
Abstract
Introduction
Childhood cancer is a distressing diagnosis for all members of the family (Long & Marsland, 2011). Among parents, psychological concerns such as anxiety, depression, and posttraumatic stress may persist longitudinally, particularly for those with preexisting mental health concerns (Kearney et al., 2015; Van Warmerdam et al., 2019). Parental experiences of a child's cancer diagnosis are further characterized by diminished control over typical routines and parenting decisions (McCubbin et al., 2002; Patterson et al., 2004). Given this context of decreased parental autonomy, factors that promote caregiver resilience and effective coping are an important focus for research and clinical intervention alike.
Activism, defined in the current study as actions taken to benefit children with cancer as a group, has not been directly investigated as a coping strategy in previous research despite its relevance to childhood cancer. Common forms of activism have often focused on raising research funding for childhood cancer treatments (Smith & Hoffman, 2016) as well as reducing the negative impact of sociopolitical variables on children with cancer and their families. Examples of these sociopolitical variables include barriers to healthcare access, stigma about the physical side effects of cancer treatment, and the medical burden of current cancer treatments (Beltrami et al., 2022; Collins et al., 2019; Smith & Hoffman, 2016). Activism efforts may take political or philanthropic forms. One example of legislative advocacy is the Childhood Cancer Survivorship, Treatment, Access, and Research (STAR) Act, which received strong support from childhood cancer lobbying organizations prior to its passage in 2018 (American Childhood Cancer Organization, 2018). Regarding philanthropic activism, charities that work to fund childhood cancer research and financial aid for families raise tens of millions of dollars per year (Alex’s Lemonade Stand Foundation, 2020).
Previous qualitative research investigating the broad impacts of the childhood cancer experience has identified activism as a possible coping strategy of interest. Activism has been described as a way to achieve a sense of meaning in the cancer experience, particularly for bereaved parents (Barrera et al., 2009; Meert et al., 2015). Among childhood cancer survivors and their caregivers, activism has been described as a means of expressing gratitude and connecting with other families affected by childhood cancer (Molinaro & Fletcher, 2018; Patterson et al., 2004). However, no prior studies have quantitatively explored activism or its psychological correlates among parents of children with cancer.
The coping model outlined by Carver et al. (1989), which includes active, socially supported/emotion-focused, and avoidant coping styles, has been used to describe coping approaches employed by parents of children with cancer. Prior research indicates that active, or problem-focused, coping is associated with less distress whereas avoidant coping is associated with more distress among parents of childhood cancer survivors (Turner-Sack et al., 2016). Cancer-related activism can be conceptualized as a form of active coping given its focus on improving survival outcomes for children with cancer. Because activism efforts frequently involve working with groups and inherently focus on children with cancer as a group rather than individual children, childhood-cancer-related activism may also be viewed as tapping into socially supported/emotion-focused coping, which refers to giving or receiving social support (Carver et al., 1989).
Among the potential positive and negative correlates of activism, one that has been thoroughly explored in prior studies is hope. Hopefulness has been described as a critical resource for coping by parents of children with cancer in various treatment stages and various prognostic circumstances (Conway et al., 2017; Kamihara et al., 2015; Sisk et al., 2018). Among self-identified activists for a variety of causes, activism is positively correlated with perceived hopefulness and a sense of agency (Klar & Kasser, 2009). This suggests that when parents are more engaged in activism efforts, they may have greater exposure to projects and policies that improve the lives of children with cancer, which may bolster their hope for the future.
Given the nature of activism as both problem-focused and socially oriented, we anticipated that activism would be positively associated with active and socially supported/emotion-focused coping styles. We also proposed that activism would be positively associated with parental hopefulness. Given that we viewed activism as a relevant and adaptive means of coping with the cancer experience, we also anticipated that activism would be negatively associated with depression. Lastly, given the recognition that many people may already engage in other forms of activism, we attempted to control for prediagnosis activism and investigate the unique salience of childhood-cancer-related activism by assessing parental engagement in both childhood-cancer-related activism and general activism (activism on behalf of any other cause) both pre- and postdiagnosis.
Study Aims
The aim of this study was to investigate self-reported types of childhood-cancer-related activism by parents of children with cancer and relations to general activism, activism rates both pre- and postdiagnosis, and potential correlates of activism, including child treatment variables, parental hope, depression, active coping, avoidant coping, and socially supported/emotion-focused coping. Given a lack of prior quantitative research in this area, the current study was primarily exploratory in nature. Although previous qualitative research on parental coping in pediatric cancer shaped the aims and expected findings of the current study, given the lack of previous quantitative research on parental activism, study questions are not explicitly framed as hypotheses.
Method
Participants
Participants in the current study were parents (including other primary caregivers) of children who were diagnosed with any type of cancer prior to the age of 18, regardless of the child's current age or length of time since diagnosis. Eligible participants included parents whose children were receiving cancer treatment, parents whose children had completed cancer treatment, and parents whose children are no longer alive. Because the current study was primarily exploratory in nature, we sought to include parents with a variety of experiences related to their child's cancer diagnosis. The consent form indicated that only one caregiver per family could complete the study. Participants were required to be able to read and write in English since all procedures were conducted in an online survey.
The necessary sample size for this study was found to be 153 based on a power analysis conducted using G*Power 3.1.4.9 statistical software (f 2 = 0.15, α = .05), using two-tailed tests with p < .05 significance. Recruitment for the study began in February 2020 and continued over a period of 5 weeks. Although the full sample size had not yet been reached, recruitment was suspended following the onset of the COVID-19 pandemic in March 2020 due to concerns that recruiting a medically vulnerable population during this time could be both overly burdensome and lead to cohort effects regarding self-reports of psychological well-being and distress.
All measures, except for demographics, required participants to respond to all items before proceeding. Thus, attrition was the only cause of missing nondemographic data. Of the 93 participants who completed the consent form, 53 completed the entire survey. Partial responses were included in the analyses if parents had completed cancer-related demographic questions, childhood-cancer-related activism measures, and at least one other measure. See Figure 1 for CONsolidated Standards Of Reporting Trials inclusion flow chart.
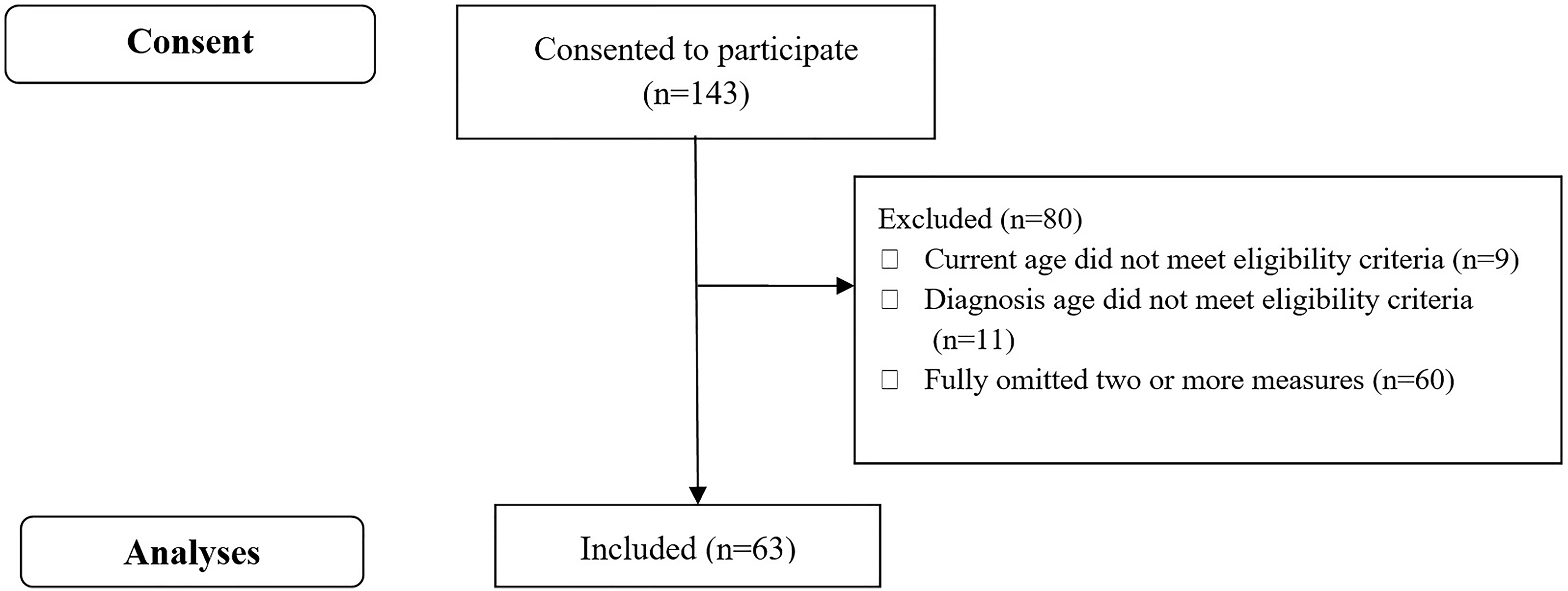
CONSORT recruitment flow chart.
Statistical Analyses
All analyses were conducted using IBM SPSS Statistics 27 software (IBM Corp., 2020). The initial analysis included descriptive statistics to assess the normality distribution across study variables. Internal reliability was also assessed for all measures. All p-values reported are of two-tailed tests, with p < .05 significance. The study aims were assessed using Pearson's r correlations and hierarchical regression. All variables included in regression analyses were first confirmed to significantly correlate with the outcome variable on a bivariate level without being intercorrelated (r > .70).
Procedure
The study was approved by the (Eastern Michigan University) Human Subjects Research Committee. All procedures were completed online using REDCap survey software (Harris et al., 2009). The consent form was at the beginning of the survey, and participants anonymously indicated their consent to proceed to the remainder of the study. The survey included measures of demographics, activism, hopefulness, coping, and depression. At the end of the survey, mental health resources (i.e., phone numbers and websites for the National Alliance on Mental Illness and National Suicide Prevention Lifeline) were listed to ensure that participants could access support if they were distressed. Recruitment took place online through Facebook and Instagram posts on accounts managed by the research team. Social media posts indicated that we were seeking parents who had ever had a child diagnosed with cancer to participate in a study about coping with the experience. As a participation incentive, advertisements indicated that $2 would be donated to a childhood cancer charity for each survey response that was completed. The link to the research study was publicly accessible via both social media platforms that were used for recruitment.
Measures
Demographics and Child Treatment Variables
This questionnaire was created for the purpose of the present study. Caregiver age, gender, race/ethnicity, education, income, current child age, age at diagnosis, child race/ethnicity, and child gender were collected for descriptive purposes. The following child medical treatment variables were collected: time since diagnosis, treatment/remission/deceased status, cancer type, type(s) of treatment received (chemotherapy, surgery, radiation, immunotherapy, bone marrow transplant) and type(s) of side effects reported (physical impairment, cognitive impairment, organ damage, secondary cancer/relapse, ongoing emotional distress). The number of treatment types and number of side effects were each included separately in analyses and collectively conceptualized as an indication of cumulative exposure to cancer-related stressors.
General Activism
General activism was assessed using the Activism Orientation Scale—Conventional subscale (AOS-C; Corning & Myers, 2002). The AOS-C is a self-report measure that assesses whether an individual has engaged in a variety of social or political activism behaviors during a specified time period or plans to do so in the future (Corning & Myers, 2002). Internal reliability of the AOS-C is strong (α = .88–.96; Corning & Myers, 2002; Klar & Kasser, 2009). The original measure used a Likert-type scale (0 = extremely unlikely to 3 = extremely likely) to assess current engagement in activism and was validated with a college student sample (Corning & Myers, 2002). In this study, we adapted the instructions of the AOS-C to elicit only retrospective responses. Participants indicated whether they had engaged in each activity (0 = no, 1 = yes) both before and after their child's cancer diagnosis. The measure was otherwise unchanged from its original form for use in the current study, with all 28 items included. Possible scores on the AOS-C ranged from 0 to 28, with higher scores indicating participation in more activism behaviors. The AOS-C demonstrated strong internal reliability for both prediagnosis activism (α = .94) and postdiagnosis activism (α = .96) in the current study.
Childhood-Cancer-Related Activism
A modified version of the AOS-C was created for the current study to measure childhood-cancer-related activism: the Childhood Cancer Activism Scale (CCAS). Modifications were made first by consulting extant literature on this topic (Barrera et al., 2009; Molinaro & Fletcher, 2018; Smith & Hoffman, 2016), and then through team discussion and reaching a consensus among all authors. Items were reworded from the original AOS-C to ask specifically about childhood-cancer-related activities (i.e., “invite a friend to attend a meeting of a social or political organization or event” was rewritten as “invite a friend to attend a fundraiser or other advocacy event for children with cancer”). Thirteen items from the original measure were not retained due to a lack of relevance to children with cancer (e.g., “present facts to contest another person's social or political statement”). The modified scale has 15 items that are each scored yes/no depending on whether the behavior has occurred, with possible scores ranging from 0 to 15. Higher scores indicate engagement in more types of childhood-cancer-related activism behaviors (see Figure 2 for the full list of items). As with general activism, parents were asked to retrospectively report actions they took both before and after their child's diagnosis. Postdiagnosis activism captured all actions taken since the child's initial diagnosis of cancer, regardless of how much time passed between diagnosis and participation in the study. The CCAS demonstrated strong internal reliability for prediagnosis activism (α = .91) and postdiagnosis activism (α = .79) in the current study.
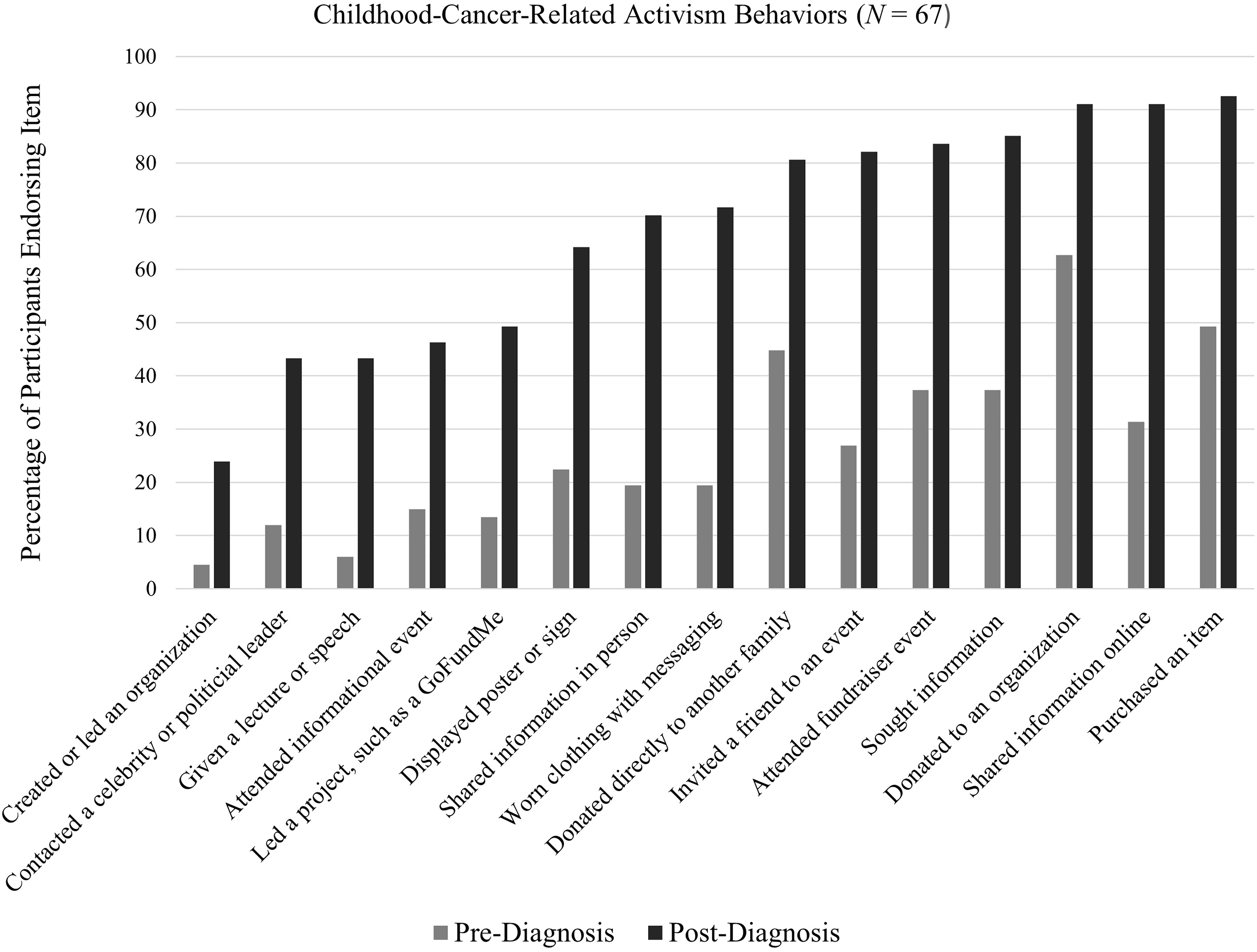
Prediagnosis and postdiagnosis childhood-cancer-related activism engagement.
Coping Styles
Twelve subscales of the COPE inventory (COPE) were used to measure active coping, socially supported/emotion-focused coping, and avoidant coping (Carver et al., 1989). Each subscale includes four items, and item scores range from 1 (I usually don’t do this at all) to 4 (I usually do this a lot). Possible scores range from 12 to 48. Higher scores indicate more usage of the coping style. The reliability of active coping (α = .62–.80) and socially supported and emotion-focused coping (α = .75–.85) are somewhat higher than the reliability of avoidant coping (α = .45–.71; Carver et al., 1989). The measure was validated using a college student sample (Carver et al., 1989). The COPE demonstrated strong internal reliability in the current study for all three subscales: active coping (α = .87), socially supported and emotion-focused coping (α = .88), and avoidant coping (α = .77).
Hope
Hope was measured using the Adult Hope Scale (Snyder et al., 1991). Items are rated on a 4-point scale (1 = definitely false, 2 = mostly false, 3 = mostly true, 4 = definitely true; Snyder et al., 1991). Possible scores range from 8 to 32. Higher scores indicate greater perceived hopefulness. The Adult Hope Scale has shown strong internal and test–retest reliability, consistently demonstrating α > .75 in its two subscales, agency and pathways (Hellman et al., 2013). It was originally validated with a college student sample (Snyder et al., 1991). When used with parents of children with cancer, the Adult Hope Scale has shown convergent validity with family functioning (Popp et al., 2015) and discriminant validity with depression and anxiety (Germann et al., 2015). The Adult Hope Scale demonstrated strong internal reliability for agency (α = .77), and pathways (α = .85) in the current study.
Depression
The nine-item depression screen on the Patient Health Questionnaire (PHQ-9) was used to measure depression in the current study (Kroenke et al., 2001). The PHQ-9 is a valid self-report measure of depression that has demonstrated concordance with mental health provider interviews with test–retest reliability of α = .84 (Kroenke et al., 2001). It was originally validated with a sample of patients in adult primary care (Kroenke et al., 2001). For each symptom, scores from 0 (not at all) to 3 (nearly every day) indicate how often the symptom occurred during the prior 2 weeks (Kroenke et al., 2001). Possible scores range from 0 to 27. A final question asks respondents to report how difficult they find daily functioning tasks using a range from “not difficult at all” to “extremely difficult” (Kroenke et al., 2001). Higher scores indicate greater depression, with a score of 10 or greater indicating that respondents should be assessed for potential major depression (Manea et al., 2012). The PHQ-9 demonstrated strong internal reliability in the current study (α = .91).
Results
Participants
The majority of the sample (N = 67) were White non-Hispanic (95.6%), female (92.5%), and married (88.1%) caregivers of childhood cancer survivors. Most were parents of children who had completed cancer treatment (n = 53; 79%), with the remainder being parents of children currently receiving cancer treatment (n = 8), or bereaved parents (n = 6). See Table 1 for additional sample characteristics.
Sample Demographics
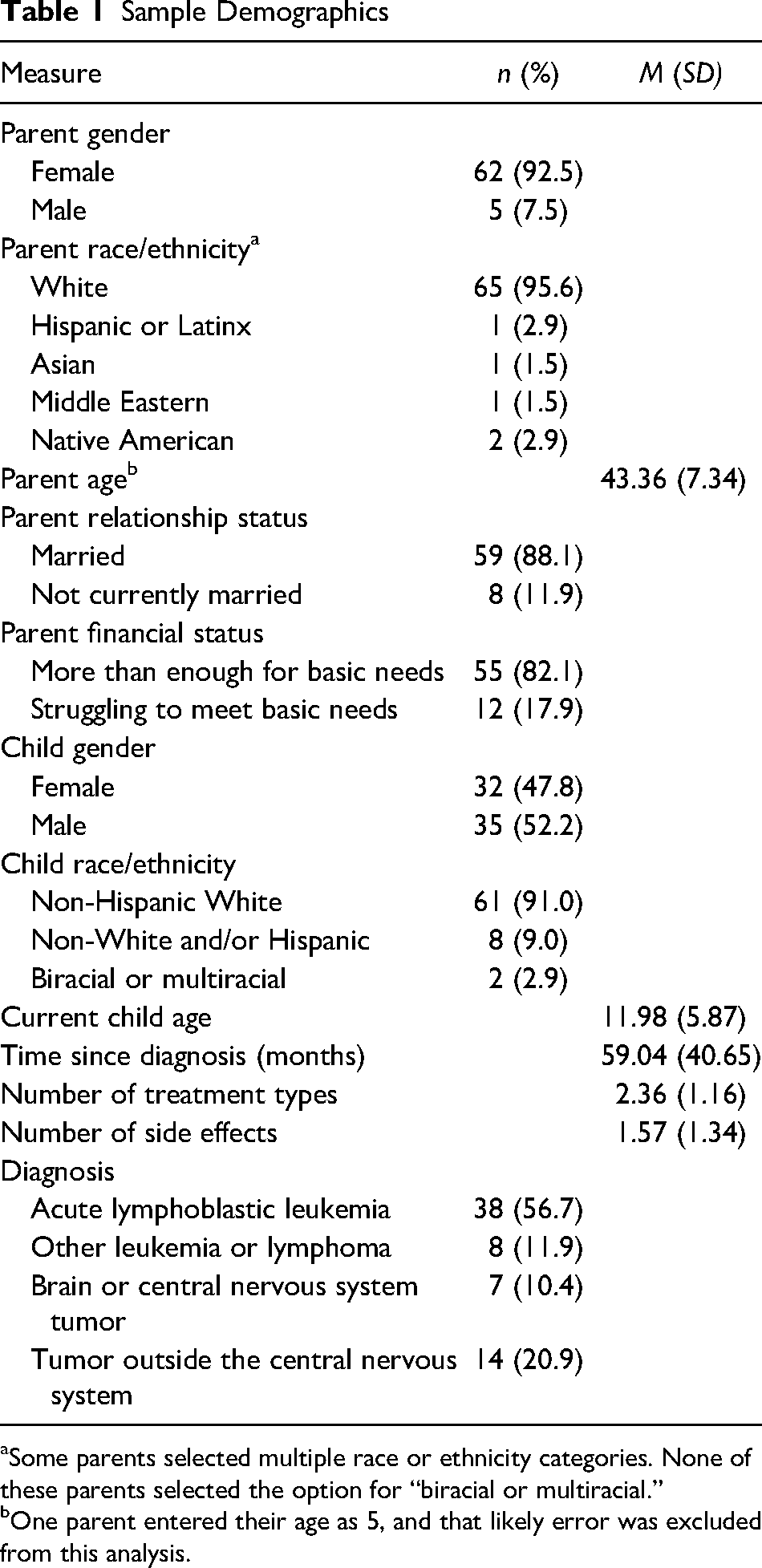
Some parents selected multiple race or ethnicity categories. None of these parents selected the option for “biracial or multiracial.”
One parent entered their age as 5, and that likely error was excluded from this analysis.
Complete responders (n = 53) and partial responders (n = 14) did not differ significantly in paired sample t tests of means of study variables. More diagnosed children were posttreatment (n = 53) than in treatment (n = 8) or deceased (n = 6). Although these three subgroups differed significantly on some variables, none of the outcomes that included these variables had different results when analyzed using the whole sample compared to posttreatment parents only. Accordingly, the full sample was used to preserve power.
Descriptive Statistics
Most parents (76.1%) reported that their child had experienced at least one long-term physical, cognitive, or emotional side-effect from cancer treatment (M = 1.54, SD = 1.34) and children generally received multiple treatment modalities (M = 2.32, SD = 1.19). The high reported rate of long-term side effects is consistent with evidence documenting near-universal chronic health concerns among adult survivors of pediatric cancer (Bhakta et al., 2017).
Of the three coping styles measured with the COPE, parents reported using active coping the most with scores ranging from 22 to 47. Socially supported/emotion-focused coping which had scores ranging from 19 to 48, was used more than avoidant coping, which had scores ranging from 12 to 33. These findings are similar to previously reported findings on how parents of children with cancer employ various coping styles; active coping is used the most, followed by socially supported/emotion-focused coping, and then avoidant coping (Turner-Sack et al., 2016).
A significant minority of parents (38.7%) endorsed clinically significant depression on the PHQ-9 as evidenced by scores of at least 10 (Manea et al., 2012). Additionally, 10 parents (18.9%) endorsed experiencing thoughts of suicide or self-harm at least once during the 2 weeks prior to completing the survey. Parents generally reported moderate to high levels of general hopefulness on the AHS, with scores ranging from 15 to 32. See Table 2 for means and standard deviations of measure scores.
Means and Standard Deviations of Scores on Study Measures
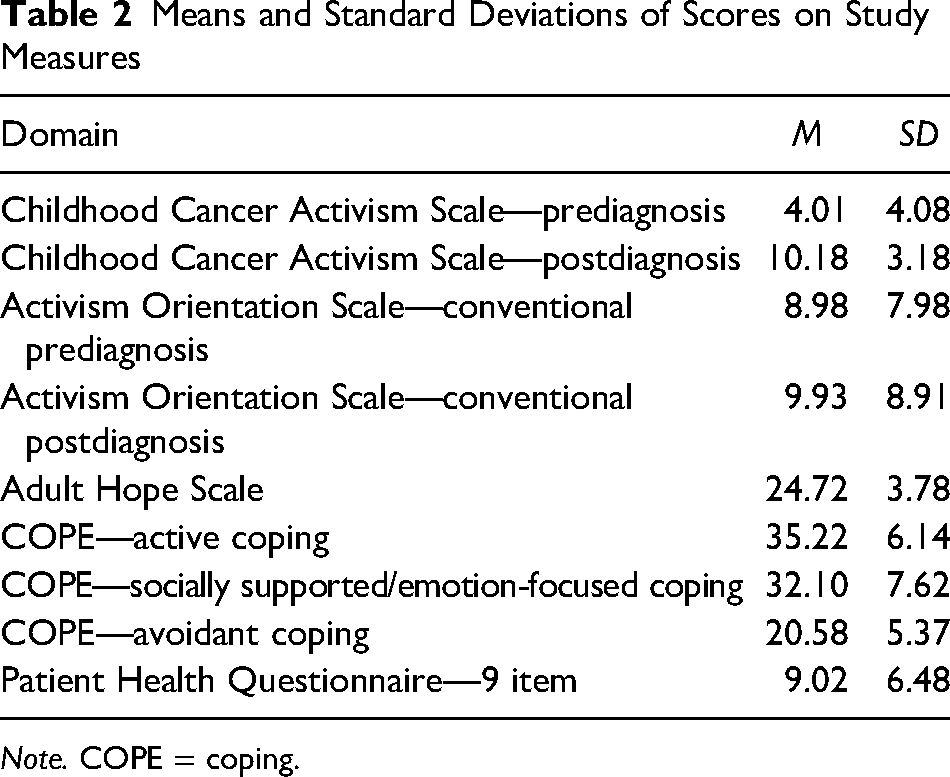
Note. COPE = coping.
Changes in Activism Following Diagnosis
For childhood-cancer-related activism (N = 67), postdiagnosis engagement (M = 10.18) was significantly higher, t(66) = 11.57, p < .001, d = 1.41, 95% CI [1.07, 1.75], than prediagnosis engagement (M = 4.01). For general activism (n = 55), postdiagnosis engagement (M = 9.93) was not significantly different, t(54) = 1.31, p = .195, d = 0.18, CI [−0.09, 0.44], from prediagnosis engagement (M = 8.98). Notably, 100% of participants engaged in at least three childhood-cancer-related activism behaviors following diagnosis, compared to 54% of participants who did so prediagnosis. See Figure 2 for the full list of forms of childhood-cancer-related activism and the percentage of participants who endorsed each one pre- and postdiagnosis.
Correlations Between Activism, Coping, Hopefulness, and Depression
Postdiagnosis childhood-cancer-related activism was positively correlated with hopefulness (r = .46, p < .001) and active coping (r = .50, p < .001), but negatively correlated with avoidant coping (r = −.28, p = .030). Postdiagnosis childhood-cancer-related activism was not significantly associated with socially supported/emotion-focused coping (r = .13, p = .32) or depression (r = −.19, p = .16).
Predictors of Activism and Hopefulness
Participants who completed the COPE (n = 60) were included in a regression analysis to assess predictors of postdiagnosis childhood-cancer-related activism. Higher levels of postdiagnosis childhood-cancer-related activism were uniquely predicted by treatment variables (side effects and treatment types, combined) and higher levels of active coping. Socially supported/emotion-focused coping was not included in the regression model due to a lack of association with postdiagnosis childhood-cancer-related activism. The entire model accounted for 31% of the variance in activism (Table 3).
Predicting Activism From Treatment Variables and Coping Styles
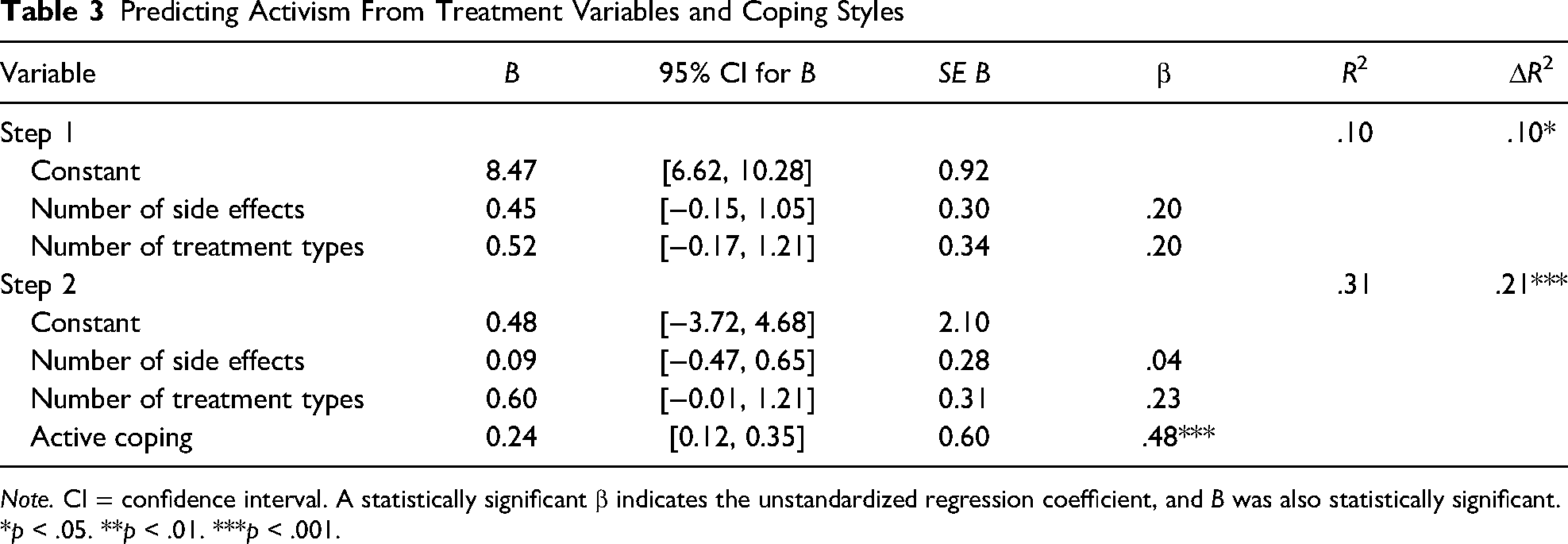
Note. CI = confidence interval. A statistically significant β indicates the unstandardized regression coefficient, and B was also statistically significant.
*p < .05. **p < .01. ***p < .001.
Participants who completed all activism measures (n = 55) were included in a second regression analysis to assess predictors of hopefulness. Higher levels of hope were uniquely predicted by the level of postdiagnosis childhood-cancer-related activism after accounting for parental demographic factors (age, gender, and ethnicity), prediagnosis childhood-cancer-related activism, and postdiagnosis general activism. The entire model accounted for 33% of the variance in hopefulness (Table 4).
Predicting Hopefulness From Activism Engagement
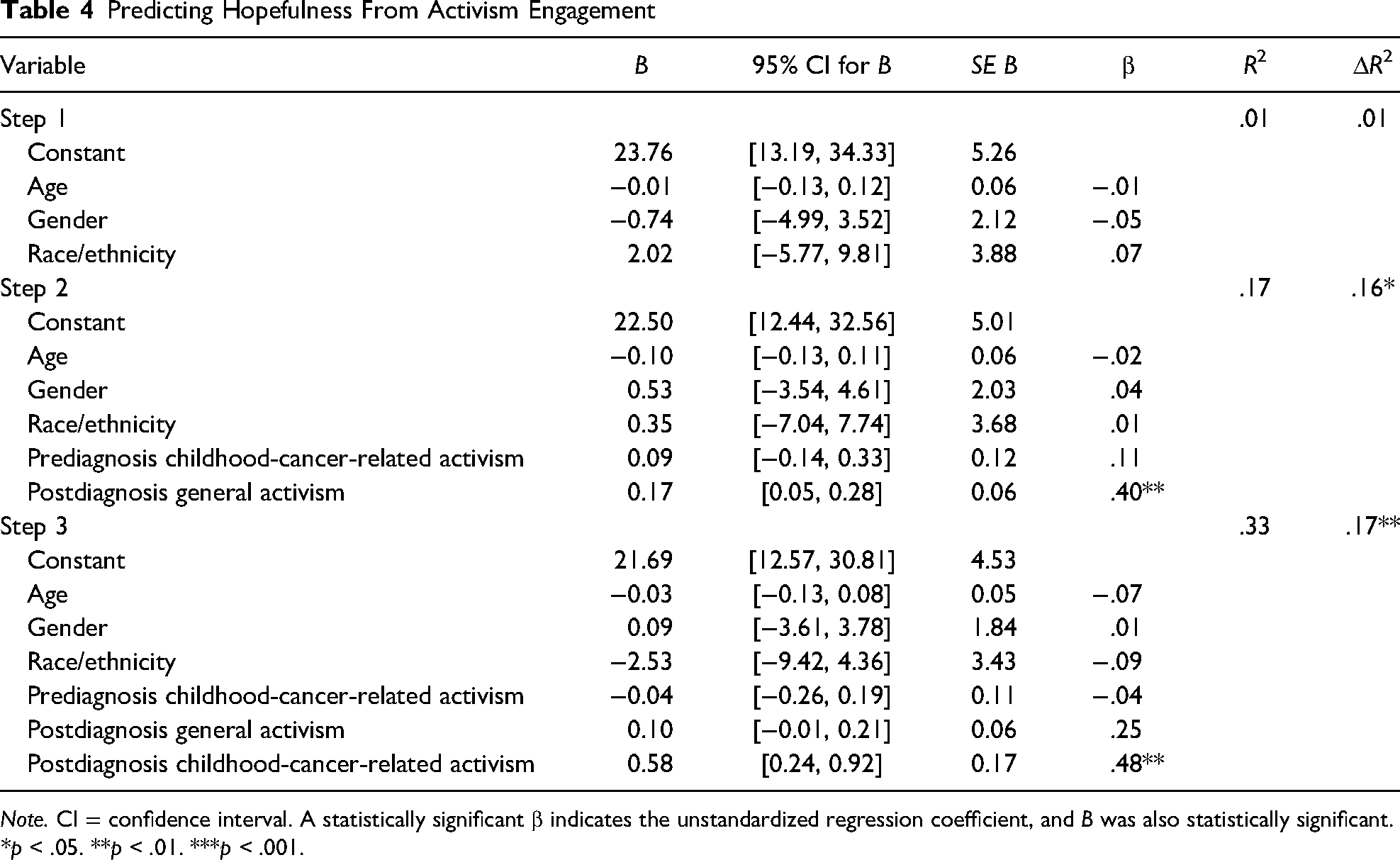
Note. CI = confidence interval. A statistically significant β indicates the unstandardized regression coefficient, and B was also statistically significant.
*p < .05. **p < .01. ***p < .001.
Discussion
Summary and Contributions
The current study, to our knowledge, is the first to investigate activism, both general and cancer-specific, among parents of children with cancer as a primary variable of interest, as well as the first to measure activism quantitatively. Parents universally reported engaging in at least three childhood-cancer-related activism behaviors following their own child's diagnosis, compared to roughly half of the parents who did so prediagnosis. Overall, participants reported that engagement in childhood-cancer-related activism more than doubled following their own child's diagnosis. Given that parents routinely describe the childhood cancer experience as disorienting and overwhelming (Long & Marsland, 2011), it is notable that participants reported such a marked increase in activism behaviors in the face of intense caregiving demands. These findings suggest that activism is both a feasible and desirable activity for parents of children with cancer to engage in.
More treatment types and side effects (collectively) and higher levels of active coping both predicted higher rates of activism. Each of these findings suggests that parents who endorse that their child had a more intense cancer experience are more likely to be highly engaged in activism. In other words, parents who report a higher number of treatment types and side effects throughout their child's cancer treatment are likely to have spent more time and energy helping their child cope with their condition, and such efforts broadly represent active coping. Treatment-related influences on activism engagement are particularly relevant given that a key goal of childhood-cancer-related activism is to improve medical treatments and outcomes for children with cancer (Smith & Hoffman, 2016). Families who have a child with high exposure to cancer treatments and side effects are likely disproportionately burdened by the cancer experience, and the current findings indicate that parents of these children may be particularly motivated to support other children with cancer on a broader scale.
Activism participation was not correlated with socially supported/emotion-focused coping or with depression in the current study. Although activism inherently involves interacting with others to raise awareness for a valued cause, further research is needed to understand whether activism may function as an opportunity to give or receive social support. Similarly, although activism engagement was positively correlated with hopefulness, it is unclear why high activism engagement was not correlated with reduced depression. The findings highlight the nuanced psychosocial support needs of parents of children with cancer.
Overall activism engagement on behalf of any cause accounted for over 30% of the variance in parental hopefulness, with postdiagnosis childhood cancer activism alone accounting for 17% of the variance in parental hopefulness. Prior literature has established the indispensable nature of hope for maintaining resilience in the face of childhood cancer (Conway et al., 2017; Germann et al., 2015; Kamihara et al., 2015). Parental hope may fluctuate as a function of their own child's health, creating a need for ways to support parental hope throughout the illness trajectory (Barrera et al., 2013). Outcomes that extend beyond the survival of one's own child are particularly important for parents of children with advanced cancer (Kamihara et al., 2015) and may spur resilience and the ability to make meaning of tragedy. Findings from the current study add to the existing hope literature by identifying hope for other children with cancer as a way that parents can continue to honor their child in a healthy manner, whether or not their child survives. Activism is a behavioral coping strategy that may promote hopefulness and effective coping for parents of children with cancer, and this possibility should be explored in future research.
Limitations
The contributions of the current study must be understood in the context of its limitations. An important methodological limitation is that only retrospective reports of activism were used, so causal relationships between activism and other variables cannot be defined. It also cannot be verified that self-reports of activism behavior reflect parents’ actual engagement in activism with complete accuracy. Similarly, the online recruitment method, which included a donation-based incentive, may have yielded a sample with elevated rates of activism given that participation itself could be considered a form of activism. However, the overall reliability of the CCAS and the robust effect size of the increase between pre- and postdiagnosis childhood-cancer-related activism support the claim that a meaningful increase in activism after diagnosis did, in fact, take place.
Significant homogeneity in family demographics indicative of various forms of privilege limits the generalizability of these findings to all parents of children with cancer. Participants were predominantly White, female, married caregivers who may have greater support to participate in activism opportunities compared to other populations. The current study also did not explicitly address health disparities unique to children with cancer who are exposed to stressors such as poverty or racism (Beltrami et al., 2022). Further research is needed to better understand activism experiences that support the needs of children with these intersecting identities. Due to the exploratory nature of the current study, the sample included parents of children at a wide range of treatment stages, including bereaved parents. Given that the current findings indicate that activism may be both a common behavior and salient to parental hopefulness, further prospective research should address whether these findings are typical across all parents of children with cancer and how activism may change across the treatment trajectory.
Implications
The current study has significant implications for nursing professionals regarding the clinical care of children with cancer and their parents. Parental activism serves as a reminder to providers that the burden of childhood cancer remains untenable despite increased survival rates, and providers should be mindful of ways they can support parental initiatives to reduce this burden. That parents are willing to take on the task of activism alongside the challenge of caring for a child with cancer speaks to the urgency with which parents seek improved treatment processes and outcomes for diagnosed children. Additionally, providers should be aware that activism is a highly prevalent practice associated with the cancer experience that may have positive correlates for families in ways we have only begun to explore. Nursing staff are uniquely positioned to support families during acutely difficult phases of children's cancer trajectories, and activism may offer an opportunity to promote effective coping with these experiences.
Importantly, although participants in the current study were generally both hopeful and highly engaged in activism, PHQ-9 scores indicate that this sample still experienced moderate levels of depression. This finding underscores the need for long-term psychosocial support and informed care for children with cancer and their families, which has already been identified as a standard of care (Lown et al., 2015). Similarly, this finding indicates that even parents who are engaged in positive coping strategies may benefit from additional support from nursing staff. Such support may include validating parents’ efforts to support other children with cancer, offering space to process feelings of sadness or frustration that may arise from activism experiences, and referring families to mental health services when persistent distress is present.
Future Directions
The relevance of activism for other family members, such as siblings, and diagnosed children themselves should be explored given the known relationships between coping and distress among parents and children in the context of pediatric cancer (Bakula et al., 2019). Additionally, activism-based interventions should be explored as a potential means of fostering hope among parents of children with cancer, given the positive correlations observed in the current study. Attention should be paid to ensuring that such research includes sufficient diversity with regard to race/ethnicity and socioeconomic status, as these may influence the degree to which activism is beneficial for a given family without further depleting their resources. Such research should also be mindful of parental distress and explore potential burdens of activism engagement given that activism was not associated with lower depression in the current study. Overall, activism appears to be a common activity among parents of children with cancer, and providers should work to identify and promote appropriate and effective opportunities for parents to engage in it in an empowering manner.
Footnotes
Acknowledgments
The authors would like to thank (Eastern Michigan University) University Writing Center for support with formatting during manuscript preparation.
Author Note
Flora Hoodin is also affiliated with Department of Psychiatry, University of Michigan, Ann Arbor, MI, USA.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
Authors disclose the following financial support: This research was made possible in part by a small financial grant ($400) from the (Eastern Michigan University) Department of Psychology.