
Abstract
Partnerships between public health and faith-based organizations draw on the strengths of both sectors to achieve a shared interest in promoting health and reducing disparities. However, information about implementation of faith and public health partnerships-particularly those involving diverse racial-ethnic groups-is limited. This paper reports on findings from qualitative interviews conducted with 16 public health and congregational leaders around the country as part of the early phase of the development of a faith and public health partnership to address health disparities in Los Angeles, CA. We identified eight themes regarding the barriers and facilitators to building faith and public health partnerships and distilled these into 10 lessons for developing such approaches. These interviews identified that engaging religious organizations often requires building congregational capacity of the congregation to participate in health programs; and that trust is a critically important element of these relationships. Further, trust is closely related to how well each organization involved in the partnership understands their partners’ belief structures, approaches to addressing health and well-being and capacities to contribute to the partnership. Tailoring congregational health programs to match the interests, needs and capacity of partners was identified as an important approach to ensuring that the partnership is successful. But, this is complicated by working across multiple faith traditions and the racial-ethnic backgrounds, thus requiring increased and diverse communication strategies on the part of the partnership leadership. These lessons provide important information for faith and public health leaders interested in developing partnered approaches to address health in diverse urban communities.
Introduction
Health disparities accrue because of the complex interplay of factors at multiple levels, including the health system, community, and individual. This suggests that solutions to address disparities must also be multifaceted. Partnerships between public health agencies and faith-based organizations have been increasingly promoted to address health disparities, both in the U.S. and worldwide.1–3 The public health sector, which comprises a network of many organizations including local health departments (LHD), community clinics and hospitals, and community-based social service organizations, among others, typically plays a major role in population health improvements, especially in underserved neighborhoods. 4 But profound cuts to this sector have strained the capacity of public health to achieve its goals. 5 Partnerships between public health agencies and faith-based organizations (FBO) can help increase the capacity of both types of organizations to build and implement initiatives designed to address health disparities. 6 In some cases, these partnerships can also be leveraged to conduct research on the development of new strategies to improve health. 7 Such partnerships draw from public health’s expertise in health promotion and disease prevention and religious congregations’ history of providing social, medical (including health promotion and care) and spiritual support for the community. 8
Congregations are valuable to this partnership not just as venues for promoting health, but as key community stakeholders who contribute understanding on how best to approach the development of programs to meet the needs of the populations they serve. 4 For example, addressing disparities requires developing successful relationships with minoritized communities 9 to scope the barriers to good health and the feasibility of intervention options. Congregations can serve as physical and social locations for health promotion activities, but also can leverage their relationships with community stakeholders to identify and understand community health needs. Religious congregations are credible, stable entities that have significant reach within underserved neighborhoods. There are currently an estimated 384,000 religious congregations in the US, 10 and national surveys have found that about 50% of adults attend religious services at least once or twice a month.11,12, In addition, African Americans and Latinos are more likely to self-identify as religious than the general population.13,14 Congregations provide physical infrastructure and complex social networks that can be leveraged for health promotion and services. 1 They also provide access to informal support, food, health care, and educational and job opportunities through extended social networks and linkages with other community institutions. 15 Minoritized congregations are often viewed as trusted resources by their members1,3,15–17 as well as the broader community and can help provide culturally sensitive programs to improve health. Further, they have a history of social change and advocacy, which can be a key component of some programs and may lead to longer term, structural changes required to truly address health disparities. 1
There is a relatively long history of involvement by the faith sector in health care including early development of hospitals.18,19 However, collaborations between public health agencies and FBOs to achieve specific public health outcomes today are rare and underutilized,3,4,18,20 and the evidence of their effectiveness is limited. This raises the need to develop and evaluate such partnerships. 2 Doing so can provide lessons learned about partnership challenges, approaches taken to overcome these challenges, facilitators to successful collaboration, sustainability and replicability.
Recent research focusing on public health and faith community partnerships suggests that some barriers may include limited resources and funding to sustain the partnerships;1,21,22 resistance to forming relationships due to low trust or competition among potential participants;1,22 and disagreements about goals or approaches among partners.1,22 Conversely, faith and public health partnerships may be facilitated by an approach in which each sector is viewed as an equally important contributor, builds opportunities for increasing partner capacity, has strong communication among partners, and provides transparency around leadership decisions and resource distribution.1,3,21,22 Successful partnerships may also depend on contextual factors such as the political climate, and alignment of goals among partners.1,22 However, it’s not clear how these barriers and facilitators are manifested in partnerships developed in different contexts and among diverse populations or how best to operationalize this information into actionable steps for maximizing partnership efficiency and impact.
The purpose of this paper is to report findings from qualitative interviews conducted with public health and congregational leaders in the early phase of developing a multi-ethnic faith and public health partnership to reduce disparities in South Los Angeles (LA). As has been discussed in more details elsewhere, 6 the RAND Corporation, a nonpartisan, nonprofit research organization, and Los Angeles Metropolitan Churches (LAM), a research and advocacy membership organization of small and mid-sized congregations in Los Angeles (LA) sought to establish a faith and public health partnership to collaboratively address health disparities. The partnership involved religious congregations and public health organizations in South Los Angeles, an area that is overwhelmingly Latino and African American (68% and 28%, respectively, in 2017), medically underserved, and has poor health outcomes across various measures relative to the rest of LA County. The partnership was led by a Steering Committee of 12–15 faith and public health leaders and recruited 66 religious congregations and leaders from the local public health department and four federally qualified health centers to participate in the partnership. A unique feature of this partnership was that it integrated African American and Latino churches that represented the diverse faith traditions and cultures of these communities.
We expected that although the partnership’s diversity was critical, it could also pose challenges for coordination and implementation. Further, we did not choose a health disparity condition to address prior to engaging the partnership. Rather, we wanted to work together with our partners to identify a health issue that would be a community-driven priority and feasible to address in this context. The partnership ultimately chose obesity and diabetes prevention, developed a multi-component and multi-level intervention to address these health issues, and piloted the intervention in a cluster randomized controlled trial with five congregations. The pilot trial found preliminary efficacy of the intervention in reducing weight/weight gain and BMI as well as improving diet in the intervention churches relative to churches in the control condition (6).
As we were embarking on this public health and faith community partnership, we conducted qualitative interviews with faith and public health leaders who had experience in such partnerships to inform our approach and identify practices that we might replicate. This paper examines in detail the themes raised in these interviews which may be more broadly useful to organizations interested in developing faith and public health partnerships.
Methods
Sample/Outreach
Our Community Steering Committee nominated individuals that they knew had participated in faith-health partnerships, in particular those that involved multiple racial-ethnic populations and those that involved bringing FBOs together with public health or health care organizations. We sought a purposive sample, i.e. one that would be diverse across racial-ethnic backgrounds, gender, and sector (faith, public health).
A total of 35 community experts were identified by the Community Steering Committee, representing a range of races and ethnicities, genders, and sectors (faith, public health). The research team attempted to contact and screen all 35 using a standard protocol. This screening process allowed us to collect general background information about each person’s faith and health partnership experiences and asses which experiences were most relevant for our project. A total of 30 people were screened (5 were not reached after multiple attempts). After screening, we excluded six participants because we determined that they did not have sufficient experience with partnerships between public health agencies and faith-based organizations. Instead, they had experience building health focused programs from their experience as public health or faith leaders. We then attempted to recruit the remaining 24 partnership experts, who were from LA and several other cities, to participate in the in-depth confidential interview. Of those, 16 agreed to participate in interviews (3 declined and 5 did not respond after multiple attempts), which were conducted between December 2013 and April 2014.
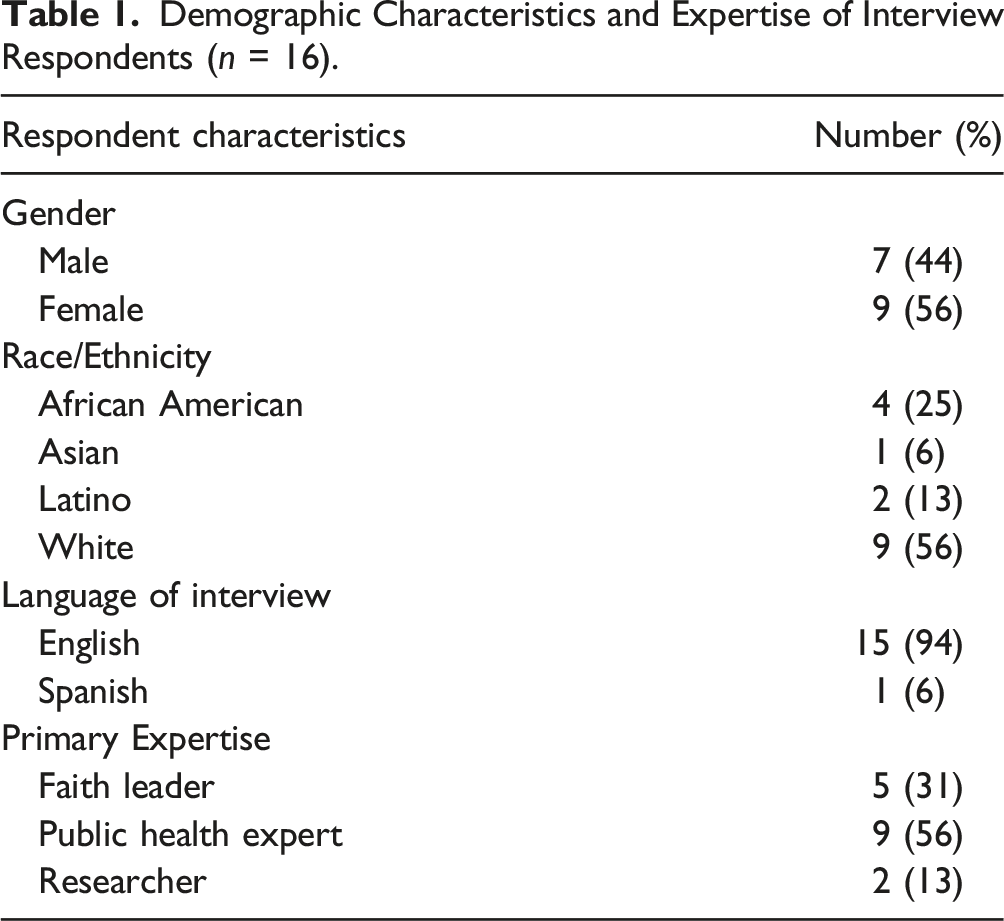
Demographic Characteristics and Expertise of Interview Respondents (n = 16).
Interview
The main interview was conducted by phone (11 interviews) or in-person (5 interviews), based on participants’ locations and preferences. All interviews were audio-recorded (with permission). One interview was conducted in Spanish by a trained bilingual interviewer given the participant’s language preference (Table 1). All interviews were co-led by one of three members of the research team who had extensive training and experience in qualitative research methods. A research assistant took detailed notes and later listened to the recording to embellish the notes and add verbatim quotations. The interview protocol consisted of open-ended items designed to collect feedback from experts about their perspectives about three main topics: (1) past experiences in building faith and health partnerships, including leadership arrangements, organization, and number and type of participants; (2) critical barriers and facilitators to engaging the best-suited participants; and encouraging appropriate levels of participation, leadership, and sustainability; and (3) lessons learned for facilitating consensus, participation, and success. Interviews lasted on average 1 hour.
All study protocols were approved by the RAND Human Subjects Protection Committee. We obtained verbal consent from study participants prior to commencing the screener and the main interview. Our oral consent script covered the standard elements of informed consent including a statement of our confidentiality promise.
Analysis
The screener and main interview data included detailed interview notes, translations (when needed), and audio-recordings. The interview notes were generated and cleaned by the note-taker using the audio recording for each interview 24–48 h after each interview. The lead interviewer then edited the interview notes for clarity and approved the final notes for each interview they conducted. Two of the lead interviewers, who were experts in content analysis techniques, coded and analyzed the interview notes independently to identify major themes in the interview data. Because these interviews were conducted as a first step in a multi-year community-based participatory research endeavor, the partners deemed it important to be able to efficiently glean findings from the interviews and apply them to developing the partnership. Thus, detailed interview notes were chosen over transcripts, given the substantial effort and resources required for the latter. A major goal of the content analysis23,24 was to identify themes that were consistent about partnership building across types of participants, as well as any critical barriers and lessons learned. The two coders created a matrix of themes by respondent and then met to discuss these themes as well as the quoted text representing each theme to gain clarification and arrive at a consensus on the total number of themes. The decision was based on the frequency and how important the coders felt the theme was to all features of the partnership described. The analysts shared preliminary results with the larger research team, which included our faith-based organization partners at LAM, for feedback and then distilled a draft list of themes in the form of potential practices that could guide the management of the partnership, which was shared first with the Community Steering Committee co-chairs and finally the entire Community Steering Committee. Feedback from the Community Steering Committee was used to further refine these potential practices.
Results
We identified a total of eight themes regarding the barriers and facilitators to building faith and public health partnerships. Our respondents had experiences across multiple communities, but some provided specific expertise on the challenges for these kinds of efforts in large urban and diverse areas like LA. Below we summarize these themes and the 10 practices that were derived from the themes that can inform others desiring to undertake similar efforts. The focus of this research was identifying best practices for improving health in the community at large rather than in specific congregations. However, respondents’ experience and comments covered both frames. There is also overlap in these frames as health improvement activities can improve health of both congregants and communities. Nevertheless, we tried to draw out themes related specifically to the broader goal of improving health in the surrounding community.
Building the Capacity of Religious Congregations to Participate in Health Projects
One important barrier to congregational involvement in health projects was identified as limited experience among some congregations with implementing evidence-based health projects. As one researcher with insights on faith-based organizations put it, “Unless you strengthen institution [al capacity to implement the health program], they don’t have the capital that allows them to act [on these interventions].” Forming partnerships with public health organizations is one way to help strengthen the capacity of the congregation. As one faith leader suggested, the simple act of developing partnerships is an important capacity-building tool, “once one relationship is established, it opens the doors and possibilities to other partnerships that can help connect the community to much needed resources.” The capacity of congregants was also mentioned as a motivating factor for congregations to participate in health projects. Thus, providing specific trainings/certifications for congregants facilitates skilled volunteers for a specific health project but also allows the church to provide a resource to its members. For example, at one congregation, fitness classes were offered to congregants, but some class attendees wanted to play a bigger role in the program, so they were trained to become instructors, further increasing capacity to provide classes both in the congregation and to the broader community.
Stigma as a Barrier to Choosing a Health Condition
One element of the community-partnered approach of this project was to facilitate a process for choosing a health disparity condition to address. Respondents identified several ways in which perceptions about health and the church’s role in addressing health may affect how religious congregations make this choice. Some were concerned about the ability of religious organizations to focus on stigmatized conditions such as HIV or mental health. One public health expert cautioned that churches tend to gravitate away from issues related to sex, sexuality or drug use. This respondent also stated that people tend to be wary of mental illness and therefore have difficulty discussing it. Similarly, one faith leader suggested that some groups tend to use language to avoid discussing mental health problems directly. As evidence, he cited the use of the euphemism “attack of the nerves” for mental illness used by some Latinos. Further, respondents were concerned that stigma not only means that a congregation will be less likely to address an issue, but it also reduces the likelihood that an affected person will seek help in a congregational setting.
During the interviews, a couple of suggestions were offered to help increase the likelihood that a congregation might address a stigmatized condition. One public health expert suggested that it would be better to focus first on safer topics such as cancer, obesity, and diabetes and then work in issues that are more difficult to discuss. Another public health expert suggested that exposure to people with a stigmatized condition is important for moving congregations to addressing such an issue. One approach for accomplishing this would be to bring people into congregations to share their own compelling stories.
Trust
Respondents described a variety of ways in which trust is an important element of partnered activities between congregations and other entities such as public health agencies and research institutions. They also discussed how trust is a valuable resource that congregations bring to partnerships (e.g. the trust congregations have among congregants and community members), and that it is important to structure partnerships in ways that prevent distrust from forming.
Respondents emphasized the importance of developing trust with religious congregations as potential partners. As one faith leader indicated, there is a certain level of comfort that needs to be established for a partnership to be successful. Other respondents suggested that when trust is not present, basic intervention activities are difficult to implement. For example, one faith leader noted that congregants might be reluctant to answer sensitive questions on surveys from organizations they do not know or trust. Thus, data quality can depend on the trust that the congregation has in a research partner. Another faith leader further suggested that once trust is established, it is easier to convey the need for social and health services programs. Although multiple respondents suggested that trust is an iterative process developed over time, one researcher pointed out that trust can be embedded within an individual in a partnering organization. He shared that community representatives expressed an underlying distrust of his university but were willing to partner when he was a leader there; however, when he left, trust weakened.
Despite clergy’s common interests and experiences, respondents stressed that there can be distrust among faith leaders in the same community, since congregations compete for congregants and resources. Thus, key members of faith-based organizations in the same community may harbor jealousy and distrust about the intention and impact of interventions. Further, as they struggle for resources, they may focus more intense scrutiny on the distribution of resources within the partnership. As one faith leader suggested, when funding within a partnership went to only one entity it caused the partnership to dissolve. Thus, it was suggested that partnerships should ensure that leadership and resources be distributed equally among partners and that there needs to be a transparent approach to leadership. As one researcher stated, “disclosure and transparency enable you to get past things that seemed closed or shady. In this community, anything shrouded in mystery is imbued with mal-intent.”
Understanding (or Lack thereof) of the Faith Community
Trust can be tested by some researchers’ and public health leaders’ misconceptions about how such programs may fit in the church context. Examples of this were described in several different ways. First, project calendars must consider important church dates and holidays. Second, organizations must recognize that churches are not merely an access point for reaching certain groups of people but have their own interests in participating in health projects. Partners must take the time to build rapport with the congregation to understand these interests before recruiting participants. Further, researchers and program planners need to realize how foreign the research process may be to church participants. As one faith leader shared, depending on the type of project, the work of completing research requirements and planning the project can seem like ticking off a series of objectives rather than the focusing on the health of the population being served. Third, despite the desire to develop formal programs with churches as partners, informal arrangements may be more appropriate or preferred. As one faith leader noted, many church-based programs run without a lot of financial resources, but this draws out volunteers with a strong commitment to success. Finally, several other respondents reflected on the unique challenges of raising funds for non-traditional church activities. One public health expert suggested that many foundations won’t fund a church directly, so they had to create a 501c3 non-profit organization or partner with one to receive funding. Another respondent who had extensive experience both in the faith and research communities pointed out that outside funding comes with contractual obligations that may be difficult or onerous for some congregations to address. From her perspective, these obligations can be a barrier to establishing rapport between funders and congregations. She also felt that the funding organization’s staff sometimes becomes too focused on numbers and reports and that a less bureaucratic structure to funding would be essential for successful partnerships.
In addition to these points, two factors were raised as being facilitators to partnership with congregations. First, one public health expert remarked that churches with liaisons designated to handle health-related issues in the church are good partners because they avoid overburdening the pastor. Second, another faith leader suggested that having a knowledgeable and committed pastor helps lend credibility of the approach for the congregation and community.
Importance of Tailoring and Flexibility
Because of the variability in congregational contexts and populations served through congregation-based programs, some respondents emphasized the need for tailoring health activities to fit the needs, interests, and cultural traditions of the different congregations and mentioned several different strategies. One suggestion was to make the health issue and approaches to addressing it more relevant to the congregation. For example, one faith leader reported that he had suggested showing culturally relevant movies that also highlight a health condition, but the movies he suggested were ultimately turned down because they were viewed by other church leaders as being too secular. Several respondents also mentioned the importance of developing a community-engaged approach to identify how best to tailor the program. As one researcher expressed it, “You may run in the door with a plan, but that plan might be changed. So, I think I come away looking to achieve community engagement in any direction; that is a positive thing. If I want to do x, y, z in the community and the community wants to do [something else], I’m fine with it as long as the community takes ownership-that they understood what their mission was and were very committed to that; that’s what I view as a mark of success-i.e. is the ownership that happened.”
Working Across Racial-Ethnic Groups
Because our proposed partnership involved African American and Latino congregations, we asked respondents about lessons learned in working across racial-ethnic groups. One barrier raised was the misperception that the Latino community is monolithic. Thus, to be successful in working in Latino congregations, a focused effort must be placed on understanding the specific cultural backgrounds of Latino sub-groups that are dominant in the congregation and then shaping the program to fit this perspective. However, other respondents suggested that tailoring can be excessive and is not efficient. Another concern was that diverse populations working together for the first time must develop skills for partnering, whether they are truly integrated into the leadership of the project or merely sharing community space. For example, one faith leader observed that in a past project, there was no familiarity between the different groups of people who could make use of a community park (mostly African American and Latino community members), so the project coordinators held a listening campaign to discuss how to plan park activities. Surprisingly, language and communication were not a major point of discussion, however one researcher noted that their facilitation of a discussion between Latino and African American pastors was strained by the need to simultaneously translate the discussion, and in the future, they would consider running parallel discussion groups separated by language to avoid this difficulty.
Working Across Different Faith Traditions and Congregational Types
Several respondents pointed out that African American and Latino churches’ polity and traditions are different and must be considered when developing relationships with church leadership and planning programs. For example, there was a perceived difference in the willingness of church leaders to engage in health partnerships (although respondents disagreed over whether Catholic churches were more willing to do so than Protestant churches). In addition, respondents emphasized the effect of hierarchy on decision making with more hierarchical or connectional churches sometimes needing permission from the denomination as well as congregational leaders to participate in health or social service programs. Non-denominational churches or those with less hierarchy had more flexibility to make decisions to participate in these activities. Another issue raised was related to congregation size, since smaller congregations tend have fewer resources to address health. Two other issues may make working across various racial and ethnic groups in urban areas where there has been substantial demographic transition such as has occurred in South LA. First, as one researcher described, there are two separate congregational landscapes in South LA. Given demographic transition in South LA, African American churches now tend to be commuter churches while Latino churches tend to be neighborhood-based. This means that the two congregation types have members with different perspectives about South LA. African Americans tend to view this community as the “historic” home for the congregation, where now they live someplace else, and others have moved in. This might impact their commitment to addressing health issues in that community relative to Latino congregants who largely live in the same community as their church. This researcher highlighted another concern, which is that African American church leaders have had a relatively long history of working with political leaders within the city of LA and over time this has institutionalized power within the African American church. However, that power has not been transferred to Latino churches despite the growth of this population in South LA, suggesting that African American churches may have greater access to partners and other potential resources needed to work on social and health services.
Ideological Concordance/Discordance
Related to church context, several respondents highlighted that ideological concordance with the project and its goals is a key facilitator of partnerships. This took on several different meanings. First, the beliefs of the church with respect to engaging in social or health services was considered important. One faith leader considered this a great challenge for partnerships, stating that he had experienced a lot of resistance in his attempts to include the church in a partnership and its proposed health initiatives. Many people within his congregation felt that [health] was beyond their scope of practice, while he felt that this was a central point to their practice stating that “you cannot have a healthy congregation without a healthy community.” Another public health expert suggested that more conservative congregations are less excited about addressing health especially when the frame of the program focuses on topics that might be considered politically liberal, such as health care as a right.
Potential Practices
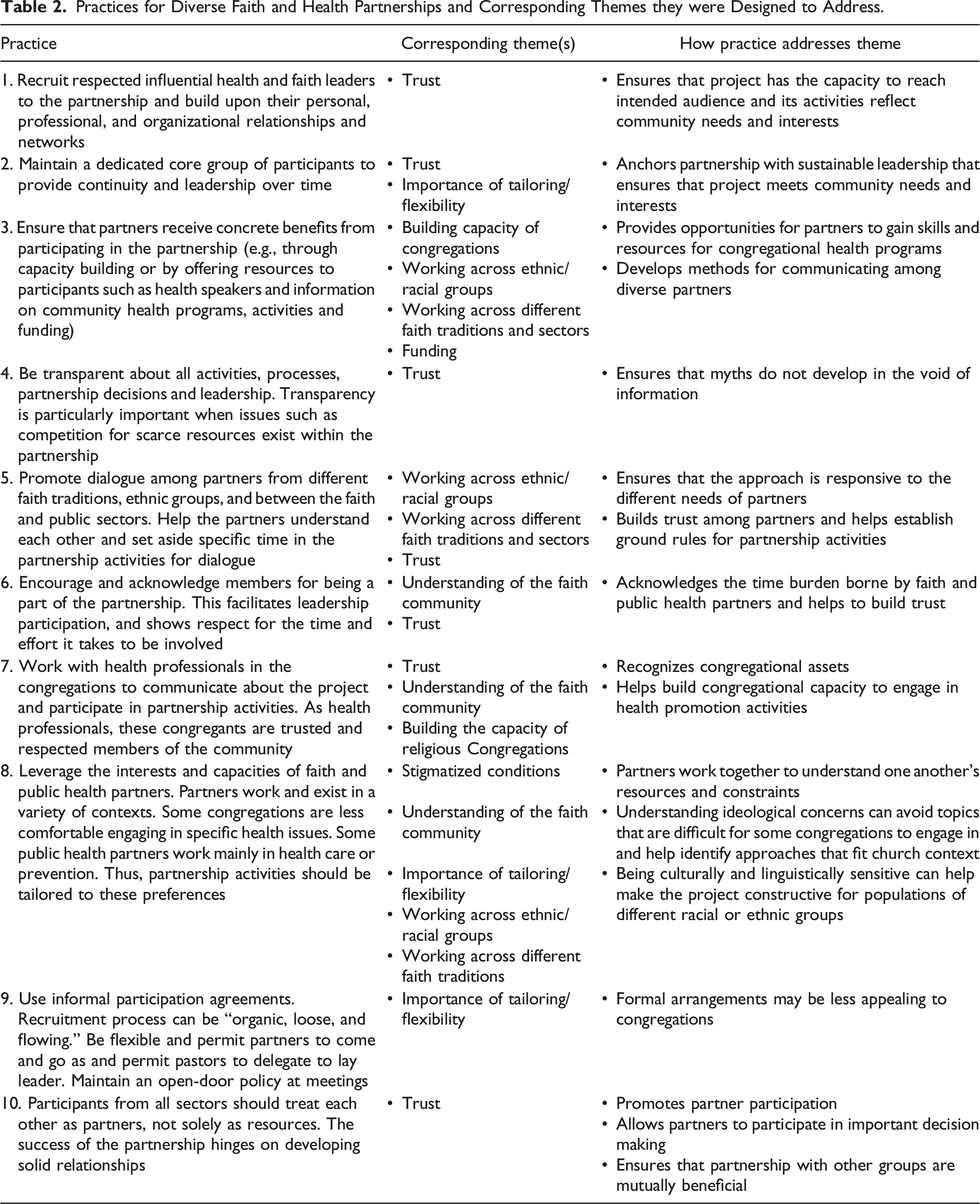
Practices for Diverse Faith and Health Partnerships and Corresponding Themes they were Designed to Address.
Discussion
The growth in multi-sectoral community health partnerships involving faith-based organizations creates an opportunity to derive lessons learned for further development of these practices. The published literature on such interventions suggests that there are common barriers and facilitators.1,3,21,22 Consistent with these studies, we found that engaging religious organizations often requires building congregational capacity to participate in health programs; or strengthening the congregation in other ways such as providing skills training to congregation members or other activities that support the long-term viability of the congregation. This not only helps to gain the buy-in of the congregation and its leaders, but it also makes it possible for the congregation to contribute to the project. Related to this is that establishing trust among partners is critical. To that end, many of the suggestions that our interviewees raised to address trust confirm those from the literature including being transparent about expectations of partners 22 and treating congregations as equal partners in the work.21,22 Respondents also identified that alignment between partners and project goals is important for sustainability of the effort, which was also found by Young and colleagues. 21
Our respondents also emphasized that although successful partnerships need pastor buy-in, partnership activities may need to be carried out by a trusted delegate. Research and public health partners must directly engage the pastor early in the project and highlight how health activities fit organizational mission, provides a benefit to the congregation and the community, and is consistent with church doctrine. However, since pastors are extremely busy, successfully working with the church often means having the pastor identify a trusted delegate to help lead the project.25–27 Identifying and engaging such leaders is also an important early step. This too requires flexibility in the expectations of partners for how to work with different congregations. In some cases, this surrogate will be a paid staff member or lay leader. While pastors will ultimately choose the lay leader, partners can help identify needed skillsets and, in some contexts, provide incentives to encourage active participation by the leader. Some of our respondents suggested that it is important to seek a health care professional to serve in this role.
Another important theme identified through our interviews was public health and research partners’ understanding the faith community. This includes understanding organizational issues such as the church calendar; being aware of the church’s experience with attaining outside funding and working with funders; and knowing whether the church prefers a more informal structure to the partnership. Although this understanding is even more complex when there are diverse faith partners, public health and research partners can address this by focusing time and effort at the beginning of the project to distill this information from potential partners, engage them in planning conversations to identify activities that are feasible, and allow each congregation to tailor the project to fit its own context.
Ideological concordance was also an important but related theme that highlighted the need to understand the church’s specific belief structure regarding health programming and is consistent with the experience of other researchers. 3 Prior research has identified that more conservative congregations are less likely to engage in health or social services at all;28–30 while congregational characteristics such as predominant race-ethnicity, size, level of staffing and engagement activities have been identified as predictors of general health activities. 31 For our current project, we had to understand how these characteristics might impact our approach and, although our Community Steering Committee provided insights at each stage of partnership development, several critical lessons learned in the interviews (detailed in Table 2) helped drive how we structured the partnership, which are highlighted in the practices.
Of note, what is less common the literature are descriptions of faith and health partnerships that involve multiple racial-ethnic groups. This kind of diversity can pose challenges to developing programs since it requires that the partnership be responsive to multiple competing needs of the congregations 1 and communications issues related to language and cultural differences. Diverse and dynamic communities such as South LA exist in many urban contexts and as such, a complex set of partners are needed to address health and social concerns. Thus, this paper adds to the broader literature on such approaches and identifies several facilitators and barriers to establishing a successful partnership in this context.
Specifically, in the LA context, African Americans congregations have a mix of formal denominational and non-denominational affiliations. Latino congregations follow national statistics that show that most Latino churchgoers are Catholic and others are affiliated with a variety of mostly Evangelical and Pentecostal congregations. And although South LA has seen over the past several decades a steady decline in its African American population (representing 27% of the population in 2017), largely due to migration to other areas, and a dramatic increase many of Latinos (68% of the population in 2017), many African Americans commute back for services and other congregation activities. 32 As a result, the perception of the community is different in the two church types with African American congregations considering South LA a historical home and Latino congregations having members that live and go to church there. The implications for the current project were that we engaged all congregations in the process for choosing the health condition and developing the intervention. This meant that we could develop an approach that was feasible across diverse contexts.
This research is limited by several factors. First, we had a relatively small sample, and, given the diversity among our participants, this may mean that we did not reach saturation on the range of public health and faith community partnership experiences especially among Latinos. However, our purposive sampling strategy (including individuals from various races-ethnicities, genders, and sectors) did enable us to explore a diverse range of perspectives, and, because we had participants from and working across the U.S. our findings may resonate with other similarly complex communities. Second, the highlighted action steps were not formally tested. Thus, we don’t have an objective method for identifying whether they help to support partnerships in an effective way. Future research should look at whether and how these activities improve partnership functioning in multiple contexts. Third, our choice to analyze notes from the interviews rather than transcripts may introduce bias related to how we chose quotes or elements of discussions to include in the analysis. Further, these data are drawn from interviews that occurred approximately 8 years ago. They may not reflect respondents’ current views or changes in the funding and social needs environments in which such partnerships might be formed today. However, public health efforts continue to be challenged by limited resources and the need to partner with FBOs to address new concerns such as disparities in COVID-19 outcomes and vaccination rates is clearly present. Thus, we consider these results relevant to the today’s challenges in addressing racial and ethnic disparities in health.
Despite these limitations, we have identified critical factors unique to multi-ethnic, multi-denominational faith and public health partnerships to address health. In this paper, we not only identified those challenges, but also worked within our own partnership to distill specific approaches we could use to facilitate a successful approach. Although in some cases the lessons learned are derived from expertise around a specific context, they are broadly applicable to the development of faith and public health partnerships. As interest in these arrangements grows across funders and other stakeholders having tangible examples of how to approach and structure these partnerships is important.
Footnotes
Acknowledgements
The Authors would like to thank the other members of the Community Steering Committee, especially Rev. Rosalynn Brooks, Rev. John Cager, Rev. Walter Contreras, Jaime Huerta, Rev. Martín García, Dr. Jan King, Rev. Felipe Martínez, Bp. Gwendolyn Stone, Nina Vaccaro, and Bp. Craig Worsham for their generous dedication of time and energy to this project. The Authors would also like to thank the LAM Faith Organizers, Rev. Jawane Hilton and Rev. Juan Sarmiento, for their dedication in recruiting partners from the faith community.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Institute of Minority Health and Health Disparities of the National Institutes of Health under grant Award Number R24MD007943. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.
Author Biographies