attentive listening (Holmqvist, 2019). According to Article 18 in the UNCRC, a child should be surrounded by parents or guardians who jointly take responsibility for the child's upbringing and development. A finding from this study, which demonstrates this, is how parents expressed gaining knowledge through FTI about the children's (both ill children and healthy siblings) reactions in crises and learned strategies that empowered them to put the spotlight on the children. This illustrates that the parents gave the children space, for example, in the family meetings where the parents listened to them, which contributed to lifting the children's voices in the family. Parents also referred to the validation they were given during their participation which empowered them to become role models for their children and be open with their own thoughts and emotions.
This study fulfills a knowledge gap regarding the long-term evaluation of a family intervention in pediatric oncology; however, it has some weaknesses. The study only included Swedish-speaking participants, and the majority were highly educated. This could limit the possible transferability of the results. Additionally, children were not asked about their retention of FTI; however, 5 years is a long time in a child's life, and it is challenging for children to recall events from such a distant past, which we experienced in another long-term follow-up concerning the palliative care of adults involving dependent children. Another limitation is the difficulty in distinguishing between parents’ perceptions, their actual experiences, and their ability to reliably recall the factors that influenced them. This is a common challenge in qualitative research and should be considered when interpreting the findings. However, it is both a strength and a limitation to conduct dyad interviews, as in this study. A strength might be related to the dyads feeling safe and helping each other to recall their experiences and retention. On the other hand, one parent's retention might affect the other parent's feelings and memories.
Conclusion and Implication
Long-term evaluation provides valuable insights into an intervention's sustainability and potential intended or unintended consequences over time. It ensures that the intervention remains relevant to changing needs, supports evidence-based improvements, and strengthens its credibility for wider implementation and policy decisions. In this evaluation of FTI, parents of children cared for in pediatric oncology reported that they had learned strategies from their participation that persist long-term. These strategies have continued to help them maintain an open communication in their daily family life and to put the spotlight on their children and their needs. It seems that an intervention such as FTI contributes to increasing parents’ resilience when facing adverse life events later in life. Full-scale studies of FTI in clinical practice are now ongoing and it is essential to ensure its effectiveness, adaptability to children and their families’ needs, and integration into standard care.
Footnotes
Acknowledgments
We would like to express our sincere gratitude to all the parents who participated in our interviews. We deeply appreciate their generosity in sharing their experiences with us and for dedicating their time and effort to be a part of this study.
Data Availability
Data generated and/or analyzed during the current study are not publicly available due to individual privacy that could be compromised but are available from the corresponding author on reasonable request.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclose the following financial support: Swedish Childhood Cancer Fund (grant number: TJ2022-0028), the Swedish state under the agreement between the Swedish government and the county councils, ALF agreement (grant number: RS2022-0674), Swedish Research Council (grant number: 2021-00999), and Swedish Research Council for Health, Working Life and Welfare (grant number: 2021-00260).
Ethical Approval
The study received ethical approval from the Swedish Ethical Review Authority (Dnr 2018/250-31/2, 2018/1852-32, and 2023-01365-02).
Informed Consent
Verbal and written information about the study was provided to all participants, and written informed consent was obtained before the interviews were conducted.