
Abstract
Introduction
The prevalence of traumatic stress symptoms (TSS) in parents of children with cancer is high, with 40%–83% reporting symptoms within the first month of a child’s diagnosis (Price et al., 2016). For most parents, TSS will diminish and stabilize throughout treatment and remission. However, for a subset of parents, TSS remains severe (Price et al., 2016). With the focus of clinical care on their child with cancer, these parents may struggle unnoticed without supportive services, impacting their own mental health and the care they are able to provide to their child (National Scientific Council on the Developing Child, 2009). A recent meta-analysis examining the prevalence of mental health challenges in parents of children with cancer (58 studies, 9,262 parents) revealed that a significant subset of parents experienced clinical levels of anxiety (21%), depression (28%), and posttraumatic stress disorder (PTSD; 26%) (van Warmerdam et al., 2019). Early identification of parents with significant TSS is essential to providing timely and individualized supportive care (Wiener, Kazak, et al., 2015).
Standards for the Psychosocial Care of Children with Cancer and Their Families provide evidence-based recommendations for psychosocial care that hospitals should provide to all children with cancer and their families. Standard six is dedicated to early and ongoing assessment of parent/caregiver mental health needs to inform access to appropriate care (Kearney et al., 2015; Wiener, Kazak, et al., 2015). The availability of brief screeners validated for parents of children with cancer is critical to meeting this standard. Currently, there are screeners for overall psychosocial risk (Psychosocial Assessment Tool 3.0; Kazak et al., 2018), depression (Patient Health Questionnaire–9; Kroenke et al., 2001; Spitzer et al., 1999), and anxiety (General Anxiety Disorder–7; Williams, 2014); however, there is an absence of validated short screeners for TSS in pediatric cancer. A validated screener, like the six-item abbreviated PTSD Checklist–Civilian (PCL-6), which could be administered by bedside or advanced practice nurses, would allow for quick standardized assessment of TSS, enabling supportive care clinicians to accurately identify, prioritize, and allocate services.
The PTSD Checklist (PCL) has been used in clinical care and research across many populations and has population-specific versions, including PCL-Military, PCL-Civilian, and abbreviated PCL-Civilian (PCL-6; Lang et al., 2012). While widely used in research related to parents of children with cancer, only one study has examined the psychometric properties of the PCL-C for this population (Adkins et al., 2008; Bressler et al., 2018). The investigators established the convergent diagnostic utility of the PCL-C with SCID–PTSD. However, the authors noted that the recommended cutoff score might not be appropriate for this group and is better utilized as a screening tool for parents of children with cancer (Manne et al., 1998). Despite the popularity and utility of the PCL-6 for parents of children with cancer, its psychometric properties have not been thoroughly examined for this population.
The aims of this secondary analysis were (1) to evaluate the convergent construct validity of the PCL-6 with the Impact of Events Scale–Revised (IES-R; Marmar et al., 1997) and Profile of Mood States–Short Form (POMS-SF; Shacham, 1983), (2) evaluate the divergent construct validity of the PCL-6 with the Index of Wellbeing (IWB; Campbell et al., 1976), and (3) evaluate the internal consistency of the PCL-6 as a screener for parents of children with cancer. Based on previous literature, we hypothesized that total severity scores from the PCL-6 would have a moderate positive correlation (r = .40) with total scores from the IES-R (Marmar et al., 1997) and a moderate positive correlation (r = .40) with total negative mood scores from the POMS-SF (Aim 1). For Aim 2, we hypothesized a moderate negative correlation (r ≤ −.40) with overall scores from the IWB (Campbell et al., 1976). For Aim 3, we hypothesized that there would be good internal consistency across all six items of the PCL-6 (α = .80−.90) (Adkins et al., 2008; Bressler et al., 2018; Chaffin & Shultz, 2001; Cortina, 1993; Creamer et al., 2003; Curran et al., 1995; Kazak et al., 2004; Lang et al., 2012).
Method
This secondary analysis used data collected during a multisite trial examining an intervention to lower distress and improve health outcomes in children (ages 3–8 years) with cancer and their parents (NINR R01NR1578 (Robb, PI); Robb et al., 2023). The Institutional Review Board of Indiana University (study identification #1511888386) approved all data collection procedures. In this trial, investigators collected measures of TSS (PCL-6; IES-R), mood disturbance (POMS), and well-being (IWB) from parents during their child’s cancer treatment at three time points (baseline, postintervention (3 days after baseline) and 30 days after baseline). For this analysis, we only used baseline parent self-report data to examine the construct validity and internal consistency of the PCL-6. Full details from the original trial are available in the primary publication (Robb et al. 2023).
Participants
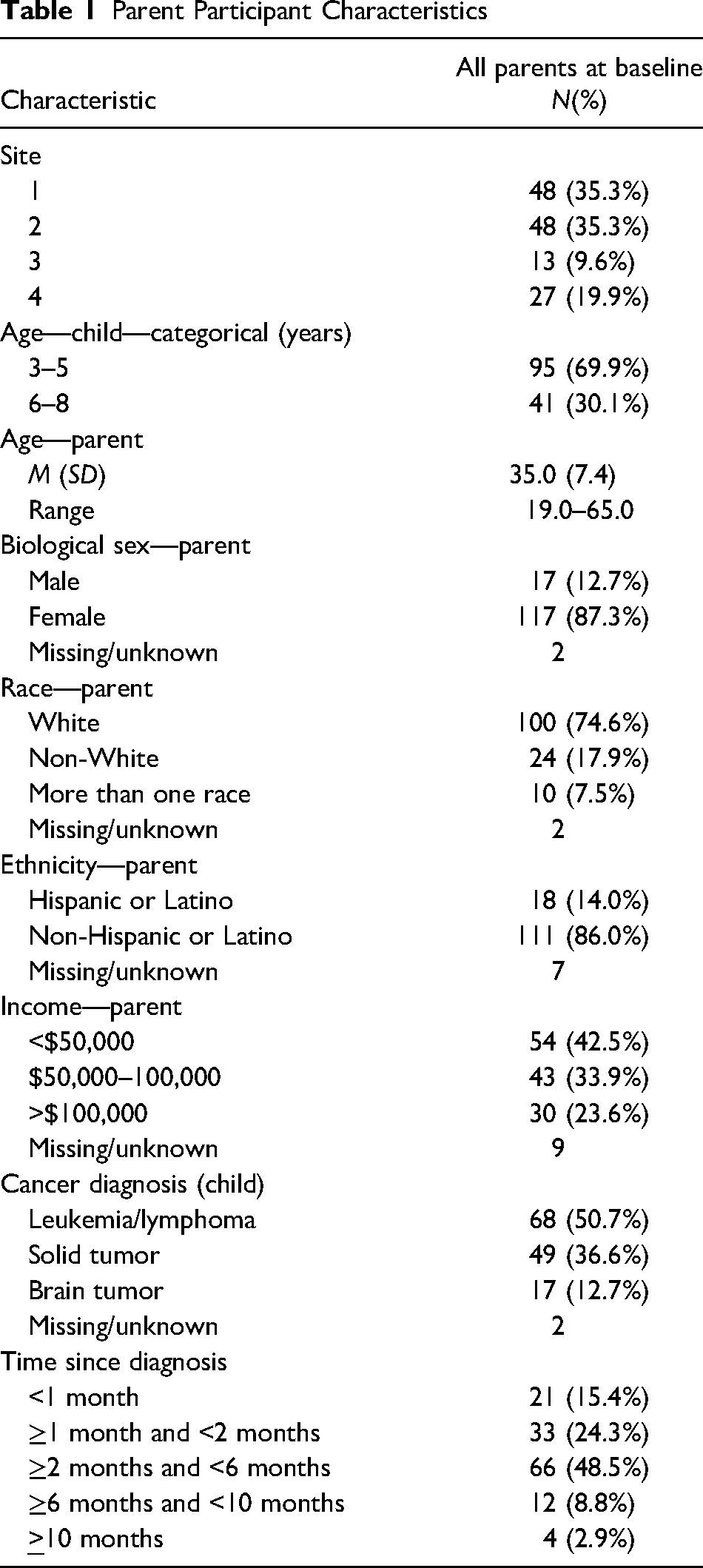
All parent/caregiver participants who completed baseline measures for the PCL-6, IES-R, POMS-SF, and IWB (Table 1; n = 136) were included in this analysis. To be included in the main trial, the parent had to be (a) the primary caregiver of a child undergoing active cancer treatment between 3 and 8 years of age, (b) aged >18 years at the time of consent, and (c) able to be present for all intervention sessions. Active cancer treatment was characterized by an expected treatment course of at least 3 days to receive moderate- to high-intensity chemotherapy (in-patient or outpatient). Full details from the original trial can be found in the primary publication (Robb et al., 2023).
Parent Participant Characteristics
Measures
Abbreviated PCL-6
The PCL-6 is the abbreviated six-item version of the 17-item PCL-C (Lang et al., 2012; Weathers et al., 1994). Respondents rate items on a 5-point Likert-type scale. Higher scores indicate higher levels of TSS. The PCL-C demonstrated good internal consistency (Cronbach’s α = .94 (95% confidence interval [CI] [.93, .95]) pooled from 135 studies of a variety of clinical and nonclinical populations (Bressler et al., 2018). The PCL-C also demonstrates good test–retest reliability = .79 at 1 month or less, pooled from six studies of various clinical and nonclinical populations (Bressler et al., 2018). The PCL-6 accounted for 94.3% of the variability (r = .943) when correlated to the full PCL-C (Lang et al., 2012).
IES-R (22 Items)
The IES-R is frequently used as a self-report measure of traumatic stress reactions to a specific event and with parents of children with cancer in numerous studies (van Warmerdam et al., 2019). The IES-R has acceptable reliability and validity across clinical and nonclinical populations, including good internal consistency (α = .94−.96; Adkins et al., 2008; Creamer et al., 2003; Rash et al., 2008). Like the PCL-6, higher scores indicate more traumatic symptoms associated with the specified event. For this study, the specified event was the parent’s experience of their child’s cancer treatment.
POMS-SF
The POMS-SF is a 37-item self-report of mood disturbance (Shacham, 1983). Higher scores indicate a greater number of mood symptoms. The POMS-SF is valid (concurrent r = .95) and reliable (α = .92) and has been used extensively to assess parent emotional distress in pediatric cancer research (Curran et al., 1995).
IWB
The IWB is a nine-item self-report quality of life measure. The IWB is a semantic differential scale that asks respondents to state feelings about their present life using adjective extremes (example: 1 = discouraging; 7 = hopeful). High scores indicate higher levels of well-being. The scale has consistently been reported as having construct validity (Campbell et al., 1976). Evidence of reliability includes a Cronbach’s alpha of .88 in our previous work with this population (Hasse et al., 2022).
Statistical Method
Convergent and Divergent Construct Validity
We compared baseline scores of the PCL-6 to baseline scores of the IES-R and POMS-SF to establish convergent construct validity and the IWB to establish the divergent construct validity of the PCL-6. With a sample of 136 at baseline, a two-sided Fisher’s z-test (α = .05) has 80% power to detect a Spearman correlation ≥.24. We calculated Spearman’s correlation coefficient to determine the strength of the correlations, hypothesizing moderate correlations (r = .4−.6). This range is consistent with other studies of construct validity for other versions of the PCL (Bressler et al., 2018). Primary correlation was calculated with the IES-R, a standard measure of TSS. Additional correlations between measures of mood disturbance (POMS-SF; convergent validity) and IWB (divergent validity) provide supporting information as mood disturbance has been associated with TSS, and feelings of well-being are generally negatively correlated to TSS (Gold et al., 2012). We calculated Spearman’s correlations, 95% CIs, and p-values due to the non-normality of the measures as indicated by Shapiro–Wilk tests.
Internal Consistency
To calculate internal consistency, we calculated Cronbach’s alpha using the scores of each of the six items of the PCL-6 for all parent/caregiver participants at baseline (n = 136). We also calculated item-to-total correlations. Before data analysis of the PCL-6, we calculated descriptive statistics for each item.
Results
Convergent Construct Validity
Results indicated good convergent construct validity for the PCL-6 with the IES-R and POMS-SF. Total IES-R scores had a strong positive correlation with total severity PCL-6 scores (Spearman’s rho = .656, p = .001, 95% CI [.545, .745]). There was also a strong positive correlation between POMS-SF total negative mood scores and total severity PCL-6 scores (Spearman’s rho = .733, p = .001, 95% CI [.641, .804]).
Divergent Construct Validity
As hypothesized, results indicated moderate divergent construct validity for the PCL-6 with the IWB, an indicator of well-being. For the IWB overall score and the total severity PCL-6 scores, there was a moderate negative correlation (Spearman’s rho = −.416, p = .001, 95% CI [−.550, −.262]). See Table 2 for results and Figure 1 for visual depiction.
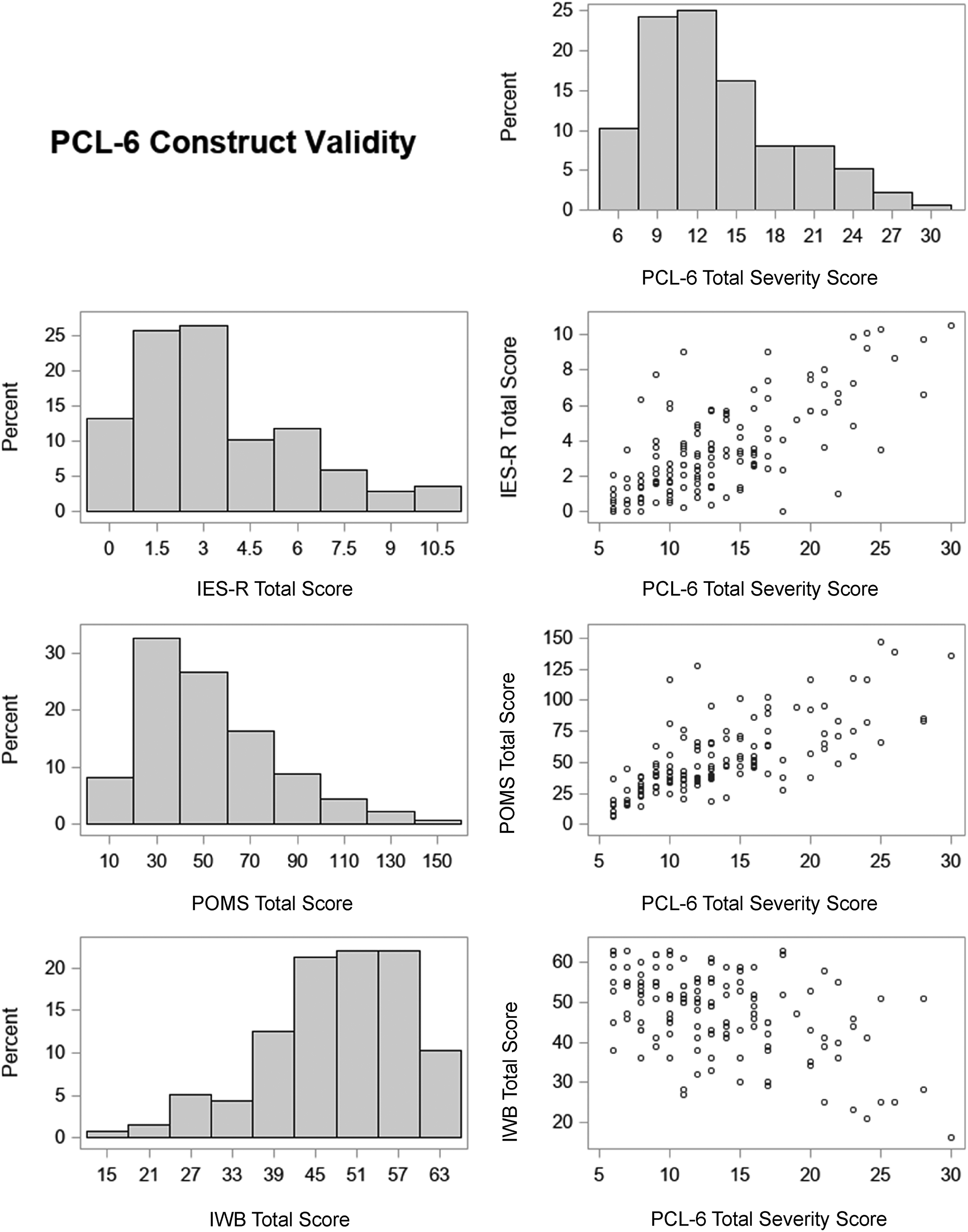
Visualization of results.
Construct Validity
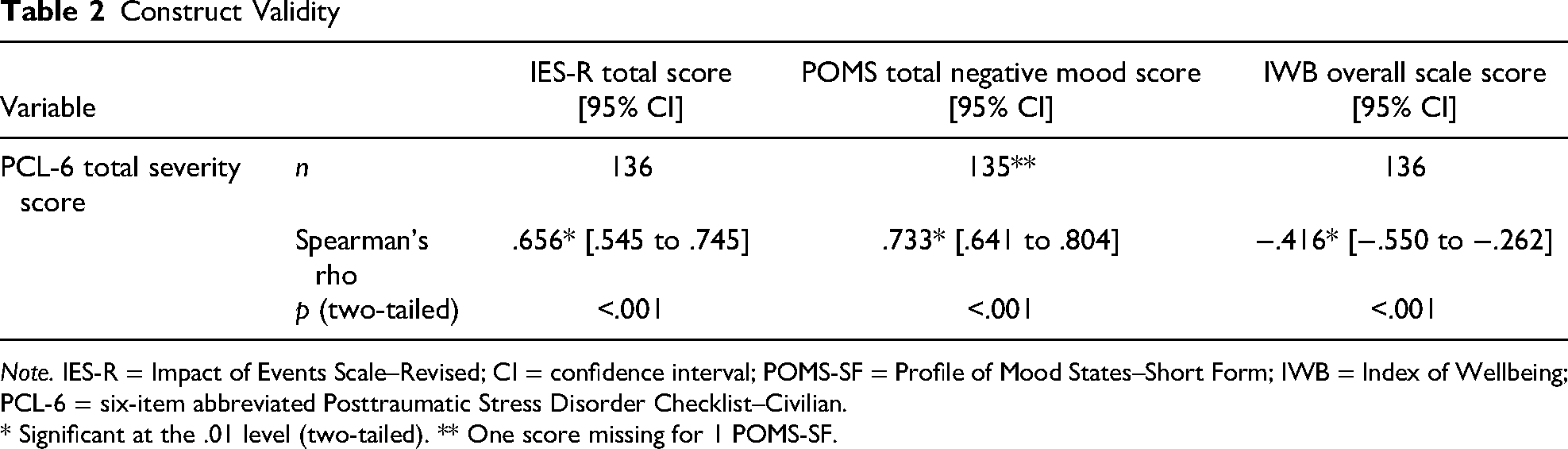
Note. IES-R = Impact of Events Scale–Revised; CI = confidence interval; POMS-SF = Profile of Mood States–Short Form; IWB = Index of Wellbeing; PCL-6 = six-item abbreviated Posttraumatic Stress Disorder Checklist–Civilian.
* Significant at the .01 level (two-tailed). ** One score missing for 1 POMS-SF.
Internal Consistency
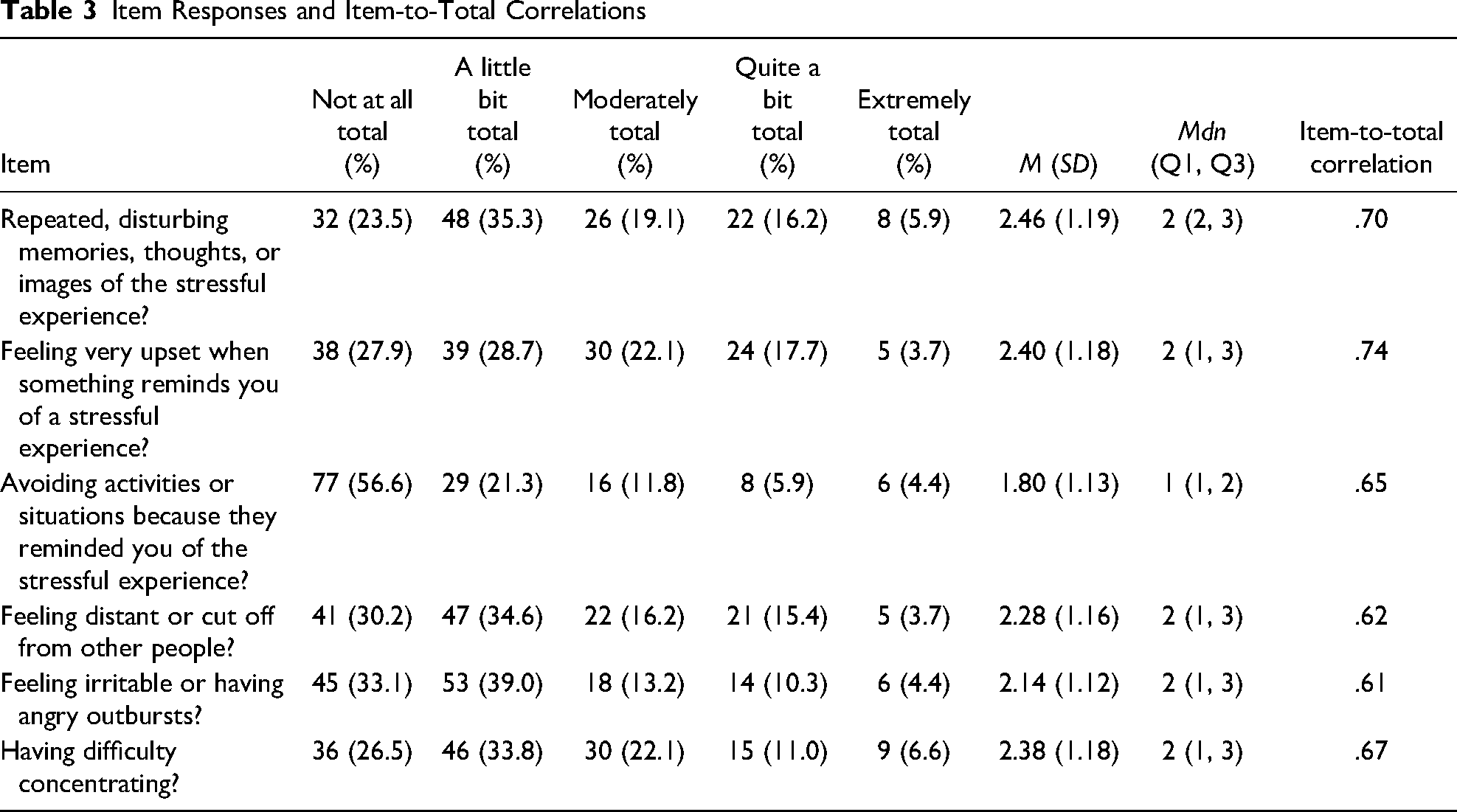
Consistent with our hypothesis, results indicated good internal consistency across the six items of the PCL-6 with Cronbach’s α = .868. Item-to-total correlations ranged from .61 to .74. We provide item statistics in Table 3.
Item Responses and Item-to-Total Correlations
Discussion
This study examined the psychometric properties of the PCL-6 as a TSS screener for parents of young children diagnosed with cancer. Taken together, these results indicate good convergent construct validity for the PCL-6 against other frequently used measures of traumatic stress (IES-R) and mood (POMS-SF), and reasonable divergent construct validity with a measure of wellbeing (IWB), and good internal consistency. The availability of a brief validated screener for this specific population is valuable as it allows for a variety of clinicians, including bedside and advanced practice nurses, to screen parents for TSS symptoms to identify parents who may need specialized care (Wiener, Viola, et al., 2015).
Implications for Nurses
Bedside and advanced practice nurses may be the first to notice that a parent is in need of extra support. However, supportive care resources may be limited in many pediatric oncology units, especially for parents/caregivers. A short screening tool like the PCL-6 would allow bedside nurses, advanced practice nurses, or allied health professionals to screen and identify parents/caregivers with clinically significant symptoms who may need additional support, while also providing concrete evidence to support the referral for psychosocial support services. PCL-6 scores may serve to communicate about a distressed parent across disciplines, improving communication between bedside nurses and psychosocial care providers. Access to supportive services is part of the Standards for the Psychosocial Care of Children with Cancer and Their Families and is essential to quality pediatric cancer care (Kearney et al., 2015; Wiener, Viola, et al., 2015).
The psychological well-being of parents plays a central role in the health and well-being of children with cancer. Children, especially young children, are vulnerable to the neurological, physiological, psychological, and developmental impact of trauma and toxic stress (Bates et al., 2022). Positive interactions with a parent and/or trusted adult have been identified as a powerful factor for “buffering” or resilience in young children (Shonkoff et al., 2012). If a parent is experiencing high levels of TSS, their capacity to provide emotional support to their child decreases (National Scientific Council on the Developing Child, 2009). Therefore, improving psychosocial support for parents is beneficial for both parents and children.
Limitations
The existing data provided a large enough sample to achieve adequate power for the secondary analysis, and the rigorous data collection and fidelity procedures used in the original trial helped ensure data quality ([citation redacted for blind review]). Although household income varied, the sample was relatively homogeneous for race and ethnicity, limiting the generalizability of these findings for parents often underrepresented in research.
Conclusion
These findings provide initial support for the PCL-6 as a valid screener to assess TSS, which is common in parents of young children with cancer. Additional testing is needed to examine its validity in a racially and ethnically diverse sample of parents. Access to valid screeners is essential for implementing the Psychosocial Standards of Care for Children with Cancer and their Families (Kearney et al., 2015) and supporting clinician efforts to efficiently and accurately identify, prioritize, and allocate supportive care services to parents in need.
Footnotes
Clinical Trial Registration
Clinical Trials.gov Identifier: NCT03085927
Data Availability Statement
Data that support the findings of this study are available from the last author upon reasonable request.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
This study was approved by the Indiana University Institutional Review Board (Study #1511888386). All methods for this study were carried out in accordance with guidelines and regulations set forth by the Indiana University Institutional Review Board.
Funding
The authors would like to disclose the following financial support for this study: NIH/NINR (R01NR1578, Sheri Robb, PI), Champion Center for Cancer Control Research (Elizabeth Harman, PI), and NIH/NCI (T32CA117865, Champion and Mosher, MPI).
Informed Consent
Informed consent was obtained from all the participants involved in the study. Parent participants provided written/signed informed consent for their own participation. For all child participants, we obtained written/signed informed consent from the child’s parent and/or legal guardian. In addition to written/signed informed consent from the child’s parent and/or legal guardian, we also obtained written assent from the child if they were 7 years of age or older.