
Abstract
The diagnosis of cancer or a blood disorder in childhood or as an adolescent/young adult (AYA) can have a significant effect on the developmental trajectory of a patient. Yet the psychosocial services provided to these patients and their families vary widely across the United States and the world (Scialla et al., 2017). The Psychosocial Standards of Care Project for Childhood Cancer was conceived to address these gaps and build consensus around psychosocial standards of care for this population. This work started in 2012 with a group of psychosocial oncology professionals from oncology, psychiatry, psychology, social work, and nursing. Guidelines were disseminated in 2015 for broad use (Wiener et al., 2015a). In 2017, the group conducted a survey to explore current staffing and service availability at pediatric cancer centers in the United States (Scialla et al., 2017). The authors noted that most programs have the basic level of staffing needed to implement some of the Standards but lacked the more comprehensive multidisciplinary team necessary for full implementation. The survey focused on the most provided services, leaving gaps in our understanding about the availability and use of music therapy as a member of the psychosocial care team called to advance the Psychosocial Standards of Care.
Music therapy is becoming a standard psychosocial supportive care service in many pediatric hospitals across the United States (American Music Therapy Association, 2020; Knott et al., 2020). As pediatric oncology centers strive to implement the Standards for Psychosocial Care for Children with Cancer and Their Families (Wiener et al., 2015a, 2015b), it is important to consider how credentialed music therapists are helping to advance the standards through research and evidence-based interventions, innovative programming, developmentally appropriate care, and collaboration as members of the multidisciplinary care team. Credentialed music therapists use music within a therapeutic relationship to address physical, emotional, cognitive, and social needs of patients and their families (American Music Therapy Association, 2021). Research supports the use of music to manage symptoms, support development, improve coping, and provide family support (Bradt et al., 2016; Coughtrey et al., 2018; Facchini & Ruini, 2021; Lee, 2016; O’Callaghan, 2016; Stegemann et al., 2019; Thrane, 2013).
The purpose of this paper is to analyze how music therapy services support implementation of the Psychosocial Standards of Care. First, we provide a brief overview of the music therapy service structure in United States (US) pediatric medical settings. Second, we provide an overview of the standards and synthesize the evidence from music therapy that demonstrates this discipline supports the Standards. Finally, we provide two clinical program descriptions demonstrating music therapy as an integrated psychosocial care service and case examples illustrating implementation of the Standards.
Music Therapy Service Structure in Pediatric Medical Settings
Music therapy is becoming a standard of psychosocial care in many pediatric medical settings, with forty-nine of the 50 Best Children's Hospitals for Cancer employing one or more credentialed music therapists (U.S. News & World Report, 2021). The first US survey of music therapists working in pediatric medical settings provides an overview of current service delivery and program structure (Knott et al., 2020), with most respondents (76%) providing services to hematology/oncology patients and their families.
In addition, survey findings of music therapists working in pediatric care settings indicate: 1) a ratio of about one music therapist for every 100 hospital beds, 2) one-third of respondents are the only music therapist in their pediatric care setting, and 3) half of the positions are philanthropically funded. Prioritization of patient referrals is almost always based on acuity (>97%), with palliative care and pain the most highly prioritized needs (Knott et al., 2020). While this cross-sectional survey was not designed to answer questions about how music therapists are implementing the Standards, it does provide insight into how music therapy services are provided and the alignment of current clinical practice with the Standards.
Music Therapy and the Psychosocial Standards of Care
The Psychosocial Standards of Care project yielded 15 standards for patients and families dealing with cancer (Wiener et al., 2015a; Appendix A). The Psychosocial Standards (PSS) address a wide range of needs for patients and families across the cancer continuum. Based on a recent national practice survey (Knott et al., 2020), published literature, and current Scope of Music Therapy Practice (American Music Therapy Association, 2015) we identified nine Standards that are being implemented through music therapy services (PSS 1, 4, 6, 7, 8, 9, 10, 13, 15).
PSS1: Psychosocial Assessment as a Standard of Care
Referral and assessment are central to the practice of board-certified music therapists (CBMT, 2021). A majority of programs use a referral-based system (Knott et al., 2020). However, high patient to therapist ratios necessitate referral prioritization based on acuity and/or need. Prioritization requires communication among psychosocial team members and ongoing assessment to provide the best care when and where it is most needed. Areas for systematic assessment include patient/family strengths and needs across a range of domains including emotional status, coping, mental health, and symptom distress, among others [American Music Therapy Association (AMTA), 2021]. The affective salience of music provides a distinct view into the psychological and emotional experience of hospitalized children and their families, offering a unique perspective to the psychosocial care team (Loewy, 2015; O'Callaghan et al., 2012, 2013; O’Callaghan, 2016; Shoemark et al., 2018).
PSS4: Psychosocial Interventions and Therapeutic Support as a Standard of Care
As clinicians, music therapists spend the majority of their time providing direct patient care in both inpatient and outpatient settings (CBMT, 2020; Knott et al., 2020). Based on clinical practice survey data, the top three needs addressed include coping, pain management, and palliative care/bereavement (Knott et al., 2020). A growing body of research, coupled with clinical practice knowledge, informs the evidence-based use of music by credentialed music therapists. Examples include music listening, songwriting/digital video production, and active music-making to improve coping, alleviate distress, promote self-expression/communication, and support parent-child interactions (Barrera et al., 2002; Barry et al., 2010; Haase et al., 2020; Robb et al., 2008, 2014, 2017; Stegemann et al., 2019; Uggla et al., 2018; Yates et al., 2018).
PSS6: Assessment and Support of Caregiver Needs as a Standard of Care
Music therapists employ a model of family-centered care that actively involves parents/caregivers in assessment, treatment planning, and care delivery (Lindenfelser et al., 2012; Shoemark & Dearn, 2008). Stress experienced by children and AYAs with cancer and their caregivers is highly interrelated. Studies have documented parent-reported benefit from witnessing improvements in their child or AYAs mood, engagement, and overall well-being as result of music therapy services (Docherty et al., 2013; Robb et al., 2014, 2017; Yates et al., 2018), with recent trials investigating development of dyadic interventions to directly address the interrelated needs of caregivers and their children (Holochwost et al., 2020; Robb et al., 2017; Yates et al., 2018).
PSS7: Psychoeducation for Patients and Families
Central to music therapy practice is working collaboratively with patients and families to identify ways music can be used as a self-management strategy for procedural distress, treatment side effects, and social isolation that can result from extended hospitalizations and treatment. For example, Rodgers-Melnick et al. (2019) created a group music therapy program to address health challenges faced by AYAs with sickle cell disease as they transition to adult medical care. Group drumming was used to promote cohesion and social support, followed by educational sessions that were co-facilitated with a medical provider. Sessions focused on medication management, disease knowledge, and pain management skills. Music experiences (songwriting, instrumental improvisation) were used to teach and reinforce new knowledge and skills. Other programs have incorporated parent instruction, music resources, and ongoing projects to encourage uptake and independent use of music as a support strategy (Barry et al., 2010; Holochwost et al., 2020; Lindenfelser et al., 2012; Robb et al., 2014, 2017).
PSS8: Procedural Preparation and Support as a Standard of Care
Pain management is one of the top three areas of care reported by music therapists (Knott et al., 2020); this focus includes procedural preparation and support, often in collaboration with child life specialists. Extensive evidence supports the use of music to manage pain, anxiety, and emotional distress during invasive procedures (Bradt et al., 2016; Lee, 2016; Nguyen et al., 2010; Thrane, 2013). Examples include music assisted relaxation, singing familiar songs to slow breathing rate and promote self-regulation, engaging in music play to regulate attention for the purpose of distraction, and music listening to support positive imagery and/or regulate mood (Armington et al., 2016; Giordano et al., 2020; González-Martín-Moreno et al., 2021; Nguyen et al., 2010).
PSS9: Providing Children and Adolescents Opportunities for Social Interaction as a Standard of Care
In addition to individual music therapy, group sessions for children and AYAs are also frequently offered (Knott et al., 2020). Music is a highly social phenomenon, reflecting culture, personal identity, and development. As such it provides a unique pathway to support children and AYAs, fostering social interaction among patients, family members, and peers (Docherty et al., 2013; Haase et al., 2020; Holochwost et al., 2020; O'Callaghan et al., 2012, 2013; Rodgers-Melnick et al., 2019; Shoemark et al., 2018; Shoemark & Dearn, 2008).
PSS10: Sibling Support as a Standard of Care
During acute cancer treatment, music therapists provide sibling support through scheduled group sessions and involve siblings in patient-directed sessions when they visit the unit (Duda, 2013; Hodkinson et al., 2014; Knapp et al., 2009; Knott et al., 2020). Music therapists also provide services to siblings as part of bereavement care. Music therapy has been identified as a valued source of sibling support by parents (Knapp et al., 2009; Tucquet & Leung, 2014), and represents an area for service expansion.
PSS13: Palliative Care as a Standard of Care
Music therapy is uniquely suited to provide holistic care for patients and families dealing with a life-threatening illness. Referrals for palliative, bereavement, and end-of-life care are prioritized in pediatric music therapy programs (Knott et al., 2020). Music therapists provide creative opportunities to address the physical (symptom management), psychological (coping, self-expression), social (bonding, connectedness), and spiritual (meaning-making, legacy) needs of patients, families, peers, and staff. In addition to pain and symptom management strategies described under PSS8, music experiences like active music making, songwriting, and heartbeat recordings are used to support social connectedness, create positive memories, and promote self-expression during treatment and at end-of-life (Daveson, 2001; Duda, 2013; Hilliard, 2003; Walden et al., 2020).
PSS: 15: Communication, Documentation, and Training Standards as a Standard of Care
Music therapists are integral members of the pediatric hematology/oncology care team, participating in psychosocial care rounds, providing education and training, and documenting services in the electronic medical record. Music therapists are board certified and deliver services consistent with their professional Scope of Practice (AMTA, 2015). Education and training include completion of a music therapy degree (bachelor's or higher), followed by a clinical internship (AMTA, 2021). Graduates are then eligible to sit for the national board certification exam for music therapists (CBMT, 2020) and engage in continuing education to maintain their credential. For music therapists working in pediatric medical settings, a majority hold a Master's degree and more than half have completed advanced training (Knott et al., 2020).
Music Therapy Program Descriptions and Case Examples
While the music therapy practice survey has identified trends in service delivery, there is no one-size-fits-all approach. Each hospital is unique in mission, vision, philosophy and available resources (Ernst, 2020; Zigan et al., 2009), and though similarities exist, there are often differences in how music therapy services are integrated at each institution. The next section will describe music therapy services from two Midwestern pediatric hospitals, focusing on the integration of services within cancer care and the alignment of those services with the Standards.
Riley Children's Health at Indiana University Health Program
Riley Children's Health at Indiana University Health is a nonprofit, comprehensive children's hospital with 22,300 admission and observations annually, 200 primary care and 400 specialty care physicians along with 229 residents and fellows across 40 specialties. Riley is an academic health center affiliated with Indiana University School of Medicine. The music therapy program has a rich heritage that began with one full-time music therapist in 2000, and now includes 4 full-time positions in 2021. The music therapy department uses an evidence-based practice model, aligned with the hospital's values, to support cohesive care across patient populations. One full time music therapist provides care for the inpatient Hematology/Oncology/Bone Marrow Transplant units.
Role of the Music Therapist
Music influences development, family experience, and socialization of nearly all children (DeNora, 2000). Given their training, music therapists are uniquely positioned to leverage these individual relationships to music to improve health outcomes. In times of relative wellness, the therapist emphasizes patient development, including healthy aspects of self. The music therapist also serves as on-going companion, witness and facilitator of a safe and creative space for patients and families. They provide a reliable and consistent presence, creating an alliance with patient, family and/or staff and stimulating musicality to serve as a safe space or pathway in which the patient can endure. The therapeutic relationship acknowledges the role of music in the identity of each patient, reflecting their culture, community, and individual ‘self’ (Amir, 2004; Ruud, 2010).
Model of Care and Service Allocation
Riley's model of care delivery was created using a team-based service development program, grounded in collaborative reasoning (Laursen, 2018; Shoemark et al., 2018). Therapists provide pathways to improve psychological, behavioral, and physiological functioning using music. The program focuses on three domains of care: distress tolerance, functional skills reinforcement, and resilience.
Distress Tolerance (PSS 8, 13)
Music interventions to promote distress tolerance focus primarily on procedural support and palliative care, particularly at end-of-life. Therapists often provide support before, during, and after procedures, using music to provide distraction, regulate attention, and support relaxation strategies. Goals of procedural support are to alleviate pain and agitation by regulating physiologic states, lowering arousal, and supporting the patient to return to a calm state. Music therapists also work closely with the palliative care team to address pain management, especially at the end of life. This can include live music at the bedside to promote comfort for the patient and family before and at time of death.
Functional Skill Reinforcement (PSS 4)
Music interventions in this domain focus on reinforcing or improving functional skills that are impacted by cancer and its treatment. Therapists use music to enhance motor, speech and cognitive skills and build tolerance to stimulation. Music therapists often co-treat with occupational, physical, and speech therapist to help patients, especially those with brain tumors, regain skills lost due to disease progression and/or treatment. Therapists use music interventions to motivate patient engagement in these therapies. Rhythm and melody are used to target specific outcomes related to rehabilitation. Examples include walking on a floor piano or standing to play drums to work on functional skills.
Resilience (PSS 9, 10, 13)
In this domain, therapists use music to support patients’ and families’ ability to endure, manage or overcome stressors such as loss of family cohesion and/or social support, and strengthen skills that promote coping, confidence, and hope. Resilience interventions often include music making, songwriting and therapeutic music education to encourage self-expression and increase self-esteem. Therapists also work with the family unit, including siblings, to help them manage their own stress. In addition to individual sessions, patients and their families have access to a weekly peer music group on the inpatient unit. At the end of a patient's life, the therapist works with the family to create legacy projects such as heartbeat recordings or personal songs that encourage reminiscence. Heartbeat recordings integrate the patient's heartbeat into a piece of music that is important to the family.
To best meet patient needs with available staff, the team employs a tiered service delivery model adapted from Ann Kazak's three-tiered Pediatric Psychosocial Preventative Health Model (Kazak, 2006), which prioritizes patients based on need using a gradient of service delivery. Given staffing limits, the model helps therapists identify patient/families whose needs are best addressed by music therapy services. Based on assessment, patients receive services at one of three levels: universal targeted, or clinical (Figure 1). Music therapists work closely with the psychosocial and medical care teams to prioritize care. For example, all inpatient Bone Marrow Transplant patients receive a music therapy referral and assessment. For hematology/oncology inpatients, referrals are made by a member of the psychosocial or medical team to address a specific concern.
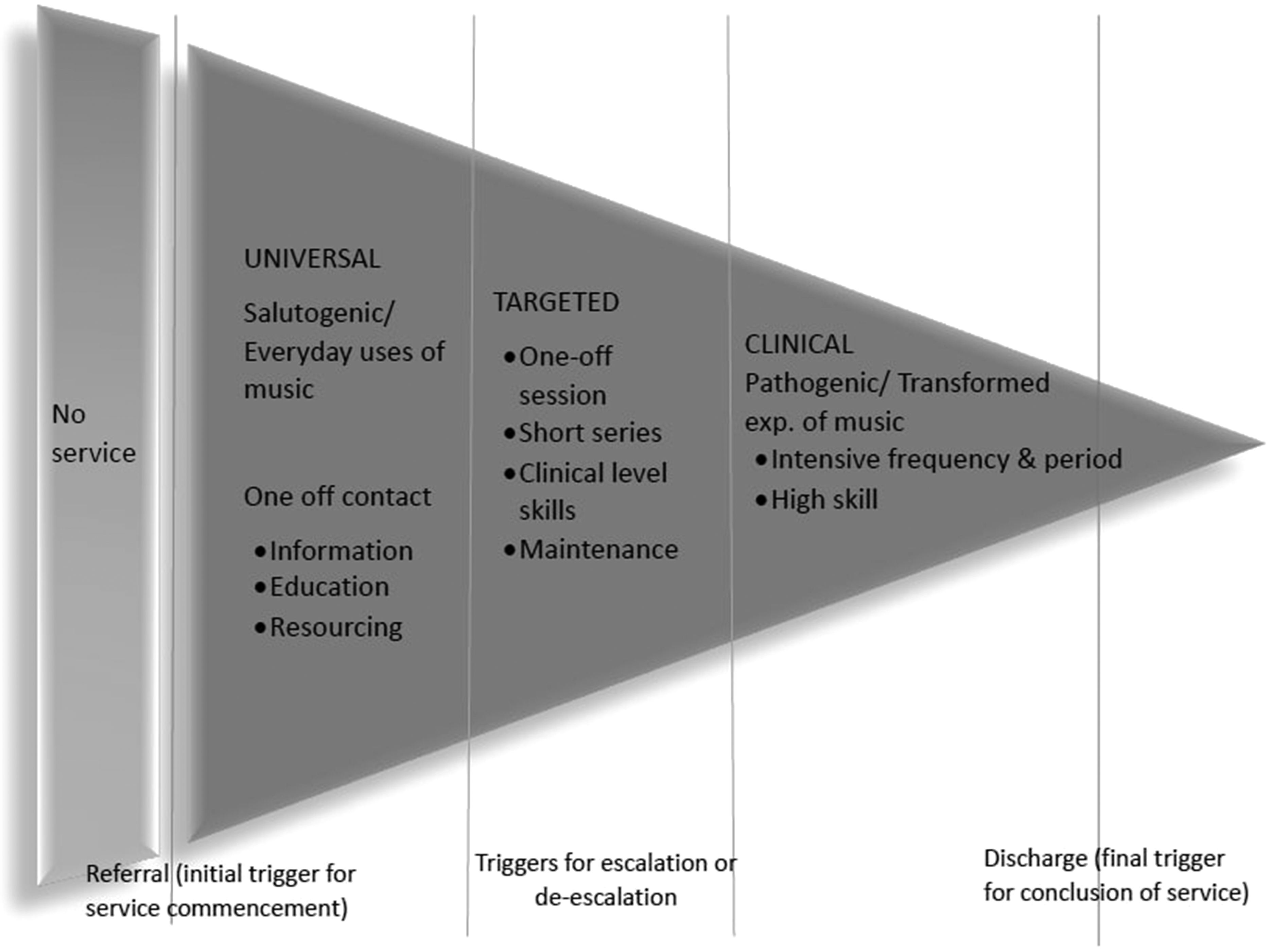
Riley hospital for children triage model adaptation of KAZAK's PPPH model (2006).
Case Example
This composite case example illustrates how specific Standards are being implemented through music therapy services.
Patricia was diagnosed with osteosarcoma at the age of 12 years. Her treatment required surgeries and multiple rounds of high dose chemotherapy. She struggled with side effects throughout her treatment. Patricia came from a tight knit family that included siblings, parents and grandparents. Unfortunately, her family lived over 2 h away, and they were not always able to be at her bedside. During her initial hospitalization, her primary nurse initiated a referral for music therapy services after noticing that Patricia really enjoyed watching movie musicals.
During the initial consult and assessment session, the therapist learned that Patricia had a history of music making outside of the hospital. Prior to her illness, she played piano, dabbled with the guitar and sang in the school choir. This information helped the therapist determine interventions that would aide in Patricia's coping with her new diagnosis. Due to the severity of her illness and marked change in her mood, the therapist recommended Patricia receive individual music therapy twice weekly and participate in a weekly music group on the unit as available (PSS4). The group involved patients of a similar age, with the goal of building community and providing socialization for patients, caregivers, and staff (PSS9). During her hospitalization, Patricia was able to receive individual sessions two to three times per week on a consistent basis. She attended music group only a few times due to her symptom distress.
During individual sessions, singing, playing instruments, and moving to music helped Patricia achieve functional goals (walking, reaching and bending) (PSS4), connect with her family (through shared music making and music video creation) (PSS6), and gain a sense of autonomy (through choice making during her hospital experience) (PSS4). Her family felt that participation in music therapy helped her feel safe in the hospital environment, motivated her to achieve challenging milestones in physical, occupational, and speech therapy and motivated her during treatment and recovery (PSS6). Her mother shared that music therapy sessions provided the first time Patricia smiled and wanted to be engaged in something. “She is working in music therapy, but she doesn’t realize it because for her, she is just having fun and that's what she deserves, to just be a kid. She is enjoying it.” her mother stated.
Following her initial course of treatment, Patricia's cancer returned. During this time, the music therapist focused more on her mental health and wellbeing (PSS4). Patricia began to engage in songwriting. She created songs to cancer- telling cancer how she felt, including her feelings about the diagnosis and relapse, as well as songs for her parents and siblings expressing her gratitude for them (PSS13). In addition, she wrote a song for the hematology/oncology unit and created a music video interviewing fellow patients, staff and caregivers (PSS9).
As her disease progressed, Patricia's pain was increasingly difficult to manage. The music therapist used Patricia's preferred music to provide an alternate focus during painful episodes, and education on how to use music listening or music-making as a self-management strategy for anticipated or actual pain (PSS8, PSS7). Music therapy services continued until Patricia was discharged to hospice care, where she used music to talk about and share her feelings about nearing the end of her life. She chose songs to share her concern and fear about leaving her family, and to communicate her love and appreciation. At Patricia's funeral, the family shared several of the songs she loved and some that she created as they gathered to celebrate her life (PSS13).
Children's Mercy Hospital Program
Children's Mercy Hospital (CMH) is a nonprofit, comprehensive pediatric medical center with 367 inpatient beds, 786 pediatric specialists on medical staff, and over 8000 employees. The Music Therapy department consists of four full-time board-certified music therapists, three clinically focused and one manager. Administratively, the department resides within the Patient and Family Services section of the Care Management and Patient & Family Services division of the hospital. The inpatient Hematology/Oncology/Bone Marrow Transplant (BMT) unit was the first area in the hospital to receive music therapy services in 1997, beginning with one part-time position. Today, the inpatient Hematology/Oncology/Bone Marrow Transplant unit is served by one music therapist, who also provides services to the Intensive Care Nursery and the Pediatric Intensive Care Unit.
Model of Care and Service Allocation
Prioritization of patients receiving music therapy services is based on research and best-practice models. Critical care, longer admissions, chronic need, and greater psychosocial complexity characterize these patients. Music therapy is integrated into the psychosocial treatment team that includes child life specialists, psychologists, social workers, hospital-based schoolteachers, chaplains, nurses and physicians. Regular communication between these professionals via psychosocial rounds and treatment team meetings assures that the needs of high-risk patients are met, and that all staff are supported in delivering the psychosocial plan of care. Music Therapy services are initiated via referral, either formal (order in the EMR) or informal (treatment team member communication of need). Each music therapist provides treatment sessions to approximately 5–9 patients each day and carries a caseload of between 20–30 patients.
Once a referral has been received, music therapists conduct a standardized assessment that includes information from the EMR and multidisciplinary team, an initial assessment session with the patient and family, and completion of the Music Therapy Therapeutic Needs Scale (TNS). The TNS was developed internally by the music therapy team and is consistent with the Pediatric Psychosocial Preventative Health Model (PPPHM) described by Kazak (2006). The PPPHM is a “biopsychosocial framework for assessing and treating families of children in pediatric health care settings” (p. 381) and involves a collaborative approach to care across members of the multidisciplinary treatment team to match patient/family strengths, needs and risk to appropriate services (Kazak, 2006). While the TNS is not as comprehensive as the PPPHM, it does include items representative of the patient and family's strengths, presenting concerns, diagnoses, and psychosocial risk factors, and assists the therapist in identifying the most appropriate level of care for the patient and family along the music therapy continuum of care.
The TNS produces a score that places the patient into one of four levels, representing the continuum of care provided by music therapy services (Figure 2). Patients assessed as Level one have a higher level of identified needs and generally receive 3–4 music therapy sessions per week. In contrast, patients assessed at Level four generally have good support and coping skills, and they usually benefit from lower intensity service. An example of this level of care would include occasional visits (1–2 times a week) from a music volunteer and/or brief interactions with a board-certified music therapist. TNS scores, interactions with the patient/family, and consultation with the multidisciplinary team collectively drive decisions concerning where the patient/family can best be served along the continuum of care. The music therapy treatment plan and session documentation are fluid documents in the EMR that are updated after each music therapy session, thereby providing information to the treatment team about the current status of the patient and their progress.
Music Therapy Continuum of Care.
Case Example
This composite case example illustrates how specific Standards are being implemented through music therapy services.
John is a 7-year-old male, admitted to the inpatient hematology/oncology unit with a diagnosis of acute myelogenous leukemia (AML). This is John's first inpatient hospitalization. He presents with fever, fatigue, bone pain, lower extremity weakness when ambulating, and is anxious when unknown people enter his room, including treatment team members. He is receiving chemotherapy and is expected to be in the hospital for 2–3 weeks.
His family consists of his mother, father, and a 2-year-old female sibling. They live in a small town two hours away from the hospital. Mother and sibling will remain with John at the hospital, while father returns home to work as he is the primary financial support for the family. Parents are concerned about John's prognosis and comfort level. John and his parents are also concerned about continuing with school as he likes school and is missing his peers. Additional stressors for the patient and family include their separation during hospitalization and the financial burden of the additional travel for visits.
His nurse refers him for music therapy after learning of John's love of music. He is excited to hear that this will be part of his treatment plan. The music therapist starts the assessment process by consulting with the treatment team and providing an initial session to better understand John's strengths and needs (PSS 15). The MT documents the session and completes the TNS in the EMR. John is assessed as level two because he presents with a new diagnosis of a potentially life-threatening disease, first hospitalization, pain and physical weakness, separation from friends, and anxiety with care providers. The family also needs support as they learn how to comfort and care for John while coping with separation. The music therapist determines that a session frequency of 2–3 times per week for the duration of John's admission will best meet the needs of John and his family (PSS 1).
The documented treatment plan includes music interventions to increase comfort, decrease anxiety, and promote coping via opportunities to experience autonomy and mastery (PSS 4). The music therapist provides developmentally appropriate preparation and support for procedures as well (PSS 8). To support the family, the music therapist engages them in music-making to encourage family cohesion and well-being (PSS6). More specifically, when his sister is present, she will be included in sessions to encourage sibling engagement and promote support and belonging in the care environment (PSS 10). Treatment team members will be included in sessions of music-making or singing to build rapport (PSS 9). John's progress will be documented in the EMR and discussed during weekly psychosocial rounds (PSS 15).
Discussion
Providing appropriate psychosocial care to children with cancer and their families requires effort, communication and collaboration from the entire multidisciplinary team. The Standards for Psychosocial Care were developed to provide guidance for optimization of this care. Advancing them from paper to practice and idea to implementation requires a collective and coordinated effort. Recent initiatives have focused on raising awareness about the Standards, supporting their implementation within cancer care settings, and assessing their integration across disciplines to maximize efficiency and effectiveness (Jones et al., 2018; Kazak et al., 2018; Kazak et al., 2019; Scialla et al., 2017, 2018; Wiener, Canter, et al., 2020; Wiener, Kupst, et al., 2020).
Music therapy practice has not previously been assessed for alignment and integration into the Standards despite playing an integral role in the care of children with cancer and their families. Bringing all psychosocial care providers into the work at this point is vital. Initial development of the Standards and subsequent survey studies have focused on four primary psychosocial disciplines including child life, social work, psychology, and psychiatry (Jones et al., 2018; Kazak, Scialla et al., 2017, 2018; Scialla et al., 2018; Wiener et al., 2015a, 2015b). These provider groups are integral to psychosocial care. However, the psychosocial team is often larger, including additional disciplines such as chaplains, hospital teachers, care coordinators, and creative arts therapists – including board-certified music therapists (Scialla et al., 2017).
To initiate conversations about the role of music therapy in psychosocial care, this paper explored research, clinical practice survey data, and program descriptions to identify which Standards music therapists are implementing. Music therapy services are consistent with nine of the fifteen Standards and span the continuum of cancer care, beginning at the time of diagnosis, continuing through active treatment, and are often prioritized for patients with high palliative and end-of-life care needs. In addition, services are not limited to the child or AYA with cancer, and often address the needs of parents, caregivers, and siblings as well. This suggests music therapy can assist psychosocial care teams in meeting most of the Standards including those identified as being less often met, such as palliative and bereavement care and the provision of parent and sibling support (Scialla et al., 2018). At many hospitals, music therapy services are also well integrated into the larger program of psychosocial care as evidenced by use of referral systems, documentation through the EMR, interdisciplinary collaboration, and participation in psychosocial rounds.
Survey studies indicate that psychosocial care teams generally have a small number of providers who represent a wide range of disciplines (Jones et al., 2018; Knott et al., 2020; Scialla et al., 2017). This places teams at risk for providing fragmented care and necessitates broader conversations to support the integration and prioritization of services across disciplines. Music therapy programs, which often have a high patient to therapist ratio, have adopted a tiered approach to services, providing direct services to patients with acute needs, but also developing and implementing music programming that can be more universally applied to meet the needs of lower risk patients and families. These programs allow music therapists to share their skills and expand the reach of their service through trainings for other healthcare team members and music volunteers. The coordination of such care with other providers ensures that each patient and family is receiving care that meets their individual needs while promoting appropriate stewardship of the often-limited psychosocial resources. Assessing the extent to which specialized psychosocial staff members, like music therapy, are available at pediatric cancer programs is a natural next step to advancing implementation of the standards.
The music therapy practice survey (Knott et al., 2020) provides preliminary data concerning the availability of music therapy services, but the survey was not targeted specifically to pediatric cancer programs. Similarly, we have limited data concerning the extent to which each Standard is being implemented and integration of services within the larger psychosocial care team. As such, we recommend a national survey of pediatric cancer programs to determine the availability of music therapy and to identify how the Standards are being met through these services. We recommend the survey be modeled after practice surveys conducted by the Psychosocial Standards of Care Project for Childhood Cancer team (Jones et al., 2018; Scialla et al., 2017, 2018) to expand on initial findings centered on social workers, child life specialists, psychologists, and psychiatrists.
As previously stated, the Standards were developed to identify key assessments that every patient and family should receive to optimize psychosocial care. Nurses are in a unique position to identify needs due to their proximity and prolonged contact with patients and families. This makes nurses a natural fit for promoting the standards of care on a broad level, while ensuring patients receive the services they need on a more focused level. Knowledge of available services is an important first step to enacting these efforts. Music therapists are working as collaborative members of the psychosocial care team, providing evidence-based services that align with the Psychosocial Standards of Care. Increased awareness is necessary for the integration of music therapy services as psychosocial and healthcare professionals strive to provide the most personalized, comprehensive care to patients and families dealing with cancer and blood disorders.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Institute of Nursing Research (grant number R01NR015789).