
Abstract
Background
Community-based participatory research coproduces knowledge by emphasizing bidirectional exchanges between participants, communities, and researchers.
Purpose, Research Design, and Study Sample
We highlight three studies in historically marginalized communities on separate continents (Richmond, CA, USA; Rio de Janeiro, Brazil; Marseille industrial zone, France) to exemplify how community-based participatory research improves research, offers tangible community benefits, and values residents more than traditional research methods.
Data Analysis
We provide insights into the process of conducting meaningful community-based participatory epidemiologic research.
Results
In each of these communities, community-based participatory research led to high-quality research that helped inform context-appropriate policies and programs to improve health and advance health equity in these communities.
Conclusions
We recommend that researchers consistently engage with community members during all phases of research so that they can engage more participants, more deeply in the research process, build local capacity, improve data collection and data quality, as well as increase our understanding of research findings to inform future applied research and practice.
Background
Community-Based Participatory Research and Epidemiology
Community-based participatory research (CBPR) is a research framework in which researchers and community members collaborate to address a topic of mutual interest, 1 with the goal of redressing historical power imbalances between researchers and community members. 2 There is a long and well-documented history of CBPR in public health.1,3 When done well, CBPR engenders greater rigor, relevance, and reach than traditional research methods. 4
This article focuses specifically on intersections between CBPR and epidemiology. Epidemiology seeks to describe and analyze health patterns in populations, 5 and one of the primary tenets of epidemiology is to apply research findings to subsequently improve health outcomes in populations under study. 6 One of the best ways to fulfill this mission is to engage the community in the research process. There is also a rich history of popular epidemiology, in which laypeople employ epidemiologic methods themselves to study health issues of local interest. 7 Additionally, increasing numbers of researchers and practitioners seek to use epidemiological analyses to understand and address health equity concerns, 8 another goal of community-based public health research.9–11 There is a growing movement to encourage epidemiologists to center their work in cultural competency and humility as well as equity-oriented approaches.12–14
While our research builds upon literature focused on CBPR and epidemiology, 15 we recognize that CBPR also has a long history in sociology (where it is often called public sociology),16,17 anthropology, 18 community psychology, 19 and other social and health sciences. 20 Additionally, the term “citizen science” has been used in a number of scientific disciplines, including public health. 21
Case Examples
How Our Three Cases Aligned With Best Practices for Participatory Research Identified by Davis & Ramírez-Andreottai. 23
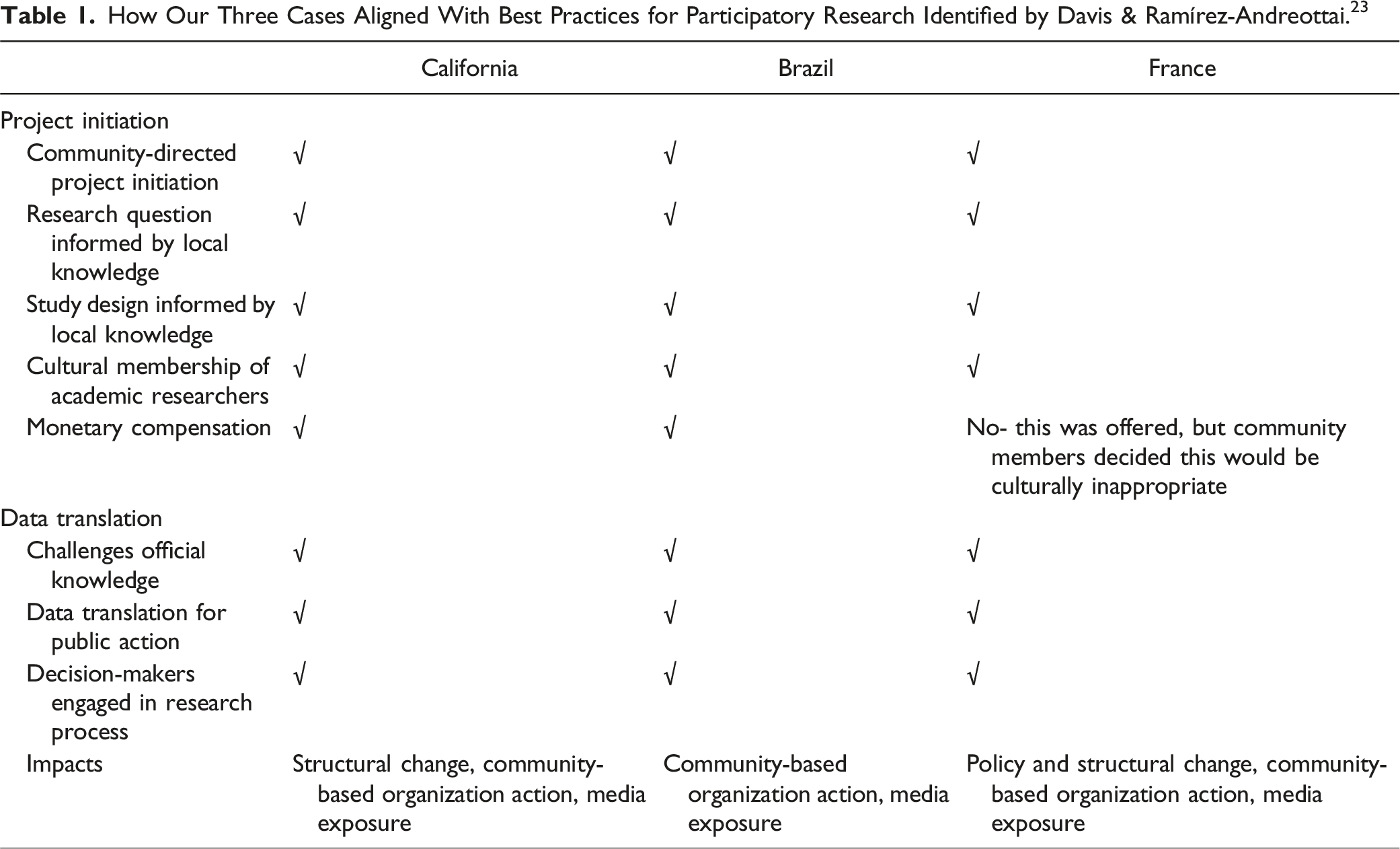
In Richmond, California, USA, the research focus was documenting environmental health and environmental justice issues in a historically marginalized urban community that borders major stationary and mobile polluters. 24 Epidemiology, environmental health science, and social science researchers partnered with two community-based organizations that are focused on environmental justice to conduct a cross-sectional study. 25 This study of approximately 200 residents involved random sampling in some neighborhoods and snowball sampling in others. 24 In the time since the research was conducted, the research findings have informed community organizing and advocacy efforts to reduce exposure to environmental pollution in the region. 25
In Niterói, a city in the greater metropolitan area of Rio de Janeiro, Brazil, the research focus was to evaluate the burden of diabetes mellitus in an urban community. Epidemiologists and lab scientists partnered with the local primary healthcare facility and residents to conduct a prospective cohort study. This study used a census sample of roughly 600 diabetics and non-diabetic community-controls derived from the primary care patient list. 26 This research informed the future activities of a local health clinic to support its patients.
In the towns of Fos-sur-Mer and Port-Saint-Louis-du-Rhône, France, the research focused on documenting environmental health issues in the industrial zone of the Marseille metropolitan area. While a number of other studies had been done in this region, they had not adequately addressed residents’ concerns. 27 A team of Franco-American epidemiologists, sociologists, and anthropologists partnered with the leaders of local environmental associations, and health providers to develop and implement a cross-sectional epidemiology study. 28 This study included a random sample of over 800 residents and a supplemental volunteer sample of 75 in the cross-sectional study,29,30 and qualitative data collection in focus groups discussing the study findings. 31 This study received extensive media coverage 32 and informed local, regional, and national advocacy efforts to improve health in the region. For example, midway through the study (while data collection was underway), the main government health clinic that served the two communities closed, due to financial constraints. After multiple community protests and, perhaps, due in part to the increase in community awareness of relevant health issues from our study, the clinic re-opened. This also spawned a follow-up study expanding to collect data in a third town in the region that was further from industrial activity to be able to do comparative analyses in response to some of the new research questions that emerged. 33
In each of these contexts, the academic researchers were invited in to these communities as research partners, which was especially important given that some of the academic researchers did not otherwise have local ties to the communities who were participating in the research. (For example, in the Brazil and France cases, some of the academic researchers lived an international plane flight away.) In this context, academic researchers’ efforts to spend dedicated time (multi-week to multi-month trips) talking with and learning from community members in their local language (e.g., Portuguese, French) helped overcome what would have otherwise been a meaningful difficulty.
Findings
In this section, we describe some of the ways in which CBPR can support several key aspects of epidemiologic research. To help guide this section, see Figure 1 for an illustration of a CBPR approach applied to the epidemiology process, with more specific examples reflective of the California and France studies provided. A community-based participatory approach to epidemiology, as illustrated by the France and California studies.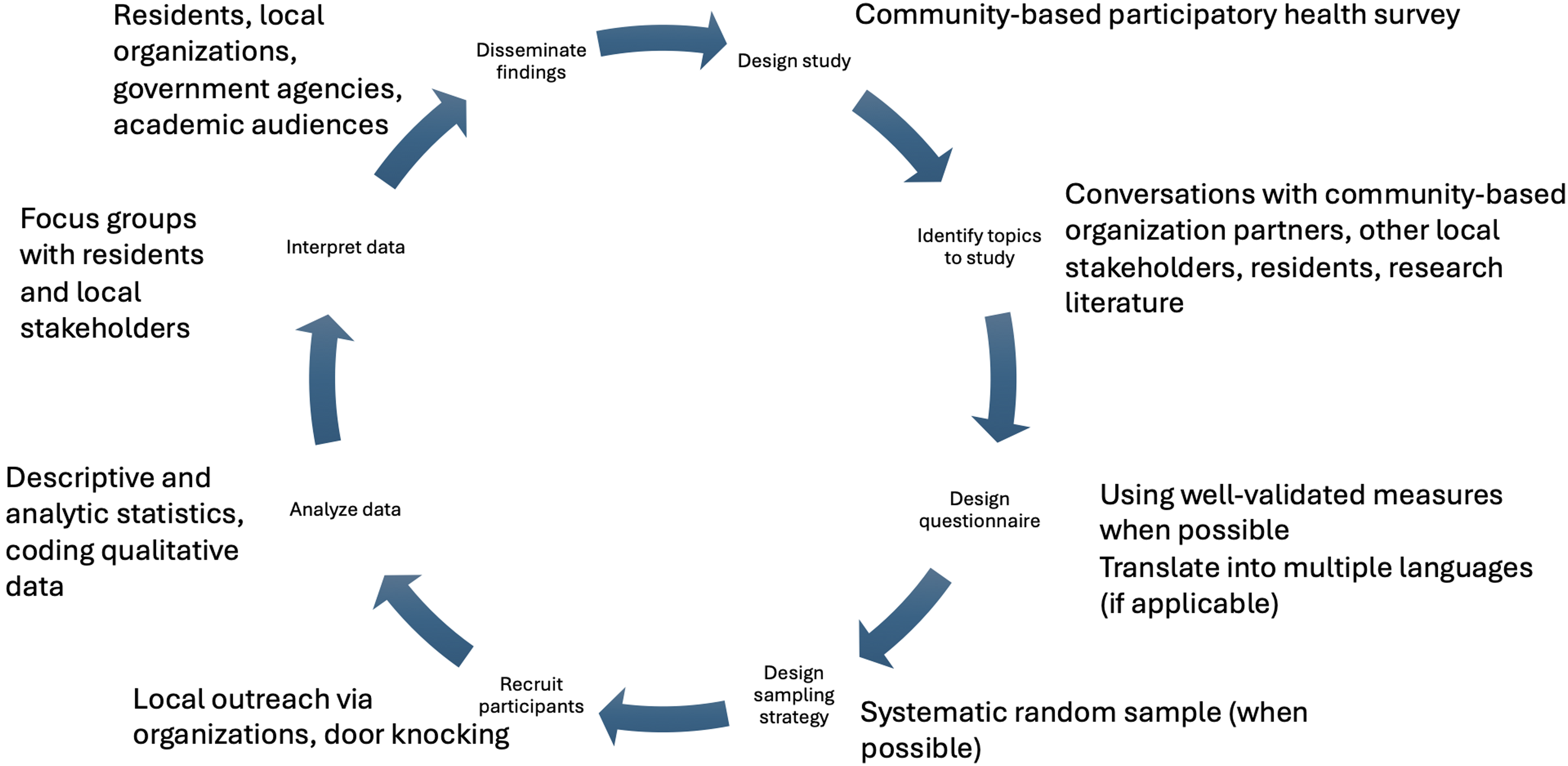
Study Design
These studies were inspired, and, in the California study, led, by community members expressing concerns about health inequalities they observed. It followed that a commitment to learning from and with community members who experienced these health issues day to day would enhance the quality and durability of the epidemiologic research, and that a CBPR approach made the most sense.
As part of the agreed-upon approach of doing community-based participatory epidemiology, researchers and community members worked bi-directionally to build local capacity. For example, in Brazil, a Brazilian nurse visited Robert Snyder’s home academic institution to present results at an international global health conference, and researchers from Robert Snyder’s home academic institution also hosted workshops with local clinic and health department employees while in Brazil to enhance their epidemiologic skillset. Primary health care in Brazil is delivered at primary care centers by community health workers (CHW) who are residents of the same communities where they work. The CHW model of care is highly aligned with CBPR: it is a community-based model for care that emphasizes patient contact and ‘boots on the ground’ by health personnel in their own communities. Researchers worked closely and bi-directionally with CHW throughout the entire study. In California, researchers hired and trained local residents in environmental health justice as well as research ethics so that they could then deploy surveys alongside research staff. A similar approach was taken in Brazil with the CHW. Working with these known and trusted actors increases the likelihood that residents will participate.
Identifying Topics to Study
We focused on identifying topics to study that were of interest to community members and would collect data on the issues of greatest concern to them. We also often supplemented this with topics that could be potential areas of concern, even if they had not yet risen to the top anecdotally. For example, based on other community-based environmental health studies done elsewhere, the California study decided to include measures of noise pollution and acute symptoms (like eye irritation) that could be linked to environmental pollution. For the France study, many residents in the fenceline communities also worked at the local industrial facilities, so we collected detailed occupational health data; in comparison, few residents in the California study worked at the local industrial facilities, so we collected less occupational health data.
Additionally, we also incorporated questions that would be beneficial to either only academic or only community partners. For example, in California, we included questions relevant to our principal community-based partner organization that would help inform their work (like asking study participants if they were familiar with the organization). In Brazil, researchers added questions to understand potential effect measure modifiers (also known as moderators or variables for conducting stratified analyses) that researchers identified during their community engagement activities, and additional questions when researchers returned for the second round of sampling. Due to lessons learned from initial sampling and analysis with community members, researchers were able to incorporate additional questions related to food security and nutrition. In France, we included questions about tobacco smoking habits, which were not specifically mentioned by residents, but were essential to estimate stratified disease prevalence and develop multivariable models while controlling for smoking, 34 which would be necessary for review by state and other epidemiologists as smoking is causally related to many health problems. 35
Questionnaire design
When possible, we used questions that had been validated elsewhere and that had relevant comparison data. For example, for the California study, we used questions that had also been used in the California Health Interview Survey, so that we could compare to county-level and state-level data on a given health outcome. Additionally, by using the same question text used by government agencies, we increased government stakeholders’ trust in our findings. Similarly, for the France study, we used questions adapted from French and European Union surveys when possible.
Researcher-community collaborations also assisted with language validation-for local colloquialisms, cultural context, and works in translation. In California, the survey was prepared and conducted in both English and Spanish; in addition to having bilingual research staff, local residents who were native Spanish speakers (both monolingual and bilingual) reviewed all translations to ensure accuracy. In Brazil, residents ensured that all vocabulary was consistent with local dialect after initial validation of survey instruments in Portuguese by local university and community partners. In France, both native and non-native bilingual French-English speakers reviewed the survey to ensure accuracy and also discuss contested translations of words like “neighborhood” (a term rarely used in France). The final survey only included questions on which there was complete agreement.
Sampling Strategy
In California and France, we conducted systematic random sampling to reach residents when possible (in California, we were only able to do this in lower-violence neighborhoods in which people were willing to open their doors to strangers). A systematic random sampling approach (which consisted of randomly-drawn loops for surveyors to walk, plus an approach to knock on every nth door) was more feasible to implement than a simple random sampling approach, and still conferred epidemiologic rigor.
In both Brazil and California, community partnerships helped overcome both the researchers’ and the participants’ concerns related to violence during data collection. In the most violent neighborhoods in Richmond, CA, stakeholders identified a safe and neutral location - a community center - where residents felt safe participating, that was also safe for surveyors. Whereas systematic random sampling was employed in other neighborhoods, at the community center, we used snowball sampling to recruit participants. In Brazil, residents identified and supported data collectors to protect the researchers from confrontations between police and drug traffickers, incorporating pre-existing internal codes and means of communication to convey the level of risk for field work at the time. Working with community residents also enhanced informal communication within their person networks to enhance researcher, participant, and public safety.
Participant Recruitment Approaches
Community engagement can increase study participation in several ways that benefit epidemiologists by improving the accuracy of the sampling frame (or at least our understanding of the accuracy of sampling frames). It does this by enhancing trust and facilitating access to hard-to-reach and vulnerable groups. In Brazil, we built trust through maintaining a physical presence at the local clinic and seeking out and engaging community leaders through formal presentations, seminars, and informational sessions while also employing flexible interviews and dynamic sampling at the health post, via phone, or at a resident’s home. In California, we conducted most surveys in the evenings and on weekends, after researchers queried residents and they indicated that they were more likely to be home and available at these times. In France, we offered flexible and convenient scheduling for interviews with sampled residents, including an opportunity to be surveyed by phone rather than in person if they indicated this preference. Residents’ extensive feedback in France also prompted shifts in survey methodology to augment collections using an online survey that residents could complete if they were not randomly sampled to participate in the in-person collections.
In each of these settings, researchers held extensive community meetings in an effort to educate residents about the research process and scientific methods, as well as to obtain residents’ input regarding best sampling practices. In California, we sent letters to everyone on the community-based organizations’ mailing lists that publicized the study and invited their participation. In France, we held both academically-oriented and community-oriented workshops to recruit participants, augmenting a separate sample of volunteers in addition to the primary random sample so that everyone who wanted to participate would be able to do so. These adaptions to incorporate CBPR could require shifts in data analysis as well. In this case, inclusion of two samples required data to be analyzed separately to evaluate for systematic differences between the random and volunteer samples. 30
Data Analysis and Interpretation
While the epidemiologic analyses using statistical software were often done by academic researchers only, we engaged community members in the interpretation of those findings and in brainstorming additional ideas for analyses. Researchers also hosted open fora and maintained consistent communication channels between researchers and community members (not only research participants but also other non-affiliated local residents) throughout the research process. It is essential that these efforts are not put off until the conclusion of the research project. In both California and France, we held focus groups to review results from preliminary analyses and also to identify additional hypotheses to test in follow-up analyses. In the French focus groups, we noticed that participants triangulated their lived experiences and other types of knowledge to reach broader conclusions about health in their community and what could help improve their health. 31 Then, in follow-up work, an ecosystem of participatory studies emerged tackling different subquestions related to environmental health equity in the region, which residents and researchers were able to co-interpret together. 36 In Brazil, we organized presentations describing our work in progress and had similar follow-up conversations with community members, also making explicit efforts to present results to administrators in the city’s family health program. These presentations were conducted by local health professionals with the support of academic researchers from Brazil and the USA.
Disseminating Findings
Prior to and during the course of these projects, researchers made deliberate efforts to discuss authorship and ownership of findings and other project products. In California, our partners from the community-based organization were co-authors on reports and peer-reviewed journal articles. Community residents that helped to conduct surveys were also credited in the acknowledgments of reports and papers. Researchers in Brazil made efforts to publish results in Portuguese-language journals whose target audience included medical practitioners active in these communities. 26 On the other hand, in France, community members requested to not be co-authors of manuscripts, indicating their continuing interests in maintaining the boundaries of the independent academic process.
We also sought to develop and utilize creative techniques to disseminate results and other project information. In Brazil, our efforts at community engagement caused significant delays in sampling because it increased the number of stakeholders. However, our efforts in this context also led to co-creating a video that was subsequently used by stakeholders to improve diabetes care in the community, facilitating uptake of results after completion (available online with and without English subtitles at https://www.youtube.com/watch?v=p80BNySqqxk). This also helped to identify stakeholders who were interested in participating in data analysis, interpretation, and dissemination of results within the community. In France, we developed a website (available online at https://fosepseal.hypotheses.org/) and also disseminated information through local classrooms and extensively engaged with journalists. These parallel outreach efforts with the media led to multiple news articles describing our research findings; in comparison, previous studies in the region, which did not use a CBPR approach, had no media coverage. 32 The extensive dissemination efforts in the France EPSEAL project led to meaningful societal impact both for local advocacy efforts and for policy and regulatory changes, which have been detailed elsewhere. 37
Discussion
Researchers’ efforts to demonstrate their commitment to the communities they work with as well as their focus on open, transparent, and accessible communication channels resulted in increased community engagement throughout the course of several research projects in Richmond, California, USA, the Rio de Janeiro metropolitan area, Brazil, and the industrial zone of Marseille, France. While we cannot compare these studies to a counterfactual version of research that was not community-based and participatory, we posit that our high levels of community engagement in the research process identified new research topics for exploration, supported developing more nuanced community-specific hypotheses to test, and supported using findings to recommend actions that improve health in these communities. By coupling local residents’ knowledge with researchers’ subject-area expertise, both groups leverage their relative strengths. Working together in this way also contributes to developing trust and respect, which we observed in each of our case studies, and which others have also documented.38,39 Democratizing knowledge has other downstream effects that may manifest later, including knowledge justice, 40 long-term health benefits, increased empowerment, 41 and/or strengthened community organizing efforts. 25
Epidemiologic research quality improved due to our community engagement. This led to an increase in response rates and a subsequent reduction in bias. This was in large part due to our enhanced access to marginalized populations within communities of interest. Other CBPR initiatives have also documented elevated participation rates. 42 Importantly, during non-participatory research surveys, these populations would be excluded from sampling. Researchers may not even be aware of the biases that result from these non-community-based methods. Via our efforts to engage residents in the analysis and interpretation of preliminary research findings, we were also able to achieve more nuanced insights into health issues as well as enhancing the implications for future research and practice. This bolsters similar conclusions reached by others that employ community-based methods. 43 To add to this evidence base, future researchers could consider replicating non-community-based participatory studies using a community-based participatory research approach, and documenting the extent to which measures of association calculated varied, to quantify any potential bias reduction.
There were also tangible benefits to the communities involved that also aligned with benefits reported by researchers in other communities,44–46 including capacity-building and health literacy. As others have reported,4,47 these partnerships lead to more rigorous research that more accurately reflects the local context of the research question. These more accurate results can then be used by both residents and researchers for specific advocacy and policy purposes. In each of these cases, partnerships discussed how putting trust in rigorous research processes meant trusting the findings, regardless of whether or not the findings aligned with initial community hypotheses; these conversations can sometimes be contentious. While in all of our cases, findings resonated with overarching community hypotheses, this may not always be the case. This may be especially likely to happen for rarer diseases, like cancer, 48 for which there may be limited statistical power to detect statistically significant differences.
Despite evidence highlighting how community engagement improves results and health outcomes, its utilization is far from universal. This may be in part due to the fact that conducting community-engaged research is time- and resource-intensive, and requires substantial relational work. For example, in researcher-driven studies, each of the steps of the research process outlined in Figure 1 would still occur, but would not involve relational work with community members and would instead go forward based on only the researchers’ ideas. Additionally, building these partnerships can take more time than is normally allotted in traditional grant cycles. In all three of the case studies described here, at least one member of the research team had been previously involved in a research initiative in these communities – facilitating further inroads. External funders rarely adequately compensate the time needed for this relational work; in each of our cases, academic researchers were effectively volunteering their time for at least some of the work on the project. It could also be because this type of work is onerous, requiring intense reflection about research ethics, 49 traditional power dynamics,50,51 and cultural differences. 52 We also acknowledge that community-based participatory research approaches progress beyond traditional epidemiology but there is still meaningful room for further progress. For example, Indigenous data sovereignty moves beyond community-based participatory research to center Indigenous communities and nations as leading research efforts.53,54
Efforts must also be made to measure the extent to which community-based participatory research projects improve health outcomes. This could be achieved by explicitly quantifying the net improvements in health outcomes over time in communities that implement community-based participatory research methods.
Building upon the work of others in the field of CBPR,1,23,55 this paper described how three case examples successfully integrated community members into the research process. Additionally, we described similarities in the case examples’ research approaches that were informed by their CBPR principles and also divergences that were initiated by our community-specific insight. We encourage researchers who are participating in CBPR to write about this process, including their accomplishments and pitfalls, and engage in cross-learning across multiple research projects. In journals that do not explicitly request this information, or allow space for description of these efforts, researchers must make an effort to do so. We argue that there will be further insight across multiple disciplines. While this paper focused on community-based participatory epidemiologic research, there would also be important insights from community-based participatory research in other disciplines. We encourage future epidemiologic research to incorporate principles of CBPR as thoroughly as possible to lead to higher quality and more useful research.
Global inequality continues to increase. 56 We posit that CBPR can help work across differences and conduct studies to rigorously understand and address inequality and some of its root causes. CBPR can also democratize the production of knowledge by encouraging co-produced knowledge, which can promote knowledge justice. It is particularly important to acknowledge the public service mandate of research, given the extent to which research in the United States is publicly funded. When done well and with sustained investment, CBPR offers tangible opportunities for community residents to engage in opportunities that would otherwise be unavailable, and can lead to more informed action.
Footnotes
Acknowledgments
Cohen was supported in part by the Agence Nationale de Sécurité Sanitaire de l’Alimentation, de l’Environnement, et du Travail (ANSES) (Cancer ITMO AVIESAN 2014/1/023 and 2017/1/035). Snyder was supported by the US Fulbright Student program, NIH Research Training Grant # R25 TW009338 funded by the Fogarty International Center and the Office of AIDS Research at the National Institutes of Health, the U.C. Berkeley Center for Emerging and Neglected Diseases, and Fundação de Amparo à Pesquisa do Estado do Rio de Janeiro – FAPERJ. Lucia Calderón and Amy Rich provided useful research assistance.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the UC Berkeley Center for Emerging and Neglected Diseases, US Fulbright Student program; Fogarty International Center; R25TW009338, Fundacao de Amparo à Pesquisa do Estado do Rio de Janeiro, Agence Nationale de Securite Sanitaire de l'Alimentation, de l'Environnement et du Travail; Cancer ITMO AVIESAN 2014/1/023, Agence Nationale de Securite Sanitaire de l'Alimentation, de l'Environnement et du Travail; Cancer ITMO AVIESAN 2017/1/035.
Author Biographies
At the time of the research,