
Abstract
Keywords
Specific knowledge is required in the field of pediatric oncology, and specialization of nurses was identified in 1994, and later in the World Health Organization (WHO) Global Initiative for Childhood Cancer, as a nursing priority (Hinds et al., 1994; Pergert et al., 2020). Furthermore, continuing education is a baseline standard for pediatric oncology nursing globally (Day et al., 2014).
In many countries, including Sweden, specialist education is offered in oncology and pediatrics, but international research has shown that there is a lack of opportunities for much-needed sub-specialization in pediatric oncology (Sullivan et al., 2020). Continuing education for nurses is essential to enable nurses to develop their clinical practice, to perform nursing research, and to lead education and training (Hollis, 2005). A pediatric oncology nurse is expected to provide care in accordance with evidence-based nursing. There is a need to implement evidence-based research results into practice (Linder, 2021). Yet due to vague and hard-to-interpret results, most nursing research is still not implemented (Enskär et al., 2015). To be able to implement the practice of evidence-based nursing in pediatric oncology, there is a need for education on evaluation and research (Cline et al., 2019).
In clinical pediatric oncology nursing, the practice must incorporate both the science and the art of the discipline to enhance positive physical and psychosocial outcomes for patients (Cantrell, 2007; Enskär, 2012). Research has shown a positive association between the educational level of nurses and patient outcomes (Aiken et al., 2014). Every 10% increase in nurses holding a bachelor's degree was associated with a 7% decreased risk of dying (Aiken et al., 2014) and an average reduction of 7.47 deaths per 1,000 patients with complications (Kutney-Lee et al., 2009).
In a research review, educational level was identified as a component associated with job satisfaction that could influence a nurse's intention to leave (Coomber & Barriball, 2007). Furthermore, previous studies have reported that when nurses received new knowledge and specialization through education, their perceptions of personal growth, satisfaction, autonomy, and confidence increased (Enskär, 2012; Garrison et al., 2018). In addition, gaining increased knowledge and autonomy may enhance personal initiative, which can add to job satisfaction (Kagan et al., 2021).
In Sweden, nursing education has undergone major changes in recent decades. In 1993, basic nursing education was formalized into an academic educational program including a bachelor's degree. Through the European cooperation and the Bologna Process, a three-level higher education system was implemented in 2007 through amendments (SFS, 2006:1053) to the Ordinance of Higher Education (National Agency for Higher Education, 1993:100). The three levels of education are basic (bachelor's), advanced (master's), and research (doctoral) (European Commission, 2018). Thus, nursing specialist education in Sweden today is on the advanced level (60 higher education credits) and includes a 1-year master's degree. However, nurses who studied before the implemented changes might still lack these academic degrees.
A 2-year national educational program in pediatric oncology nursing has been offered in Sweden since 2003. Initially, it was offered at Gothenburg University and comprised 45 credits. Since 2012, it has been offered at Karolinska Institutet and comprises 30 credits. It is the only university program in pediatric oncology care for nurses in Sweden. The teaching is carried out by nurses, physicians, researchers, and other professionals who are considered to be the best in the country in their subject area. The education is on the advanced level of study and is aimed at nurses who care for children with cancer, at pediatric oncology centers, or at shared care wards/hospitals. Nurses with an earlier education, without an academic degree, have also been accepted. The employers (nursing managers) select interested nurses who may apply and who are granted paid study leave. The program is offered by the university as “contract education” funded by the Swedish Childhood Cancer Fund. The aim is to give nurses the opportunity to acquire in-depth knowledge and expertise in pediatric oncology (10 credits) and nursing care of children with cancer (20 credits), including practice-integrated learning. Thus, topics are covered from both a nursing and a medical perspective and these are integrated as much as possible.
The aim is also to retain nurses and improve pediatric oncology care. In a previous evaluation of the three first cohorts (2003–2010) of the program, a total of 54 of the 66 graduated nurses participated. None of the participants who at the start of the education were working at pediatric oncology centers (33/54) had left pediatric care (Pergert et al., 2016). Almost all (53/54, 98%) participants stated that they were more secure in their work after the education (Pergert et al., 2016). The education gave the nurses higher self-confidence and was an important step in their becoming experts in clinical practice (Enskär, 2012; Pergert et al., 2016). Furthermore, they perceived that they were better equipped to deal with the advanced and highly specialized care necessary in pediatric oncology (Pergert et al., 2016).
Three more cohorts graduated from the national educational program in pediatric oncology nursing between 2012 and 2019. The aim of this study was to gain knowledge of the impact of the national educational program in pediatric oncology nursing, from the perspective of nurses in the three cohorts.
The specific research questions include:
How many have left pediatric oncology and what were the reasons for leaving? Have the nurses’ positions changed? How many nurses have academic degrees, and are there differences between groups? What are nurses’ perceptions about their importance in the multidisciplinary team and being listened to, and are there differences between groups? To what extent do nurses use the network and keep up to date on healthcare research, and are there differences between groups? To what extent are nurses involved in training, quality improvement work, and healthcare research, and are there differences between groups?
Methods
In this cross-sectional study, a study-specific questionnaire was used to explore the perceptions of nurses who completed the educational program.
Sampling and Participants
The total number of graduates in the three cohorts of the national educational program offered at Karolinska Institutet was 82 (2012–2014, n = 23; 2015–2017, n = 27; 2017–2019, n = 32) nurses. Lists of the graduates of the educational program were available at the university. Current email addresses were procured from various contacts, such as the local clinical lecturer working at the six pediatric oncology centers. All graduates, except two, in these cohorts, were invited to participate in the study. One graduate's contact information could not be found, and one graduate was a member of the evaluation team and thus excluded.
Data Collection
A study-specific questionnaire, constructed for an evaluation of previous cohorts of the educational program offered at Gothenburg University (Pergert et al., 2016), was developed and extended with additional questions. Five cognitive interviews in the form of think-aloud interviews were conducted to test the functional level of the questionnaire (Collins, 2014). The interviews were conducted with nurses in pediatric oncology, of whom three were students in the current cohort of the educational program (2019–2021) at Karolinska Institutet. This resulted in minor re-formulations of a few items. The questions concern the working experience at the start of the education; past and present position; current work situation and tasks; how the education had affected their professional practice and work situation; as well as questions to those who had left pediatric oncology (why they left and what would make them want to come back). Some questions have the response alternatives Yes or No, and some a 4-point Likert-type scale including not at all (0), to a small extent (1), to a fairly large extent (2), and to a large extent (3). The question about reasons for leaving pediatric oncology includes 12 response alternatives including “Other.”
A link to the electronic questionnaire in the Artologik Survey & Report, Version 4.3 (Artisan Global Media) was sent by email to potential participants. Data collection was performed between March 30 and May 17, 2021, and three reminders were sent via Artologik Survey & Report to those who had not yet answered the questionnaire. When data collection was closed, the data was transferred to IBM SPSS Statistics for Windows, Version 28.0.
Data Analysis
All statistical calculations were conducted using SPSS Statistics, including descriptive statistics (such as frequency and percentage). The differences between groups were evaluated using Pearson's chi-squared test. The compared groups included centers versus shared care wards/hospitals and groups based on years of experience in pediatric oncology (<5, 5–10, >10 years). Associations were measured using Spearman's rank-order correlation. p-values below .05 were considered statistically significant.
Ethical Considerations
The graduates of the program received an invitation via email to participate in the study and an information letter describing the aim of the study and stating that participation was voluntary. Participants had to confirm that they had read and accepted the terms and conditions to get access to the questionnaire. The questionnaire was answered anonymously, and the number of background questions was minimized to protect the participants’ privacy. For example, there were no questions about gender because of the few male participants in the educational program. The Swedish Ethical Review Authority (2021-00391) gave an advisory statement and had no ethical objections to the study.
Results
Eighty nurses who completed the program were invited to participate and 59 (74%) responded. The number of participants from each cohort were: 2012–2014, 13/22 (59%); 2015–2017, 23/26 (88%); 2017–2019, 22/32 (69%). At the start of the education, more than half of the participants (33/59, 56%), in all three cohorts, were working at pediatric oncology centers (Table 1). Most of the participants had been working as nurses for more than 10 years (77%) and almost half (44%) had more than 10 years of experience in pediatric oncology (Table 1). In the third cohort, 91% of the participants had been working for more than 10 years as nurses and half of them had more than 10 years in pediatric oncology (Table 1).
Characteristics of the Participants in the Three Cohorts of the Education
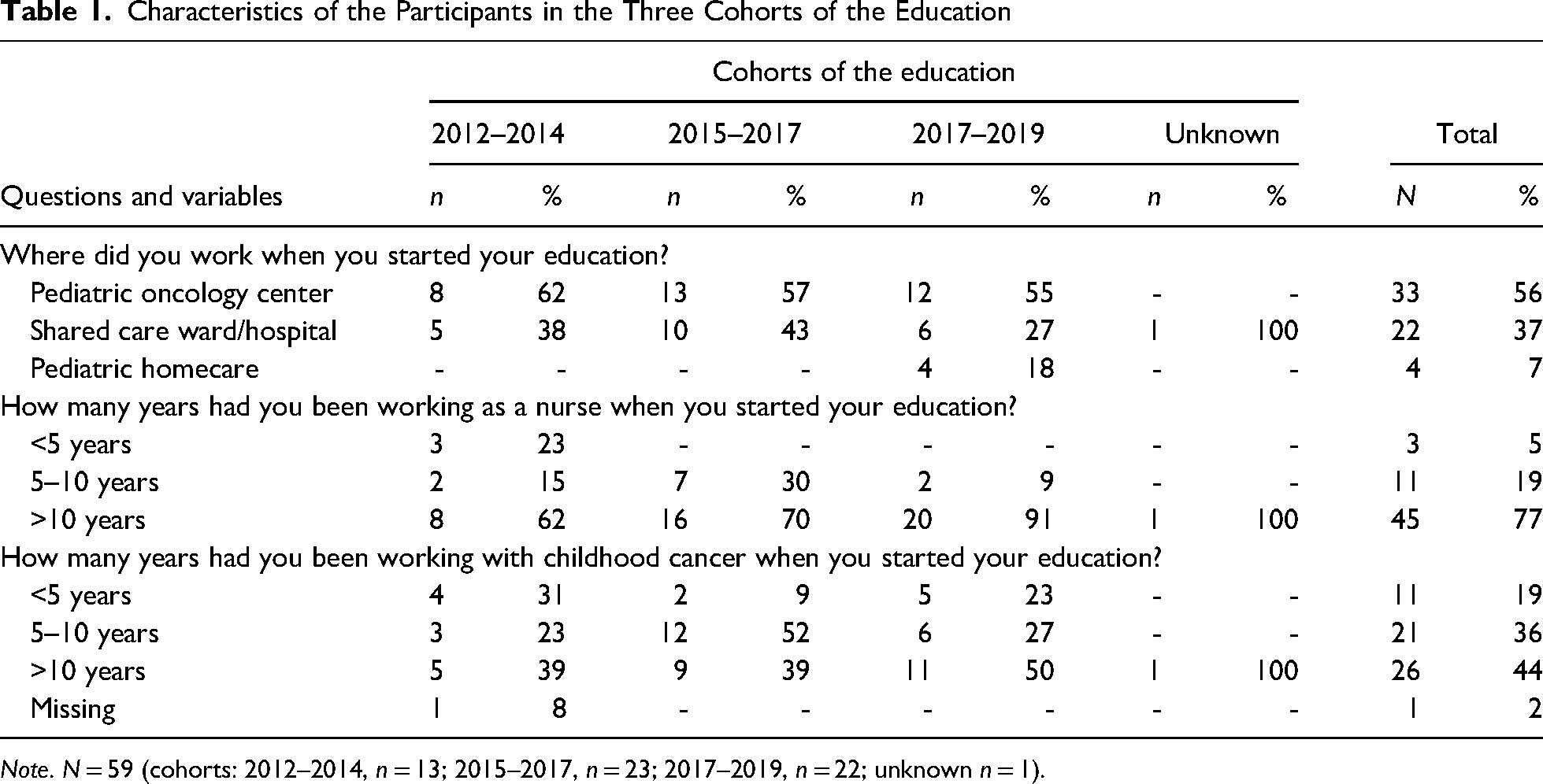
Note. N = 59 (cohorts: 2012–2014, n = 13; 2015–2017, n = 23; 2017–2019, n = 22; unknown n = 1).
A total of 21 graduates did not respond, of whom 10 (52%) were working at a pediatric oncology center when they started their education and 11 (48%) at a shared care ward/hospital. To the question of whether they would recommend the program to their colleagues in pediatric oncology, 90% of the 59 participants responded that they would to a large extent and 8% to a fairly large extent.
Participants Who Had Left Pediatric Oncology
Out of the 59 participants, 15 (25%) had left pediatric oncology care. These 15 nurses were asked to choose the three most important reasons for leaving pediatric oncology, although some gave more/fewer reasons. A total of 46 responses to this question were provided. The stated important reasons for leaving pediatric oncology have been divided into three categories: “Poor working environment” 21/46 (46%), “Career and appreciation” 12/46 (26%), and “Life situation” 13/46 (28%). The most common important reasons for leaving pediatric oncology were related to “poor working environment” (Table 2). The poor working environment was mainly related to the organization and the management, and never related to the patient/family. In the category “Career and appreciation,” the most frequently indicated reason was “Low salary/deficient benefits.” “Working hours did not suit me” was the most selected reason in the “Life situation” and the most common reason of all (Table 2).
Reasons for Leaving Pediatric Oncology Care
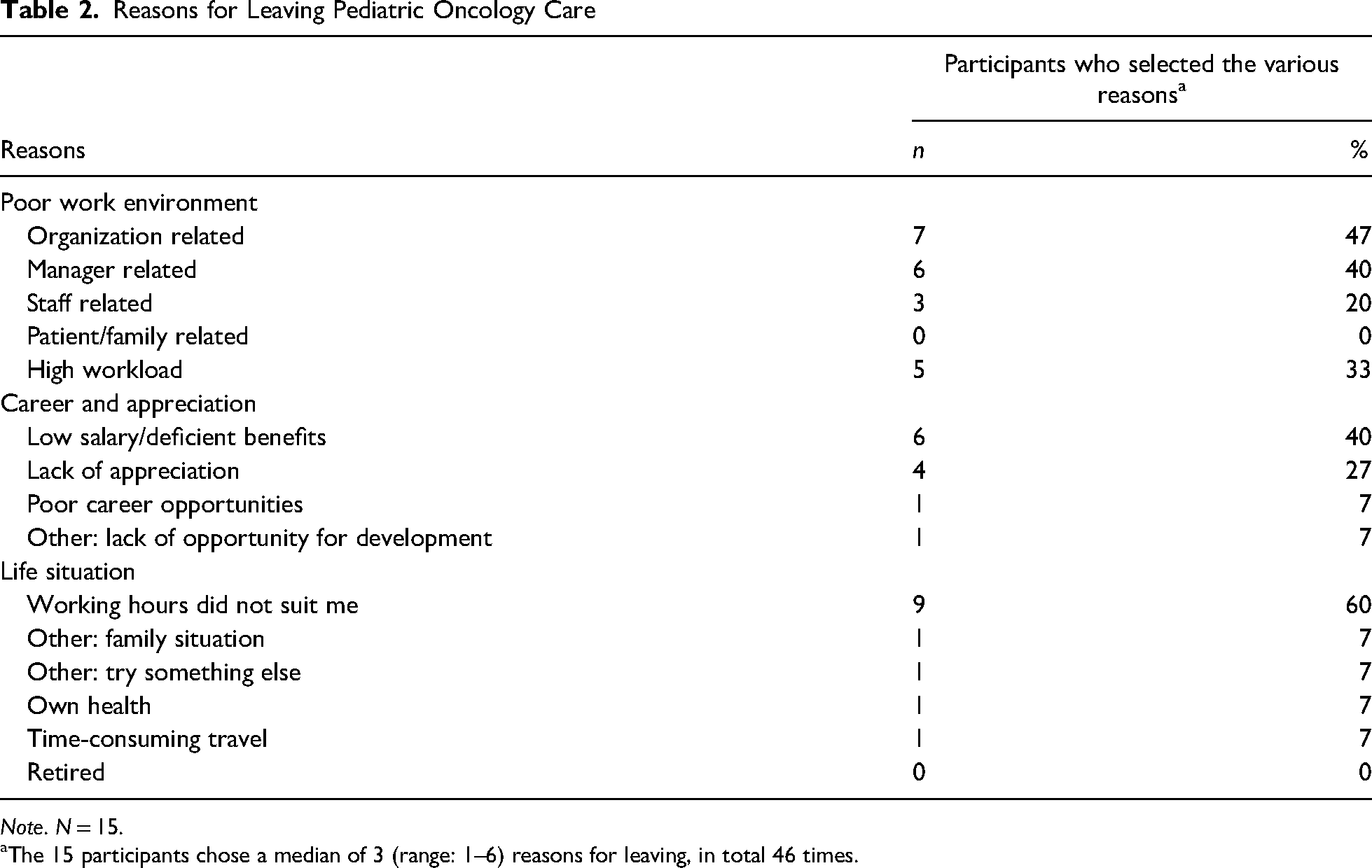
Note. N = 15.
The 15 participants chose a median of 3 (range: 1–6) reasons for leaving, in total 46 times.
Positions Before and After the Education
There were significant (p = .001) differences in positions at the start of the education and when answering the survey. At the start of their education, nine (20%) nurses held special positions as consultant, contact, coordination, or research nurses (Figure 1). The number of nurses with special positions 2 to 7 years after completing the education, increased to 26 (59%), including two (4%) who had become managers. At the start of the education, most nurses (37/44, 84%) were working bedside, of which two combined this with a special position. At the time of the survey, 31 (71%) nurses were working bedside, including 13 (30%) combining this with a special position.
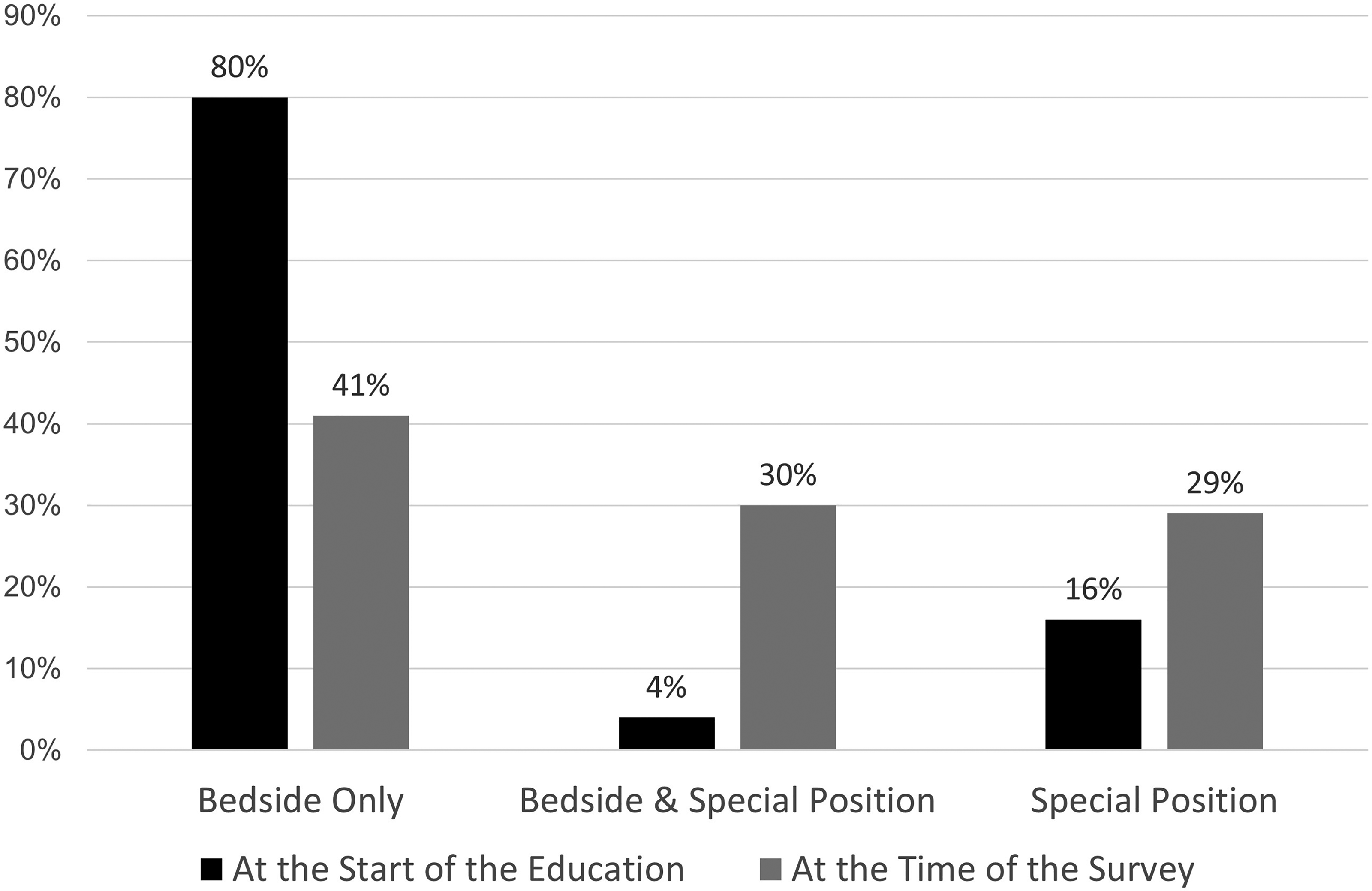
Participants’ positions at the start of the education and when answering the survey.
Academic Degree
There was a significant difference (p = .026) in academic degrees between nurses working at pediatric oncology centers and nurses at shared care wards/hospitals, as a larger proportion of nurses at centers had a master's degree (1 or 2 years) and a larger proportion of nurses at shared care wards/hospitals had no academic degree (Table 3). There were no correlations between academic degree and position at the time of the survey.
The Highest Academic Degree of the Participants Divided by Workplace
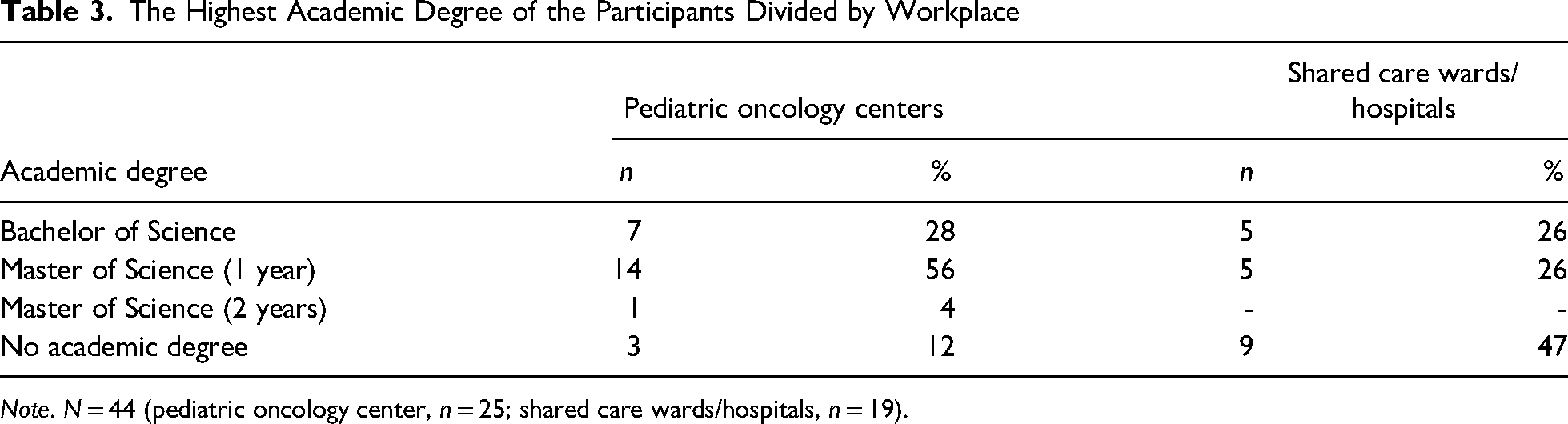
Note. N = 44 (pediatric oncology center, n = 25; shared care wards/hospitals, n = 19).
Knowledge From the Education
The vast majority (39/44, 89%) stated that the knowledge from their education had helped them in their work to a fairly large/large extent. Furthermore, the participants (39/44, 89%) perceived that the knowledge from the education to a fairly large/large extent contributed to them becoming more confident in their encounters with the patient/family.
Importance in the Multidisciplinary Team and Being Listened to
Most of the nurses with 5 years of experience or more in pediatric oncology perceived that they to a large extent were considered important in the multidisciplinary team, and that nurses and parents listened to and valued their knowledge (Table 4). All except two perceived that the physicians listened to a fairly large/large extent. None of the nurses perceived that the parents to no/small extent listened to them. There was a significant difference in the numbers of nurses who to a large extent perceived that the parents listened and valued their knowledge, between those with less than 5 years of experience and those with 5 years or more (Table 4).
Perceptions Regarding Importance in the Multidisciplinary Team and Being Listened to, Divided by Years of Experience From Pediatric Oncology
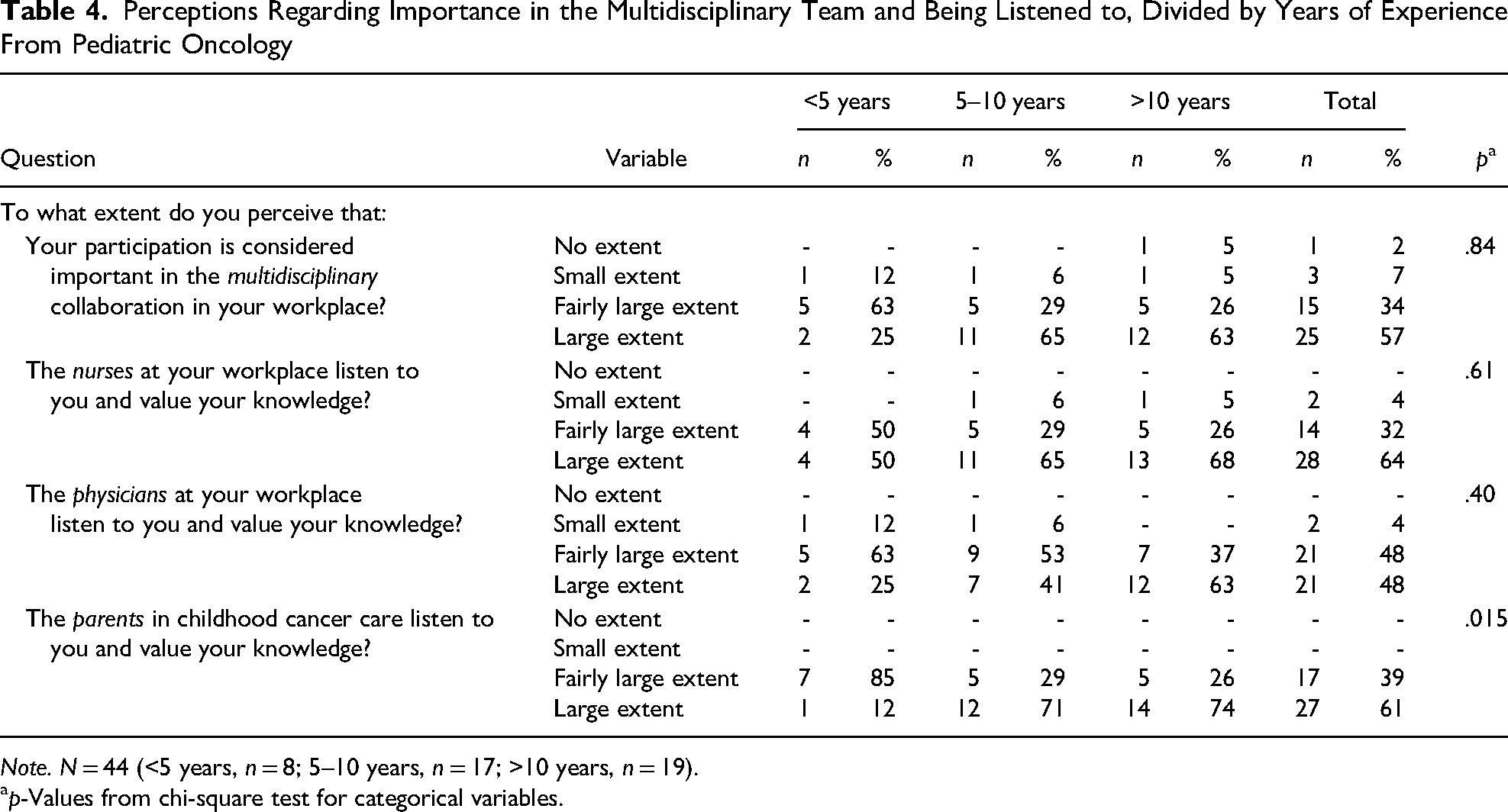
Note. N = 44 (<5 years, n = 8; 5–10 years, n = 17; >10 years, n = 19).
p-Values from chi-square test for categorical variables.
After the education, a larger proportion of the nurses at pediatric oncology centers than the nurses at shared care wards/hospitals perceived that their participation in the multidisciplinary team was considered important and that nurses, physicians, and parents listened to and valued their knowledge (Table 5). This difference was significant regarding parents. Less than half of the nurses at shared care wards/hospitals perceived that their participation in the multidisciplinary team was considered important and that physicians and parents listened to and valued their knowledge (Table 5).
Positive Answers (Large Extent) Regarding Importance in the Multidisciplinary Team and Being Listened to, Divided by Workplace
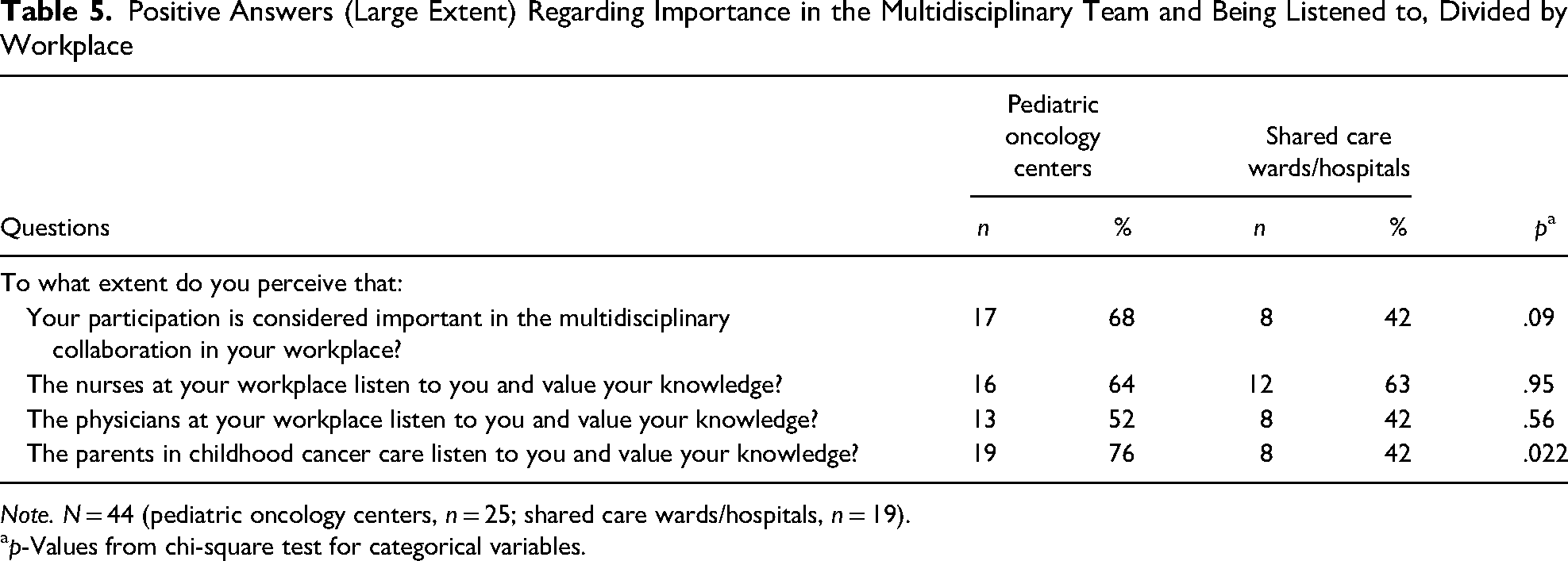
Note. N = 44 (pediatric oncology centers, n = 25; shared care wards/hospitals, n = 19).
p-Values from chi-square test for categorical variables.
Use of Network and Keeping Up to Date on Healthcare Science Studies
Half of the nurses (22/44, 50%) answered that they had used the national pediatric oncology network from the program to a fairly large/large extent. Participants working at pediatric oncology centers used the national network to a higher extent than nurses from shared care wards/hospitals (Table 6). Participants with 5 years of experience or more used the national network to a significantly higher extent (p = .019) than nurses with less experience. There were significant correlations between the position at the time of the survey and using the network, r(42) = .57, p = .001.
Positive Answers (Fairly Large/Large Extent) Regarding Network, Knowledge, Training, Quality Improvement Work, and Healthcare Science Research, Divided by Workplace
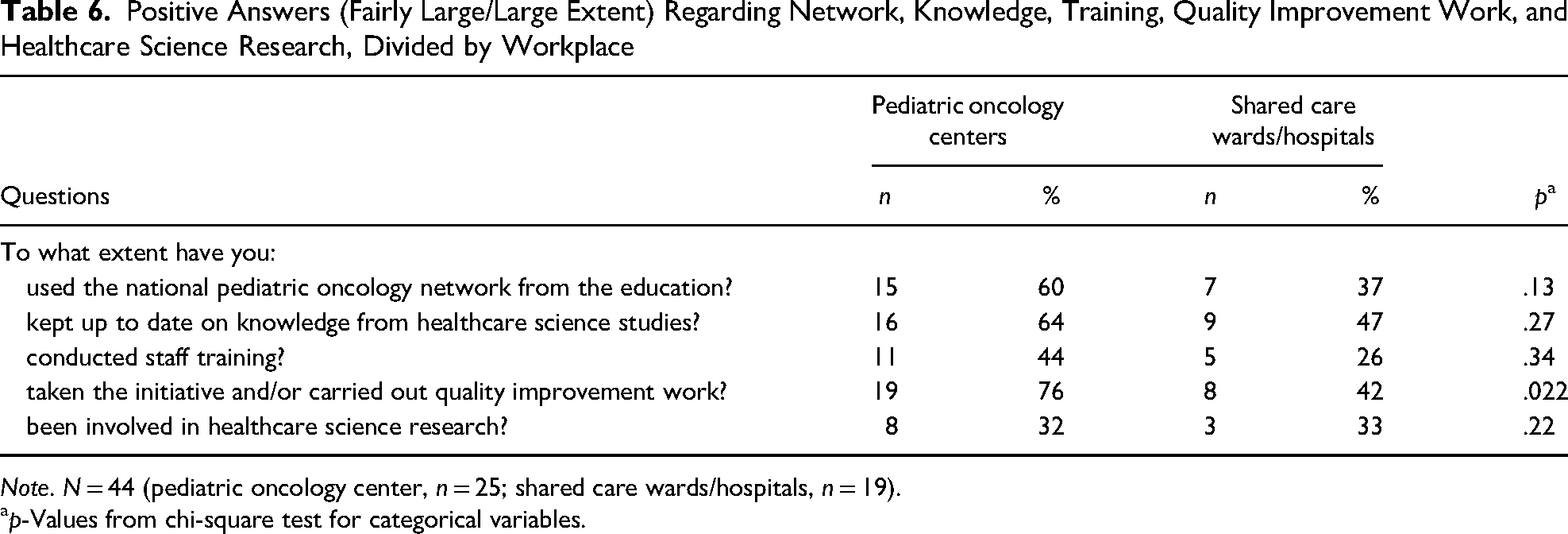
Note. N = 44 (pediatric oncology center, n = 25; shared care wards/hospitals, n = 19).
p-Values from chi-square test for categorical variables.
More than half of the nurses (25/44, 57%) stated that they had kept up to date with knowledge from healthcare research to a fairly large/large extent. Participants working at pediatric oncology centers kept up to date on knowledge to a higher extent than nurses from shared care wards/hospitals (Table 6). There was no difference related to years of experience in pediatric oncology. Furthermore, there were no correlations between academic degrees and keeping up to date on knowledge.
Involvement in Training, Quality Improvement, and Research
Of the 44 nurses, 16 (36%) answered that they, to a fairly large/large extent, conducted staff training. More than half of the nurses (27/44, 61%) stated that they, to a fairly large/large extent, had taken the initiative and/or carried out quality improvement work, and 11 (25%) had been involved in healthcare research. Nurses at pediatric oncology centers were more involved in staff training, and significantly more involved in quality improvement work. However, there was no difference regarding healthcare research, in which a third of the participants were involved (Table 6). Furthermore, there were no differences between participants with more or less than 5 years of experience in pediatric oncology in involvement in staff training, quality improvements, and research. There were no correlations between academic degree and involvement in research, training, and quality improvements. However, there were significant correlations between the position at the time of the survey and involvement in quality improvement work, r(42) = .53, p = .001, and involvement in training r(40) = .43, p = .005.
Discussion
In this evaluation of the Swedish national educational program in pediatric oncology, nearly all the participants would, to a fairly large/large extent, recommend the education to their colleagues in pediatric oncology. Most of the participants had extensive working experience prior to entering the educational program. Seventy-five percent of the nurses were still working in pediatric oncology. The reasons for leaving among the 25% who had left were mainly related to the poor working environment, and the most-stated single reason was unsuitable working hours in the category “life situation.” After the program, the number of nurses with a special position increased and many combined it with bedside work. The vast majority stated that the knowledge from the education helped them in their work and contributed to increased confidence in their interactions with patients and their families. Compared with nurses at shared care wards/hospitals, nurses at pediatric oncology centers to a larger extent perceived that parents listened to and valued their knowledge, and they were to a larger extent involved in quality improvement work. It is reasonable to assume that parents may perceive nurses at shared care wards/hospitals as less specialized in pediatric oncology because most of the patients they care for have non-oncological diseases. It has previously been reported that parents perceive nurses at the center as the real experts and that they have concerns regarding the expertise of nurses at the shared care wards/hospitals (Sepion, 2004).
Nurse retention is one of the goals of offering an educational program in pediatric oncology (Swedish Childhood Cancer Fund, 2016). The majority of participants were still working in pediatric oncology at the time of the evaluation, 2 to 7 years after completing the educational program. Previous research presents contradictory results regarding the association between attained educational level, job satisfaction, and the intention to leave (Coomber & Barriball, 2007). To work in pediatrics, including pediatric oncology, a degree as a nurse specialist in pediatrics is warranted. However, having a specialist degree also increases the risk of the nurse leaving highly specialized inpatient care for a position as, for example, a school nurse with a higher salary and daytime hours. This education gives increased opportunities for career development within pediatric oncology and is thus likely to increase the retention of nurses. However, it is not enough to just educate nurses (Coomber & Barriball, 2007) since 25% of the nurses had left pediatric oncology care after the education, a number in line with an earlier evaluation in Sweden (Pergert et al., 2016). There are other possible explanations for low job satisfaction and for the finding that some participants chose to leave pediatric oncology despite the education. In this study, poor working environment was mainly related to the organization and the management. The importance of good management has previously been highlighted among nurses working in pediatric oncology, with findings showing that formal and informal support, in addition to a positive working climate, can enhance nurses’ professional growth (Enskär, 2012). Furthermore, in one study, work environment was significantly associated with job satisfaction (Kagan et al., 2021). Another important aspect for nurses in this study, leaving pediatric oncology, was related to working hours that did not fit the life situation. It is reasonable to believe that this is related to the fact that most of the participants were women, who might find it difficult to combine shift work with family life.
Graduates of this program had extensive experience in pediatric oncology, especially in the third cohort, indicating that despite the program having been offered since 2002, not all nurses with extensive experience have been able to enroll in the program. Furthermore, despite extensive experience, this education is relevant and in this study, the number of nurses with special positions had, 2 to 7 years after completing the education, increased to 55%, which could be compared with 50% in the 2016 evaluation (Pergert et al., 2016). The professional development and advancements in position could, in line with previous research, have contributed to increased job satisfaction (Takase et al., 2016). In this study, more nurses had a specialist position after the education but still, most of the nurses, 70%, remained bedside after the education was completed, even the ones with a specialist position.
The vast majority (89%) of the nurses in this study stated that the knowledge from the education had helped them in their work and contributed to them becoming more confident in interactions with the patient/family (89%). Knowledge is described as the most powerful factor in clinical competence (Carper, 2004) and in being an expert nurse (Benner, 1984). Previous findings show that nurses in pediatric oncology perceive their knowledge as a prerequisite for them to feel secure and confident in caring for children with cancer (Enskär, 2012; Pergert et al., 2016). Furthermore, specialist training in pediatric nursing can reduce the barriers to research utilization in clinical practice (Andersson et al., 2007). With this in mind, it is highly unfortunate that pediatric oncology centers in Sweden, due to the shortage of nurses with specialist training in pediatrics (Statistics Sweden, 2019), have no other option than to employ nurses without such training.
In this study, most of the nurses perceived that they were considered important in the multidisciplinary team and that nurses, physicians, and parents listened to and valued their knowledge. This was encouraging because one of the six baseline global standards for nursing care states that “nurses should be acknowledged as core members of multidisciplinary pediatric oncology teams” (Day et al., 2014, p. 682).
In this study, half of the nurses were using the national pediatric oncology network. Furthermore, working at pediatric oncology centers, having more than 5 years of experience, and the type of position at the time of the survey seemed important for the use of the national network. It can be assumed that some positions at pediatric oncology centers benefit from collaboration with national networks. Collaboration on national and international levels has been suggested as a key to the medical success story of pediatric oncology (Gatta et al., 2014). In addition, networks across the country have been identified as one major contribution to becoming a specialist nurse in pediatric oncology (Enskär, 2012). Furthermore, in this study more than half of the nurses kept up to date on knowledge from healthcare research. In contrast to our results, a previous Swedish study in pediatric care found that specialist nurses with more than 5 years of experience perceived more barriers to the utilization of research than registered nurses with less experience (Andersson et al., 2007). Surprisingly, the present study showed that an academic degree did not influence the use of healthcare research.
Furthermore, a majority of the nurses in this study stated that they had initiated quality improvements on the ward. This is encouraging, considering that one-third of the nurses in the study by Rudman et al. (2012) reported that they seldom or never implemented current knowledge in their clinical practice and thereby “contributed to change.” Initiated quality improvements not only benefit the care organization but personal initiatives have also been found to be positively associated with job satisfaction (Kagan et al., 2021).
Although this was a national study, the Swedish pediatric oncology context is unique due to its strong national and international collaborations and existing charity funding, and hence, the generalizability of the results is uncertain. In this study self-reported survey data was used, thus, the results are based on the perceptions of nurses who had graduated from the educational program. Furthermore, participating nurses chose to start and complete the education as well as the survey. A possible limitation is that no control group was used, for example, in relation to the number of nurses who had left pediatric oncology and those who had received a special position. Furthermore, the analysis of reasons for leaving pediatric oncology is based on answers from a relatively small group. On the other hand, several responses were given by most of them. Also, when comparing sub-groups, the number of participants in each group is small, for example, nurses with less than 5 years of experience, which needs to be taken into consideration.
Implications for Clinical Practice and Future Research
To meet the demands of highly specialized pediatric oncology care, it is essential to provide continuing education to nurses. An established education program in pediatric oncology for nurses contributes to improved competence and knowledge in clinical work, increased confidence in the interaction with affected families, and greater involvement in quality improvement work. Furthermore, continuing education has an impact on the career opportunities of nurses in clinical practice, for example, through various special positions.
To retain competent nurses within pediatric oncology care, employers need to be aware of the role of the work environment, aspects of work–life balance and career paths. Furthermore, qualitative research is needed to gain a deeper understanding of why nurses, despite continuing education, decide to leave pediatric oncology care. It is also important to understand the experiences of nurses working with pediatric oncology care at shared-care wards/hospitals and their roles in improving care and becoming experts.
Footnotes
Acknowledgments
The authors would like to thank the pediatric oncology nurses who completed the questionnaire. A special thanks also to Kristina Edner from the Swedish Childhood Cancer Fund for her significant contribution to the development of the questionnaire and Kirsti Pekkanen for gathering email addresses as well as giving input on this manuscript.
Author Contributions
Margareta af Sandeberg: conceptualization, data curation, formal analysis, project administration, writing –original draft, review, and editing; Maria Olsson: writing –review and editing; Torben Ek: writing –review and editing; Karin Enskär: writing –review and editing; Margaretha Stenmarker: writing –review and editing; Pernilla Pergert: conceptualization, data curation, formal analysis, project administration, writing –original draft, review, and editing.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Barncancerfonden (Swedish Childhood Cancer Fund) (education grant and TJ2017-0011).