
Abstract
Community-based participatory research (CBPR) and integrated knowledge translation (IKT) are methodological approaches that emphasize the value of equitable partnerships between researchers and community partners. The main difference between these approaches is that CBPR is advocacy-centered and aims at addressing inequities by instigating systemic and policy changes, whilst IKT is application- and upstream solution-oriented especially within the context of health and social care improvement. Previous studies that have used a collaborative approach mainly focused on either CBPR or IKT to a lesser extent.
The CAN-HEAL project employed an innovative methodological approach that integrates CBPR and IKT to address mental health needs among Arab immigrants and refugees in Ontario, Canada. Integral to this approach are three pillars: (1) establishment of a multi-level community partnership; (2) adherence to cultural sensitivity principles; and (3) commitment to social justice and application. The use of an CBPR-IKT approach led to numerous successes, including the co-development of a holistic upstream-downstream-based health promotion action plan to tackle inequities. This approach was associated with different challenges (e.g., limited resources), which were mitigated by employing certain enablers (e.g., assistance from community leaders). Based on lessons from this project, recommendations are made for governmental agencies and academic institutions to advance CBPR-IKT research to promote the sustainability and well-being of communities.
Keywords
Introduction
Background on Community-Based Participatory Research
Community-based participatory research (CBPR) has increasingly been used to effectively address health and social inequities among marginalized populations.1,2 CBPR is identified as action research, and its roots can be found in the global ‘northern’ and ‘southern’ traditions. 3 The northern tradition stems from Kurt Lewin’s collaborative research to tackle pressing community problems. 4 According to Lewin, 4 community members should be involved in all of the stages of the research process, including determining the issues that need to be addressed, developing a plan and taking action to address these issues. The southern tradition draws upon Paulo Freire’s emancipatory philosophy that aims to address societal inequities and bring about social change. 5 Freire argued that marginalized community members should be involved in research as subjects (not objects) by ensuring their full reflective participation in the act of their liberation, which could only be achieved by involving the community in directing the research process and tackling power differentials. CBPR is thus a collaborative approach that involves an equitable partnership between researchers and the community and recognizes each party’s unique strengths and experiences throughout the research process towards achieving common goals. 6 Participants in CBPR health research are active contributors to generating knowledge about their lived experiences, including those related to structural and social determinants of health. 6 The goal of CBPR is to emancipate community members and participants and ultimately bring about social change. 7
Community empowerment is an integral component of CBPR. There has been an increase in the use of participatory research tools which enable researchers to go beyond data collection towards empowering community members to push for social change.8,9 An example of a participatory tool is “Photovoice”, which empowers participants by enabling them to produce photographic evidence of issues that impact their lives with the aim of raising awareness and enacting policy and systemic change to advance social justice. 8 The CBPR approach emphasizes cultural sensitivity at every research stage by incorporating the community’s values and accommodating participants’ needs. 10 This approach is associated with many benefits, including acceptance of research by communities, generation of context-specific knowledge and community-informed solutions, and production of culturally appropriate pathways to community action, support and knowledge dissemination.11,12 The community-centered characteristics of CBPR make it an ideal approach for efficiently addressing the complex health and social needs of marginalized communities, including immigrants and refugees.
Background on Integrated Knowledge Translation
Integrated knowledge translation (IKT) is an emerging approach that aims to increase the relevance and applicability of study findings for knowledge users (i.e., those expected to act on research findings, such as practitioners, policymakers and community members) by shifting the research paradigm from a researcher-driven approach to a more equitable, partnership-based research model.13,14 IKT engages community partners and knowledge users at the outset of the study and continuously throughout the research process.15,16 The IKT approach addresses the underutilization of research knowledge by encouraging the production of upstream solutions for health and social care inequities.17,18 Initially advanced by the Canadian Health Services Research Foundation and then by the Canadian Institutes of Health Research, IKT has widely been promoted to produce applicable knowledge that enhances patient-centeredness within health and social care systems.16,19 IKT deploys collaborative principles that are similar to those of CBPR by emphasizing the value of equitable partnerships between researchers and community partners throughout the research process.7,20 Although IKT is a relatively new research approach compared to CBPR, researchers have been striving to set foundations to inform the implementation of IKT-based research. 21 Understandings and usage of IKT continue to crystalize as decision-makers, and researchers, together with community stakeholders, increasingly seek novel approaches to produce knowledge that is applicable to improving health and social care systems. 18
Similarities and Differences Between CBPR and IKT
The research practices of CBPR and IKT share common aim, the co-production of knowledge that is product of equitable partnership and expertise of researchers and community partners, known as knowledge users.6,7,20 Hence, CBPR and IKT are both methodological approaches that emphasize and facilitate engagement of knowledge users throughout the research process as active contributors to producing knowledge that serves to mitigate inequities and benefit society. 7 A unique characteristic of CBPR, however, is that it guided by principles that primarily emphasize social justice by incorporating advocacy, lobbying, and community empowerment activities to ultimately advance social transformation.22,23 This feature of CBPR allows it to produce research that yields social justice-oriented products (i.e., materials and interventions) and action (e.g., organizational and policy changes), preferably ones with upstream solutions, that address the root causes of health and social inequities.11,12 An example of CBPR study is the one by Breland-Noble et al 24 that partnered with Black people in the US to address historical abuse and mental health needs of this community with a goal of advancing social transformation.
IKT approach primarily focuses on producing research to generate applicable knowledge with upstream solutions to be applied in practice, particularly, in the context of health and social care systems.17,18 While this approach may eventually lead to social justice, its primary aim is to generate applicable knowledge to support and facilitate the needs of knowledge users. An example of an IKT-based study is the one by McGrath et al 25 that developed an applicable treatment program to support child mental health.
An Amalgamated Approach
Thus far, previous studies that employed a collaborative research technique have mainly focused on one or the other of these approaches, CBPR or IKT.7,20 In this paper, we argue that integrating both approaches is not only beneficial, but also crucial for effectively addressing complex health issues that are a result of social injustice and at the same time are socially stigmatized (e.g., mental health) among marginalized populations. This is fundamental for immigrants and/or racialized groups, who are often disproportionately disadvantaged by health inequities such as racism, and lack of cultural sensitivity in health and social care systems.26–28 For example, a review of mental health (MH) among Arab immigrants and refugees (AIR) found that this population suffers various structural stressors (e.g., discriminatory policies, post-September/11 increase in stereotyping) as well as barriers to equitable health and social care due to a lack of culturally sensitive services. 29 The review also noted that previous AIR-MH research is mainly biomedically centred and lacks in-depth engagement with the Arab community, which is crucial for cultural sensitivity, particularly for stigmatized topics like MH. Similar complex issues have been found for other racialized communities. For example, historical oppression against Black people in the US has contributed to poor MH in this population. 30 Further, the lack of availability of culturally sensitive healthcare has been associated with poor access to MH care amongst African Americans. 31 These examples underscore the need for integrated and novel methodological approaches to effectively address the complex health needs of marginalized communities. Integrating CBPR and IKT provides the opportunity to combine the strengths of both approaches; it allows for working collaboratively with community and knowledge users whilst ensuring cultural sensitivity throughout the research process towards advocacy, action, empowerment and conscientization for social reform as well as production of applicable knowledge with upstream solutions to improve healthcare practices and address health and social inequities.12,18 The combined CBPR and IKT approach serves to best promote immigrant communities’ health and well-being.
AIR Community and the Current Study
Between 2013 and 2024, Canada received about half a million AIR. 32 Ontario is the most Arab-populated province, where around 50% of AIR in Canada reside. AIR, like all immigrants, are at high risk for MH challenges, food insecurity and behavioural health issues, but they face distinct stressors (e.g., anti-Arabism, anti-Arab policies) that often exacerbate health and social inequities. A Canadian longitudinal study of MH among Syrian refugees (n = 1924) uncovered concerning prevalence of depression symptoms (15%) at baseline that worsened in year two (18%), with this decline being attributed to social and structural barriers (e.g., dissatisfaction with health and social services, low social support). 33 The 2023 Canadian income survey found high food insecurity rates among Arab-identified individuals compared to white Canadians (32% vs. 22%, respectively). 34 A scoping review of physical activity participation found lower attendance at exercise programs among AIR in Western countries, including Canada, compared to the broader population. 35 These examples underscore the various complex health and social inequities that AIR face, which require a holistic methodological approach to effectively address this population’s needs.
This article draws upon a Canadian study (CAN-HEAL, stands for Canadian Arab Nutrition, Health Education and Active Living project) that integrated both CBPR and IKT to address the MH needs, including those related to food security and physical activity among AIR in Ontario, Canada.36–38 Integral to the CBPR-IKT approach are three pillars: (1) development of an efficient multi-level partnership with knowledge users (community members, health and social care providers, and students who may be part of marginalized communities and/or future knowledge users); (2) adherence to principles of cultural sensitivity; (3) and commitment to social justice and application throughout the project (Figure 1). In this paper, we discuss these pillars after elaborating the study context below. We then present successes, challenges, and the enablers we used to attain project goals and overcome challenges. The paper concludes with recommendations based on lessons from this project for implementation by governmental agencies and institutions to advance CBPR-IKT research and to work towards equitable health and well-being for marginalized groups. Model that shows pillars of integrated CBPR-IKT approach, structure of research actors, and associated outcomes in the CAN-HEAL project.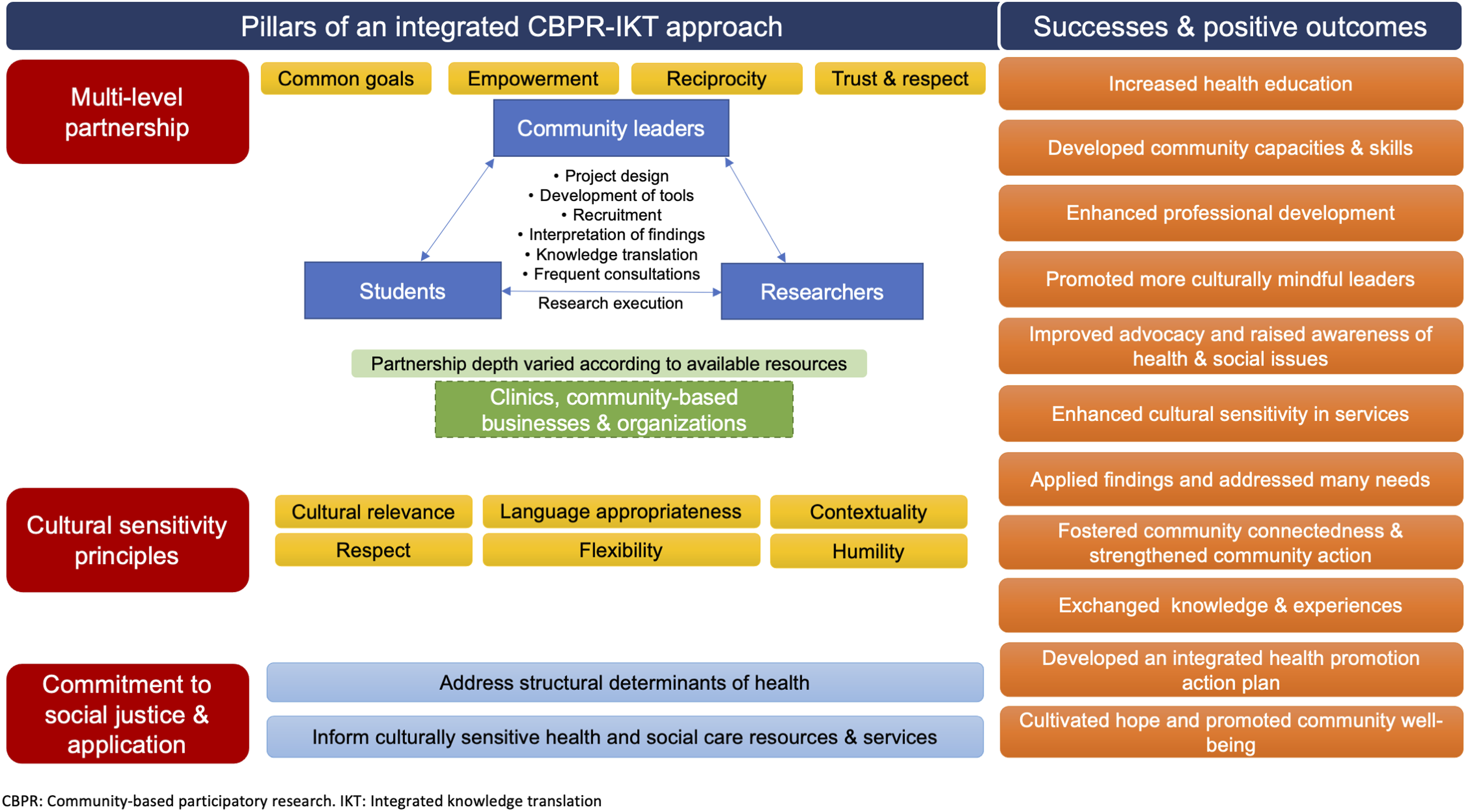
Study Context and Methodology
The CAN HEAL project was formed in partnership with AIR community members and knowledge users in Ontario, with the aim of promoting AIR’s MH and well-being. 36
Study Setting and Participation
Due to COVID-19 restrictions in 2020–2022, the Zoom platform was utilized to conduct this research. Three sampling approaches (convenience, purposive and snowball) were employed to recruit 60 socio-demographically diverse AIR participants. Eligibility criteria included being an AIR aged ≥18 years who originated from any of the 22 Arab countries 39 and currently lived in Ontario. Fifty percent of participants were aged 31–49, 73% were females, 90% were Muslims, 53% were voluntary immigrants, 36% were refugees, and 43% immigrated less than 5 years ago. More details about the characteristics of participants are reported elsewhere. 37 All participants provided an informed, voluntary consent. Ethical clearance of the study was obtained from the Research Ethics Board.
Multimethod and Theoretical Triangulation
A multi-method approach was adopted by employing three different research methods, interviews, Photovoice and a socio-demographic survey with questions about mental well-being, food security and physical activity. In the interviews, participants were asked about their experiences and factors that impacted their MH, food security and physical activity participation. They were also asked about solutions needed for addressing inequities and promoting MH. As part of Photovoice, participants shared and discussed photographs that depict their MH, food security and physical activity experiences as well as solutions for promoting health and social equity. Interviews aided in-depth exploration of participants’ experiences, whilst Photovoice empowered participants to creatively engage in critical reflection via symbolic imagery to elucidate their own lived realities pertaining to structural and social determinants of health. 40 This approach helped identify areas for policy change and inform innovative solutions, including initiatives performed as part of this project, as presented in this paper. More information about data collection methods used in this research can be found elsewhere. 37
To enhance reliability and applicability of the findings, the study adopted theoretical triangulation by deploying different frameworks. To thoroughly understand the complex contexts and factors that shape AIR’s MH and relate to inequities, the study used a social determinants of health (SDoH) framework. 36 The use of SDoH addresses health and social inequities by identifying and informing areas for potential social transformation as per CBPR. In addition, we used an integrated upstream-downstream framework to develop a holistic health promotion action plan that aims to reduce health and social inequities among AIR. The upstream-downstream framework emphasizes two strategies for addressing social determinants of health: (1) macro-level strategy that is tied to structural determinants of health and addresses the root causes of inequities, and (2) micro-level strategy that focuses on issues related to equitable access to health and social care resources that are tailored to each group’s needs. 41 The use of an integrated upstream-downstream framework aligns and serves the above-mentioned goals of CBPR and IKT.
Multi-Level Partnership Framework
A multi-level partnership was established from 2019 to 2021 with the community and knowledge users at the outset with continuous interaction and collaboration over the study’s timeframe (Figure 1). This involved partnerships with AIR community leaders, community organizations, clinics, community-based businesses, and postsecondary students. These efforts resulted in the establishment of a diverse advisory working group that collaborated on the project and shared a common goal of empowering AIR and other ethnic minorities across Canada to take action to improve their health and well-being. All partnering knowledge users mobilized resources within the community and followed principles of empowerment, trust, respect, and reciprocity (i.e., mutual exchange of knowledge).
Community Leaders
Partnerships were formed with 25 AIR community leaders (68% females, 56% young adults under 25) with experience in health, wellness, community engagement, activism and/or social justice from across Ontario. These were selected based on availability and interest to partner on the project. The lead author first consulted with them about the study topic and design to assure that they aligned with the AIR community’s needs. The community leaders were involved from the start to the end of the project, including the design of the project, development of research tools, recruitment, interpretation of findings, advocacy, and knowledge translation. Frequent consultations and discussions were held with the community leaders as needed throughout the study via virtual communication tools (e.g., the Zoom platform).
Community Organizations
Partnerships were formed with various community organizations (e.g., providing MH, wellness, and/or food services), clinics and community-based businesses based on recommendations from the partnering AIR community leaders. Partnership depth varied according to each organization’s available resources. Overall, community-based organizations collaborated mainly on participant recruitment, knowledge translation and advocacy efforts, with some virtual consultations and meetings about the study design and applicability of the findings. Clinics and community-based businesses supported knowledge translation initiatives and advocacy efforts.
Students and Youth
A team of students and youth from across Canada was formed. After receiving appropriate training, this team was involved in directing the entire research and knowledge translation processes. Involving postsecondary students as part of the research team in this project was based on recommendation from the partnering AIR community leaders to maximize the project impact, given the creative ideas and strong potential youth often possess as drivers of social change. There has been an increase in youth engagement models that call for involving youth as partners in health promotion research with the aim of enhancing study robustness, while contributing to the professional development of youth. 42 The TYPE Pyramid Model proposes that efficient youth engagement goes beyond understanding the research and the issues at hand and involves shared control and decision-making. 43 The McCain Model of Youth Engagement incorporates four integral principles to increase authenticity of youth engagement: (1) flexibility regarding roles and milestones, (2) mentorship for youth, (3) reciprocal learning between researchers and youth, and (4) authentic, shared decision-making. 44
We adapted this model by integrating two additional principles that further reinforced engagement: titles and leadership, and celebration. Self-reflective titles in community groups and organizations have been found to be associated with reduced emotional exhaustion, and improved performance. 45 Assigning titles and clear roles to youth throughout their involvement in directing this project motivated them and cultivated a sense of belonging. The CAN-HEAL student representative team constituted seven prime committees working towards the project goals. Each student was given a title (e.g., design and visualization lead), aligning with their interests and the project goals. There is growing evidence about the role that achievement celebration plays in enhancing joy in work and promoting team-building.46,47 Given the magnitude of this CBPR-IKT project and the need to motivate the team involved, frequent celebration of accomplishments was essential to foster motivation, ease transitions and acknowledge efforts. Celebrations included award ceremonies and multi-cultural events with prizes. These efforts collectively resulted in an effective organizational climate that promoted success in the desired outcomes of the project.
Guiding Principles for the Project
The CBPR-IKT approach of the CAN-HEAL project was guided by commitment to social justice and application and principles of cultural sensitivity to enhance the study’s rigour and the meaningful application of the findings.
Commitment to Social Justice and Application
Commitment to social justice and application was integral to this CBPR-IKT project to effectively address the complex health needs in the AIR community. This has been guided by an upstream- and downstream-based action plan that was co-developed and informed by the CAN-HEAL research findings with the aim of achieving health and social equity and promoting AIR’s MH and well-being (Figure 2). Discussion of the commitment to social justice and application and examples of resources produced and initiatives held throughout the project towards social justice and application are presented below (Supplemental Files 1 and 2). Upstream-downstream-based health promotion action plan from the CAN-HEAL project.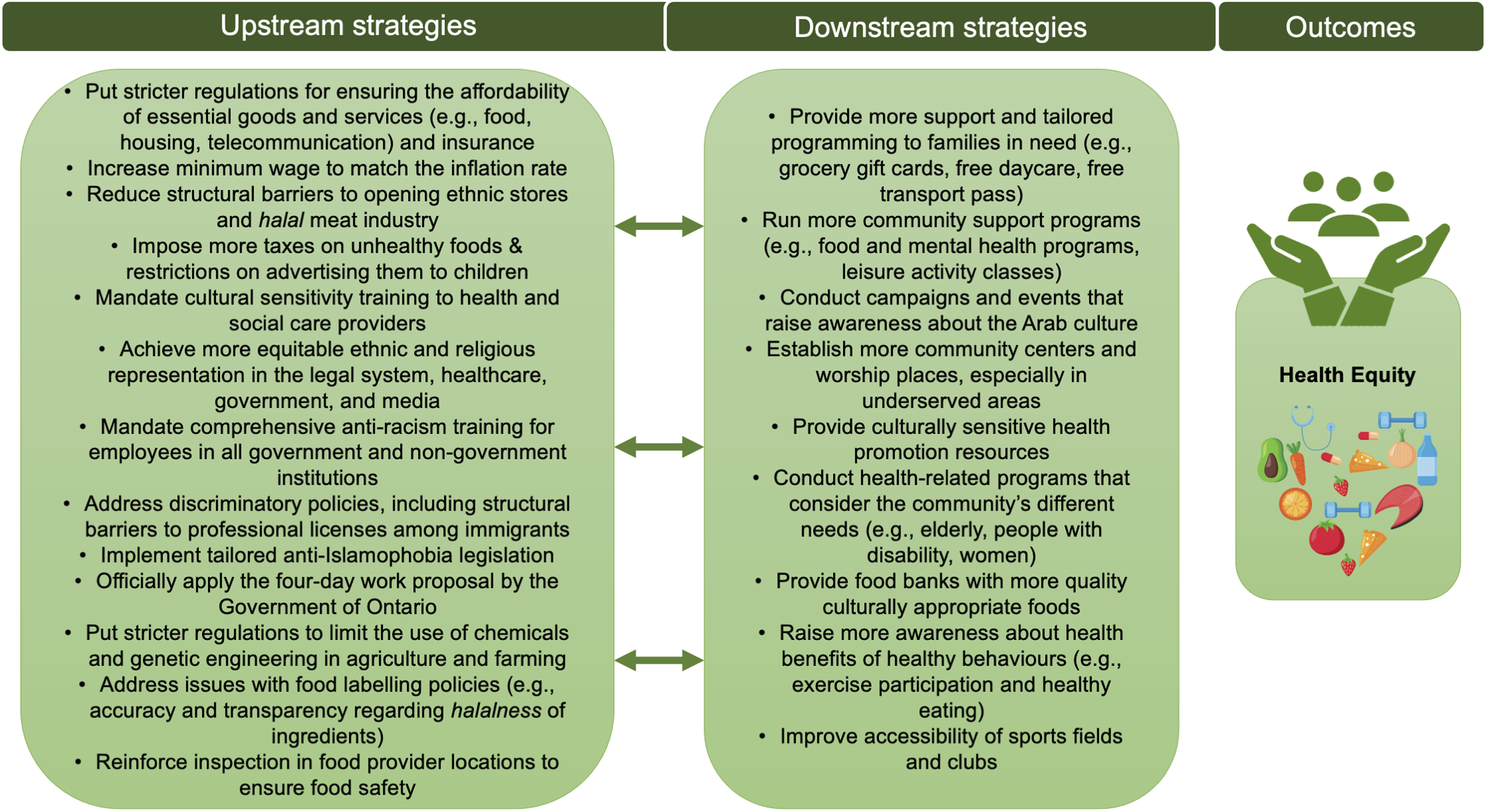
Social Justice
The commitment to social justice was informed by the fact that health, including MH, is in part socially determined, and that social injustice kills people on a grand scale. 48 In response to the AIR community’s needs and priorities according the CAN-HEAL research findings36–38 and in alignment with CBPR goals, different advocacy initiatives were held to raise awareness, induce empowerment, and call for social justice. For example, the project collaboratively worked with the National Council of Canadian Muslims (NCCM) on an Ontario-wide socio-political initiative ‘Action Against Islamophobia Week’ that aimed to mobilize the community to call on the government to take concrete actions against the alarming rise in anti-Muslim hate crimes in Canada. The initiative was implemented in February 2022 and constituted two parts: (1) a virtual workshop with politicians, professionals, activists and youth, and (2) a campaign calling on the government of Ontario to push for the legislation of the ‘Our London Family Act’, which was initially proposed after the murder of a Muslim family whose innocent lives were taken in a hate crime in London, Ontario in June 2021. 49
The project also conducted a series of virtual panels under the theme “Addressing anti-Muslim hate and racism in the professional fields”. The series has covered different fields (e.g., law, healthcare, education), bringing together over 400 community members and stakeholders, including policy makers and practitioners, with the aim of raising awareness and discussing solutions to fight the rise in anti-Muslim hate in professions and workplaces. Various policy briefs have also been produced to propose possible policy options that are based on evidence from the CAN-HEAL project with the aim of advancing social justice.
Application
The CAN-HEAL project’s commitment to application for healthcare improvement was guided by its goal of informing the development of culturally sensitive health and social care systems that honour the unique and complex needs of the AIR community. Cultural sensitivity is a concept that emphasizes the achievement of cultural trust in health and social care settings by creating a space that respects the socio-cultural values of clients and patients, acknowledges power differentials in society and focuses on delivering tailored quality care. 50 The focus on cultural sensitivity can be particularly important in MH care delivery, due to stigma around this topic that is pervasive in many cultures, as well as the systemic racism against marginalized ethnic minorities, which may collectively make many vulnerable people reluctant and terrified of seeking care. 51
The commitment to application facilitated by IKT in this project has been demonstrated through maintaining ongoing mutual dialogue with practitioners and service providers to act on the research findings to improve health and social care practice and promote AIR’s MH and well-being. For example, we collaborated with different clinics, community-based organizations and health and social care providers (e.g., physicians, psychotherapists, occupational therapists, dietitians, and nutritionists) to hold eight virtual panels and workshops, informed by the research findings about MH, physical activity and nutrition, which were collectively attended by over 400 community members. In these events, many health and social care providers discussed and learnt about the research findings on AIR’s MH and behavioural health needs. For example, the term ‘mental health’ was deemed culturally unacceptable and offensive by first-generation AIR participants in this research. 36 Alternative culturally acceptable terms proposed by participants to replace the term “mental health” in health and social care settings included emotional state, feelings, mood, and well-being. Guided by these eye-opening findings, many health and social care providers expressed intention to apply the research results and start using more culturally appropriate communication in their practice. Moreover, many healthcare organizations started providing more culturally sensitive information, programming and resources about MH and behavioural health to AIR.
As part of this project, several culturally sensitive resources were co-designed in collaboration with AIR community partners and members with the aim of enhancing health education and promotion within the AIR community and informing health and social care service improvement (Supplemental File 2). For example, we co-produced a nutrition education cookbook to help provide accessible nutrition information, promote healthy food behaviours, raise awareness of the connection between food and mental well-being, as well as educate service providers about the complex health needs in the Arab community. A storybook has also been co-developed to provide a collection of culturally sensitive stories that foster positive self-talk, and self-care with the aim of promoting the community’s MH and well-being. These resources have been informed by input from community members and participants in the project further to their recommendations in the interviews and Photovoice sessions. AIR community partners and members consistently provided ideas and continuous feedback throughout the production process of these resources to help achieve cultural sensitivity and usability.
Cultural Sensitivity
The CBPR-IKT approach of the CAN-HEAL project followed best practices for cultural sensitivity to enhance the truthfulness of participants’ responses, and promote the study’s rigor and the meaningful application of the findings.52,53 These practices are cultural relevance, contextuality, respect, language appropriateness, flexibility and humility.
Cultural Relevance
The cultural relevance of this project was carefully examined prior to its inception by consulting with partnering Arab community leaders about the research design and topic to ensure that they aligned with the AIR community members’ needs and priorities. Furthermore, three separate scoping reviews on MH, nutrition and physical activity practices among AIR were performed to guide a culturally-relevant research proposal.29,35,54 Frequent consultations were conducted with community leaders and representatives to ensure cultural relevance of the design of CBPR-IKT-based initiatives that were informed by this research findings. The first author is an immigrant from the Middle East which helped frame the entire research design around core Arab cultural values (e.g. collectivism, generosity, honour, respect and religion). 55
Contextuality
Possession of culturally sensitive knowledge of structural conditions that may shape participants’ responses and interpretations of experiences is fundamental to appreciate the context for complex phenomena, ensuring the findings’ reliability and applicability. 52 As an immigrant from the Middle East, the first author’s cultural background helped to effectively achieve contextuality by displaying a comprehensive insider’s knowledge of the wide range of systemic barriers and the political history of the Arab world that places AIR’s MH at risk. Contextuality was further strengthened by engaging in consultations and collaborations with socio-demographically diverse AIR community leaders from different Arab countries throughout the course of the project.
Respect
Throughout this project, the community was treated with utmost respect, aligning with the Arab cultural values. During interviews and photovoice sessions, participants’ perspectives were profoundly respected and empathically listened to and appreciated. As per participants’ needs, photovoice sessions were limited to 2–3 participants and accommodated any gender-related requests. All participants’ religious needs were accommodated, such as giving break for prayers. 55 The cultural and religious needs were also respected throughout the design and delivery of CBPR-IKT-based initiatives (e.g., workshops, panels that shared research results with participants). This helped enhance engagement and loyalty to the project.
Language Appropriateness
Language appropriateness was effectively fulfilled by using culturally appropriate language and words for stigmatized topics (e.g., mental health) throughout the research and the designed CBPR-IKT-based initiatives and resources. Language accommodations were made in this project by making the survey, interviews, and photovoice sessions available in English, Arabic and French. The CBPR-IKT-based information resources (e.g., a nutrition education cookbook) were also produced in Arabic and English to enhance accessibility and best promote the community’s health and well-being.
Flexibility
Flexibility was maintained throughout the research by meeting participants’ and partners’ preferences for communication methods (e.g., phone) and times when addressing their questions about the project. Additionally, flexibility was sustained by accommodating each participant’s time preferences for interview and photovoice sessions. The Zoom platform was preferred by the community for interviews and photovoice sessions as well as information sharing events (e.g., workshops), given its convenience and arrangements were made to provide training to participants per request. This helped enhance participation in the project and its initiatives.
Humility
Humility was sustained throughout the project by practicing openness to learning, recognizing community’s knowledge and expertise and tackling power differentials.56,57 This was achieved by exercising self-reflection, and involving AIR community leaders and representatives in decision making of the research process and the design of CBPR-IKT-based initiatives. This approach helped create trust and empowered the community to speak up about their experiences and complex needs that are often unvoiced due to fear of government authorities.
Successes and Positive Outcomes
The integration of CBPR and IKT approaches produced numerous successes and positive outcomes as reported by community members and participants in the project during the interviews and Photovoice sessions (Figure 1). The multi-level partnership was associated with improved community connectedness and enhanced community action and capacities, through strengthening community members’ ability to cope and resist challenges by leveraging their collective resources. To explain the value of community engagement and partnerships done as part of the CAN-HEAL project, one Muslim participant stated: ‘I’m really happy that…you came to talk about like this project and you are working with different organizations to bring things to, so it’s not just the article, but you’re really working on the ground to bring, ideas, but like at the same time to implement those things. So, this can benefit our Muslim community in Canada and it’s going to benefit everyone to be honest because like I feel good when you feel good… We need to cooperate. We need to help each other. That’s something doesn’t have a price. Thank you… for your time and all the work that you’re doing.’. As part of the Photovoice methodology, one male participant took a photo of shrubs connected in a lake to symbolize the importance of connectedness and unity that could be achieved through projects like the CAN-HEAL project that uses an CBPR-IKT approach for helping the community advocate for their health and social needs and produce culturally sensitive solutions, promoting resilience and well-being (Figure 3). A photo symbolizing the importance of connectedness and unity achieved through CBPR-IKT projects like the CAN-HEAL project.
The use of an integrated CBPR-IKT approach has aided the development of a holistic upstream-downstream-based action plan with AIR community members to reduce health and social inequities by addressing structural and social determinants of health as well as promoting equitable access to culturally sensitive health and social care resources for this population (Figure 2). Participants in the project reported that they found the implemented CBPR-IKT-based initiatives (e.g., health promotion webinars, advocacy campaigns) to be helpful in promoting community health education, raising awareness of complex health and social issues that AIR experience, and facilitating application of findings by providing a platform for meaningful dialogue with stakeholders. One Muslim participant illustrated the importance of the work of the CAN-HEAL project and his engagement in the project’s advocacy initiatives in collaboration with community organizations, stating: ‘Initiatives like this, this is what you’re doing now, you know, this is something that it's really appreciated. Because the more data we have, we gonna know more about the issues that we have and that most of us is, are talking about… The other thing… that to have, like, a, higher organization that’s fighting for our right, so I’ve signed them [open letter to call on the government of Ontario to push for the legislation of the ‘Our London Family Act’, that aims to combat Islamophobia and hatred] and I was really happy with the work.’.
Collectively, the efforts exerted as part of the CAN-HEAL project have helped to cultivate hope in the community and promote resilience and well-being in the community.
Challenges and Enablers
The implementation of this CBPR-IKT-based project has been associated with numerous challenges, which were mitigated in part through certain enablers.
Challenges
Building a multi-level partnership with the community was a tedious process that required intensive planning and efforts to find middle ground to accommodate one another’s needs (e.g., schedules, resource capacity). Limited resources and funding presented a substantial challenge for the execution of the CBPR-IKT approach in this project, including the partnership formation and sustainability, the provision of assistance to community members who needed urgent support (e.g., severe food insecurity) and the implementation of the advocacy and health promotion initiatives.
Leading CBPR-IKT research with a community to whom one belongs was demanding, especially when this community has been historically racialized, and embodies unique cultural norms that need to be genuinely appreciated and accommodated. Performing collaborative research on sensitive topics like MH entails more than active listening to participants’ traumatizing experiences and needs; it requires proactively stepping up to support the community, especially during times of crisis. For example, throughout the course of the project the first author received many calls and messages from newcomer community members who required urgent referral for support during emergency situations (e.g., facing a hate crime, the 7.8-magnitude earthquake that hit Syria in February 2023, which exacerbated the impacts of the war and aggravated the crisis for many Syrian families). The process of community empowerment and conscientization was challenging and required genuine dedication to building trust and cultivating a sense of connectedness, given the historical trauma and marginalization AIR face as reported in this research. 36 Initiating dialogue with health and social care providers to encourage them to apply the research findings in their practice was a demanding process, considering the common human resistance to change and disruption of established practice routines.
Enablers
Exercising open-mindedness and consistently and thoughtfully reminding everyone of the goal the team was working towards (i.e., contributing to the development of equitable systems to improve the health and well-being of AIR and other similar marginalized groups) helped mitigate some of the challenges related to partnership formation and sustainability. To mitigate the challenge of limited resources, outreach to potential community-based businesses was deployed to ask for support (e.g., providing coupons for culturally appropriate foods and meals to families experiencing severe food insecurity) and to collaborate on implementing health promotion initiatives. AIR volunteers assisted with finding referrals to culturally sensitive support services to support community members across the province who faced emergency situations.
The use of Photovoice in this research aided the empowerment process by enabling the community to voice their experiences and needs using symbolic imagery. Incorporating cultural sensitivity principles and co-developing various advocacy-focused initiatives as part of this project, helped the community to reflect and push for policy change to advance social justice. For example, the ‘Action Against Islamophobia Week’ initiative, described earlier in the paper, helped community members reflect on the detrimental impact of hate incidents, and collectively call on the government to push for the legislation of the ‘Our London Family Act’ to combat Islamophobia and hatred after the murder of a Muslim family in London, Ontario in 2021. 49 Practicing humility and persuasive skills aided effective dialogue with health and social care providers regarding applying research findings in their practice. This was further enhanced by collaborating on the development of community-based panels and workshops to discuss the community’s needs and act on the research findings.
Discussion
The CAN-HEAL project used an innovative approach that integrated both CBPR and IKT to address MH needs among AIR in Ontario, Canada. In this paper, we have presented the components and value of an integrated CBPR-IKT approach for addressing complex health issues in marginalized communities. In the CAN-HEAL project, CBPR aided advocacy and lobbying efforts to empower the community and promote social justice, which was associated with many positive outcomes, including the development of community-informed products. Examples of such products include the delivery of policy-driven events that aimed to address the rise in anti-Muslim hate in Canada by proposing concrete solutions (e.g., implementation of anti-Islamophobia training in workplaces). Previous CBPR research also noted similar benefits regarding yielding community-informed products.11,23 Some strengths of the CAN-HEAL study, however, are that it adopted cultural sensitivity best practices, involved the community in directing timely knowledge dissemination process that supported advocacy efforts (e.g., calling on the government of Ontario to push for the legislation of the ‘Our London Family Act’ after the murder of a Muslim family in 2021). These are unique strengths, given that a recent systematic review of the use of CBPR in community health studies found a lack of efficient community engagement in the dissemination process and a need for more cultural sensitivity in CBPR. 58
IKT as an add-on to CBPR facilitated the co-production of applicable knowledge and upstream solutions for health and social care improvement. This aided dialogue with healthcare practitioners and service planners through healthcare improvement-focused panels and workshops to bring the research findings to action, by for example, providing more culturally sensitive resources about MH and behavioural health to AIR. Other emerging IKT studies have also found similar benefits from this technique.59,60 A unique strength of the CAN-HEAL study is that it mindfully addressed a commitment to application-related techniques and initiatives, with a description of how they collectively related to the project outcomes. This is an important contribution, given the gap in current IKT research as reported in a scoping review of 13 IKT studies. 60
In addition to all the above-mentioned positive outcomes, the integration of both CBPR and IKT approaches in the CAN-HEAL project facilitated the co-development of a holistic upstream-downstream-based action plan to tackle health and social inequities among AIR by addressing structural and social determinants of health and promoting equitable access to culturally sensitive health and social care resources and services. According to the upstream and downstream approach, effective health promotion intervention plans should consider and focus on two fundamental strategies: (1) macro-level strategy that is tied to structural determinants of health, and (2) micro-level strategy that focuses on issues related to equitable access to health and social care resources. 41 Ndumbe-Eyoh and Moffatt’s 61 systematic review of intersectoral actions and interventions for health equity found that 88% of studies (n = 17) included in their review focused on a downstream approach, overlooking the root causes of health inequities in society. The use of an integrated CBPR-IKT approach in the CAN-HEAL project helped address this research gap by facilitating the integration of upstream and downstream strategies. This integration provides a promising opportunity for acting on economic, legal and political factors to eliminate structural barriers to equitable health, while maximizing support by enhancing accessibility to culturally sensitive resources and services. 62 All the above-outlined benefits and opportunities from integrating CBPR and IKT approaches underscore how these approaches complement one another as each has unique strengths that are collectively important for addressing complex health needs in marginalized communities.
The implementation of this CBPR-IKT-based project was associated with numerous challenges and enablers. Building a multi-level partnership with the community and knowledge users in this project was a challenging process. Previous CBPR research has identified building partnership with the community as a significant challenge. 63 One example of a successful CBPR study is the “PCBs and the well-being of Mohawk Youth”, that worked with the Mohawk community of Akwesasne and their youth members. 22 Despite the success of the project, the community partnership formation was described as a tedious process that came with many obligations, such as constantly engaging in dialogue, local capacity-building, and advocacy efforts throughout the research timeline.22,23 The CAN-HEAL project mitigated these similar challenges through intensive planning, exercising open mindedness by exploring middle grounds to accommodate everyone’s needs, and consistently and thoughtfully reminding everyone of the goal the team was working towards.
Another major challenge experienced in this project was the limited resources and funding to support the partnerships and the research-informed initiatives. Lack of appropriate funding opportunities for CBPR has also previously been reported as a major barrier to conducting effective collaborative research.64–66 This issue was exacerbated by the COVID-19 pandemic, which precipitated massive inflation, service shutdowns, and job insecurity. 67 Community representatives and volunteers helped to mitigate this challenge by assisting in outreach and coordinating with potential culturally sensitive services to provide support for implementing community-informed initiatives and support for community members who faced emergency situations.
Developing community empowerment required intensive efforts to build trust and cultivate a sense of connectedness with the AIR community that suffers from collective trauma. 36 Similar challenges were described in Schell and colleagues’ CBPR study with Indigenous Mohawk Youth who live with a history of ongoing colonial oppression.22,23 The use of Photovoice method in this project allowed AIR community members to voice their complex needs through photographic evidence. Following cultural sensitivity principles and co-producing advocacy-focused initiatives also aided the empowerment process by helping to cultivate trust and bring the community together to advocate for systemic change and advance social justice.
Conducting CBPR-IKT research on MH with one’s own community appeared to be taxing. Mosavel et al 68 also reported that conducting community-based research on sensitive topics with the community to which one belongs can be challenging. Previous research also shows that researchers doing health research with marginalized communities may be emotionally impacted as a result of consistent exposure to community members’ traumatic experiences.69,70 A scoping review of 230 Canadian dissertations on sensitive topics (e.g., MH and trauma) found that only 5% of included dissertations involved a protocol or systematic procedure that addresses and mitigates psychological risk to the researcher, highlighting an urgent need for clear guidelines and protective measures by academic institutions to ensure the psychological safety and well-being of researchers. 71 Based on lessons from this CBPR-IKT-based project, recommendations for governmental agencies and institutions are presented below to advance collaborative CBPR-IKT research and thereby promote the well-being and sustainability of communities.
Conclusion and Recommendations
This project employed an innovative methodological approach that integrated CBPR and IKT to thoroughly address MH needs among AIR by tackling structural and social determinants of health and co-producing applicable knowledge to inform culturally sensitive health and social care. Integral to this approach was the establishment of an efficient multi-level partnership with community members and knowledge users, adherence to principles of cultural sensitivity, and a commitment to social justice and application. The use of an integrated CBPR-IKT approach in this project has been associated with numerous positive outcomes, including the co-development of a holistic upstream-downstream-based health promotion action plan. Though there were numerous challenges, some of these were mitigated by employing various enablers, such as assistance from community leaders. The CBPR-IKT approach presented in this paper serves as a model for researchers conducting health research with marginalized communities as it allows for intensive, culturally sensitive exploration of complex health issues and facilitates taking actions through advocacy, empowerment, and application to work towards health equity.
This project provided many lessons on areas for improvements to advance CBPR-IKT research and thereby promote the sustainability and well-being of communities by reducing health and social inequities. Based on lessons from this project, some recommendations are made for implementation by governmental agencies and institutions. One of the prime recommendations is to invest in providing more funding opportunities to support the conduct of meaningful CBPR-IKT research. This can be performed by allocating funds to develop joint internship programs that encourage community members and youth to engage in this type of research. This would not only strengthen community involvement in directing research and support researchers (so they can direct their efforts towards the implementation of the research), but would also provide an excellent opportunity for community members and youth to develop valuable knowledge and level up their skills through paid programs. Government funding agencies should also provide more financial support and resources to community organizations to increase their engagement in this type of research. For partnerships to be equitable, funds should be allotted to both academic researchers and community organizations to provide stipends for staff engagement in research. Moreover, allocating more funding for CBPR-IKT research and its related activities (e.g., designing advocacy and health promotion initiatives) is a crucial step towards advancing this important research that has the potential to directly promote the health and well-being of communities and strengthen community action. Finally, it is recommended that academic institutions develop clear policies and procedures to create psychologically and physically safe environments for researchers doing sensitive research, including CBPR-IKT research on MH and trauma, and minimize risk of harm. A concrete example of such policies is proposed by Orr et al 71 and includes the implementation of a trauma-and- violence-informed care approach to (1) educate researchers about potential psychological risk of conducting sensitive research and (2) replace punitive policies that perpetuate psychological distress with approaches and protective measures that support researchers’ autonomy and well-being. A ‘trauma-informed’ approach pertains to the delivery of culturally sensitive training and support measures to researchers that consider possible experiences of trauma. 72 This can be particularly important for researchers who directly work with a historically racialized and collectivistic community to which they belong.
Supplemental Material
Supplemental Material - An Integrated Methodological Approach to Address Immigrants’ Complex Health Issues: Lessons From the CAN-HEAL Study
Supplemental Material for An Integrated Methodological Approach to Address Immigrants’ Complex Health Issues: Lessons From the CAN-HEAL Study by Sarah Elshahat, Tina Moffat, Zena Shamli Oghli, Yasmine Belahlou, Yumnah Jafri, Salima Zabian, and Sarah AH Curtay in Community Health Equity Research & Policy.
Footnotes
Acknowledgements
Deep thanks to the collaborators, partners, and participants who shared their valuable insights. Sincere thanks to the CAN-HEAL representatives, committee leads and team members. The icons in the figures are sourced from Canva.
Author Contributions
S.E. conceptualized the project and methodology, led the project administration, curated, analyzed, and visualized the data, as well as wrote the original draft. T.M., contributed to critical project conceptualization and methodology, as well as led critical revision and editing. Z.S.O., Y.B., Y.J., S.Z., S.A.H.C. contributed to conceptualization, interpretation, visualization, as well as review/editing.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This paper draws on research that was in part supported by the Social Sciences and Humanities Research Council.
Ethics Approval
Ethics clearance for the study was received from McMaster Research Ethics Board (#5515). An informed voluntary consent was obtained from participants in the study.
Data Availability Statement
Data cannot be shared due to confidentiality/privacy reasons.
Supplemental Material
Supplemental material for this article is available online.
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.