
Abstract
Introduction
Thanks to enormous medical advances in the treatment of children and adolescents with cancer and the associated increase in survival rates as an additional indicator of treatment success, research increasingly focuses on children's health-related quality of life (HrQoL) (Bloemeke et al., 2020; Crame et al., 2018; Dopfer & Felder-Puig, 2006; Hutzen et al. 2019). While the World Health Organization defines quality of life (QoL) as a multidimensional and subjective construct that reflects an individual's subjective assessment of several domains of his or her life, such as physical, social, and psychological functioning (Bullinger, 2016; Bullinger & Brütt, 2018; World Health Organization, 1947), HrQoL covers physical, emotional, mental, social, and behavioral components of well-being and focusses on aspects of one's individual perception of health (The KIDSCREEN Group Europe, 2006). HrQoL can be captured at different levels. Generic instruments capture HrQoL regardless of the presence or absence of health problems, and this has the advantage that different groups can be compared. Chronic-generic tools focus on chronic conditions in general without considering the specific characteristics of particular chronic conditions. Condition-specific instruments are used only for specific diagnostic groups and assess potential problems associated with a specific disease (Brütt et al., 2009).
The diagnosis of cancer can lead to massive physical, emotional, and social burden in children and their families (Force et al., 2019; Schreiber-Gollwitzer et al., 2007; Schröder et al., 2019). Children, especially in the first years up to middle childhood with the age of 10 years, are in an important development phase. They need to develop self-efficacy (SE) and social and emotional maturity basics (Berk, 2018). Therefore, they are particularly affected by the consequences and limitations of cancer. Compared to healthy peers, children with cancer showed significantly more social problems and internalizing disorders (Van Dongen-Melman et al., 1995). According to parents, psychological problems were more often present in children surviving cancer compared to parents of healthy peers (Bradley Eilertsen et al., 2012). Additionally, children and parents of cancer survivors reported significantly impaired QoL (Bhat et al., 2005; Bradley Eilertsen et al., 2012; Kowaluk et al., 2019). Many pediatric cancer survivors, 31% to 85.2%, experience fear of cancer recurrence (Calaminus et al., 2003; Wroot et al., 2020; Yang et al., 2019) and reported increased levels of depression and anxiety (Myers et al., 2014; Yang et al., 2019). Furthermore, children with cancer reported low scores of QoL not only during treatment but also after treatment completion (Fardell et al., 2017).
Children with cancer might experience the diagnosis and treatment as a loss of empowerment and SE (Liu et al., 2020). SE is the belief in one's capability to manage a specific situation or perform a certain task at a given time (Bandura, 1977; Bandura et al., 1999). When faced with cancer, many new situations appear where the child lacks previous experience. For a child, it can be challenging to communicate one's desires in a commonly appearing care situation. The sources to build SE is a sense of mastery—experiencing success, seeing somebody else successfully perform a desired activity, eliciting feelings of capability, and verbal persuasion (Bandura, 1977, 1997; Bandura et al., 1999).
Accordingly, healthcare professionals report imposed autonomy as a common ethical dilemma in caring for children with cancer (Bartholdson et al., 2015). Although children have the right to be informed and participate in their care, research shows that children's views are often not considered in care situations (Coyne & Harder, 2011; Coyne et al., 2016; Runeson et al., 2007; Stålberg et al., 2016); for example, parents and clinicians discuss treatment and care while children are often present but not included in this discussion (Coyne et al., 2014). Thus, it is essential to strengthen children's communication and SE regarding their capacity to convey desires and needs.
Imagination in pretend play can generate coping strategies and practice and rehearse problem-solving approaches and allows the children to develop social skills such as communication and empathy (Hughes, 1999; Jent et al., 2011). Emotional processing in pretend play can help children regulate their moods and emotions. These processes can be helpful in medical settings where children are often struggling with fear, anxiety, and other negative emotions and need help developing coping strategies to deal with acute and chronic illnesses. Singer and Singer (1992) stated that using imagination in a self-paced way enables the child to “cut down the large things around it to manageable proportions.” Children can express fears in a safe setting and slowly reduce anxiety, and desensitization to feared situations is one way to reduce stress in a medical setting. In addition, engaging in pretend play can be a positive experience that improves mood (Moore & Russ, 2006).
There is evidence that play is a helpful intervention allowing children to express both positive and negative feelings (Jent et al., 2011; Seja & Russ, 1999), although there are many methodological issues that future research should address (Moore & Russ, 2006). One of the limitations has been the lack of control groups and small sample sizes. Play in a hospital setting resulted in less postsurgical pain (Ullán et al., 2014), reduced anxiety and negative emotions before surgery (He et al., 2015), reduced anxiety and increased cooperation during procedures, as well as enhanced treatment experience compared with a control group (Tsai et al., 2013).
While most clinics offer psychosocial support to address the burden of cancer treatment, this support is often not addressed to young children. So, the potential of a pretend play intervention for children aged up to 10 years was discussed with parents of children with cancer and professionals. Both parents and professionals positively rated this intervention as enhancing children's coping strategies and self-expression (Witt et al., 2019). A pilot test showed that children's HrQoL measures remained the same or increased after this intervention, demonstrating that pretend play is safe and does no harm to children (Frygner-Holm et al., 2020). Especially young children with cancer might benefit from standard play intervention procedures that can be used in many medical settings.
The present study explores whether a play intervention for children with cancer, based on identifying potential stress and resources of the young children from parents’ and professionals’ views, is associated with improved HrQoL and SE for communication in care situations over time. We hypothesize that both HrQoL and SE for communication will increase from before to after the pretend play intervention.
Methods
Patient Recruitment
The present study is part of a cooperation project Center for Research Ethics & Bioethics, Uppsala University (Sweden) and the University Medical Center Hamburg-Eppendorf, Department of Medical Psychology (Germany), aiming to investigate the well-being of children diagnosed with cancer in the course of a pretend play intervention. We conducted the study in three phases. Phase 1 focussed on preparations, including ethics, informed consent, training of the play facilitators, and recruitment of families. In phase 2, we collected the baseline data (T1), including parent reports and self-reports of the participating children before the pretend play intervention started, conducted the interventions, and collected the postdata (T2) after the last session had finished. Within phase 3, we prepared the data for analysis and completed the final report (Figure 1).
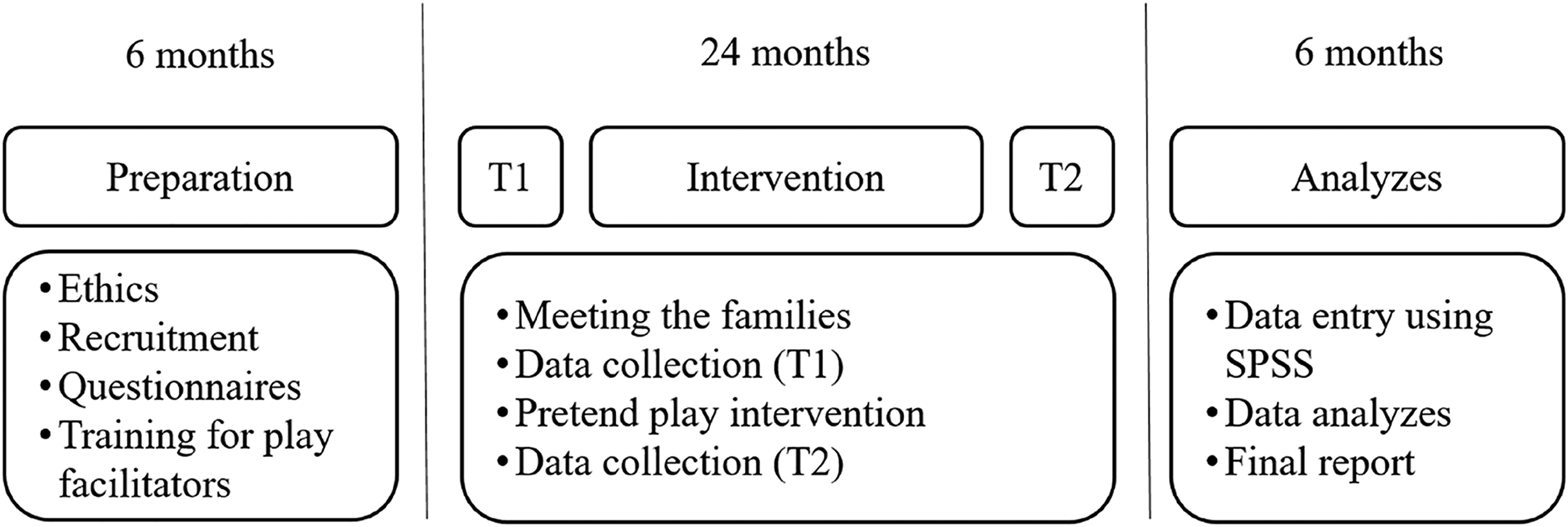
Timeline.
Uppsala’s (Drn: 2016/437) and Hamburg's (PV4987) regional ethics review boards approved the study. Participants and their parents obtained written and oral information and provided consent for participation and an agreement for data to be stored and processed only for research purposes. Special attention was given to informing the children about what participation could mean for them and that they could stop at any time they desired without questions asked.
In the present study, we enrolled children with cancer between February 2017 and November 2018 if they met the following inclusion criteria: age between 3 and 10 years, a clinical diagnosis of cancer, speaking and understanding of the German/Swedish language, and being well enough to play. Due to the explorative approach based on the children's individual needs, no further exclusion criteria were defined. In Sweden, we recruited the participating children through the pediatric oncology centers in Uppsala and Stockholm. In Germany, we recruited children and their families through the Department of Pediatric Hematology and Oncology at the University Medical Center Hamburg-Eppendorf.
The pretend play intervention consisted of six to eight weekly play sessions. Each session has a duration of approximately 30 to 45 minutes and includes three to four play themes prompted by the play facilitator (make up a story about…). These themes are based on affect, imagination, medical play, and then finish the session with the child making up a story on his/her own (Frygner-Holm et al., 2020; Witt et al., 2019). The child determines the play, and the play facilitator takes on the role assigned to him/her by the child. The child and the play facilitator can switch roles that enable the child to play both from the subjectively experienced point of view and the point of view of the doctor/therapist. The play facilitator strengthens the child's coping strategies by integrating different coping methods into his/her role (Witt et al., 2019). The play intervention was an adaptation of play intervention protocols developed for typical children (Moore & Russ, 2008) and children with sleep disorders (Fehr et al., 2016). The story prompts for the medical theme were based on issues that children with cancer struggle with (Witt et al., 2019). The play sessions were conducted at the hospital or the families’ homes, depending on the families’ choice. Depending on the children's needs, parents were present in the first sessions to enable the children to feel safe and secure.
Before the intervention started, the play facilitator and the child met to get to know each other in the presence of the parents, and the children decided to participate. The parents were asked to report any adverse event to the play facilitator during the study to ensure that the child's needs and well-being were considered. In case of any adverse events caused by the intervention, parents were instructed to withdraw from the study and seek professional help.
Due to the explorative nature of the project, a heterogenic selection of questionnaires was used to measure children's HrQoL and SE before and after the intervention. This includes generic, chronic–generic, and condition-specific measurements to cover the wide range of HrQoL components, which vary depending on the level of assessment (Assari et al., 2009; Lin et al., 2013). Additionally, we assessed parental HrQoL and family functioning before the intervention. We asked parents to fill out a questionnaire one week or less before the first pretend play session and after the last play intervention. Children answered the questionnaire with the play facilitator's assistance, who helped reading the questions, before the first and after the last pretend play session. If the children were comfortable with it, they were alone with the play facilitator. In most cases, the parents were near but in a separate room. Parents filled out the questionnaire at the same time.
Instruments/Measures
Before the intervention started, we measured parental HrQoL and family functioning using the PedsQL™ Family Impact Module (FIM) to describe the families’ situation (Varni et al., 2004). The FIM consists of 36 items rendering eight dimensions: physical functioning, emotional functioning, social functioning, cognitive functioning, communication, worry, daily activities, and family relationships. The module also yields three summary scores: total score, parent HrQoL summary score, and family functioning summary score. Answers are given on a 5-point Likert scale. Subscales were calculated and linearly transformed from 0 to 100, with higher scores indicating better HrQoL (Varni et al., 2004). Internal consistency reliability alpha coefficients for the FIM vary between 0.82 for the subscale Worry and 0.97 for the total score and the subscale Family Relationship (Varni et al., 2004).
We used the PedsQL™ 4.0 Generic Core Module (self-report for children aged 5 years and older; parent proxy report for children from 3 years) to measure generic HrQoL (Varni et al., 2002). The PedsQL™ 4.0 includes 23 items scored on a 3-point Likert scale for children aged 5–7 and a 5-point Likert scale for parents and children above 7 years. If 50% or more items were completed, the mean of the completed items on a scale was imputed. Subscales for physical, emotional, social, school functioning as well as a sum score for psychosocial health and a total score were calculated and linearly transformed to a 0 to 100 score. Cronbach’s alpha for self-reports of the PedsQL™ 4.0 Generic Core Module varies between 0.68 for the subscale social functioning and 0.91 for the total score (Varni et al., 2007a), whereas the internal consistency reliability alpha coefficients for the proxy report ranges between 0.61 for the subscale school functioning and 0.93 for the total score (Varni et al., 2007b).
To assess chronic-generic HrQoL, we used the DISABKIDS questionnaire (Baars et al., 2005; Schmidt et al., 2006). Parents filled out the DISABKIDS Chronic Generic Module-37, consisting of six dimensions: independence (six items), physical limitation (six items), emotion (seven items), social exclusion (six items), social inclusion (six items), and medication/treatment (six items). Children answered the DISABKIDS smiley version consisting of six items because it is simple to administer and is suited for young children (Chaplin et al., 2008). Items were scored on a 5-point Likert scale ranging from 1 (never) to 5 (always). Scores were transformed into a 0 to 100 scale. Higher scores indicate better HrQoL (The European DISABKIDS Group, 2006). The scores for the internal consistency range between 0.70 and 0.87, whereas the test–retest reliability varies between intraclass correlation coefficients ranging from 0.71 to 0.83 (Simeoni et al., 2007).
We assessed condition-specific HrQoL using the PedsQL™ cancer module consisting of 26 items and encompasses eight dimension scales: Pain and Hurt, Nausea, Procedural Anxiety, Treatment Anxiety, Worry, Cognitive Problems, Perceived Physical Appearance, and Communication. Additionally, a total score for condition-specific HrQoL was calculated. The PedsQL cancer module for self-report aged 5 to 7 years uses a 3-point Likert scale, and parent reports use a 5-point Likert scale. Items were scored and linearly transformed to a 0 to 100 scale, with higher scores indicating better HrQoL (Varni et al., 2002). Internal consistency reliability alpha coefficients for the self-report vary between 0.66 for the subscale school functioning and 0.88 for the total score. Cronbach's alpha varies between 0.73 for the subscale social functioning and 0.93 for the total score within the proxy report (Varni et al., 2002).
SE regarding communication in care situations was measured using five questions encompassing common situations at the hospital, starting with the phrase “Right now, how sure are you that you could.…” Instructions were to point to one out of three smiley faces. The SE scale was constructed for this project (Frygner-Holm et al., 2020), and its development is described in detail by Frygner-Holm et al. (2022). A proxy measure of children's SE in communicating in care situations was also constructed for this study. Scores were rated using a numerical rating scale with anchors 0 to 10. The validity and reliability of this scale are yet to be tested in large samples.
The children's enjoyment of the pretend play sessions were rated using a smiley scale with five faces using the anchors of 5 = really fun to 1 = really boring after each session.
Additionally, we requested the parents to answer questions on sociodemographic and clinical data, such as age, gender, diagnosis, date of initial diagnosis, number of days in the hospital, and number of people living in the household.
All play facilitators were trained based on the pretend play manual (Frygner-Holm et al., 2020; Witt et al., 2019). All aspects of adherence were discussed during supervision, and SFH supervised the play facilitator regularly. SR advised SFH whenever any insecurity regarding the play intervention arose to facilitate playing skills.
Data Analysis
All analyzes were conducted with the Statistical Package for the Social Sciences (SPSS), Version 25.0. Except for sociodemographic and clinical variables, missing items were handled according to the respective developer's guidelines. For the PedsQL™ generic core module, the PedsQL™ cancer module, and the FIM, missing values of more than 50% of the items on a scale resulted in an invalid scale (Varni et al., 2002, 2004), and data were excluded from the analysis. For the DISABKIDS, scales were calculated when at least 80% of the items of each scale had been answered (The European DISABKIDS Group, 2006). Incomplete data are demonstrated by n in each table. Missing data were mainly found at the end of the interviews/questionnaires.
Means and standard deviations were calculated for continuous variables and frequencies and percentages for categorical variables. Bivariate analyses were performed using Student's t-test (comparison of sample with reference values) and Wilcoxen's signed-rank to analyze within-group changes (from pretreatment to posttreatment) in all outcome variables, when appropriate. We calculated the changes over time by directional discrepancies, and the significance level was set at p ≤ .05.
Results
Twenty-four children (and parents) agreed to participate in the study. One child declined participation after filling out the questionnaires because the questions triggered anxiety, resulting in nightmares. Twenty-three children received at least three pretend play sessions. Three families did not finish the intervention due to time management difficulties or problems with playing creative play and dropped out. Furthermore, one family had to be excluded due to missing data for the postassessment. In total, 19 families were included in the presented analyzes, including 14 self-reports of children and 19 proxy reports of parents (Table 1). All included children participated in 6 to 10 play sessions. The play session took place weekly or every 2 weeks, depending on the availability of the child/family or the state of health of the child. With expectation of one girl, the time from the first session to the last session varied between 6 and 12 weeks. Due to practical reasons or illness, longer time could pass between play sessions. Measures were done no more than 1 week before intervention onset and in direct conjunction with the final play session.
Sample Characteristics
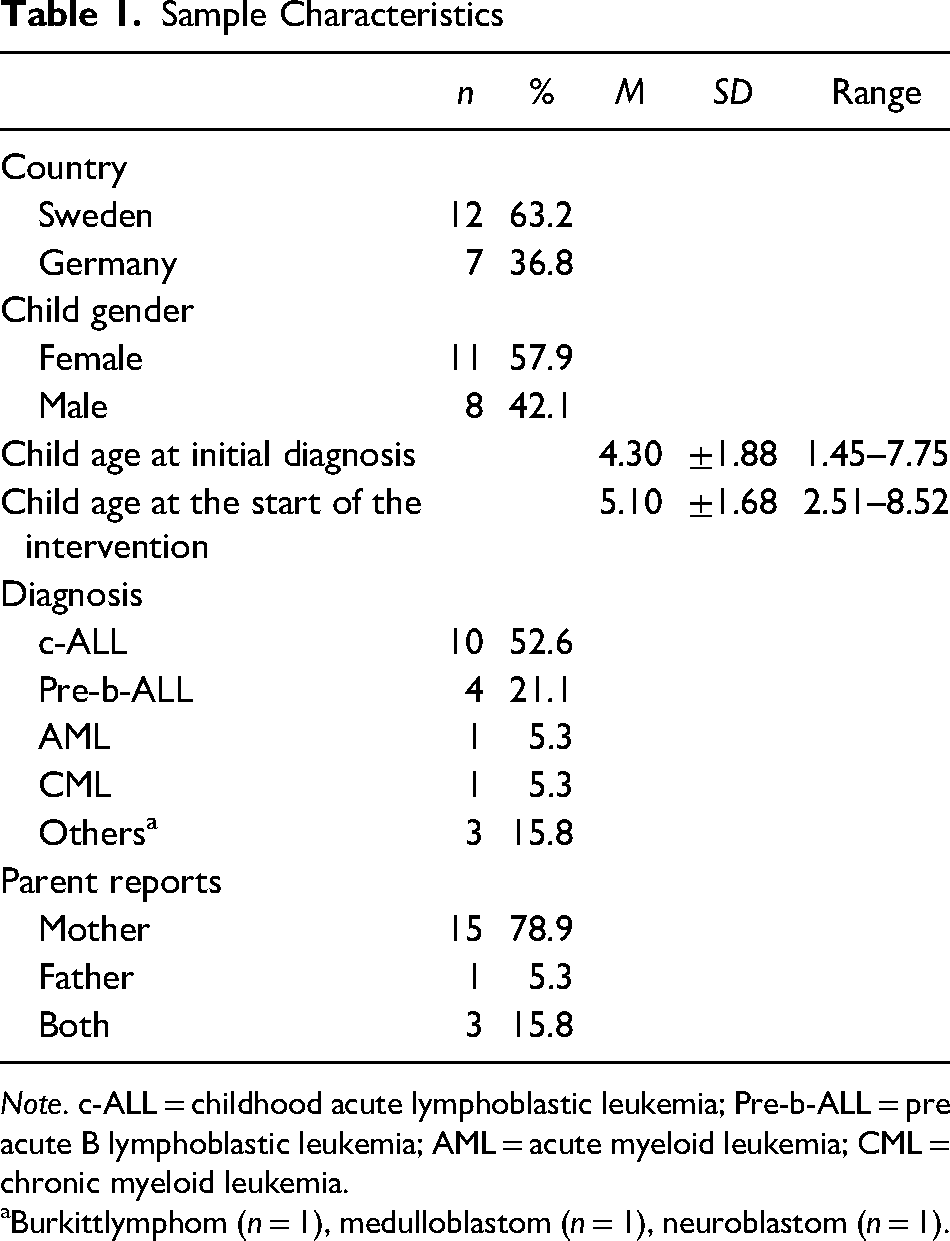
Note. c-ALL = childhood acute lymphoblastic leukemia; Pre-b-ALL = pre acute B lymphoblastic leukemia; AML = acute myeloid leukemia; CML = chronic myeloid leukemia.
Burkittlymphom (n = 1), medulloblastom (n = 1), neuroblastom (n = 1).
Family Impact
The means and standard deviations of the parents’ perceptions on the FIM assessed before the pretend play interventions started, are presented in Table 2, and compared with reference values from families with children in an outpatient setting (Varni et al., 2004). The participating families of children with cancer reported lower HrQoL than the outpatient sample on the scales Emotional Functioning (t18 = −3.198, p = .005), Social Functioning (t18) = −2.350, p = .030), Cognitive Functioning (t18 = −3.565, p = .002), Daily Activities (t17 = −2.942, p = .009), and Family Relationship (t17 = −5.118, p = .002). Furthermore, the sample of parents of children with cancer showed significant lower scores for the sum scores Parental HrQoL (t18 = −2.549, p = .020), Family Functioning (t17 = −5.741, p = .001), and the total score (t18 = −2.785, p = .012) (Table 2).
Results of the PedsQL Family Impact Module and Comparison With Reference Values
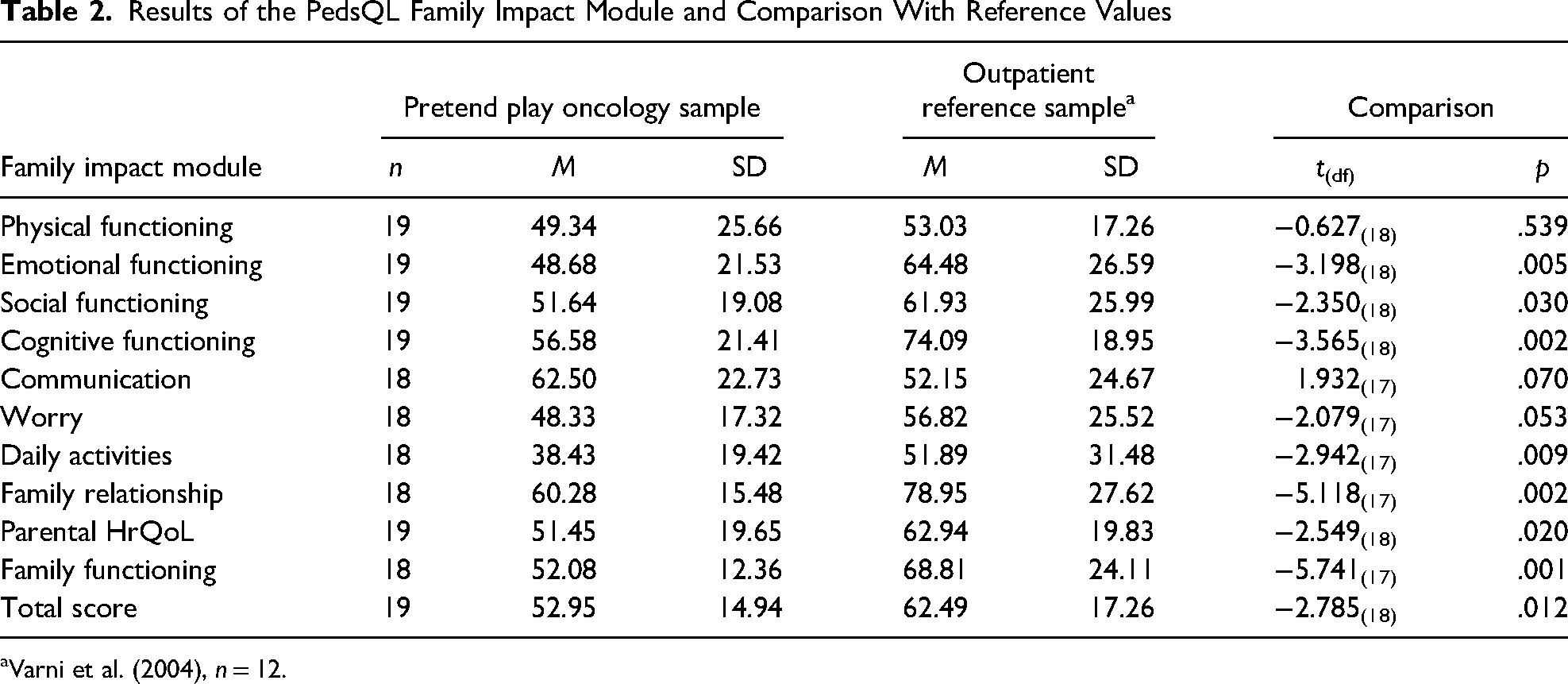
Varni et al. (2004), n = 12.
Changes in QoL
Children reported positive changes from preassessment to postassessment of generic, chronic-generic, and cancer-specific HrQoL. Changes regarding the generic HrQoL varied from 4.62 (±17.97) for the scale Social and 17.43 (±21.29) for the scale School. Generic HrQoL changes reached the significance level for the scales Emotional (z = −2.87, p = .004), School (z = −2.60, p = .009), Psychosocial (z = −3.10, p = .002), and the total score (z = −2.48, p = .013). Additionally, children reported a significant improvement in chronic-generic HrQoL (z = −2.13, p = .033). The cancer-specific HrQoL assessment showed positive changes for all scales, except the scales Worry −5.83 (±25.47) and Cognitive Problems −1.91 (±21.79). The discrepancies between preassessment and postassessment regarding the cancer-specific HrQoL showed significant differences only for the scale Communication (z = −2.68, p = .007) and the total score (z = −2.28, p = .023; Table 3).
Changes in HrQoL in the Course of the Pretend Play Intervention From Children's Self-Report
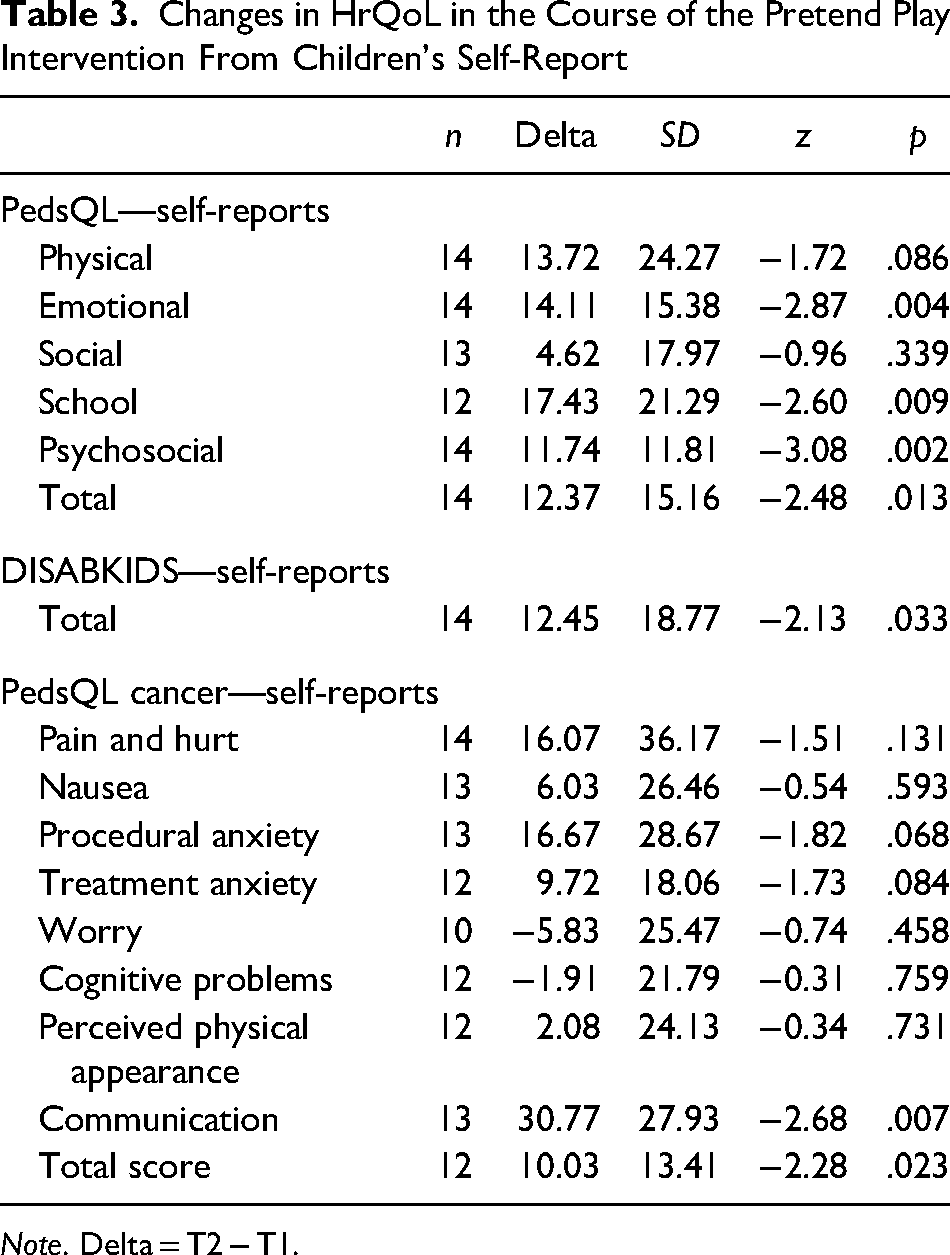
Note. Delta = T2 − T1.
Parents reported positive changes from preassessment to postassessment for all scales of generic, chronic-generic, and cancer-specific HrQoL measurements. These changes were significant for the generic scale physical (z = −3.00, p = .003), the generic total score (z = −2.58, p = .010), the chronic-generic scales independence (z = −2.08, p = .037), and Physical (z = −2.55, p = .011) as well as for the cancer-specific scales Pain and Hurt (z = −3.08, p = .002), the scale Procedural Anxiety (z = −2.61, p = .009), and the total score (z = −2.33, p = .020; Table 4).
Changes in HrQoL in the Course of the Pretend Play Intervention From Parent's Proxy Report
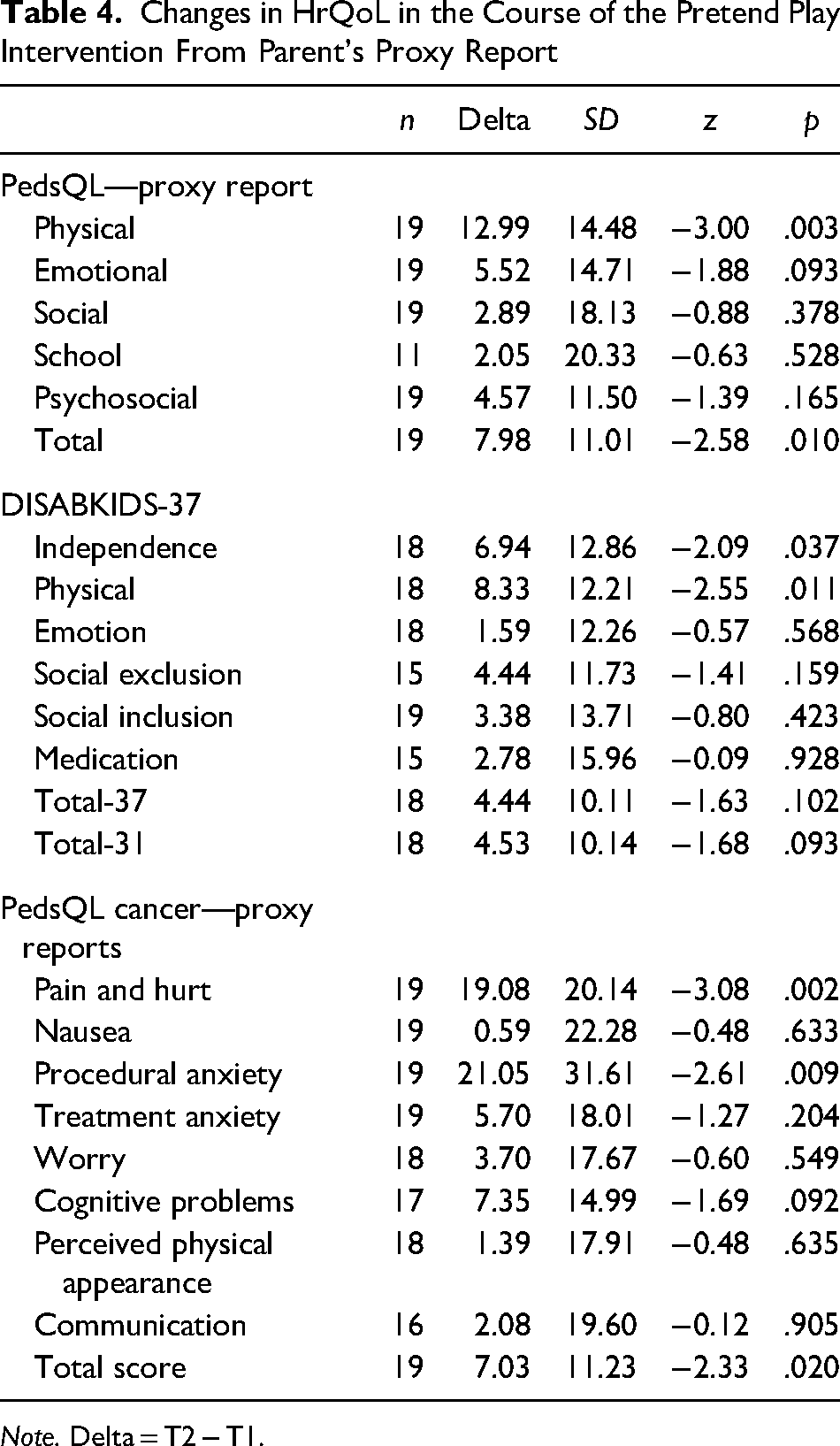
Note. Delta = T2 − T1.
Changes in SE
The participating children reported significant positive changes in the assessment of SE regarding the aspects of asking for help (Item 01: z = −2.23, p = .026), telling the staff about rejections and disapprovals (Item 03: z = −2.23, p = .026), and acceptance despite rejection (Item 04: z = −2.57, p = .010). Parents’ proxy reports also showed positive changes in SE for all aspects, but these changes did not reach the significance level of p ≤ .05 (Table 5).
Changes in SE in Care Situations From Children's and Parents’ Perspectives
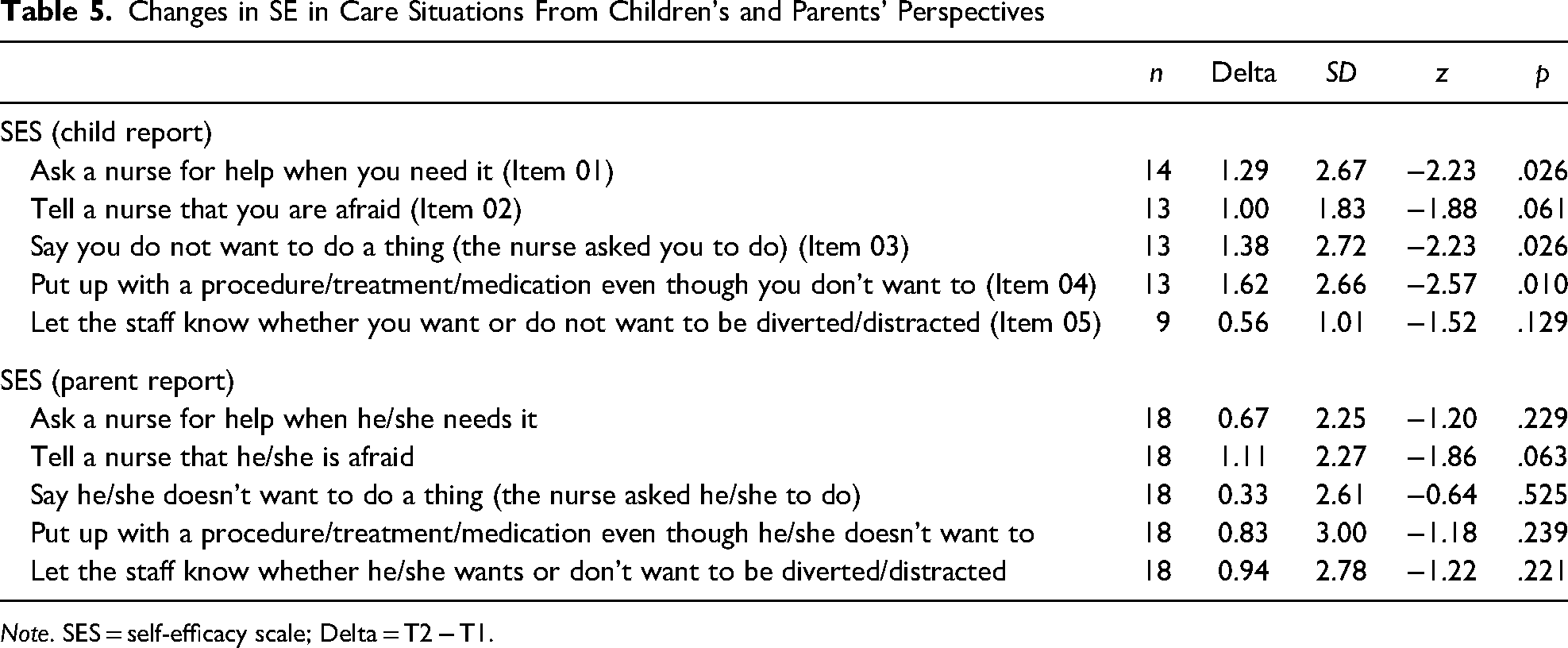
Note. SES = self-efficacy scale; Delta = T2 − T1.
After each pretend play session, the children rated their fun on a 5-point Likert scale using smileys. Higher scores indicated more fun. The mean for fun in each session was 4.55 (±1.00). No adverse events were reported after play sessions.
Discussion
We presented the evaluation results of a pretend play intervention for young children with cancer. The story stems used in the play intervention targeted ways to work through and communicate in different scenarios commonly experienced during care for children with cancer. We found improvements in child-reported domain communication, and emotional and psychosocial well-being using generic and cancer-specific HrQoL measurements. The results also demonstrated improvements for most SE items in care situations.
Moreover, children reported having fun during the pretend play intervention. The children enjoyed the play sessions, although the themes included aspects of medical treatment and daily life restrictions experienced as unpleasant. Parents and professionals highlighted this confrontation with experiences of medical treatment as necessary for disease-specific coping. At the same time, they wanted children diagnosed with cancer to be “just a child” and play as a child (Witt et al., 2019). Therefore, the presented and evaluated pretend play intervention met these essential expectations of parents and professionals.
The child-reported generic HrQoL demonstrated significant improvements from prior to the intervention to its completion. We found changes regarding the emotional, psychosocial, and school-related subscales. Parents’ experiences (Höglund et al., in press) support these findings. The intervention did not target the physical components of HrQoL, and therefore no alterations in scores were expected. However, the parents reported minor changes in the physical dimensions in both generic and chronic-generic HrQoL, along with improvements in independence. Physical aspects might be essential for parents because they are more observable than internal processes (Eiser & Varni, 2013; Patel et al., 2017; Rajmil et al., 2013). Therefore, physical aspects are easier to assess from the parents’ perspectives, which may explain why parents focus on the observable physical aspects. Additionally, the cancer-specific physical limitations and (treatment) pain result in child and parental burdens, misleading parents to rate these physical dimensions of HrQoL as very important.
An improvement in the child-reported cancer-specific HrQoL was also found. With this, the communication subscale rendered a significant change after the intervention. The main aim of this pretend play intervention was to change the social and emotional dimensions of HrQoL, not physical. No changes in the self-reported physical dimensions of HrQoL were found, and only small alterations were in the proxy measures. This could be interpreted as the children's physical status being similar after the intervention as when the play intervention started. Physical well-being was never targeted in the intervention, and therefore no alterations in scores were expected.
At the same time, they experienced that communication was more effortless than before the intervention. Especially young children with cancer were rarely involved in communication about the disease and their respective emotions (Sisk et al., 2020), so our results reveal that children experience this pretend play intervention as helpful and encouraging to communicate about emotions and needs.
The parents also reported an improvement in the cancer-specific HrQoL. Significant changes were found in the Pain and Hurt and Procedural Anxiety subscales. Research on parent–child agreement shows that it is easier for parents to rate observable domains of HrQoL, such as physical well-being (Eiser & Varni, 2013; Patel et al., 2017; Rajmil et al., 2013). Nevertheless, research on children born with esophageal atresia showed that parents have difficulties assessing children's physical well-being the same way children do (Witt et al., 2021). So it is crucial to use both child reports and parent reports to broaden the perspective on the child's well-being without attaching more importance to one perspective or valuing it more highly than another (Silva et al., 2015; Upton et al., 2008). Researchers and clinicians should consider that parental awareness and sensitivity might be higher than the child's (Upton et al., 2008). Parents may consider quite more and broader aspects in their assessment and more extended periods. Furthermore, one may assume that the changes in the physical aspects of the children's HrQoL might be influenced by the fact that parents experienced their children as happy and having fun while playing with the play facilitator. The children did not express physical pain or experience physical limitations during the play, and parents might assess these observations resulting in higher cancer-specific physical HrQoL scores.
Furthermore, there was a significant improvement in SE for asking a nurse for help, saying no to something they do not want to do, and SE for putting up with an unwelcome procedure. However, we did not find any improvements regarding saying that the child is afraid or turning suggested distractions down. Fear is essential to address in children with cancer. It is both an uncomfortable emotion and associated with increased pain, that is, when a child is fearful, levels of pain increase (Hedén et al., 2020). This association is even stronger in younger children (Hedén et al., 2016, 2020), making interventions targeting young children even more important. The fact that two SE questions did not reach statistical significance may guide a further improvement of the intervention. Nurses must be aware of children's fear and individual preferences on a distraction to adapt to the situation to meet the child's individual needs better.
The changes in the parent-reported SE did not reach significance. The reason could be that the parents could not sense alteration in their children's behaviors or that the measure is not sensitive enough to capture alteration in SE for communication. However, when the parents were interviewed after the play intervention was completed, most of the parents talked about how they experienced an improvement in their children's ability to communicate, cope with care situations and participate in their care (Höglund et al., in press).
Although HrQoL is a subjective construct, using proxy reports in HrQoL research—especially in children—is common (Dickinson et al., 2007; Silva et al., 2015). This includes the young age or impairments due to illness or cognitive abilities (Silva et al., 2015; von Essen, 2004). Clinicians and researchers should use child and parent reports whenever possible, even though parent proxy reports have often been questioned (Panepinto et al., 2010), and the results of our sample highlight the varying perceptions of children and parents.
It is worth mentioning that the intervention caused no adverse events, but one child declined participation after filling out the questionnaires because the questions triggered anxiety and nightmares. The question the child reacted to was a question from the cancer-specific PedsQL about recurrence fear. The child was referred to a psychologist at the oncology center. Thus, studies or interventions such as this should acknowledge and prepare for this kind of reaction and work in close contact with child healthcare providers.
Limitations
Caution should be given to the small sample size, as it may affect the interpretation and generalizability of the results. The results from this pilot study could be used to calculate an effect size and provide the foundation for power analysis in a large-scale randomized controlled study.
Measuring effects poses a great challenge when performing intervention studies with very young children. Some children were too young to report on HrQoL and SE, so we mainly analyzed parent reports within the German sample.
All children were assisted by an adult when completing the questionnaires. Although this support was as neutral as possible, it could influence the replies, depending on how a question was read out or emphasized. Also, children's shyness or reluctance to meet new people could impact. We tried to address this by making the children as comfortable as possible, allowing them a few minutes to play or talk before starting. A mixed-method approach is likely essential when studying children this young. Estimating the effect with a quantitative approach is plausible, but this is not enough; hence, results need to be validated by qualitative data, preferably from both children and parents.
Another limitation is that this study did not include a control group. Therefore, we cannot rule out the passage of time as a confounding variable. However, based on our clinical experience with children with cancer, it is unlikely that the passage of time alone would result in the improvements found in this study.
This condition-specific intervention should be evaluated using a larger sample, including a control group. The small sample size does not allow for subgroup analysis, so age and gender might play an essential role in the effect that remains unclear. The results need to be confirmed in larger samples with a robust research design.
To the best of our knowledge, there was no current measure available regarding SE in care situations; therefore, a scale was developed based on the recommendations by Bandura (2006). The results should be interpreted with caution when using a new, nonvalidated instrument. Studies of the validity and reliability of the SE in Communicating in Care Situations scale are in progress.
Conclusion
The cancer-specific pretend play intervention offers young children with cancer a protected environment and can contribute to their well-being, communication, skills, and enjoyment during or after cancer treatment. Besides the HrQoL measures that are important for research, children experienced much fun during the play sessions. These experiences are critical for young children with cancer because cancer treatment is associated with pain and physical and social restrictions over a long period. The combination of fun within play sessions and dealing with different experiences of cancer treatment might offer new chances for the development of appropriate and effective coping strategies.
Footnotes
Acknowledgments
We want to thank the families, especially the children who shared their experiences with us, and we want to thank the clinicians who helped recruit families. Additionally, we thank Lizbeth Tinajero for her support in preparing the manuscript.
Declaration of Conflicting Interests
The author(s) declare no potential conflicts of interest concerning the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was funded by the Swedish Childhood Cancer Fund (Grant number 2018-0071) and the Hamburg Foundation to Promote the Fight against Cancer (Hamburger Stiftung zur Förderung der Krebsbekämpfung: Grant number 193).