
Abstract
Keywords
Introduction
Public health midwives (PHMs) play a key role in the Sri Lankan public healthcare system, ensuring the health of communities, with a particular focus on children and women.1,2 PHMs are frontline public health officials appointed by the state. Research shows that the PHM service is well-established in the country and has contributed to favourable child and maternal health outcomes. 3 PHMs are field-based officials who work closely with women and children. This close interaction allows PHMs to understand specific needs of the communities they serve.4,5 However, their roles and experiences can vary depending on the environment in which they work. Therefore, contextualising or adapting their roles to reflect community-specific needs would be most beneficial for the most vulnerable communities. 6 The present study thus explored how PHMs working with children and mothers in the most vulnerable communities in Sri Lanka adapt their role as change agents for community mobilisation while providing healthcare interventions. The findings provide recommendations for enhancing capacities of PHMs through formalised training, particularly in working with children and mothers in the most vulnerable communities of Sri Lanka.
Child and maternal health outcomes in Sri Lanka are relatively good compared to other countries in South Asia. 7 However, some underprivileged communities within the country show child and maternal health deficits due to several factors, including, but not limited to, poverty, social exclusion, and systematic marginalisation.8,9 For example, the estate sector in Sri Lanka has lagged behind both urban and rural sectors, as it has been considered one of the most marginalized and impoverished social sectors in the country.10–12 The estate sector in Sri Lanka is inhabited by Tamil plantation labourers who immigrated from South India during British colonialism to work on tea, rubber, and coffee plantations.10,13
The inhabitants of these estates did not receive sufficient support from the country’s welfare policies, as they were initially not recognised as citizens. 10 Even after receiving citizenship in 1986, they encountered inadequate integration into Sri Lankan society due to their direct subordination to private plantation companies as workers on the plantations. 8 Furthermore, estate inhabitants still face discrimination and barriers to accessing public services, hindering their ability to achieve developmental outcomes. For example, Sri Lanka reports nearly one million teenage pregnancies, with a significant proportion occurring in the estate sector. 14 Despite numerous healthcare interventions by government and non-government agencies, child development outcomes and maternal health have remained low in the estate sector. 15
The PHMs’ work in the estate sector show that their efforts to improve health standards among children and mothers face significant challenges.16,17 This difficulty arises because the community is not ready to go along with certain healthcare interventions initiated by PHMs, because policies sometimes do not reflect community needs. 18 Moreover, some studies indicate that implementing PHM’s interventions could face challenges due to intra-community governing systems, which hinder these interventions by suggesting that they may compromise the cultural integrity of the community.18,19 Consequently, compared to PHMs working in rural and urban sectors of the country, those in the estate sector encounter several challenges. 20 As a result, PHMs have found it necessary to reconfigure their roles, while taking on the role of a social worker who advocates for community mobilizing as an initial step. However, state-defined role of a PHM only include maternal and child health, sexual and reproductive health, health education, gender based violence. 17
Childcare and Maternal Health in the Estate Sector
Sri Lanka is demographically divided into three social sectors: urban, rural, and estate. Over 80% of the population resides in the rural sector, while nearly 5% lives in the estate sector. 21 The estate sector emerged as a distinct social sector when South Indian Tamil labourers were recruited and settled in the mountainous regions of Sri Lanka for tea plantation work. 13 In 1986, these individuals were granted citizenship rights in the country and considered part of the Sri Lankan population. 10 However, they were still viewed as assets or property of private plantation companies, that can hinder realising citizenship rights. 10
Plantation/estate labourers are under the purview of private plantation companies. Estate labourers typically fall under the jurisdiction of private plantation companies. This means that the companies have the power to set wages, working hours, and other conditions of employment for their workers. 13 Private plantation companies also have their own internal legal systems to resolve disputes between workers and the company. As a result, from the outset, estate inhabitants were systematically excluded from welfare services and experienced severe poverty. Currently, 51% of the estate population lives below the poverty line, which has worsened since the COVID-19 pandemic. 22
Despite the implementation of various public health interventions in the estate sector, several structural barriers impede communities from attaining developmental outcomes. While absolute poverty levels have decreased over the past decade, data reveal an increase in the multidimensional poverty of this community. 23 This escalation has adverse implications for hygiene and healthcare, especially for women and children. Additionally, school dropout rates have risen, which obstructs young estate inhabitants from acquiring the necessary level of education. 24 Lack of education has the potential to lower awareness of health and hygiene issues and reevaluate PHM-led programmes. Several studies indicate that as estate inhabitants heavily rely on plantation work, their capabilities are not effectively developed. 25 This deficiency in essential capabilities makes them less likely to engage in other income-generating activities. Simultaneously, in-culture leadership holds significant influence in decision-making for community members, and hence decisions within the community precede government interventions. 18 This combination of factors creates structural barriers to effective healthcare interventions. Nevertheless, in recent years, some community members have broken free from such perilous conditions and strived to achieve developmental outcomes.
While estate labourers may have some legal rights under national labour laws, these laws may not be enforced effectively. 10 In many cases, estate labourers are vulnerable to exploitation and abuse, as they may have limited access to information and support services. 8 There have been several initiatives in recent years to improve working conditions and protect the rights of plantation and estate laborers. 26 These initiatives have included the development of international labour standards, the creation of national monitoring and enforcement mechanisms, and the establishment of trade union and worker rights organisations. However, there is still much work to be done to ensure that estate labourers are treated fairly and with dignity. These issues severely affect child and maternal health in the estate sector. 27
Families in the estate sector are particularly vulnerable to various issues, including health hazards, poverty, climate change-induced challenges, and economic crises. Moreover, the estate sector exhibits a high rate of stunting (36%), which is a significant public health concern. 28 The last demographic health survey (2017) indicates that the rates of wasting (16%) and underweight (36%) are even higher and are classified as “very high” public health concerns. In comparison to other countries in South Asia and developing nations, child and maternal health in Sri Lanka is relatively strong. However, the estate sector faces significant child and maternal health challenges for several reasons, including poverty, teenage pregnancy, and domestic violence, among many other sociocultural determinants.11,27
Antenatal care in the estate sector has been specifically recognized, with an average of 5.4 PHMs per sector, compared to 3.0 in rural areas and 2.8 in urban areas. 28 However, the attendance of estate women in well-women clinics (clinics for women with children aged below 5) is low, at 28.5%. Regarding early childhood care and education, the estate sector still lags behind the rural and urban sectors. 8 Research indicates that the estate sector’s vulnerability to poverty, social exclusion, and a lack of awareness among community members are some of the reasons why childcare and maternal health fall behind those in urban and rural sectors of the country.9,27 Consequently, the traditional role of PHMs may not be suitable for such an environment, as the conditions surrounding children and women might restrict the implementation of healthcare interventions by PHMs.
Community Mobilising and Advocacy
Community mobilisation is a process that empowers a community to take collective action, demonstrating how effective change can be locally initiated. 29 Engaging with communities to identify priorities, resources, needs, and solutions through representative participation ensures that health interventions are appropriately implemented.30,31 Studies in developing regions have recognised a close relationship between maternal care and community mobilisation. 32 Research indicates that before any social development intervention, community mobilisation is essential, as many people in vulnerable communities lack the capability to act collectively towards a common goal. 33 This process involves building relationships, empowering individuals, providing education, building capacity, and developing leadership. 34 Pastor et al. found that community mobilisation promotes health equity at the grassroots level and enables people to devise locally responsive solutions to common problems. 35
Bezboruah demonstrates that community mobilisation is essential for improving healthcare services, particularly for disenfranchised populations who often cannot afford medical care. 36 However, this can be a challenging process when strategies are misaligned, and solutions are diverse. Community advocacy is also closely related to community mobilising, which is a preventive approach that enables people to become active citizens and self-reliant in making informed decisions that affect their lives. 37 As many communities are ill-prepared to accept the changes brought about by healthcare policies, community mobilisation through advocacy is a requirement for healthcare interventions.37–39 Dodson et al. explored that even non-community-based health officials, such as paediatricians, can work as child health advocates and should be considered an important part of paediatric training. 40 Research conducted by the World Bank also suggests that the impact of community mobilisation through advocacy can positively influence reproductive, maternal, newborn, and child health in several ways. 41
Community advocacy can be implemented on different levels, including individual, group, local, national, or transnational bases. 38 The importance of community mobilisation through advocacy to strengthen maternal care and child health has been widely acknowledged, yet the interventions of PHMs in the most vulnerable communities have not received much attention. Furthermore, community-based advocacy proves effective for the most vulnerable communities, such as the estate sector in Sri Lanka. Apart from a few interventions by non-government organisations, there are no structured community mobilisation programmes in the estate sector aimed at improving child and maternal health. 42
Public Health Midwifery Service in Sri Lanka
Public health midwives (PHMs) are government-appointed healthcare professionals in Sri Lanka with the responsibility of providing maternal and infant care at the community level.1,3 PHMs are dedicated healthcare providers who focus on families and serve as frontline health workers, delivering care within the home environment to women and children. They operate under the Family Health Bureau, which is a division of the Ministry of Health. 17 PHMs play a crucial role in the implementation of family planning and reproductive health policies in Sri Lanka. Additionally, they often assist in conducting early childhood development programmes. PHMs who work in the estate sector hold significant importance, as they are an integral part of the estate community, providing healthcare services to estate residents. 8 Several studies have described how PHMs play a crucial role in addressing domestic violence through antenatal care in vulnerable communities in South Asia, with their interventions in this regard being mandatory.17,43
PHMs provide a range of services related to sexual and reproductive health, as well as antenatal, postpartum, and neonatal care in urban, rural, and estate areas. 17 Their training includes breastfeeding, healthcare services for children and mothers, clinical practice, monitoring child growth, nutrition, women and work, and low-birthweight and sick babies.1,5 While this training does not necessarily focus on community mobilising or advocacy, providing PHMs with training on such activities, including addressing intimate partner violence, can bring about significant benefits. Research has also shown that a common approach for all communities will not generate the expected child and maternal health outcomes.4,5
Jayatilleke et al. demonstrates that training PHMs to address issues at the family level, including intimate partner violence, can yield more favourable results than other interventions. 16 Conversely, the role of PHMs in some rural areas in promoting adolescent and youth-friendly health services is deemed unsatisfactory. 44 However, Fernando et al. have emphasised that the reduction in maternal deaths and disabilities in Sri Lanka was achieved through effective PHM interventions. 45 Despite research highlighting the role of PHMs in various healthcare contexts, their unique role in the estate sector, particularly in community mobilisation and advocacy, has not been adequately recognized.
Therefore, the aim of the present study was to explore how PHMs have adapted their roles as community change agent who facilitate community mobilising before implementing healthcare interventions for children and mothers in the estate sector of Sri Lanka. In addition, the current study provides recommendations on how PHMs working with vulnerable communities can be trained to comprehend their social standing in a way that aligns with the unique needs of those vulnerable communities.
Methods
Study Design
The present study employed an exploratory qualitative research strategy, which allows to produce in-depth explanations of the considered research problem from a subjective perspective. 46 The research had an inductive nature, and a reflexive thematic analysis approach was employed. 47 Given that the study aimed to comprehend the experiences of PHMs in their fieldwork together with community participants’ viewpoints, this inductive and exploratory design was chosen to explore how PHMs adapted their roles to work with people in a vulnerable community. The study adhered to the Consolidated Criteria for Reporting Qualitative Research. 48
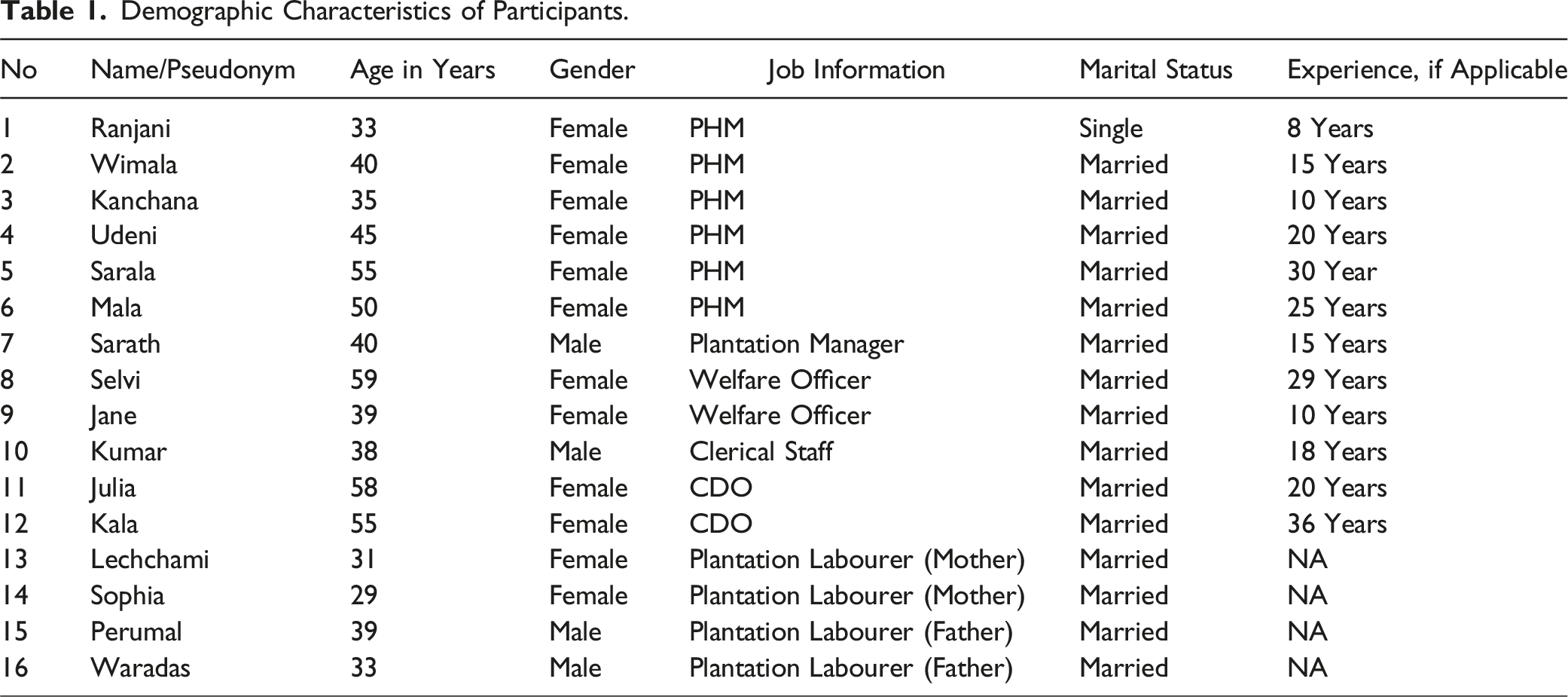
Participants
Demographic Characteristics of Participants.
Data Collection and Setting
In-depth interviews were conducted with all participants, employing two semi-structured interview guides, one designed for PHMs and the other for the remaining participants. The interview guides included open-ended questions that encouraged participants to provide detailed explanations. These interview guidelines were developed based on the insights gathered from the literature review and previous research experiences with the same community. PHMs were interviewed to explore their engagement in the estate sector, while all other participants were interviewed to understand how PHMs provide services in the estate sector. These two sets of interviews offered three perspectives on the role of midwives in the estate sector: PHMs’ perspective, estate sector bureaucrats’ perspective, and community members’ perspective. These perspectives are consolidated and presented thematically.
The interviews were conducted on-site, and all participants actively engaged in the process. No participants dropped out during the research. PHMs were interviewed in their offices at the estates, while parents were interviewed in their homes. CDOs and other bureaucrats participated from their respective offices. Two skilled research assistants helped the researcher record the participant narratives. Interviews were recorded, and field notes were taken. The support of research assistants included tracking time, observing reactions, and ensuring that all questions were addressed.
Data Analysis
Data were analysed using the reflexive thematic analysis method as proposed by Braun and Clarke. 49 The collected data were reviewed on a daily basis. The data were transcribed verbatim by the author and analysed through manual coding, with the necessary narratives being translated into English. Braun and Clarke 49 outline a six-stage thematic analysis technique, including familiarising oneself with the data, developing initial codes, identifying themes, reviewing themes, defining and labelling the themes, and writing the final document. 47 This thematic analysis method provided a flexible and robust framework to analyse the data. After developing initial themes, the findings were presented to five participants, representing PHMs, estate sector bureaucrats, and community participants, to confirm that the themes accurately reflected the reality of the estate sector. To ensure the trustworthiness of this study, Lincoln and Guba’s quality criteria for qualitative research were adopted. 50 These criteria encompass credibility, transferability, dependability, and confirmability and offer an evaluative framework for establishing the credibility of this qualitative research.
Ethics
The Research Ethics Committee of the Faculty of Humanities and Social Sciences, University of Ruhuna, Sri Lanka, granted ethical approval. The research was conducted in accordance with the guidelines of the Helsinki Declaration. Informed consent was obtained from each participant before data collection.
Results
Theme 1: Capacity for Advocacy and Community Mobilisation
Subtheme 1.1: Linking the Community With Healthcare Policy Interventions
The role of a PHM as an advocate at the community level is highly critical. PHMs serve as intermediaries, bridging the gap between excluded estate communities and state-led healthcare policies. Unlike urban and rural communities, the estate sector often lacks access to state or non-state funded services. However, PHMs’ community mobilisation interventions establish a connection between these communities and state-led health policies, thereby linking them to global sustainable development goals. The ‘link between health policy and community’ can be developed only through community-relevant mobilisation as found in this study.
A Welfare Officer note: “Estate women often lack awareness of health- and hygiene-related behaviours. When new methods are introduced, they may not readily adopt them. PHMs have the potential to effectively guide them, given the close collaboration between women and PHMs.” (Jane, 39-year-old)
However, it is worth noting that not all PHMs actively engage in these efforts, and their motivation and level of experience influence the extent to which they participate in community mobilisation in the estate sector. “I understood that the health policies discussed in training programmes should be revised and adapted to local needs before being implemented in the estate sector.” (Udeni, PHM, 50-year-old) “We connect these people to state-led programmes. Our role is like an intermediary role, which is essential for these communities.” (Ranjani, PHM, 33-year-old)
In addition to linking the community with external state-led healthcare policies, PHMs strive to communicate with policymakers to convey community-level reflections on policy implementation. Even though PHMs are not required to do this, they highlight its importance, as the progress of all programmes depends on how community members perceive them. “Instead of home gardens, we have suggested community kitchen programs to reduce malnutrition by incorporating estate residents and utilizing available resources.” (Kanchana, PHM, 35-year-old)
Encouraging the implementation of home gardens, akin to those in rural areas, poses challenges in estates due to the lack of access to arable lands. Additionally, the time constraints faced by estate workers on plantations make it difficult to allocate time for homegrown vegetable gardens. However, recognising this, PHMs have realised that promoting a community kitchen programme can effectively contribute to reducing malnutrition, even among estate inhabitants. This programme involves selecting vegetables, cooking, and sharing food among children and those in need with the support of the community. The initiative not only provides a weekly nourishing meal but also allows individuals to allocate time for self-care and foster connections within their community. “We let PHMs know what we think about certain programmes. For example, at first, they gave a cereal mix to kids in early childhood centres, but it did not work because the kids did not like eating it. After talking with PHMs, they came up with a programme on healthy biscuits that worked well.” (Perumal, Plantation Labourer, 39-year-old)
The data indicates that two-way communication is crucial because community members are less likely to communicate with higher-level authorities. Acting as intermediaries, PHMs disseminate knowledge to the local population while also conveying the community’s perceptions to higher authorities during programme evaluations. It is challenging to convey the authentic reflections of people on the ground to the policy level, as communities are not directly linked to policymaking authorities. This communication gap is bridged by PHMs, who play a vital role in conveying policy expectations to communities and reflecting community perspectives on policies to higher-level policymaking authorities.
Subtheme 1.2: Intervention as a Community Leader
Mediation by PHMs in the estate sector is crucial for mobilising community leaders, organising community preparedness to address issues, and establishing an environment conducive to child and maternal health. As community leaders who are aware of community social problems and concerns, PHMs are better suited to play this role. Although the role of a community leader who intervenes in advocacy and mobilisation is not formally stated, it is considered to be their moral obligation. “Guiding these individuals on the right path before our healthcare intervention is not explicitly mentioned but is one of our moral obligations. Some PHMs may not fulfil this due to a lack of experience or commitment.” (Mala, PHM, 50-year-old)
This shows that PHMs play an important role in keeping vulnerable communities on track and organised towards receiving healthcare services. This is because marginalised and vulnerable communities often prioritise their efforts to overcome poverty, which can lead to the neglect of healthcare services for children and women, as described above.
PHMs can take on the role of a community leader as they frequently advocate for community concerns and, in some instances, intervene in community organizing. For instance, PHMs assist communities in establishing community organisations, facilitating discussions on their issues, and proposing solutions. Given that PHMs visit families in estates with children more frequently, inhabitants are more inclined to follow their guidance, although obtaining their consent can be challenging in certain situations. A mother explains: “She not only visits our home, but she also assists in the organisation of community activities such as the community kitchen.” (Sophia, 29-year-old)
Subtheme 1.3: Capacity for Negotiation With Local Level Authorities and Local Leaders
PHMs receive support from both government and private plantation management, which leads estate inhabitants to regard PHMs as community leaders who can guide them in making informed decisions. However, certain sub-culture practices and community-level leadership structures may hinder the relationship between PHMs and estate inhabitants. This is mainly due to misunderstandings between public health officials and community members, or to policy mismatches with cultural realities. In comparison to the urban and rural sectors, advocacy interventions are thus essential prerequisites before establishing any healthcare interventions in the estate sector. “Plantation management holds more influence than the state-led administration in this context. In estate communities, people generally adhere to the rules set by plantation management. As a government officer, my first step is to negotiate with plantation management before implementing specific programs in the estate.” (Udeni, PHM, 45-year-old)
Gaining entrance to community life can be challenging without negotiations with plantation management and community-based traditional leaders. Since plantation management holds control over estate inhabitants, establishing close dialogue with them is essential before initiating any healthcare interventions.
Advocacy is generally started with discussions with these local authorities. The initial step in the community mobilising role is to adjust the community so that inhabitants can be incorporated into healthcare programs. However, this relies heavily on the negotiation skills of the PHM. Consequently, some PHMs may struggle to implement programmes if they lack experience and negotiation skills. “Initially, I faced challenges working within that estate. The plantation management and local leaders did not offer their support, and as a result, I could not carry out my work as planned.” (Ranjani, PHM, 33-year-old)
Subtheme 1.4: Connect Families to the Broader Community Context (Holistic Mobilisation)
Without a supportive family and community environment that fosters conditions conducive to the health of children and mothers, providing external services becomes challenging. The participants thus emphasise the importance of mobilisation led by PHMs at the community level. “Our parents received guidance from a midwife on how to access a good education. Otherwise, they were not aware of education or healthcare.” (Julia, Child Development Officer, 58-year-old) “Even though these people are introduced to new health practices, they are less likely to follow them. It has become a cultural norm. Community dialogues are essential to change those behaviours.” (Wimala, PHM, 40-year-old)
This illustrates that child and maternal healthcare in the estate sector of Sri Lanka is often compromised because community members do not prioritise it when dealing with poverty-related concerns. Navigating the socio-cultural environment, strongly linked to poverty and other challenges, relies significantly on the guidance offered by PHMs.
PHMs and CDOs recognise the importance of holistic mobilisation, as it engages the entire community, as far as PHMs can. According to PHMs and CDOs, advocating for estate residents in a formal office setting is less effective than educating people on healthy practices and encouraging them to adopt them in their own homes. The PHMs’ capacity for advocacy is essential in such situations. “Parents can gain firsthand experience when I educate them in their homes, without asking them to come to my office.” (Sarala, PHM, 55-year-old) “We should not only make constant visits to families with children under the age of five and mothers, but we should also try to communicate with other community members.” (Mala, PHM, 50-year-old)
PHMs can closely recognise differences between families, enabling them to intervene effectively to address case-specific issues. They visit families with children under the age of five and pregnant mothers, also making additional visits as necessary. This approach allows them to comprehend the overall situation of the family, suggesting effective solutions when needed and empowering families to understand their weaknesses and strengths. This, in turn, facilitates the identification of effective sources for the issues encountered. Given that problems encountered by families are unique, a family-specific intervention is required, varying from one family to another. This necessitates a holistic understanding of the family background. This is where the importance of PHMs’ case (family or individual) -specific interventions becomes crucial.
Subtheme 1.5: Appropriate Use of Social Capital for Community Mobilisation
Social capital, or the strength of networks among community members is an asset. In estate communities, bonding social capital, or the strength of internal community relationships, is often directed towards poverty-related concerns, leading to a lack of community awareness regarding childcare and maternal health. For example, bonding social capital may be used to promote sub-culture practices such as early marriage, endogamy, and child labour. However, social capital can also be harnessed for effective health improvements. For example, in some estates, PHMs have initiated community organisations with local leaders, including mothers and children, to focus on healthcare and family well-being. Leadership roles are given to these community members, enabling them to utilise the strength of internal community relationships to promote positive health outcomes. “With the support of PHM, we have developed a women self-help group.” (Lechchami, Plantation Labourer, 31-year-old) “Due to self-help groups, now some women and children tend to forward their family-related issues to likeminded people and seek solutions at the community level.” (Sophia, Plantation Labourer, 29-year-old)
The role of a community leader becomes evident in activities where PHMs encourage communities to identify problems related to the community and propose relevant solutions.
Subtheme 1.6: Building Self-Reliance and Self-Mobilisation at the Community Level
Despite PHMs not receiving specific training in community mobilisation, the activities they engage in with estate communities contribute to improving the readiness of estate community members for child and maternal health. This also highlights the utilisation of community assets rather than relying on external resources, which are often in short supply. Some PHMs in selected estates have promoted the use of community assets and the understanding of real needs and social standing within the community. Empowering estate communities to recognise their true social standing has motivated them to seek alternatives and opportunities to ensure the well-being of children and mothers. “Eating chapati is common, but it is not very healthy. I have encouraged them to make chapati by mixing it with vegetables, which enhances its nutritional value.” (Wimala, PHM, 40-year old) “In collaboration with an NGO, the PHM introduced a sustainable cooking system that reduces wood burning, which has been beneficial in reducing respiratory diseases.” (Sarath, Plantation Manager, 40-year-old)
Previously, women in estates used to collect firewood and burn it in their kitchens, generating a significant amount of smoke. This practice was highly hazardous, leading to an increase in respiratory diseases and, in some cases, even house fires. Children were particularly vulnerable to burns due to careless firing in kitchens. Recognising the severity of these issues, a PHM in an estate together with an NGO introduced a safe-cooking system designed to reduce smoke and mitigate the risk of fire burns for children. These findings underscore the importance of contextualised advocacy and community mobilisation in understanding real needs and leveraging existing assets without heavy reliance on external agencies.
Subtheme 1.7: Promotion of Linking Social Capital (Connect the Community to External Resources)
PHMs work to establish connections between community members and external resource centres. The current study demonstrates that the disconnect between estate communities and external resource centres, such as NGOs, can have a negative impact on child and maternal health outcomes. However, it was discovered that PHMs can bridge this gap and connect the community to external resource centres, which can, in turn, contribute to improved child and maternal healthcare outcomes. “Mothers in estates often lack access to resources because they are unaware of them. We should introduce them to these external opportunities.” (Sarala, PHM, 55-year-old) “PHMs have the ability to bring plantation management, local cultural leaders, outside institutions, and communities together.” (Kumar, Clerical Staff Member, 38-year-old)
Data indicates that successful advocacy and mobilisation efforts require PHMs to localise and tailor their interventions to local realities. In general, community-level advocacy and mobilization efforts by PHMs which are tailored to the needs of estate inhabitants can create a favourable environment for implementing health policy interventions.
Theme 2: Supporting as a Change Agent for Family-Life Adjustments
Subtheme 2.1: Initial Interventions for Capacity Development
In addition to their advocacy interventions and community mobilisation efforts, PHMs’ role as change agents at the family level can help family members effectively integrate with healthcare policies. Their support at the family level is vital for enhancing family members’ capacities in various areas, including financial management, reproductive healthcare, and interpersonal relationships. PHMs can directly intervene in developing these capacities at the family level during their initial visits and consultations with families. Unlike centre-based child and maternal healthcare facilitation, family-based facilitation is challenging in the estate sector due to the lack of organisation within families to support such interventions. Therefore, it is essential to prioritise improving the family environment in any advocacy intervention at the family level. “Although family-centred child and maternal healthcare is ideal, it is difficult to implement in estates. Therefore, we decided to promote centre-based childcare, which connects children and mothers to a service provisioning centre such as a midwife’s office. However, this approach is not sustainable. Therefore, we are now intervening to adjust families to be supportive units, which is a more sustainable approach.” (Ranjani, PHM, 33-year-old)
PHMs’ experiences reveal that they have characteristics of a change agent. PHMs are the only state-officials who work closely with families in the estate sector, and their initial belief in fostering happier families contributes to improved child and maternal care.
Subtheme 2.2: Advocacy for Financial Literacy in the Family
One important advocacy intervention is helping families manage their finances. PHMs provide support in arranging priorities for family life and managing financial resources accordingly. Estate inhabitants often show a lack of health and education development, mainly due to a lack of financial management at the family level. This is often because they have not been effectively guided. Without strong financial management at the family level, helping them with healthcare services is not worthwhile. For example, at least opening a bank account and investing money on a small scale has not been promoted, unless through PHMs’ advocacy interventions. “They lacked guidance on how to manage money within the family, which led to their income being insufficient to meet their overflowing needs. Although their income was low, I observed that it could be managed more effectively. Therefore, I constantly guided them on how to do so.” (Kanchana, PHM, 35-year-old)
Subtheme 2.3: Advocacy for Developing Interpersonal Skills
PHMs also play a crucial role in developing basic interpersonal skills among family members. This is important because family members, particularly adults in estate families, often lack these skills. Since several generations (at least four) may live in the same household, strong interpersonal skills are essential to supporting child and maternal health. For example, older adults can play a vital role in supporting child and maternal health, but this is often neglected in estates. Some PHMs have found that increasing interpersonal skills among family members can enhance their understanding of the responsibilities essential to creating a supportive family environment.
Extramarital relationships are often seen within estates, mainly due to the congested environment in families with several generations living together. This can lead to severe difficulties for children and women, including abuse and depression, as participants indicated. As external community leaders, PHMs can intervene through advocacy efforts to help families on such situations manage relationships between family members effectively. “I supported a family to build new house by negotiating with the plantation welfare officer. Extramarital relationships are more likely to occur when many people live in the same family. This needs to be explained to mothers and fathers, because they have no idea about it.” (Sarala, PHM, 55-year-old) “Intimate partner violence is a common and normalised problem here. When men commit violence, women frequently do not know how to respond. PHMs can advocate for them to self-mobilise so that they can respond effectively to such events. Without this change in the family, our healthcare interventions will be ineffective.” (Selvi, Welfare Officer, 59-year-old)
Subtheme 2.4: Advocacy for Sexual and Reproductive Health
Reproductive and sexual health (RSH) are not yet openly discussed among partners but are critical for a healthy family life. Advocating for sexual and reproductive health is part of the generic role of PHM. However, the interventions for this in the estates are unique in that PHMs are required to constantly make estate people aware of concerns related to sexual and reproductive health. PHMs are ideal to support estate residents in achieving safe and healthy RSH outcomes. Without their interventions in family counselling, several challenges can arise, including abuse, rape, intimate partner violence, and mental health disorders. In the past, unwanted pregnancies were a serious problem in estate communities. However, PHMs have played a key role in reducing their prevalence through introducing and contraceptive interventions. “I was initially opposed to the idea of contraceptives, but the PHM convinced me to reconsider. They helped me see that having several children without the financial capacity to support them could be detrimental to my family’s well-being.” (Waradas, Plantation Labourer, 33-year-old) “Some people believe that having more children is a blessing, but they may not understand how to nurture them. This knowledge should be provided to these families, as there is no one else to give it to them.” (Mala, PHM, 50-year-old)
Subtheme 2.5: Advocacy for Successful Parenting
Successful parenting is a key determinant of child well-being. Parental support is essential for children to effectively engage with PHMs’ interventions. Many estate residents lack parenting skills because they are unaware of them. PHM guidance is needed to inculcate successful parenting skills in these parents. Successful parenting involves helping children develop their self-esteem, strong communication skills, and the courage to think critically and make good decisions at home, school, and in the community. However, the findings of this study show that parents are often unaware of these important aspects of parenting. Therefore, PHM support is essential to helping them change their behaviours so that they can better meet their children’s needs. “Many mothers and fathers lack the knowledge and skills to nurture their children effectively. We should guide parents to become successful parents by providing them with parenting education and support.” (Wimala, PHM, 40-year-old)
Child development requires a supportive family environment. This is not possible without changing the mindset of family members. PHMs’ advocacy has enabled some families to become self-advocates, so they can make informed decisions about their family life while contributing to child and maternal health care interventions.
Subtheme 2.6: Support for Work-Family Balance
When men migrate to urban areas in search of employment, women are often left behind to manage both household responsibilities and contribute to estate work. As a result, women were predominantly engaged in unpaid care work (such as childcare and household tasks), which becomes exceptionally challenging when it prevents them from engaging in estate work, thereby affecting their monthly income. PHMs’ guidance in such situations can play a pivotal role in helping women manage the balance between household and work life, which is a significant determinant of child and maternal health. “I had to decide to go to Colombo for a construction-sector labour job, leaving my wife and our newborn child. My elderly parents can support her, but she constantly asks me to resign and come home because she is barely managing her work and family chores. The midwife has helped her a lot to cope with these problems, even advising how to leave their children with older adults.” (Perumal, Plantation Labourer, 39-year-old)
Women play a key role in child health, and child and maternal health are closely interconnected. Consequently, the absence of adequate maternal healthcare often results in diminished child health outcomes in the estate sector. Women’s contributions to their families, particularly in terms of childcare, are indispensable. When women are unable to actively participate in childcare, external interventions become less effective and are at risk of failing. A mother noted (Sophia, 29-year-old): “I have four children. My husband works as a contract worker in Hatton. In order to feed my children, I have to work on the estate, but this is very difficult as now I have to take care of the youngest child, who is three months old. The eldest daughter (8 years old) now looks after my other children. The son, at the age of five, even supports this.”
Despite knowing that both children cannot provide the necessary care for the toddler, even while compromising their own needs during childhood, the mother is often powerless to act. PHMs and other estate officials have addressed many such severe cases through partnership interventions, often led by PHMs.
The second theme illustrated how crucial advocacy interventions by PHMs at the family level are for keeping estate community members on track with child and maternal health.
Discussion
Globally, several health-related policies have been adopted to improve child and maternal health, with a particular focus on the most vulnerable communities. 51 Child and maternal healthcare are at the heart of many public health policy interventions across countries. The findings suggest that family-centred health care facilitation is challenging, and PHMs’ advocacy intervention is essential to creating a supportive family environment in the estate sector. The study illustrated that a common approach for PHMs cannot be employed for every community, and it must be adapted to reflect local realities. Without recognizing the upstream factors, 9 any health intervention at the community level is likely to be jeopardized. If the community is not ready and organised to go along with the policies and services provided, no benefits can be obtained from those interventions.
The findings mainly indicated that the prevailing vulnerability of estate communities, attributed to factors such as poverty, low levels of education, low income, and barriers to accessing services, is closely linked to diminished health and hygiene outcomes among women and children in these communities. Welfare policies have not effectively supported estate communities since their inception, which makes it more difficult for women and children to access healthcare.8,10,19,52 The findings of the present study reaffirm this observation while acknowledging the contributions of PHMs in improving health and hygiene among women and children. However, what previous research often overlooks is the unstated role of PHMs as community agents who assist in mobilising communities before implementing healthcare-related programmes.
Even though community mobilisation and advocacy are required to some extent in the urban and rural sectors, the estate sector requires them even more before healthcare interventions, as the participants in this study indicated. Even though PHMs were not provided with formal training in community mobilisation and advocacy, 17 their experience with vulnerable communities enabled them to develop certain capacities to improve the community environment and prepare it for healthcare interventions. The participants’ reflections show that child and maternal health in the estate sector can only be ensured through PHMs’ initial advocacy and mobilisation efforts. However, their training did not include a component on advocacy or mobilisation adjusted to working with vulnerable communities.3,17 Thus, this study shows that without formal training, PHMs have to rely on their experiences and support from other PHMs to advocate for and mobilise communities.
Previous studies have shown that the estate community in Sri Lanka is a highly vulnerable and marginalised community that does not provide a favourable environment for child and maternal healthcare interventions.8,18,52 Some of the reasons for this include poverty, conflict between local leaders, and the dual identity of plantation labourers. 18 The present study supports this argument, but it also shows that effective PHM interventions through advocacy can encourage and enable community members to receive healthcare services and ensure their sustainability. The advocacy process should also be a two-way process in which community realities are reflected, in addition to PHMs’ inputs. 38 However, ensuring self-advocacy and self-mobilization must be at the heart of this process.
PHMs’ role as community change agents is important for achieving child and maternal health goals. Some studies have shown that community nurses and community development officers can help adjust communities in South Asia.16,45 The findings of the present study suggest that this approach could be regularised and provided through proper training. This is necessary because relying on PHMs’ experience and moral commitment alone is not sufficient to ensure child and maternal health for all. When policies are adopted at the estate sector, as shown by Guruge et al. 53 family centred approach would be important, yet findings of the present study reject their conclusion stating that centre based child care can bring about benefits particularly for estate communities.
The findings also illustrated that social capital in estate communities can lead people to promote healthcare-irrelevant culture-based practices, as is the case in some parts of the world.8,54 Studies have found that despite the significance of bonding social capital, which represents the internal strengths of community networks, it can lead to the promotion of culture-specific practices, which may sometimes be hazardous for health.8,25 Some recognized the need of building social capital anew to achieve child and maternal health goals, 55 yet the findings of this study show that existing social capital can be redirected toward child and maternal health policy implementations. Holistic mobilisation is thus recognised as one of the important approaches that a PHM can work on, through which the entire community can be enabled for child and maternal healthcare. Some developing countries in sub-Saharan Africa have shown that community mobilisation can be achieved through non-governmental health organisations, 56 but the findings of this study suggest that state-led PHMs are better suited for this task in the estate sector.
There are gaps in health administration despite the significant improvements brought about by Sri Lankan public health interventions in raising the health standards of vulnerable communities. For instance, De Silva et al. 2 highlight that the number of PHMs available to provide services is insufficient at significant levels. Jayatilleke et al. 16 further note that formal training should include the recognition of issues at the community level for PHMs. In specific areas, such as the special care needs of children, Rohanachandra et al. 57 found that PHMs lack adequate knowledge. Notably, even in India, a South Asian country, inadequate training of community pharmacists has been linked to decreased health outcomes in communities. 58 The findings of the present study complement these observations, indicating a lack of training for PHMs in intervening with vulnerable communities. However, it is noteworthy that there is a capacity for learning from practice. This implies that configuring the role to adapt as a community advocate in the community they serve should take precedence before any other healthcare intervention is provided.
Research indicates that the healthcare of women and children in estate communities has long been compromised.11,25 This is primarily attributed to factors such as poverty, a low level of education, systematic discrimination, and barriers to accessing healthcare services.11,27,59 PHMs’ interventions in these communities have played a pivotal role in raising awareness about primary healthcare, especially for women and children. The administration of estate sectors differs from other rural and urban sectors, as private plantation companies hold significant power in overseeing estate labourers. 18 As a result, these plantation companies oversee issues related to welfare, including health and education. At the same time, studies have confirmed that the pursuit of increased profits in tea plantations has led to the neglect of women and child health. 8 Therefore, as this study found, PHMs role as an advocate is essential for enhancing health of women and children, adopting an approach that combine both plantation management and community members together.
As the present study reveals, capacities and healthcare strategies among estate inhabitants are largely unnoticed. However, it also highlights that existing capacities, particularly those associated with bonding social capital, are vital assets for mobilising people towards health and hygiene practices. Overall, estate inhabitants are not effectively organised for positive change. 20 Therefore, there is a need to empower and mobilise them to recognise the importance of healthcare for women and children. The role of PHMs should be redefined as that of a catalyst or community leader to support the initial organisation of communities and subsequently work towards healthcare improvements. The study emphasises the importance of developing community capacities, with PHMs playing a crucial intermediary role as advocates in this process.
The strengths of the present study include its purposive sample of PHMs, estate bureaucrats, and community members, who shared their experiences with PHM interventions from three different perspectives. Their consolidated viewpoints illustrated the multidimensional role of PHMs working with vulnerable people, and the policy suggestions are based on real-life experiences. This study is the only one conducted in Sri Lanka to understand PHM interventions in the most vulnerable communities, exploring the contextualised techniques they employ to mobilise communities. However, the study’s focus on estate communities limits its understanding of other vulnerable communities, such as indigenous and slum communities. Further research on these communities is suggested.
Policy Implications
Even though the public health midwifery service is well-established in Sri Lanka, the present research found that it needs to be contextualised to reflect community-specific concerns. As PHMs are not specifically trained to comprehend the wider sociocultural context of health, they must acquire knowledge through experiences to understand how the surrounding sociocultural environment influences the health of children and women. Therefore, PHMs’ training should include a component on the social and cultural determinants of child and maternal care. PHMs should also be trained to work with vulnerable communities, in addition to receiving general sexual and reproductive health training. PHMs’ intervention in estate communities should not be reduced to just make aware communities on RSH. Instead, it should be recognised as a service that involves community mobilisation for better change. Negotiating with several agencies such as NOGs, dealing with local leaders, and promoting positive behaviour change are all activities that require careful and formal training. Therefore, it is recommended to provide PHMs with training on advocacy and community mobilisation. To support PHMs in their community mobilisation and advocacy efforts, policymakers and programme implementers can allocate resources to PHMs to implement community mobilisation and advocacy initiatives; work with community members to promote understanding and support for PHMs’ work; and address social and cultural determinants of health that can hinder community mobilisation and advocacy.
Conclusion
Despite the lack of formal arrangements, PHMs are morally committed to engaging in community mobilisation and advocacy in addition to their main responsibilities. However, this moral obligation can sometimes be neglected. The role of a PHM in the estate sector differs significantly from that in the urban and rural sectors, given the significance of their interventions in family health. Nevertheless, their role as a community change agent in mobilising the community through advocacy is an essential element in the estate sector and is closely associated with positive maternal and child development outcomes. This suggests that community mobilisation is a prerequisite for implementing health policies for child and maternal health in vulnerable communities. Both community-level and family-level advocacy interventions and mobilisation efforts are equally important to establishing a supportive environment, without which any child and maternal healthcare interventions are difficult to implement. The voluntary commitment of PHMs to foster an enabling environment in the estate sector is acknowledged, but they may face challenges in meeting this commitment. These challenges can include a lack of formal training or support for community mobilisation and advocacy, a lack of resources to implement community mobilisation and advocacy initiatives, resistance from community members who are not open to change, and unfavourable social and cultural determinants of health.
Footnotes
Acknowledgements
We extend our deepest gratitude to all who have contributed to this research by freely sharing their stories.
Author Contributions
S.U. conceptualised the research, collaborated in data collection, conducted data analysis, participated in manuscript preparation, and revised the paper. L.S.D.Z. and A.B. contributed to data collection and proofread the final manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.