
Abstract
Background
Equity-deserving groups face well-known health disparities that are exacerbated by rural residence. Health technologies have shown promise in reducing disparities among these groups, but there has been no comprehensive evidence synthesis of outcomes.
Purpose
The purpose of this systematic review was to examine the patient, healthcare, and economic outcomes of health technology applications with rural living equity-deserving groups.
Research Design
The databases searched included Medline and Embase. Articles were assessed for bias using the McGill mixed methods appraisal tool.
Analysis
Data were synthesized narratively using a convergent integrated approach for qualitative and quantitative findings.
Results
This evidence synthesis includes papers (n = 21) that reported on health technologies targeting rural equity-deserving groups. Overall, patient outcomes - knowledge, self-efficacy, weight loss, and clinical indicators - improved. Healthcare access improved with greater convenience, flexibility, time and travel savings, though travel was still occasionally necessary. All studies reported satisfaction with health technologies. Technology challenges reported related to connectivity and infrastructure issues influencing appointment quality and modality options. While some studies reported additional costs, overall, studies indicated cost savings for patients.
Conclusions
There is a paucity of research on health technologies targeting rural equity-deserving groups, and the available research has primarily focused on women. While current evidence was primarily of high quality, research is needed inclusive of equity-deserving groups and interventions co-designed with users that integrate culturally sensitive approaches. Review registered with Prospero ID = CRD42021285994.
Introduction
Individuals living in rural areas face significant healthcare access barriers,1–3 including provider shortages, geographical hurdles, high-speed internet unavailability, and service scarcity.3,4 Overall, evidence suggests a widening gap in mortality and morbidity between rural and urban populations. 5 Studies point to rural populations being older, unhealthier, less affluent, and scoring lower on social determinants of health than urban populations. 6 Superimposed on rural location are socio-demographic factors that have been shown to impact health and health inequalities and are heterogeneous between and within rural communities.7,8 One USA study hypothesized that rural dwellers would outlive their urban counterparts if social demographics and healthcare access were similar. 9
Building on the literature on urban-rural health and healthcare disparities, there is an emerging body of knowledge focusing specifically on the needs and challenges of equity-deserving groups living in rural areas. Equity-deserving groups are comprised broadly of Black, Indigenous, Persons of Colour (BIPOC); Persons with Disabilities; Women; and Lesbian, Gay, Bi-Sexual, Trans, Queer, and 2-Spirit (LGBTQ2S*) individuals. 10 These population groups face additional barriers in accessing resources due to systemic disadvantage and discrimination and are acutely affected by inequitable access to healthcare. 11 Evidence shows existing and widening health disparities between equity-deserving and non-equity-deserving groups.12–14 One USA-based study showed that rural areas with predominantly black and indigenous populations had the highest premature death rates. 15 Studies have demonstrated disparities among rural women compared to urban women across a wide range of healthcare services, including preventive care, 16 cardiac care, 17 and cancer care. 18 Similarly, the disparities in access, health outcomes, and experiences of sexual and gender minorities in rural areas are well documented. 19
Digital technologies emerging in the new millennia have shown promise in addressing inequitable healthcare access in rural communities. 20 Digital technologies include software or hardware that utilize computers, smartphones, tablets, and wearables to deliver care, facilitate communication, and monitor health status. The availability of varied online technologies for providing education and healthcare (e.g., appointments, lab results review) shows enormous potential and benefit for rural health delivery and access. 3 However, research has shown barriers to digitalization in rural areas, including socio-cultural (e.g., distrust, fear), technical (e.g., lack of connectivity), economic (e.g., costs), and regulatory-institutional (e.g., data management). 21
There is also increasing demand from equity-deserving groups for digital solutions to address healthcare access barriers. Mounting evidence suggests that equity-deserving groups find technology-enabled healthcare acceptable for a variety of services, such as palliative care, 22 chronic disease management, 23 health promotion, 24 and mental health. 25 Despite preliminary evidence supporting health technologies for equity-deserving groups in rural communities, no comprehensive synthesis of health technologies targeting rural equity-deserving groups has been conducted. Equitable care and inclusive technologies for equity-deserving groups are a priority for healthcare systems. 26 A systematic review of the current state and progress of evidence in this domain to date could be a valuable addition to this growing body of knowledge and have meaningful implications for practitioners and policymakers.
The purpose of this systematic review was to examine the patient, healthcare, and economic outcomes of health technology applications used with rural living equity-deserving groups. Specific questions included: (1) Do health technologies serving equity-deserving populations in rural communities improve outcomes (i.e., patient-reported, clinical indicators, healthcare-related, cost-related) and; (2) What are the economic implications of the use of health technologies (i.e., cost of telehealth interventions) for equity-deserving rural populations.
Methods
This study used a mixed studies systematic review to maximize the scope of evidence by integrating mixed studies. 27 It is important to distinguish mixed studies reviews from mixed methods reviews, as the former involves the integration of studies with diverse designs (Quantitative, Qualitative, Mixed Methods), while the latter specifically encompasses reviews that include only studies employing mixed methods, integrating both quantitative and qualitative approaches. 27 In health research, mixed studies reviews prove particularly valuable given the intricate and context-specific nature of the phenomena, enabling a comprehensive understanding of the multifaceted challenges and opportunities inherent in complex contexts such as health technology applications used with rural living equity-deserving groups. 27
Search Strategy
The search strategy was developed in conjunction with a health sciences librarian (RJ) who grouped keywords, subject headings, and MeSH terms into the main subject areas: “rural,” “equity-deserving groups,” and “health technology.” Before finalization, the search strategy was reviewed by all team members for appropriateness (See Appendix A). The databases searched included Medline and Embase. This study was conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines. 28 Database searches were limited to publications from the previous decade (2011) to October 11, 2023, to capture relevant technology and emerging innovations. Records generated by the search were managed using Covidence systematic review software (Veritas Health Innovation, Melbourne, Australia) for organization, removal of duplicates, screening, full-text review, and quality assessment.
Inclusion/Exclusion Criteria
Included studies met the following criteria: (1) a health technology intervention for patients (inclusive of virtual visits, wearables, apps, and websites); (2) rural populations or settings; (3) one or more equity-deserving groups (i.e., Black, Indigenous, and Persons of Colour (BIPOC), Persons with Disabilities, Women, or Lesbian, Gay, Bi-Sexual, Trans, Queer and 2-Spirit (LGBTQ2S*)); and (4) Geographical location of Canada, USA, Australia, or New Zealand. Studies were limited to English-speaking countries with similar geographical rurality challenges (topographically, bandwidth infrastructure). Studies were excluded if they were not original research (e.g., editorials), protocols, pilot or feasibility studies, review articles, or focused on children or youth under 19 years of age.
Article Selection
Following standard review guidelines, dual reviewer (LB & MF) title and abstract screening was completed on a 20% sample of records from the final citation library (with duplicates removed) against the stated inclusion and exclusion criteria.
29
Following the dual screening, conflicts were resolved, inclusiveness criteria were clarified, and modifications were made as appropriate with three team members (LB, MF, & KLR). Following screening calibration, the remaining title and abstract screening were conducted independently by two team members (LB & MF), consistent with systematic review methodologies.
29
Conflicts were assessed and resolved using consensus by two team members (LB & MF). The full-text review process was piloted with 10 articles to calibrate the process before the remaining articles were reviewed independently by two team members (LB & MF),
29
and any disagreements were resolved through discussion with a third team member (KLR). The final search results are presented in a PRISMA diagram (Figure 1). Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ 2021;372:n71. doi: 10.1136/bmj.n71.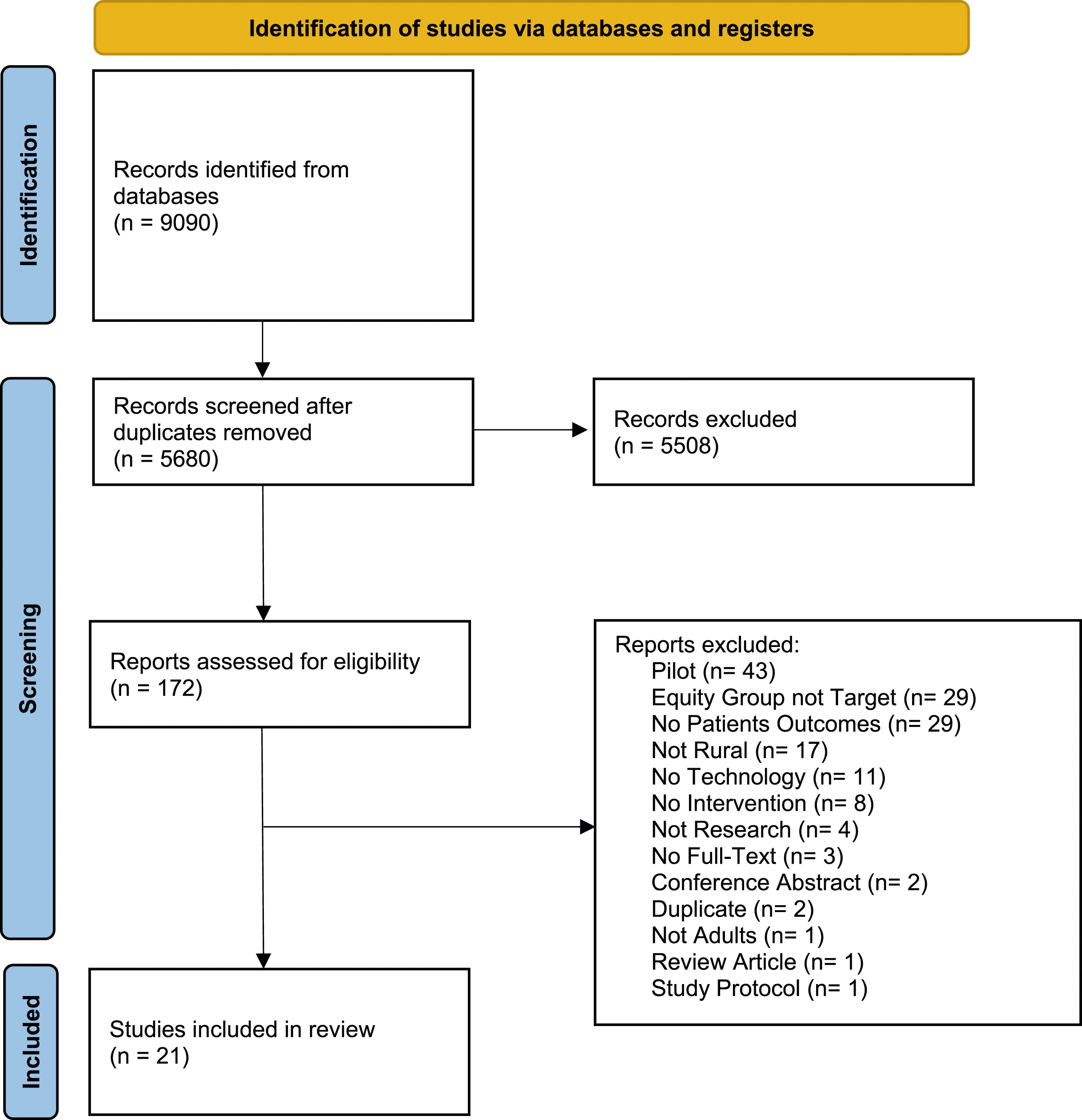
Quality of Evidence
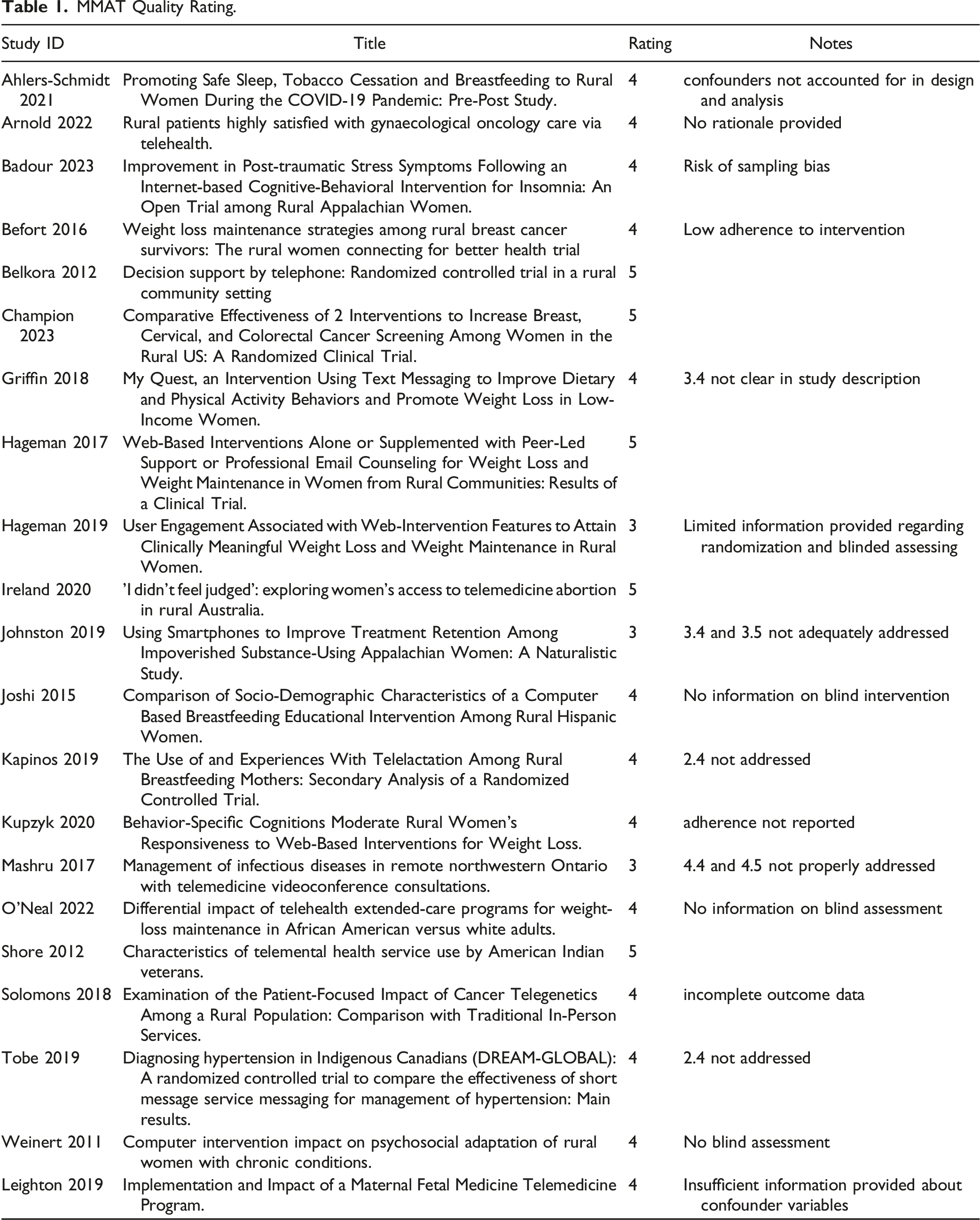
Articles were assessed for bias using the McGill mixed methods appraisal tool (MMAT; version 2018). 30 The MMAT was the most appropriate risk of bias tool as it allows for tailored appraisal based on study design27,31 and has been used extensively in previous mixed studies reviews.32–34 No studies were excluded based on the risk of bias assessment.27,31,35 Each study design was scored “yes” or “no” according to five criteria to create a total score ranging from 0 (high risk of bias) to 5 (low risk of bias). A single reviewer (MF) conducted risk of bias assessments that were verified by a second reviewer (LB).
Data Extraction
The data extraction focused on equity-deserving groups, the health technology interventions, and three important categories of outcomes: (1) patient-related (e.g., health metrics, satisfaction), (2) healthcare-related (e.g., access, utilization), and (3) cost-related. The data extraction tool, developed in Excel (see Appendix B), was piloted using two included studies before being entered into Covidence for final extraction. 29 Data extraction was then conducted by a single reviewer (MF), which was checked for correctness and completeness by a second reviewer (LB). 29 Findings related to each of the outcomes, whether significant or non-significant) were extracted and did not undergo recalculations or transformation. Significant results refer to statistical significance unless specified as clinical significance.
Analysis
Study characteristics were analyzed descriptively (e.g., countries/equity-deserving populations represented, health technologies used, research design). Findings were synthesized narratively from extracted study outcomes and grouped according to each research question (patient, healthcare, and cost-related outcomes). 29 Quantitative and qualitative findings were integrated within appropriate outcome groups to enhance understanding of both effectiveness (quantitative) and experience (qualitative). 36
Findings
Overview of Studies
MMAT Quality Rating.
Seven articles provided a definition for rurality. These were based on designation by U.S. census, 37 Rural-Urban Commuting Area Codes provided by U.S. Department of Agriculture, Economic Research Service,38,39 National Rural Health Association Policy Position, 40 Federal designation as medically underserved area/medically underserved population by U.S. Census Bureau, 41 Accessibility and Remoteness Index (Australia), 42 and 25 miles outside a town or a city of 12,500 or more. 43
Summary of Included Articles.

Outcomes were themed according to patient, healthcare, and costs, and sub-themes generated within each of the main themes. Significant and non-significant findings are reported.
Patient Outcomes
Fifteen articles reported on patient outcomes, including knowledge, self-efficacy, and weight loss.38–41,43,45–51
Knowledge
Knowledge was measured as an outcome in three studies, with consistent findings of technology use yielding knowledge improvements similar to usual care and with no between-group differences. Two studies used videoconference compared to in-person delivery for educational46,47 and counselling 47 interventions, while the third study compared a computer-based educational intervention to printed educational material. 40 However, in one study, pregnant or post-partum women receiving a sleep intervention via videoconference sessions were more likely to know about local resources at the end of the sessions compared to in-person sessions (p < .001). 46
Self-Efficacy
Domain-specific self-efficacy was reported in two studies with mixed findings. Rural women with cancer who received a decision support telephone intervention showed a significant increase in their confidence to be informed and involved in care (decision self-efficacy) compared to rural women who had usual in-person care (p = .006). 41 In contrast, in another study, breastfeeding self-efficacy was not significantly different between Hispanic pregnant women receiving the computerized education intervention compared to those receiving print education. 40
Psychosocial
Psychosocial outcomes (social support, acceptance, depression, and stress) were measured in one study examining the impact of an 11-week web-based intervention for women with chronic diseases. 43 The intervention group showed significantly better scores in acceptance of illness score (p = .001), depression (p = .010), and stress (p = .005) compared to the control group. 43
Weight Loss
Five studies exploring diverse technology-based interventions (telephone, text, web-based) found significant improvements in weight lost, regained, and/or maintained in rural women following the interventions.38,39,43,45,48,49 Women cancer survivors in a group telephone weight-maintenance intervention regained significantly less weight than the mailed printed newsletter group that received no individual contact (3.3[4.8] vs 4.9[4.9], p = .03). 38 In a comparison of individual versus group telephone-based extended-care with educational control between African American and White adults, researchers found differential treatment effects on weight regain. 49 Compared to the control group, white adults in the individual telephone condition and African American adults in the group condition regained less weight during the 12-months weight maintenance period. 49
Web-based interventions alone or when enhanced with other modalities, were found to achieve significant weight loss outcomes. 45 In a comparison of a web-based versus web and email intervention, 48% of all women achieved a clinically significant weight loss of ≥5% in 6 months, and 37% had a significant weight loss of ≥5% at 18 months. 48 Women who received messaging engagement and self-tracking email counselling along with the web-based intervention were 1.65 times more likely to meet the weight-loss targets when compared to the web-only group (p = .046). 48 Self-tracking had no unique effects, but highly engaged women were between 3.75 and 2.33 times more likely to meet weight-loss targets compared to low (b = −1.32, se = 0.34, p < .001) or moderately (b = −0.85 se = 0.31, p < .007) engaged women, respectively. 48 Another comparative study of a web-based intervention with either peer support or professional counselling enhancements showed similar weight-loss averages (∼2.7 kg) after 30 months. 50 However, baseline eating self-efficacy moderated treatment success with high self-efficacy women more likely to meet weight-loss targets in the counselling group and lower eating self-efficacy women more likely to meet weight-loss targets in the peer-support group compared to the other condition. 50 One study using a one-group 12-weeks text-message intervention for rural low-income women found a significant post-intervention reduction in mean body weight (204.3 vs 199.6 lbs, p = .004) and BMI (34.7 vs 33.9, p = .002). 45
Asttrition Intention
Breastfeeding attrition intention did not differ significantly between breastfeeding pregnant rural Hispanic women receiving computerized education compared to print education. 40
Cancer Screening Uptake
In their three-armed RCT comparing usual care, DVD messaging, and DVD plus telephone calls with a trained patient navigator social worker, Champion et al. 51 found the DVD plus patient navigator intervention significantly more effective than usual care (OR 4.01; 95% CI 2.60-6.28; p < .001) in promoting up-to-date cancer screening at 12 months (breast, cervical, colon). The DVD intervention alone was not significantly different from usual care. 51 People living in less disadvantaged rural areas were more likely to undergo cancer screening (OR 0.99; 95% CI 0.98-0.998; p = .03) compared to those in more disadvantaged rural areas. 51
Clinical Outcomes
Three studies measured clinical indicators.52–54 In their RCT, Tobe et al. 52 found both passive and active text message-based hypertension management intervention reduced Blood Pressure among rural indigenous Canadians in 1-year follow-up, but there was no between-group difference. In another study, women who had a perinatal telemedicine consultation had lower rates of premature delivery (p = .022) compared to those receiving in-person services. 54 In their pre-post non-randomized study, Baldour et al. 53 found a significant reduction in Post Traumatic Stress Disorder (PTSD) symptoms following a 9-week, six-module web-based insomnia program for women with PTSD (t(36) = −2.81, SE = 0.65, p = .008). PTSD symptoms were reduced significantly after adjusting for baseline insomnia and depression (F(1,34) = 4.06, p = .05). 53
Healthcare Outcomes
Twelve articles reported healthcare outcomes related to access, utilization, patient satisfaction with the service, and technology challenges.
Access
Six articles reported on healthcare access37,42,47,54–56 and the greater ease and convenience in accessing health services because of the technology-enabled services delivery. An RCT that provided intervention participants with 24-h access to lactation consultants found that 41% (34/83) of video calls occurred outside of regular business hours (between 6:01 p.m. and 7:59 a.m.), giving patients access to otherwise unavailable services. 37 Similarly, a chart review of First Nations veterans who had received mental health services via videoconference saw a significant increase in access to any other health service (p < .01). 56 Over half the women receiving telehealth perinatal care reported having saved over 2 h in round trip driving time, over 75% reported the telehealth visit allowed for a family member to attend, and, for 11% of the women, telehealth prevented them from forgoing care. 54 In another study, patients found videoconference more accessible, not only reporting saved travel time but also saving missed work and easing childcare needs. 47
Ireland et al.’s 42 qualitative study, guided by the Patient-Centred Access model, found that rural women were able to access remote telephone abortion services not provided by their local primary care providers despite it being within their scope of practice. 42 Receiving remote abortion services saved them from one to 16 h of travel time compared to in-person services; however, they were still required to travel for screening checks prior to their telehealth appointment. 42
Despite improved access, technology-enabled services did not remove all barriers.42,47,55 Only 14.7% of telehealth appointments for infectious disease consultations required no travel, but the remaining 85.3% of appointments involved travel to a central hub that housed the telehealth infrastructure; however, the study was of lower methodological quality. 55 Similarly, for patients receiving videoconference genetic cancer counselling, 13% reported travelling 50 miles or more for their appointments at the remote clinic with telehealth infrastructure, but 81% would have travelled similar distances for in-person services. 47
Ireland et al. 42 similarly discussed challenges with accessing telemedicine abortion services. Women reported challenges in transitioning from telehealth to in-person follow-up services. 42 Additionally, the authors noted that the service required women to have high digital literacy and self-efficacy, alongside other favourable situational or personal circumstances such as transport, thus inadvertently perpetuating known health inequities for certain rural population cohorts, especially minority, Indigenous, marginalised, or socially vulnerable women, who may be in the greatest need for access to reproductive health services. 42
Healthcare Utilization
One study reported healthcare utilization. Leighton et al. 54 found in their study, lower NICU use (p < .001) and shorter length of NICU stay (p < .001) among rural perinatal women receiving telemedicine consultation, compared to in-person consultations. Additionally, women in the telemedicine group were 0.65 times as likely to have a NICU stay (p < .02) and 0.20 as likely to have NICU stays longer than 1 day (p < .001) compared to women receiving in-person consultations, indicating no negative impacts on healthcare utilization from the use of telemedicine services.
Patient Satisfaction with Services
Eight studies reported patient satisfaction with technology-enabled healthcare services.37,41,42,44,46,47,54,55 Satisfaction was high with videoconference, ranging from 80% 54 to over 90%, with three studies reporting as high as 98% satisfaction,44,46,55 with another reporting “general” satisfaction with videoconference appointments. 47 Women using an app for lactation support similarly had high (91%) satisfaction. 37 The one study that compared videoconference with in-person care found no significant difference in patient satisfaction. 41 However, between-study comparisons were difficult because of variability in the satisfaction measures used which included qualitative responses (n = 1), standardized Likert scale measures (ranging from 1 to 16 Likert point items) (n = 6), and no measures described (n = 1).
In one study inviting open-ended responses from Australian women with gynecological malignancies about their experiences receiving telemedicine consultation, satisfaction and acceptability were high. 44 Participants valued the relationship building with the specialist and meeting them pre-operatively but valued the local team presence during the consultations to help interpret the information and to provide emotional and practical support. Women valued communication and gained helpful, clear, detailed information and explanations, had their questions answered, and had no suggestions for improvement. Similarly, women accessing remote abortion services were “pleasantly surprised” by staff professionalism and would recommend services to other women. 42 The telemedicine services provided adequate and appropriate information, made the initial screening process timely and smooth, met expectations, was trusted, and didn’t make them feel judged. 42
Technology Challenges
Four studies reported limitations to care and challenges due to the technology.37,47,55,57 During remote genetic cancer counselling, a minority of patients (5%–9%) reported problems with picture freezing and loss of internet; however, 90% of those reporting problems felt they were adequately addressed. 47 Similarly, restrictions from poor cell tower coverage and internet access limited engagement with an app-based service for rural women. 57 Conversely, of participants receiving a telelactation intervention, 50% did not have any video calls, because of discomfort with video (11%), no problems with breastfeeding (26%), no longer breastfeeding (8%), and being too busy (7%). 37 For those receiving remote cancer genetic counselling 32% would have preferred an in-person appointment and 13% did not feel the health technology addressed their needs. 47 Similarly, clinicians in one study reported limitations to videoconference consultations regarding infectious diseases due to poor image resolution and hands-on physical exams. 55
Costs
Eight articles discussed the costs of the technology-enabled interventions but varied widely in the metrics they used to report costs.37,38,41,42,45,51,54,57 While some studies reported the actual program costs of delivering the intervention,38,41,45,51 other studies reported the direct patient costs,42,54 or patient costs related to ownership of the required technologies.37,45,57
Program Costs
Four studies reported additional program costs to traditional in-person services,38,41,45,51 and three acknowledged the additional costs as overall low-cost options for delivering health services.38,41,45 Griffin et al.’s 45 text message weight loss intervention program costs $159/month for all participants, compared to commercially available weight loss programs, which charge each participant between $66 to $204 for a 12-weeks program. Champion et al.’s 51 study to increase cancer screening calculated the cost of their DVD intervention at $326,012 and for the DVD plus patient navigator intervention at $344,829. This cost included the costs of the DVDs, personnel time cost for DVD production and distribution, and consultant costs for DVD production. Befort et al. 38 reported increases in both total program (primarily provider-related) and participant (average hourly wage for all program activities) costs for their group phone counselling compared to the usual mailed newsletter: total program costs of $280 vs. $88 and participant costs of $270 and $189 for the group phone counselling and mailed newsletter respectively. Conversely, Belkora et al. 41 calculated the cost for their telephone cancer decision support intervention as an average overhead charge ($4.99) multiplied by provider time and found the telephone ($48) cost less than in-person ($78).
Patient Costs
Costs to patients were reported in five studies.37,42,45,54,57 One Australian-based study discussed medical abortion services, for which patients had to directly pay out-of-pocket, despite the healthcare system having a public universal insurance scheme. 42 The remote medical abortion services cost women $250AUD (charged through the phone companies) compared to $1500AUD for an in-person surgical abortion. 42 Despite this apparent benefit of the remote service, the researchers do not make explicit if there were any differences in the treatment approaches between the two types of abortion services. Researchers estimated the average cost saving for women receiving telehealth perinatal care of $90.28 per consultation in saved travel using national gas prices and average hourly wage. 54
Technology Ownership Costs
Three studies reported on economic implications for patients of their interventions related to technology ownership rather than direct cost.37,45,57 Of participants in an app-based telelactation study, 97% had a smartphone at baseline 37 compared to participants of an app-based substance use intervention, where no participants had smartphones at baseline because they could not afford them. 57 Similarly, Griffin et al. 45 reported the costs associated with their weight loss intervention included the cost of cell phone ownership, text messaging, and cellular data.
Discussion
The purpose of this systematic mixed studies review was to examine the impact of health technology-enabled interventions serving equity-deserving populations in rural communities. Although outcomes varied across the 21 studies, overall patient and healthcare outcomes improved. Few studies examined the cost implications of health technologies, but early evidence supports cost savings for patients, except for the cost of technology (e.g., smartphone, cellular data plan). The health technology interventions used in the review studies generally improved outcomes comparable to or better than usual in-person care. However, only 11 studies employed RCTs to provide the most rigorous evidence in establishing causality. Further, there were few and highly variable outcomes examined in the reviewed studies, and outcomes were highly specific to the intervention focus, such as weight loss in response to a technologically enabled weight loss intervention, thus making it difficult to draw conclusions about the broader impact of the technologies.
Despite the focus of the studies on equity-deserving groups, a finding from this work was the underrepresentation of all equity-deserving groups except for women. This finding is consistent with the historical underrepresentation of racial and ethnic minorities (people of color) in randomized controlled trials, with a recent study reporting a total minority inclusion of only 3.95% from all RCTs published in the United States during the last 25 years. 58 Further, of the 21 studies included in the review, the majority were targeted at predominantly Caucasian women and addressed “highly gendered” health issues, such as perinatal weight loss and breast cancer. In the few studies that had representation from multiple ethnic groups, beginning evidence suggests differential impacts of telehealth extended care programs for weight loss maintenance between African-American and white adults - racial groups may benefit from different technology-enabled approaches. 49 Although there have been pilot and exploratory studies aimed at health technologies for rural equity-deserving groups, few studies have rigorously tested their effectiveness.
Except for the perinatal studies that were explicitly directed at women, studies did not address how the technologies were tailored to the specific needs of the equity group. Yet beginning evidence from this review for the differential effects of technology-enabled interventions points to the need to tailor technology interventions to user needs. Equally relevant is having technology-based interventions culturally tailored to the needs of equity-deserving groups. Im et al. 59 identified several specific considerations in the cultural tailoring of technology-based interventions for racial and ethnic minority groups, including technology literacy and preferences; language issues; cultural attitudes, beliefs, and values; intervention staff competence; security and confidentiality issues; and time and geographical constraints. User-centered designs are increasingly being used for tailoring interventions and are especially important as technology increasingly penetrates rural communities, as a result of the COVID-19 pandemic.
Findings showed that health technology interventions targeted at rural women and indigenous communities had high levels of satisfaction, consistent with other literature on rural populations 60 and urban-based racial minority populations. 61 Studies have shown that equity-deserving groups can have lower satisfaction with healthcare,62,63 which can, in turn, impact patients' ability to access health services. 64 The high satisfaction reported among the equity-deserving groups in studies included in this review suggests that health technologies generally improved access to health services for these equity-deserving groups. Decreased travel time is a well-established benefit of health technologies. 65 Similar to our findings, poor infrastructure in rural and remote communities, inclusive of reliable internet and cellular networks, has been shown to contribute to challenges with technology solutions in healthcare.66,67 Overly complex health systems limit the uptake of health technologies in rural communities. 68 However, there is a potential bias related to volunteer participants who may have self-selected, are more highly motivated, and are more inclined to be favourable to these technology services. 69
There are costs associated with health technology services. Current findings resonate with other studies, that remote health services save patients money in time and travel. 65 Yet, in some cases, rural participants were still required to travel to access services, a requirement that may in part be addressed as infrastructure development continues to advance in rural communities to allow a full suite of digital tools (e.g., video). However, findings give preliminary evidence of the implied cost of these interventions, particularly the need for technology to utilize services, such as cellular data plans, smart devices, or computers.
Strengths/Limitations
Findings highlight promising evidence for the use of a range of technology modalities across various health services to effect positive outcomes for rural equity-deserving groups. Yet, the findings highlight an emphasis on predominantly white women and an under-representation of many rural equity-deserving groups. The inclusion of only four high-income English-speaking countries may be seen to be a limitation in underrepresenting the scope of technology for equity-deserving groups. Still, for this review, it was important to ensure homogeneity regarding rurality and infrastructure to provide common contexts for drawing meaningful conclusions. Additionally, the diversity of healthcare issues, methodologies, and outcome measures limited the interpretability of findings and the generality of conclusions. Although the COVID-19 pandemic catalyzed the rapid emergence of health technology and a burgeoning of pilot and proof of concept studies to test these emerging technologies, they reflect limited outcomes-focused studies, thus their exclusion from this review.
Conclusion
The use of health technologies for rural women and Indigenous communities showed improved outcomes, high satisfaction, and the potential for low-cost health services. Evidence from the current review indicates that further work is needed to develop knowledge specific to the gaps in understanding of the technologies' influence on equity-deserving groups in rural communities outcomes. Specifically, considerations for the cultural appropriateness of health technologies with underrepresented equity-deserving groups, such as Indigenous populations,70–73 ethnic minorities,22,74,75 and persons with disabilities. 76 While a body of evidence has supported the use, development, and acceptability of health technologies for rural equity-deserving groups, there is a paucity of research testing these interventions. Advancing this promising work through the use of stronger designs (e.g., RCTs), will contribute to a stronger evidence base for health technology applications across a diversity of equity-deserving groups. Yet real-world applications are imperative as they account for the user, their context, and the influence of technology on outcomes. Understanding the experiences of and outcomes that matter to these equity-deserving populations is a strategic research area to better tailor technology-enabled interventions to the users of the technology. Leveraging qualitative work, which to date has been limited, will provide much needed insights to complement the need for more robust research designs. By addressing these gaps in the research, we can better tailor technology-enabled interventions to the unique needs of these populations, ultimately advancing the field of health technology for underserved communities.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.