
Abstract
Background
Palliative care is a key component of the healthcare system, yet structurally vulnerable populations face significant barriers to accessing it and its support in care planning. This study explored beliefs, needs, and concerns related to palliative care and advance care planning among these populations.
Methods
Two semi-structured focus groups were conducted in major cities in the province of Quebec, Canada, in May and August of 2022. Participants had to be at least 18 years old and be able to speak and understand French. They also had to attend or use the services of a partnered community organization serving the target population. Data was analyzed according to the thematic content analysis approach.
Results
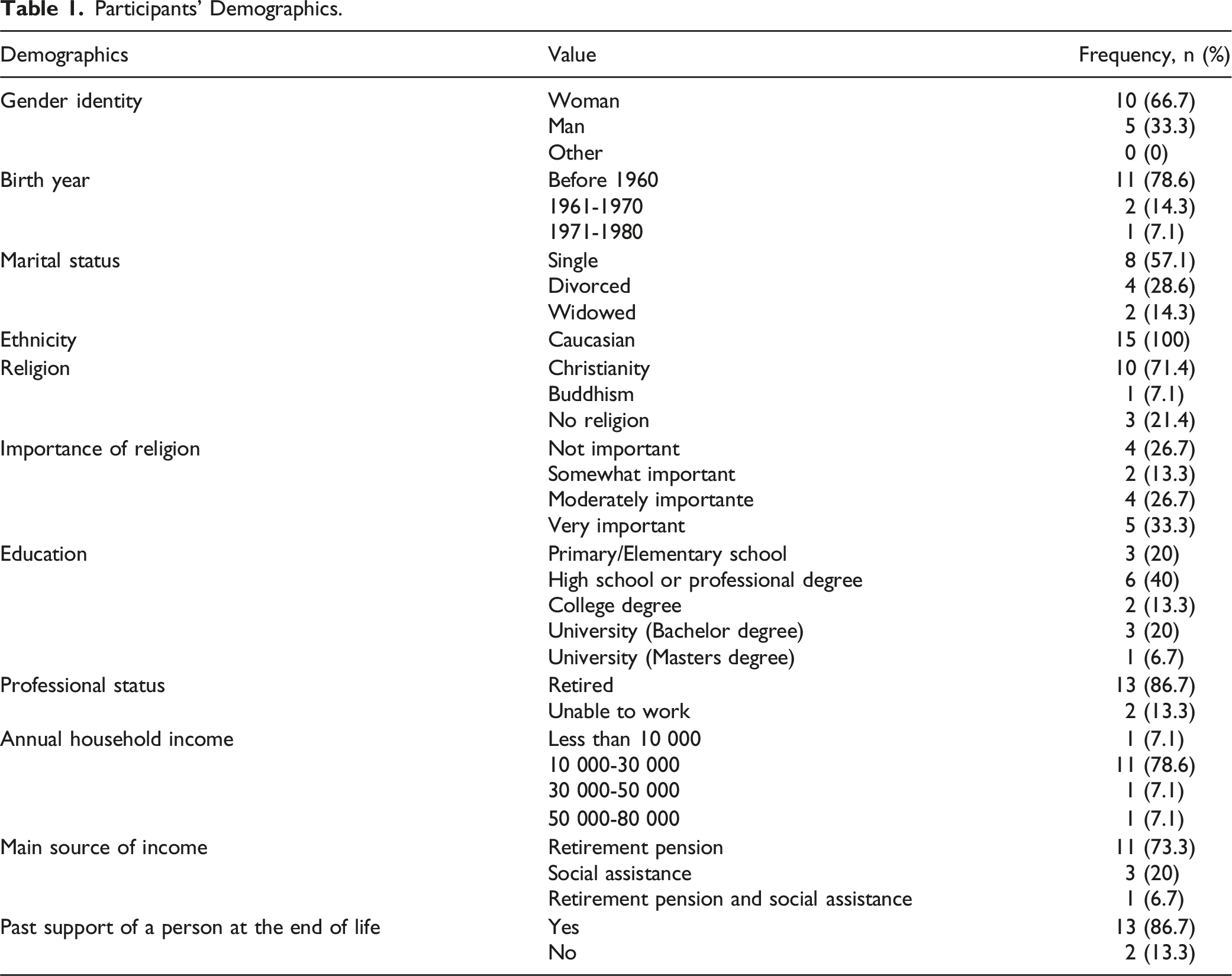
Fifteen (15) persons participated: all were Caucasian, and most were women, born before 1960, single, and retired. Misconceptions and a lack of awareness of the various palliative care options were generally observed among participants. Experience with caring for a dying person, access to a family physician, and access to a legal professional were identified as elements promoting awareness of palliative care. Participants raised an urgent need for more accessible information about palliative care and advance care planning, and for more access to care.
Conclusions
A good understanding of palliative care options helps individuals and families make informed decisions and be better prepared for the end of life. Structurally vulnerable people urgently need accessible information to support this preparation. This study supports the development of equity-focused policies and tailored interventions to improve access and planning for this population.
Keywords
Introduction
Palliative care is recognized by the International Association for Hospice and Palliative Care as ‘‘the active holistic care of individuals across all ages with serious health-related suffering due to severe illness, and especially of those near the end of life’’. 1 Palliative care should be available in all care settings and be provided based on need rather than prognosis. 1 Integrated early palliative care enhances the quality of life and well-being of both patients with advanced illnesses and their family. Patients who received early palliative care experience a broad range of benefits, including better physical symptom management,2,3 extended survival,4,5 and enhanced quality of life. 6 Additionally, caregivers report higher levels of satisfaction 3 and reduced symptoms of depression. 7 Palliative care has become an integral component of the World Health Organization’s framework for Universal Health Coverage, 8 and access to quality palliative care is recognized as a human right, ensuring individuals facing life-limiting conditions receive compassionate care.9–11 Yet, it has been identified as one of the most inequitable areas of health care worldwide, as only about 14% of people who need palliative care currently receive it. 11 There is a growing need to improve equity and early access to palliative care for all, especially for underserved populations, which is recognized in the Action Plan on Palliative Care in Canada. 12
While access to palliative care for older people has emerged as a key area of focus for researchers amid population aging, the impact of structural vulnerability on such access remains significantly understudied. Structural vulnerability refers to the risk of negative health outcomes that arises from an individual’s or population group’s position within overlapping socioeconomic, political, and cultural power hierarchies. 13 Individuals are considered structurally vulnerable when their place within these intersecting hierarchies—such as socioeconomic status, race, or cultural identity—and their institutional or policy context (e.g., immigration status, employment) limits their ability to maintain a healthy lifestyle and their access to healthcare. 13 Structural vulnerability is dynamic, evolving with external forces such as policy changes or economic shifts that impact access to resources. 14
Structurally vulnerable populations experience disproportionate and overlapping barriers to healthcare access.15–17 These inequities continue and exacerbate at the end of life. Stigmatization, reluctance to seek medical care following negative experiences, prioritization of daily survival over care, and having difficulty navigating the complex and rigid healthcare system can prevent them from accessing the services they need at the end of life, altering their quality of life.16,18 Paradoxically, structurally vulnerable people also require more care due to adverse health outcomes resulting from significant systemic challenges and disparities in social determinants of health such as wealth, education, health literacy, and access to quality healthcare.15,16,19,20 Moreover, structurally vulnerable individuals who desire to live the end of their life outside of the conventional healthcare system, whether at home or in a trusted environment (e.g., shelter), encounter considerable obstacles. Specifically, recent studies documented a lack of accessible and safe public and community infrastructures and services for providing palliative care outside of institutions, especially in the context of substance misuse issues and for homeless people.21,22,23 They also highlighted gaps in procedures for health teams, social stigma and discrimination, challenges managing pain in the context of substance use, and limited social support.21,22,23 However, studies on the topic are scarce and predominantly focused on homeless populations or those with substance use issues, and not on low-income or less-educated individuals in general.
A structural gap in death literacy is also known as a barrier to dying at home and to advance care planning (ACP). 21 Health literacy commonly refers to “the degree to which individuals have the capacity to obtain, process, and understand basic health information and services needed to make appropriate health decisions”24,25 As a direct determinant of health, health literacy affects people’s health and quality of life, but also indirectly influences access to health information, such as documentation on palliative care, and the use of health services.26–29 Structurally vulnerable people often have low levels of literacy,27,30 and are less likely to have meaningful information and awareness of palliative care,31–34 therefore, they could be less inclined to approach these services for support. 35 Structural vulnerability is also associated with less knowledge of ACP options.31,36
Death literacy refers to a body of knowledge and skills that enable people to understand and act on palliative care and dying options.37,38 Death literacy is made up of four functionalities: knowledge, skills, experiential knowledge, and social action. 38 According to this framework, caring for a dying person can be an opportunity for people to develop their knowledge of death. 38 A Death Literacy Index was developed to assess interventions with individuals, communities and societies, and has recently undergone validation in Turkey, China, Sweden, and the UK.39–42 A recent study showed an association between sociodemographic factors (widowhood, being older and having a religious or spiritual belief) and higher levels of death literacy according to the death literacy index but did not find an association with gender or education level. 43 Enhanced death literacy was substantially correlated with experiential characteristics, including involvement in palliative care, supporting a bereaved individual, and engaging in paid or informal labour with dying or grieving individuals. 43 Furthermore, our previous research findings revealed significant gaps in knowledge about palliative care practices among individuals with lower levels of education and among those experiencing financial hardship. 33 While these factors often intersect, educational attainment and socioeconomic position may shape individuals’ understanding of palliative care through different pathways. More studies on the influence of sociodemographic factors on death literacy and on means to develop structurally vulnerable populations’ death literacy are needed to enable them to act on palliative care options.
In Quebec, Canada, Medical Aid in Dying (MAiD) (The administration by a physician or nurse practitioner of drugs that cause death (clinician-administered medical assistance in dying) or the prescription of a drug that an eligible person takes themselves to cause their own death (assisted suicide). 44 ) was legalized in 2015 under the Act Respecting End-of-Life Care, which also regulates continuous palliative sedation (The administration of medication to reduce consciousness in the treatment of intolerable and refractory symptoms in patients with an advanced progressive illness, often continued until death. 45 ) and advance medical directives, a mean to express end-of-life preferences (Advance care planning is a process that enables individuals to define and communicate their preferences for future medical care and decision-making. This involves discussions about values, goals, and treatment preferences, and it can include the documentation of these preferences to guide healthcare providers and families if the person becomes unable to express their wishes directly. 46 ). 47 Given the multitude of treatment options and recent legislative changes, it is important to study what structurally vulnerable people know about existing options and their needs to ensure equitable access to care. Furthermore, few studies on palliative care provide structurally vulnerable people with the opportunity to express their needs and concerns and to reflect on solutions.
Purpose
This study aimed to explore the beliefs, needs and concerns of structurally vulnerable populations concerning palliative care and ACP.
Conceptual Framework
The conceptual framework of death literacy, developed by Noonan, Horsfall, Leonard and Rosenberg 38 guided our study and, consequently, the development of the interview guide and the analysis of the results. Questions relating to the four functionalities of death literacy, namely the knowledge, skills, experiential knowledge, and social action, were included in the interview guide. The interview guide includes questions pertaining to the four dimensions of death literacy: knowledge, skills, experience knowledge, and social action. 38
Methods
Study Design and Qualitative Approach
A descriptive qualitative design was chosen to provide comprehensive descriptions of experiences and perceptions related to specific phenomena48,49 and interpret the meanings individuals attach to events, helping to grasp human experiences.50,51 This approach was deemed most suitable for understanding the beliefs, needs, and concerns of people facing situational social and economic vulnerabilities regarding palliative care, while allowing analysis through the death literacy framework. Focus groups were selected for data collection, as they allow gathering information on specific situations 52 and exploring perceptions, feelings, attitudes, and motivations. 53 This method is particularly useful with marginalized groups, as it provides a space for expressing views and can foster awareness of their own situation. 52
Researcher Characteristics and Reflexivity
The main researcher, a master’s nursing student and experienced emergency room nurse, brought her clinical expertise to the research despite having no prior experience as a researcher. The research team had expertise in either ACP, palliative care, or health promotion, but were not experts in all three domains simultaneously. The master student led the data collection after reviewing literature on conducting focus groups and engaging in detailed discussions with one of her supervisors, who has over 20 years of experience working with structurally marginalized communities. Additionally, the research team consulted community groups on our approach and research questions, discussing our concerns to ensure relevance and sensitivity to participants’ needs. The main researcher had no prior contact with participants and maintained a logbook to document research progress, communication strategies, and reflections, which she shared with her supervisor.
Sampling Strategy
The target population consisted of structurally vulnerable individuals. Participants were recruited through two community organizations that serve financially or socially vulnerable populations, with whom we established a partnership. To qualify, participants needed to be at least 18 years old and able to speak and understand French. We collaborated with organization representatives to ensure diversity in the sample regarding age, sex, gender, and racialized status. Community workers approached potential participants to gauge their interest in joining the focus groups, as many lacked access to the Internet or a phone. We provided the community workers with a document containing essential information to share with potential participants, along with a poster for display at the organization’s premises. Each discussion group aimed to include between four and eight participants, a number chosen to foster a comfortable environment for sharing and interaction. 54
Data Collection Instruments
Focus Group Guide
The interview guide was semi-structured to foster discussion and allow unplanned topics to emerge [see Additional file 1]. Developed by the research team, it included various themes to be addressed in no specific order, depending on the flow of conversation. These themes covered beliefs about palliative care practices such as MAiD and continuous palliative sedation, ACP, expectations and challenges in planning end-of-life care, factors that facilitate knowledge development, and additional needs. Before the focus groups, the guide was reviewed by community organization workers to ensure appropriateness and accessibility for the target population.
Socio-Demographic Questionnaire
All participants completed a socio-demographic questionnaire, pre-approved by community organization partners. It included questions on gender identity, age, marital status, ethnicity, religion, education, professional status, family income, and experience with the end of life.
Data Collection and Processing
Two semi-structured focus groups were conducted in May and August 2022, each lasting about 90 minutes and audio recorded with participants’ written consent. Participants received monetary compensation, and the sessions took place at the organizations’ premises. Community organization workers were present to help build trust and support communication through clarifications, concise summaries, and reformulations.
Data Analysis
A thematic content analysis approach was used to identify, analyze, and interpret themes within the data. 55 Data analysis began during data collection, as discussions raised new questions and topics.56,57 Focus group recordings were fully transcribed, followed by a “vertical” analysis: an initial overview, a detailed reading alongside field notes, and a coding process to extract key words and expressions indicative of meaning. 58 Another researcher independently coded the data, and the themes were discussed collaboratively. Guided by the death literacy framework, themes were categorized into main and sub-themes. To enhance trustworthiness, preliminary results were reviewed by the research team, refining themes and interpretations.
Data Validity
After the second group, results from the first group were discussed with the second group to assess the concordance and plausibility of the interpretations 59 and to strengthen validity. Triangulation of research methods (with our initial study 33 ) further supported result validity. 60 External validity was strengthened by involving a substantial number of participants across two focus groups. Lastly, the findings were reported following the Standards for Reporting Qualitative Research checklist. 61
Results
Participants’ Demographics.
Beliefs regarding Palliative Care
Participants generally expressed having limited knowledge about the different palliative care options. Many stated that MAiD is more widely discussed in the general population, but that the difference between MAiD, continuous palliative sedation, and palliative care was not clear for them. Only one participant was aware of continuous palliative sedation. Although many participants knew that MAiD is legal in Quebec and involves the administration of medication at a specific moment to cause death, they held varying beliefs and understandings about this practice. One participant expressed the belief that the morphine administered to their relative at the end of life accelerated their death, drawing a comparison to MAiD or assisted suicide: She asked for medical aid in dying, but the doctor said that it would take too long, but that he could help her die faster, without pain. I think that's it; they injected her with morphine or something, and then she died three days later. But we knew she was going to die. We had been warned that she had started the treatment, and she was going to die. That's almost like assisted suicide.
In this verbatim quote, when questioned about MAiD, the participant implies that their relative, who had been receiving morphine for 3 days, was receiving a form of MAiD. However, this situation resembles palliative care but does not constitute MAiD according to its legal definition. Furthermore, a participant who had previous experience in caring for a relative at the end of life believed that MAiD was the administration of medication on a long-term basis, which is not aligned with MAiD (administration of medication meant to cause death in a very short time). Another participant talked about the “last injection” that causes death up to the day after the injection: It's normal that when you give the last injection, it can take one hour, two hours, 10 minutes, a day, a night. But it is certain that you will leave (die) with it.
In this verbatim quote it is unclear if the participant incorrectly thought that MAiD takes hours to cause death or if they thought that the administration of medication in palliative care hastened death. Nevertheless, it highlights confusion about these practices. Finally, many participants were unsure how to access MAiD, and some were unaware of the eligibility criteria or where to find more information about it.
Beliefs About Advance Care Planning
Participants had some knowledge of ACP. Many said they had designated a proxy for incapacity, and some said they included provisions in their advance directives indicating no resuscitation in case of cardiac arrest. Some had shared their wishes with loved ones. One participant mentioned that after their parents completed their ACP, they and her family created incapacity mandates and informed relatives of their wishes. Others had considered their preferences, such as for resuscitation, but hadn’t documented or communicated them.
Factors Influencing Access to Information
Experience with the End of Life
Participants with experience caring for individuals at the end of life generally had a better understanding of palliative care, which prompted them to reflect on their own end-of-life situations and wishes. However, some had misconceptions despite their experiences. Many felt minimally involved in decisions regarding end-of-life options, expressing that their families played a passive role and had little influence over the care and decisions made by healthcare professionals.
Perceptions of Family Physicians’ Access and Role in End-of-Life Conversations
Some participants expressed that they felt fortunate to have access to family physicians who were available to listen to their concerns. Those with access to a family physician indicated that they could likely obtain information about palliative care if they asked about it. Participants noted that many people in Quebec have access to a family physician, making them ideal professionals for providing information about palliative care and ACP. Many participants had a family doctor. Conversely, according to participants, a lack of access to a family doctor complicates obtaining information on these topics and hinders the process of ACP.
However, some participants discussed the inadequate communication of family physicians regarding palliative care and ACP. They felt that family physicians do not initiate discussions on these topics with their patients, or fail to communicate effectively when they do, creating a significant barrier to accessing essential information. One participant argued that it should be mandatory for family physicians to inform their patients about palliative care and ACP. In contrast, some participants believed that family physicians might not be the best suited for these discussions due to their heavy workloads, which limit the time they can spend with each patient, and their own lack of confidence in addressing such topics. As one participant said: I wouldn't go down that road. They are in such a hurry. I don't have that vision; I think they stick to the usual questionnaire, and that's fine. [...] Well, that's because I wouldn't trust the family doctor to inform people.
These remarks imply that for them, family physicians could not be the most trustworthy to inform their patients about these issues. Another participant suggested that more specialized professionals might be better equipped and suited to discuss this matter. Additionally, those who had cared for a relative noted that the interdisciplinary team often failed to communicate the various palliative care options and their implications to patients’ families. This lack of communication led to misunderstandings among family members, the patient, and the medical team, creating friction and making the end-of-life experience more challenging.
Access to Legal Professionals
Some participants had used ACP, particularly the appointment of a proxy and advance directives, during a consultation with a notary who discussed various options with them and provided valuable guidance. One participant noted that their consultation with a notary was facilitated by a community organization they attend. However, another participant pointed out that since the notaries are not present in hospitals during healthcare experiences, the responsibility for conveying information about ACP falls to the individual or their proxy.
Lack of Access to Governmental Information
Participants highlighted the absence of clear information on palliative care and ACP provided by the government. They described the difficulty of accessing information on hospice palliative care, particularly for individuals without Internet access or those who struggle to read and comprehend online information. Many participants emphasized that the government should be responsible for informing people about their ACP rights.
Representation in Art and Culture
One participant discussed the representation of palliative care in art and culture, noting its importance in raising awareness and understanding. They recounted watching a film about MAiD which provided valuable insights into the procedure and its implications. This experience highlighted how artistic expressions can play a crucial role in informing the public and shaping perceptions of palliative care options.
Issues and Needs regarding the End of Life
Lack of Access to Health Care
A participant discussed convincingly the issue of access to quality care for marginalized people: In all care in the Ministry of Health, when you're poor, or you're homeless, homosexual, you suffer prejudice. It's a very conservative environment. If, on top of that, you have a psychiatric diagnosis, not only do you get bad care, but you also better forget about end-of-life care; it's certain that you won't get it, that's for sure; I'm convinced of that.
This verbatim quote highlights their perception of existing barriers in accessing quality and equitable health and palliative care for stigmatized groups. Another participant denounced the challenges associated with accessing mental health care, especially for older adults. Another participant, who agreed, stated that many older adults resort to suicide, which they mentioned as an option for coping with end of life, apart from palliative care. According to them, this has been a path taken by some of their loved ones who struggled to accept the decline in their quality of life due to illness.
Administration of MAiD to Vulnerable People
One participant expressed deep concern that with increased access to MAiD, vulnerable individuals might receive it without their consent: That's what I think. Kids are like, “Oh well, Mom can't do anything; even if she goes, it doesn't matter”. I've seen patients in the hospital, and I'm still enraged by it, a lady who gave Christmas presents to all her children, and no one came to see her. What do you think would happen? They'd inject her. If I were a doctor, I'd wonder about that.
This passage reflects their fear that older adults who are no longer “useful” to society may receive MAiD without genuinely wanting to, or under pressure from their children.
Need for Accessible Information
The primary need expressed by all participants was for readily available information about death and dying, palliative care options, and ACP. Many participants indicated that such information was either not easily accessible, hard to understand, or both.
Suggested Courses of Action
More Involvement from Physicians
Some participants emphasized that physicians play a crucial role in educating patients about palliative care and ACP. One participant highlighted that family physicians bear a significant responsibility for the individuals they care for. Additionally, some participants expressed a desire for face-to-face dialogue with health professionals instead of relying on online information services. A participant conveyed strong emotions regarding the lack of services provided by healthcare professionals to educate patients and to address their questions: It doesn't have to be online precisely. It must be someone, a physical person in an office, that you knock on, “I would like information on something”. Does it exist? Because you must stop sending people systematically online. This is not a personalized service! What we need is personalized services. Not online.
This assertion implies that online information regarding health care is not sufficient, and facilitated access to consultations with qualified professionals is needed.
The Community as a Resource of Proximity
Many participants stressed the importance of personalized and accessible consultation or support services, which they found to be more prevalent in the community settings than among healthcare professionals. They identified the community as a valuable resource for information on palliative care and ACP. One participant proposed organizing discussion workshops where individuals could explore various palliative care and ACP options together. This participant believed that demystifying these topics through shared experiences would help people become more familiar with death and prepare for it: It's a subject that is too taboo. If we demystify it, through our lived experiences, I find that it's a preparation, it's like when there are prenatal courses, it's like learning to live with a new baby, I find that it could help to calmly tame death as you go through the stages. […] We must talk about it, exchange with others on it. I find that the information then becomes more real in your life.
This participant said that a shared preparation process to the end of life could be beneficial to better understand and prepare for this stage. Some participants also felt that a more personalized consultation service would be particularly relevant. They expressed that the support of a community worker trained in these topics would enhance accessibility and assist them in completing ACP documents. Such support could also facilitate Internet access for those without it at home, especially for learning about palliative care. Meeting with a qualified outreach worker could fulfill a vital need for reassurance about end-of-life issues.
Governmental Advertising Campaign
Many participants emphasized the need for a large-scale awareness campaign to educate the public about various issues related to palliative care and ACP. They suggested that the government should disseminate information on palliative care practices, ACP, and individuals’ rights through accessible public forums. This information should be regularly communicated through various media, including television, radio, newspapers, and the Internet. Additionally, one participant proposed sending letters to individuals upon retirement, informing them of the various palliative care options and how to proceed with ACP.
Telephone Consultation Service
Finally, two participants mentioned the potential of utilizing an existing governmental telephone health consultation service to obtain information about palliative care and ACP. They also discussed the idea of creating a new free and confidential telephone service for this purpose. However, they recognized that not everyone has access to a phone, which could limit this solution’s accessibility for the most vulnerable.
Discussion
This study explored the beliefs and understanding of palliative care practices and ACP among structurally vulnerable individuals, identifying significant gaps in accessible information and support. Focus group participants expressed limited knowledge of palliative care options and misconceptions about MAiD, underlying the need for clarity and reliable sources. Many stated that they had used some forms of ACP but pointed out obstacles in accessing both health care information and legal assistance. The availability and engagement of a family physician were seen as crucial for palliative care awareness, making the lack of access to such professionals a significant barrier. Participants criticized governmental information as overly complex and inaccessible, especially for those without Internet access. They suggested large-scale public awareness campaigns, a free telephone consultation service, and active involvement of family physicians and community organizations to bolster palliative care awareness. Community-based guidance and support were also recommended to help individuals better navigate palliative care planning and discussions. Participants raised concerns about the potential for MAiD to be administered to vulnerable individuals without proper consent. They also highlighted the broader challenges that marginalized populations face in accessing needed healthcare services.
Several studies have similarly associated socio-economic vulnerabilities with limited knowledge about palliative care, with our initial quantitative findings affirming that individuals living in poverty had on average a lower knowledge score (56.4%) regarding palliative care practices - such as treatment withdrawal, assisted suicide, administration of respiratory distress protocols, and MAiD - compared to those with higher incomes (70%). 33 Similarly, individuals with only a high school education level scored lower (58.6%) than those holding a university degree (72.9%). 33 These results are also consistent with other studies suggesting that individuals with lower incomes tend to have less knowledge about palliative care.32,36 A low level of education and literacy has also been linked to reduced understanding of various palliative care practices and their planning.62–65 People with lower incomes and low levels of education or literacy could therefore have lower death literacy. 38
Some focus group participants had already considered their end-of-life wishes and discussed them with close relatives. However, this may reflect a pre-existing interest in the topic, as those who chose to participate in the focus groups may have been more inclined to engage with the subject. These results also contrast with Tripken, Elrod and Bills, 36 who found that individuals with lower incomes are 27% less likely to have discussed their end-of-life wishes. Other studies suggest that less-educated individuals tend to talk more often about their preferences with family and clinicians, 66 while written tools like advance directives seem more frequently used by those with higher education levels. 67 A recent qualitative study in Quebec also suggested that advance medical directives may be unfamiliar to the general population of the province. 68 Even if the results highlighted knowledge gaps for structurally vulnerable people, misconceptions about palliative care also exist in the general population.62,69,70 In fact, participants in a recent qualitative study involving the general population similarly showed a general lack of awareness about palliative care. 71 The use of various terms and expressions internationally, such as “euthanasia”, “assisted suicide”, “medical assistance in dying” and “death with dignity”, could contribute to confusion regarding the specifics and legality of different practices.72,73
Results suggest a link between experiences and awareness and knowledge of palliative care and ACP, as participants who had supported individuals at the end of life reported a greater understanding of palliative care. This was consistent with results from a study about the general population in Quebec. 74 Similarly, a Northern Ireland study found that personal experience as a patient or caregiver contributes to gaining knowledge of these topics. 75 However, exposure to death does not guarantee accurate knowledge, and the depth of involvement in past experiences may affect understanding. This underscores the need for clear communication between healthcare professionals, patients, and families. This conclusion is also supported by a systematic review on physician-patient communication in palliative care. 76 Lack of access to and involvement of family physicians also hampers awareness, as they are key in accessing and coordinating palliative care.77,78 Yet studies indicate that many family physicians lack confidence in discussing palliative care. 79 Clinicians also often assume that structurally vulnerable patients are reluctant to engage in ACP due to mistrust or cultural beliefs, leading some to avoid these conversations or address patient goals superficially. 80 Rigid views on successful ACP, insufficient institutional resources, 80 and time constraints 81 further limit clinician engagement with vulnerable patients. Therefore, increased awareness, support, and training for clinicians could enhance access to information about these services. 82 A participant suggested that some older adults resort to suicide to avoid facing the decline of their abilities due to illness. This alarming fact deserves further documentation and further reinforces the importance of preventive action to raise awareness among individuals in need of palliative care about the different legal options available to them.
Participants recommended large-scale public awareness campaigns and a free consultation hotline to improve access to government information and raise public knowledge on palliative care. In a study by McIlfatrick, Noble & al., 75 television advertisements were suggested to educate and raise awareness about palliative care. Innovative dissemination methods, like podcasts, are getting created in Quebec and in Canada, and could reach a global audience, like a podcast in the UK on this subject. 83 Free consultation hotlines for individuals and health professionals exist in Taiwan, where the population prefers dying at home. 84 A retrospective study on this hotline revealed that 94% of calls from the general population were related to general inquiries stemming from a lack of knowledge and understanding of palliative care. 84 Many participants highlighted barriers related to digital exclusion, preferring in-person interactions over online resources. This finding indicates that palliative care and ACP initiatives must consider digital literacy and equitable access to ensure that vulnerable populations can fully engage with end-of-life planning. 85
Community-based services, such as personalized guidance and support groups, were proposed to empower individuals in their ACP. A recent systematic review on interventions aimed at facilitating ACP for vulnerable populations emphasized the need for improved, personalized, and holistic communication and better-equipped facilitators to support ACP decision-making. 86 Meet-up cafés and living labs could be innovative ways to discuss this matter in community settings, especially for the older adults. 87
Implications for Health Promotion and Equity
The findings suggest that structurally vulnerable individuals may have limited awareness of available palliative care practices and the process and criteria surrounding them. This may reflect a lower level of death literacy, at least in relation to the knowledge and skills components. Death literacy is built through learning about death and dying through direct experiences, fostering a community’s capacity to care for those at the end of life through empowerment and social support. 38 Consequently, these results imply that structurally vulnerable people may lack the knowledge and skills necessary to prepare adequately for the end of life, potentially feeling unprepared to care for their loved ones at home. As noted by a palliative care professional in Quebec, families lacking these skills are more likely to call emergency services, leading to hospital admission for dying individuals. 21
Comprehensive health literacy is crucial for health outcomes and has vast potential in health promotion by enhancing overall population health and addressing health inequalities. 28 Those with lower health literacy often face significant challenges in making informed care decisions due to communication barriers that limit their understanding of essential health terms.88,89 Ensuring the right to accessible, comprehensible information is key to ensuring that everyone can die with dignity.
A recent literature review suggests that establishing discussion groups, rooted in popular education principles, can foster knowledge exchange between professionals and communities. 90 These principles support empowerment of individuals and equitable conditions 91 and offers benefits for older adults in community-based health promotion initiatives, such as improved memory, self-esteem, reduced anxiety, and an enhanced appreciation for self-care. 90 They could be applied in community-based health promotion initiatives, including those aimed at enhancing understanding of end-of-life care and palliative options. In addition to advocating for improved access to information, healthcare providers, public health officials, and social service organizations should also support structurally vulnerable populations in navigating and understanding all available palliative care options. Efforts should address not only physical access but also eligibility, acceptability, and the availability of appropriate resources. Reducing these barriers must be a government priority, as they exacerbate vulnerabilities at the end of life and hinder death literacy development.
Future research should focus on interventions aimed at increasing awareness and training of clinicians on palliative care issues to enable them to discuss these subjects and ACP with their patients, especially those who are structurally vulnerable. Additionally, there is a need to explore the implementation and impact of community-based education approaches, such as compassionate communities - support networks for sharing end-of-life knowledge and skills 92 - particularly in relation to empowering structurally vulnerable populations. The compassionate communities model offers a promising approach to address these gaps by providing education, training, and support within the community. Such programs could empower individuals, enhance death literacy, and enable more confident participation in end-of-life care for themselves and others. 38 However, its effectiveness may be limited by the existing knowledge gaps and misconceptions about end-of-life care among community members.
Strengths and Limitations
This study has limitations. Firstly, the intended sample diversity was not achieved, as all participants were Caucasian. Research shows that racialized individuals experience the care system differently, particularly for palliative care.93,94 Additionally, many participants were women, who often serve as primary caregivers for the seriously ill95,96 and are generally more aware of palliative care options, preferring palliative care over curative treatments at the end of life. 97 Many participants had prior experience accompanying someone at the end of life, aligning with the death literacy framework. 38 While the relative homogeneity in terms of social context, age, background, status, and gender may have facilitated focus group interactions by minimizing power dynamics,98,99 it also limited the breadth of perspectives. The focus groups were conducted in urban community organizations, limiting insights into the realities of socio-economically vulnerable individuals in rural areas. In these areas, community and health resources may be less available, and health status and socio-economic conditions may be more disadvantaged, 100 however social cohesion may be higher. 101 Secondly, participants’ affiliation with these organizations and the presence of some university-educated individuals may have skewed the results, as they were likely more informed. Lastly, the study did not include comparisons with the non-vulnerable populations. While gaps in knowledge were observed among participants, existing literature suggests that limited knowledge of palliative care and ACP is also common in the general population.33,74 Without implying a quantitative difference, our findings highlight the specific experiences and challenges of structurally vulnerable individuals.
The data collection method that allowed structurally vulnerable individuals to share their knowledge and perceptions of palliative care is a key strength of this study. Since recruitment was carried out by community organization workers who are familiar with the individuals receiving services, many of the participants approached were talkative and felt personally engaged with the topic. Giving them a voice also helped demystify end-of-life care based on their lived experiences. The presence of community organization workers in each discussion group also seemed to facilitate trust-building with the participants, and many felt comfortable enough to share their situations and express their fears. Additionally, the intervention avenues discussed are those identified by the participants themselves and are therefore the ones they consider applicable to their situation. The focus group created a safe space for discussion, raising social awareness among participants. Participants learned from each other’s experiences, enhancing their awareness of their rights, and fostering empowerment. The focus groups also facilitated questions, alleviating concerns; for instance, all participants in the second group believed morphine hastened death, but they felt relieved to learn this was not entirely true. Many expressed interest in completing advance medical directives and thanked the researcher and workers for their support.
Conclusion
Participants identified varying levels of awareness regarding palliative care, highlighting gaps in knowledge and understanding that may affect decision-making about palliative care. Thus, the findings underscore the importance of educating the population about these topics. Participants expressed a significant and urgent need for easily accessible, simplified information regarding various palliative care practices and ACP. Several barriers to accessing and planning for this type of care were also identified, including discrimination against marginalized individuals, difficulties accessing family physicians, and insufficient information dissemination by the government and healthcare professionals. Potential solutions were also identified by participants to address the population’s needs and uphold every citizen’s right to information. These concrete solutions can be implemented by various stakeholders in public and private sectors, including the Quebec government, healthcare professionals and community organizations. Community-based interventions for death preparation and education, grounded in the principles of Health Promoting Palliative Care, 102 emphasize the significance of communities taking ownership of the dying process and death and strengthening its caregiving capacity. 103 Future studies should focus on better understanding the confusion surrounding end-of-life issues, which can lead to anxiety, disengagement, and reluctance to ask healthcare professionals questions—particularly because some people could believe they do not need to understand nor plan since access to MAiD is guaranteed. Increasing awareness of structurally vulnerable people about their end-of-life options and ensuring their wishes are respected in cases of incapacity is a crucial step toward equitable access to palliative care for all Quebecers, as stipulated in the Act respecting end-of-life care. Additionally, initiatives aimed at demystifying end-of-life issues could contribute to reducing stigma and improving the end-of-life experience for the population and have the potential to help everyone die with dignity, regardless of socio-economic status.
Supplemental Material
Supplemental Material - Exploring End-of-Life Perspectives in Structurally Vulnerable Populations: A Qualitative Focus Group Study
Supplemental Material for Exploring End-of-Life Perspectives in Structurally Vulnerable Populations: A Qualitative Focus Group Study by Anouk Bérubé., Sophie Dupéré, Diane Tapp, Ariane Plaisance in Community Health Equity Research & Policy
Footnotes
Acknowledgements
The authors sincerely thank the participants for their valuable contributions and express deep gratitude to the partnering community organizations. Their support in approving the interview guide, facilitating recruitment, and participating in the focus groups was crucial to the research’s success.
Author contributions
AB, SD, and DT designed the study. AB and SD conceived the focus group guide and the sociodemographic questionnaire, which were reviewed by DT. AB collected the data and did the transcription of the data. AB and SD interpreted the data. AB, SD, DT and AP revised the article critically for important intellectual content and approved the final version of this manuscript to be published.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The authors want to thank the following organizations for the scholarships they awarded to the principal author: Réseau québécois de recherche en soins palliatifs et de fin de vie (RQSPAL), Chaire de recherche en soins palliatifs de l’Université Laval, Ordre des infirmières et infirmiers du Québec (OIIQ), Ministère de l’Enseignement Supérieur, Faculty of Nursing of Université Laval, Centre de recherche de Montréal sur les inégalités sociales, les discriminations et les pratiques alternatives de citoyenneté (CREMIS), Institut d’éthique appliquée (IDÉA) de l’Université Laval, Fondation Desjardins, Caisse Desjardins de la Chaudière. These scholarships had no influence on the design, data collection, analysis, and interpretation, nor the dissemination of the results of this study.
Ethical Considerations
This project was approved by the Quebec Heart and Lung Research Centre (approval number MP-10-2019-3237).
Consent to Participate
Participation was voluntary and written informed consent was obtained after the consent form was read and explained to the group. Each participant was assigned a code to ensure anonymity and data was stored in the secure servers of the research center.
Data Availability Statement
The datasets supporting the conclusions of this article are available from the corresponding author upon reasonable email request.
Supplemental Material
Supplemental material for this article is available online.
Appendix
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.