
Abstract
Background
Immigrants with spinal cord injury (SCI) experience challenges with co-morbidities and lack of access to medical supplies and equipment. Much of the current disability and SCI literature does not include Latinx immigrants with SCI. To address this gap in knowledge, the present study explores the intersectional impact of disability and immigration on health as well as the health status and health needs of immigrants living with SCI.
Methods
This community-partnered study is a secondary analysis of needs assessment data collected in February 2019 with 24 of the members of Living Hope Wheelchair Association, a nonprofit organization serving Latinx immigrants living with SCI in Houston, Texas.
Results
Participants shared challenges with accessing healthcare, comorbidities, mental illness, transportation, and discrimination by healthcare professionals. They also shared difficulties accessing medical supplies, medical equipment, and the need for adaptations in their homes and vehicles.
Conclusion
The findings corroborate those of previous studies with people with SCI, but highlights additional layers of marginalization and challenges faced by immigrants living with SCI. More research is needed to understand the health needs and health status of this population, including their access to care and management of chronic diseases such as diabetes and heart disease. Findings support the need for public health and immigration policies to promote inclusion and equitable access to services as well as improve the health and quality of life of immigrants.
Introduction
Despite the protections of the “Latino health paradox,” which refers to the lower mortality rates for Latinxs compared to non-Latinx whites, this paradox does not seem to apply to the category of disability. 1 While Latinxs (a gender-neutral term referring to individuals from Latin America) in the U.S. live longer, they face more health risks, disability, and stress than whites.2,3 Disability rates among Latinxs are higher than that of non-Latinxs, and foreign-born Latinx people have the highest burden of disability among all racial/ethnic groups by years of reported difficulties concerning self-care. 1 The concentration of Latinx individuals in “backbreaking” or physically demanding jobs in agriculture, construction, and domestic work is tied to workplace injuries that may result in higher rates of disability. 1 Scholars have documented injuries and disabilities that result from migrant work, particularly for farm work and food processing4,5,6 and for day laborers. 7 In Houston, as in much of the U.S. South, undocumented workers make up a large percentage of construction workers, an industry with high rates of injury, low pay, heat stress, and limited health insurance. 8
Spinal Cord Injury (SCI)
A spinal cord injury (SCI), a traumatic, life-altering injury associated with loss of mobility and sensation, results in disability. 9 There are approximately 288,000 people living with SCI in the U.S., and about 17,700 new injuries occur annually. 10 Because the spinal cord cannot recover from this type of injury, the traumatic physical and psychosocial effects of SCI last throughout the lifespan. 11 The causes of SCI vary considerably for Latinxs as compared to Whites. SCI for Latinxs is more likely to result from violence than for Whites. 10 For Latinxs, vehicular accidents (35.8%) and violence (31.5%) are the most common causes of injury, while vehicular accidents caused 47.6% of injuries for Whites and violence caused only 6.4% of injuries. 10 The average cost of care for SCI in the first year alone is approximately $523,089, 12 and research shows that only 35% of people with SCI return to work. 13 Of the 58% of people who are employed at injury, only 12% are employed 1 year after their SCI. 10
People with SCI experience a myriad of physical and mental health complications. Physical complications include pressure ulcers, which can result in hospitalizations, new or worsened disability, surgery, and fatal infections.14,15 Pressure ulcers occur in about 85% of people with SCI, and estimated annual costs of treating ulcers among people with SCI in the U.S. is between $1.2 to $1.3 billion.11,14 Preventable urinary tract infections (UTIs) and respiratory illnesses are also common causes of re-hospitalization among people with SCI. 15 People living with SCI experience multiple comorbidities, chronic pain, limited or lack of access to transportation, insurance limitations, and lack of access to medical supplies and equipment.9,16 Other need areas include lack of access to employment, education, and accessible public infrastructure (including ample disabled parking, enforcement of disabled parking laws, accessible streets, and ramps). 16 Mental illnesses, such as depression, are also common among individuals living with SCI.9,14,17 The prevalence of depression among people with SCI is 22.2% (significantly higher than the 3.2% prevalence in the general population) and this prevalence ranges from 7% to 48% in the scientific literature. 17 The prevalence of anxiety-related disorders in the general population is 7.3%, but estimated to be 27% among people with SCI. 17
Other Factors Impacting Immigrant Health
In addition to higher rates of disability, Latinx immigrants experience discrimination, violence, increased immigration enforcement and workplace raids, and family separations, all of which negatively impact their physical and mental health.18,19 Previous studies point to the ways multiple inequalities – including structural racism, discrimination, residential segregation, and immigration policy – as opposed to individual behavior and cultural factors – impact immigrant health outcomes. 20 Additional studies document stress from immigration enforcement and raids, food insecurity resulting from heightened enforcement, and how undocumented status negatively impact mental and physical health.21,22,23,24,25
Gaps in Knowledge
While significant research has been published on health and immigration and on health and disability, there is less research on the intersection of these two areas. 26 There is a growing body of research on the health and lived experiences of immigrants and refugees; as noted, some scholars have previously documented injury, illness, and disability resulting from farm work, particularly for undocumented populations.(e.g. 4,5,6,7) However, undocumented immigrants and people perceived as “illegal” face specific healthcare barriers, discrimination, and marginalization. 20 Previous studies have noted the limited public health literature on undocumented immigrants and health, as they are often excluded from public health research and disease surveillance efforts. 24 Further, much of this evolving research landscape is presented in the form of literature reviews and framework analyses(e.g. 18, 20, 24), and there are few empirical studies with undocumented immigrants providing firsthand account of their health needs and health status. Likewise, a considerable amount of the existing literature on immigrants and refugees is not focused on disability(e.g. 7, 19, 22, 23, 24, 25), is gender-specific(e.g. 6, 7, 19), focuses on the health needs of the U.S.-born children of undocumented immigrants(e.g. 25), and a few others do not explicitly sample or identify undocumented persons as participants(e.g. 6, 26). Additionally, much of the research on immigrant health has focused on behavioral and cultural frameworks which emphasize individual choice, often overlooking the impact of immigration, labor policies, and discrimination.18, 20
An understanding of the unique challenges faced by immigrants with disabilities, especially those who are undocumented and living with SCI, is useful for identifying interventions and policies to improve health outcomes and quality of life. The present study’s distinct contribution to the growing literature is its focus specifically on undocumented individuals living with SCI, its focus on the intersection between immigration and disability, the interdisciplinary background and perspectives of the researchers, and its community-engaged research process. Other scholars have noted that intersectionality, interdisciplinary perspectives, and community-engaged methods are needed in this field of study in order to enable analysis of driving factors of inequities and potential interventions. 24
The Present Study
To deepen our understanding of immigration and disability, the authors of the present study focused on the structures that create and maintain health inequities rather than on individual behaviors, bringing together trilateral disciplinary perspectives of Public Health, Anthropology, and Community Organizing. A social determinants of health approach requires examination of upstream structural factors, including jobs and wages, affordable housing, access to social services, the impact of discrimination, and other factors critical for well-being. 18 In addition to a social determinants of health framework, the authors of this study utilized the intersectional approach of Black Feminist scholars, who pointed out how multiple oppressions create “new measures of oppression and inequality.” 27,28 A social determinants of health and intersectionality approach allowed close examination of how the enduring legacy of systemic racism in the United States has resulted simultaneously occurring inequities that disproportionately affect the health and wellbeing of minoritized communities and individuals with disadvantaged social positions (e.g. race, class). These include inequities in healthcare access, economic, education, and employment opportunities. The methodological design of the present study as well as interpretation of the findings were anchored by this systemic lens. This included consideration of the combined effect of these inequities in the development of the survey instrument and the analysis of the topics discussed by participants in the open-ended questions.
The objective of the present study is to provide a unique window for understanding of the health of undocumented Latinx immigrants with disabilities through an assessment of the health needs and health status of individuals living with SCI in Houston, Texas. The following research question was used to guide the design and interpretation of findings: What is the intersectional impact of disability and immigration on the health status and health needs of Latinx immigrants living with SCI in Houston, Texas? This community-engaged study was conducted in partnership with Living Hope Wheelchair Association, and provides a case study that documents the structural factors impacting the health of immigrants with disabilities. This article, like the work of Living Hope Wheelchair Association, addresses the intersectional impact of disability and immigration on health and explores the health status and health needs of Latinx immigrants living with SCI.
Methods
Study Design
This exploratory needs assessment study was conducted in partnership with the members of Living Hope Wheelchair Association, a nonprofit organization providing medical supplies and equipment to undocumented immigrants with SCI located in Houston, Texas. The needs assessment was conducted to facilitate strategic planning, to guide fundraising, and for program development for the organization and its members. The needs assessment was conducted utilizing face-to-face, interviewer-administered surveys conducted in Spanish over several days in February of 2019.
The present study was a collaborative, community-driven effort intended to inform community programming to improve the health needs and health status of immigrants with SCI. Methodologically, community-engaged research is a useful, oftentimes necessary, process for conducting research to understand undocumented immigrants. 24 Collaborative research provides useful data for the organization, creates trust between researcher and members, and allows researchers to observe impacts of discrimination and lack of services on health. 24
Study Setting
Living Hope is a grassroots organization founded in 2005 by Spanish-speaking immigrants from Mexico and Central America with SCIs to respond to their survival needs. The organization was founded in response to a policy decision of the Harris County Hospital District to stop providing necessary medical supplies and equipment to people with disabilities who were non-Medicaid eligible.29,30 Supplies such as catheters, diapers, and sterile gloves are expensive, required daily, and a necessity for survival. For the past 17 years, Living Hope members have collected and distributed medical supplies and equipment monthly and provided transportation support with and for people with SCI. Medical supplies are distributed not only to members of the organization but also to a growing number of clients, including U.S. citizens and veterans. Its members serve as quality-of-life promoters who meet with immigrants with disabilities twice a month for peer training and support. The group’s core team of leaders, themselves immigrants with SCIs, have concrete skills in community organizing, leadership development, advocacy, and mental health support. They have created a community of mutual aid, providing emotional support to members and their families.
Though they only make up 3.3% of the U.S. population, there are more than 10 million undocumented individuals living in the U.S., and they are concentrated primarily in metropolitan areas across the country. 31 Houston is home to more than 500,000 undocumented immigrants (about 28% of Houston’s population), the third largest undocumented population in the country behind Los Angeles and New York.31,32 Mexicans made up 44% of Houston’s immigrant population, while another 13% were from Central American countries such as Guatemala, El Salvador, and Honduras, with 70% living on incomes twice below the Federal Poverty Level, and more than half reported limited to no English proficiency. 33
Houston is home to the largest medical center in the world, the Texas Medical Center, with over 10 million patient visits a year and over 100,000 employees. 34 Yet the uninsured population in Houston is the highest in the country, with about one in every five people uninsured, a total of 1.4 million people. 35 Almost 20% of Texas residents are uninsured, double the national average of 9.2%. 35 Undocumented immigrants in Texas have limited access to publicly-funded healthcare; those living in poverty can only qualify for “Emergency Medicaid,” if they have lived in the U.S. for at least 6 months. 36 Texas is one of 12 states that has refused Medicaid Expansion, which means it does not receive additional federal funds to support publicly-funded medical care. 37
Data Collection & Recruitment
Members of Living Hope (N = 24) were invited to participate in a survey to assess the health needs and health status of immigrants with SCI in February of 2019 during the program’s monthly supply and equipment distribution. The needs assessment was carried out using a convenience sampling strategy, as the participants invited were already on-site receiving services. The needs assessment inclusion criteria focused on individuals who were aged 18 and older and individuals who were active members of Living Hope Wheelchair Association at the time of the study. It excluded individuals under the age of 18 and individuals outside of Living Hope’s membership.
Each survey lasted approximately 45 min, and all participants provided verbal informed consent. Though developed in English, the needs assessment survey was translated into Spanish by Author 1 (who is fluent and literate in Spanish), as the majority of Living Hope’s membership are monolingual. The interviewer-administered survey instrument included both open-ended and closed-ended items and were administered by Author 1, a trained community health researcher and someone who had been engaged with the organization for years prior to the present study. In fact, before data collection, both researchers had sustained long-term relationships with Living Hope leadership and members, engaged in long-term participant observation, and attended events such as supply distributions, marches, membership meetings, social events hosted by the organization, press conferences, and vigils. Survey questions included demographic items (e.g. age, race/ethnicity, cause of SCI, employment status, educational attainment, income) as well as questions such as, “How would you characterize your employment prior to your injury/disability?”, “How often do you experience feelings of fear and anxiety over your immigration status?”, and “Have you ever felt discriminated against by a healthcare provider?” While study participants were not directly asked about their immigration status in the survey, most disclosed this information while participating in the survey. Furthermore, in recent years, Living Hope as an organization made the decision to speak openly about the undocumented and non-Medicaid eligible status of most of its leaders and membership in order to advocate for changes to the healthcare system and immigration policy; therefore, the immigration status of the majority of the organization’s membership and leadership was public information at the time of the study.
Data Analysis
Data for this study was collected on paper by Author 1 and soon after entered into the software PowerBase, which is used by Living Hope to store and organize data. These de-identified data were cleaned using Microsoft Excel, and descriptive data were analyzed on IBM SPSS Statistics 27.38,39 Descriptive statistics include measures of frequency, specifically counts and percentages.
Open-ended responses were reviewed and translated by Author 1, followed by analysis and a categorization of responses by overarching topic by Authors 1 and 2. For each topic, a handful of relevant quotes were selected to illustrate the needs and concerns shared by participants and provide further context to the quantitative data Review of categories overall data analysis was finalized with the feedback and final review of Author 3. The open-ended categories and participant responses provided the authors with opportunities to reflect on the interrelated nature of the participants’ multiple marginalized identities, as well as the compounding effect of systemic exclusion and discrimination.
Results
Participant Characteristics
At the time of the survey, participants had been injured between 10 months to 36 years and had been living with SCI for an average of 15 years (Mean: 14.93; Median: 13.50; SD: 10.14). The most common causes of SCI among Living Hope participants were vehicle accidents (29%) and violence (29%). SCIs caused by violence were, for the most part, the result of gunshot wounds following home invasions and robberies. Some participants reported their SCI occurring due to workplace accidents, primarily falls and mechanical accidents (25%). A smaller proportion of participants reported illnesses as the main cause of their SCI, including injuries resulting from strokes (17%).
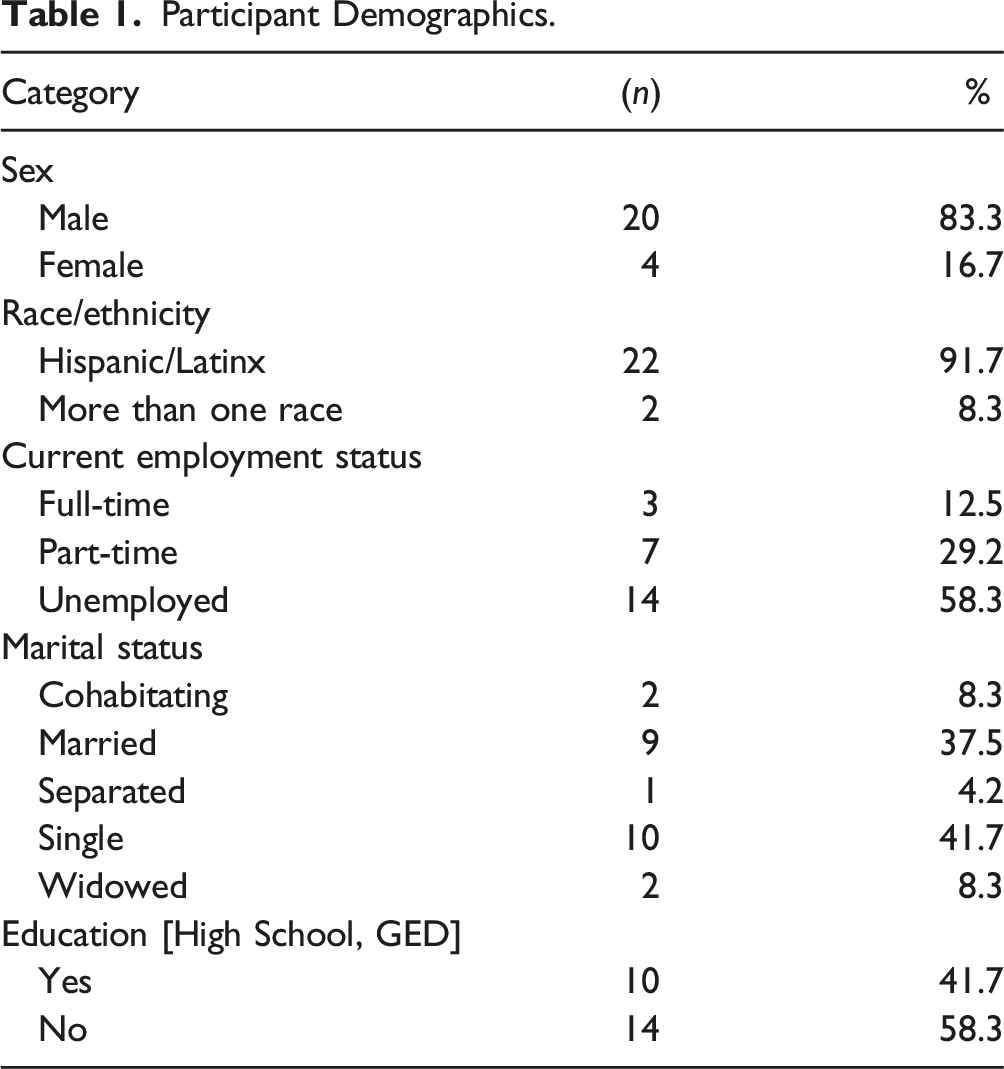
Study participants were between the ages of 28 and 76 years old, with a mean age of 49 years old and a median of 50 years old (SD: 13.56), but most were over the age of 40 (71%). The majority of participants were male (83%), and most identified as Hispanic/Latinx (96%) (Table 1). More than half had an education of less than high school or equivalent (58%). Almost half were either single (42%) or married (38%). When asked about social support, 67% reported having between 2 and 5 people that they can count on in times of trouble, difficulty, or any emergencies.
Participants reported being in the United States for decades, with only 3 (12.5%) participants stating that they have been in the U.S. for less than 10 years. At the time of the survey, Living Hope participants had been in the U.S. for an average of 23 years (Median: 21.00 years; SD: 14.91). Time in the U.S. ranged from 4 years to 75 years.
Living Hope participants shared that they were employed prior to their SCI (83%), and a majority were employed full-time (79%). Prior to their SCI, participants reported being employed in industries such as construction (33%). At the time of the assessment, more than half of participants were unemployed (58%). Several reported part-time employment (29%) and very few reported full-time employment (12.5%). Most of the individuals who reported having full or part-time employment receive a stipend for peer educator work done at Living Hope Wheelchair Association. Over half of the participants also reported an annual income below $20,000 per year (63%). Another 21% reported having no income.
Living Hope participants also reported experiencing food insecurity (63%), responding that they “always” or “sometimes” worry that food will run out before there is money to buy more. The participants of Living Hope also experience housing insecurity, with most living in low-income housing, at assisted living facilities, or with family and friends. Several participants expressed the need for housing, and shared that at the moment of the interview, they were experiencing homelessness. One participant shared that he lives in a car with a few friends. He stated, “you risk your life being out there in the street … you can get hurt.” Another participant shared, “I need a new place to stay in. I stay in a borrowed trailer with poor AC and only cold water for shower. My personal hygiene is suffering.”
Co-Morbidities
In addition to spinal cord injuries, most Living Hope participants reported living with other medical conditions (Table 2). When asked about the conditions that they were diagnosed with by a healthcare professional, many reported being overweight/obese, having high cholesterol, and suffering from mental illnesses. About half of the participants reported experiencing anxiety (46%) and depression (46%) in the past 3 months.
Bedsores (pressure ulcers), were the most commonly reported health complication among Living Hope participants (42%). Chronic urinary infections were also very common, and one participant stated that, “After so many years of chronic urinary infections, many antibiotics are not even effective on me.”
Participants also reported experiencing chronic pain (63%). Among those who experience chronic pain, 73% specified that they experience such pain daily and 82% reported taking prescription chronic pain medications for 2 years or more. Most participants expressed taking such medications since they suffered their SCI (some have been taking these for decades). Several participants shared that they would like stronger, more effective pain medication. One participant shared that he rations pain medications, and only takes the medication in instances of extreme, unbearable pain. He stated, “I need medication to help relieve pain, but I am afraid of becoming addicted.” Another participant shared, When I have pain, I hit myself. I punch my own head. I want to die. It has been about 24 h since I last felt that way …. it usually lasts about 20 min … The pain makes me scream and cry. I feel like my foot will fall off from the pain … When the pain hits, I get angry and desperate. No one but me knows what this pain is like.
Transportation
More than half of participants reported relying primarily on METROLift (54%), a public transit system in the Houston for individuals with disabilities, and 46% own a vehicle. Participants with their own vehicle often expressed the need for support in making their vehicles accessible, for gas money, and mechanic repairs. A few participants also stated that they utilize public transportation in addition to METROLift, including buses and trains (17%). Of the individuals who rely primarily on METROLift, 42% used the service 2–6 times per week and another 12.5% relied on METROLift daily. One METROLift user shared, I try to speak to the people at METROLift, and just because I don’t speak English well, they cut me off and tell me that they do not understand me without even letting speak or letting me finish what I was saying.
Another METROLift user stated, “I don’t usually pay for my chair, but two drivers will not take me if I don’t pay. I can understand them well when they talk badly about me, about Latinos, about how Trump is right to build the wall.”
Medical Supplies, Equipment, and Adaptations
The need for medical supplies, equipment, and adaptations for accessibility were among the most common challenges expressed by Living Hope participants. Though participants received most of their medical supplies and equipment from Living Hope, they expressed the need for additional supplies and equipment. These included fitted leg braces, chair backing, cushions, tires for wheelchairs, adjustable beds, exercise equipment, bathroom chairs, and equipment to support standing. The most common challenges around adaptation were bedroom and bathroom accessibility, including the need to have entryway doors widened. Living Hope participants also expressed the need for ramps for their homes, shower/bathtub repairs, and making their vehicles accessible.
Access to Medical Care
Most of the participants of Living Hope were uninsured (79%) and relied on the Harris Health Financial Assistance Program (commonly known as the Gold Card) for medical care (71%). The individuals who reported having traditional health insurance, such as Medicaid and Medicare, were American citizens or permanent residents (21%). However, such insurance coverage provided inadequate access to necessary supplies and equipment, which led them to seek additional support at Living Hope Wheelchair Association.
Participants were asked about whether they have received routine and specialized medical care in the past year. Most of the participants reported not having seen a dentist in the past 12 months (67%), an eye doctor (71%), or receiving any SCI-related physical therapy (88%). The only care that most participants reported having received in the past year was from an internist/primary care doctor (83%). One participant was hospitalized for pressure ulcers, and another 7 participants shared that they visited a urologist at least once in the past 12 months, primarily for recurring urinary tract infections (UTIs). A total of 8 participants shared either seeing a urologist in the past 12 months or having diseases of the urinary tract.
When asked about ways that healthcare access can be improved, one participant shared, “I would like appointments sooner, instead of living for weeks or months with pain.” Many of the participants also expressed being mistreated and discriminated against while trying to seek healthcare. As one participant put it, “Sometimes you go to these clinics and they don’t want to take care of you because you don’t have papers, because you weren’t born here, or because of the color of your skin.”
Experiences with Discrimination
Many of the participants shared stories of discrimination in their daily lives and while seeking medical care. Much of the discriminatory behavior was perpetrated by medical professionals within a clinical setting, oftentimes in a hospital, community clinic, or emergency department. A participant recalled one particular experience, In December, I was in the hospital and they needed to turn my body every 2–3 hours to avoid ulcers. They did not turn me all night. One nurse told me, "I have patients with insurance who need my attention.”
This participant added that the healthcare providers at this facility were rough with his body and refused to call the doctor when he asked for one. Another participant recalled, When I was hospitalized, a nurse told me, "I am not going to break my back to take you to the bathroom". I waited in my room from 7am-7pm without going to the restroom. I waited for the new nurse to come in every day for 5 days.
One participant shared an anecdote in which a physician denied him the care he asked for and didn’t believe him when he shared his symptoms and concerns. He stated, Two or 3 years ago, a doctor told me he didn’t want to give me medication through IV for an infection, which is quicker. He told me that he thought he was worse off than me and gave me pills for the infection. He told me this in Spanish.
Some individuals attempt to report and call attention to this behavior, but it sometimes backfires and worsens their situation, in some cases leading to retaliation from healthcare professionals. As one participant recalled, When I had my accident, my stomach hurt badly. I asked a nurse for a catheter, and two hours passed. My brother then asked him again. He treated me roughly, right after my surgery. My brother complained to his supervisor and then none of the other nurses wanted to help me either.
Discussion
The intersection of immigration status, ethnicity, and disability mutually impact health outcomes. Though there is scant data about immigrants with SCI, some of the experiences shared by the members of Living Hope align with the existing SCI literature. The participants of this study, who are primarily undocumented Latinx immigrants, are living through the long-term physical and psychosocial outcomes associated with SCI outlined in previous studies, in addition to the challenges associated with immigration status. 11
The experiences of Living Hope Wheelchair Association members align with some of the experiences of people living with SCI in the general population, with a majority of members identifying as males who suffered their injury in their young adulthood and vehicle accidents making up the highest proportion of SCI causes. 10 Living Hope members, however, had an equal proportion of SCI cases caused by violence and workplace accidents were the third common cause of SCI among Living Hope members, resulting from employment in physically demanding industries (e.g. construction) that have been previously associated with high rates of injury. 8
Although the members of Living Hope were living in poverty prior to their injuries, they have sunk deeper into poverty since their injury due to being unable to work, worsening health, and their lack of access to healthcare. Though a majority of participants had not seen a dentist, eye doctor, or received physical therapy in the past year, many had seen a primary care doctor, surgeons, and urologists for repeated UTIs, which have been described in previous studies as a common complication among people with SCI. 15
As reported in studies about immigrants and health, the participants reported housing insecurity, homelessness, and food insecurity, conditions which directly impact physical and mental health.21,22,23,24,25 Participants also reported incomes below the poverty line as well as unemployment, low wages, and limited employment, which further exacerbate homelessness, housing insecurity, and food insecurity.16,21 As reported by other researchers studying the broader population with SCI, only a few of the members of Living Hope reported a source of income, while most reported being unemployed.10,13
Living Hope participants reported challenges with transportation, a need for adaptations, medical supplies, and necessary equipment to increase independence and prevent infection, which are barriers that have been reported in previous studies.9,16 More than half of participants reported reliance on Houston’s public transit system for individuals with disabilities, but such a system was often inaccessible for them due to cost. Cost is also a concern for individuals with personal vehicles, as these needed adaptations, gas, and mechanical repairs. Though most participants received medical supplies and equipment from Living Hope, there were additional and costly items they still needed, such as leg braces, wheelchair tires, exercise equipment, bathroom chairs, and cushions. Adaptations to improve door access, bathroom access, and entryway access in their homes were also mentioned as needs.
Participant Demographics.
Medical Conditions Diagnosed by a Healthcare Provider.
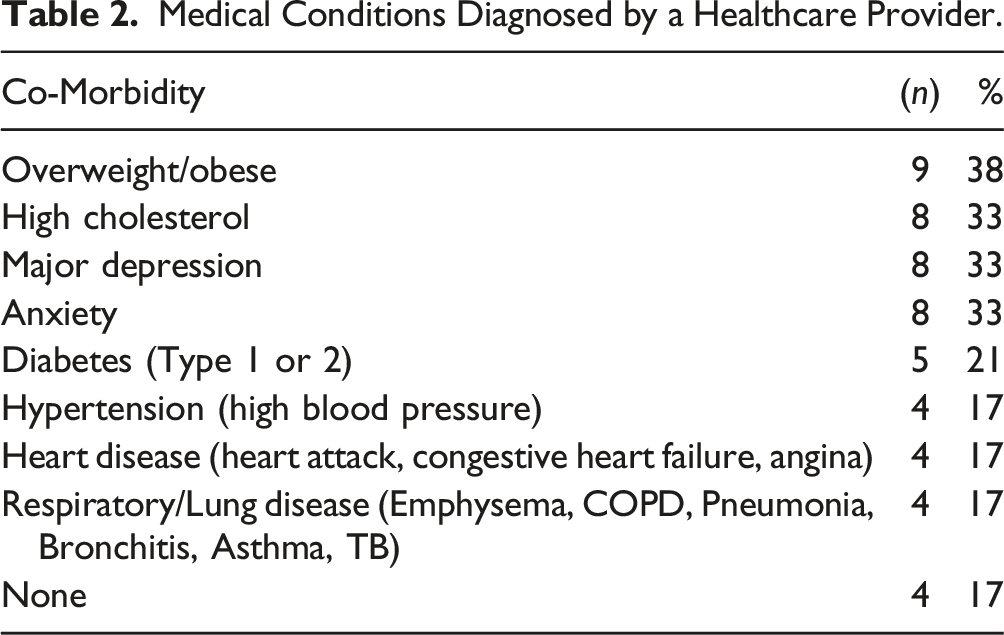
The high rates of mental illness among Living Hope participants may result from their intersectional location as Latinx immigrants with disability. Almost half of participants reported being diagnosed with anxiety and depression. Previous studies have reported high rates of mental illnesses such as depression and anxiety among people with SCI,9,11,14,17 yet this population experiences discrimination based on ethnicity as well as stress and anxiety due to their lack of legal status.
Interviews with Living Hope members revealed multiple examples of discrimination that resulted in poor care and result in additional health complications. Participants shared having been denied care due to immigration status and being uninsured. This behavior, which often goes unreported due to fears around retaliation and fears of deportation, can result in further health complications, delays, and poor health outcomes among people with high need and limited access to healthcare. Participants also reported being denied help to use the restroom (which can cause or worsen UTIs), and another shared that he was not turned for extended periods of time (which can cause pressure ulcers). The discrimination faced by participant not only discourages accessing lifesaving healthcare, but it erodes trust between immigrants and disability and healthcare professionals. Additionally, these discriminatory behaviors have serious and potentially life-threatening consequences on the already fragile health of immigrants with disability. Previous studies have connected discrimination based on race/ethnicity to poor mental health outcomes. 19 Discrimination in health care, in addition to a lack of access to care, requires additional attention.
A key issue not only for access to health care and for health and well-being more broadly is the definitions of who is defined as “deserving” or “unworthy.” Immigrants, particularly individuals who are undocumented, are often labeled as “undeserving.”18,40,41,36 Scholars in the past have observed that state criteria about who is considered a full person or citizen impacts who is defined as being worthy of healthcare. 36 For example, in the Rio Grande Valley of Texas, undocumented patients with end-stage renal disease (ESRD) could only receive dialysis under emergency situations, a policy with severe health consequences. 36 Indeed, one member of Living Hope with ESRD was not eligible for regularly scheduled dialysis and died in 2019 following 2 years of only receiving emergency dialysis without health insurance. 42 The discrimination reported by Living Hope members in healthcare settings points to the ways their bodies are marked as being undeserving and their lack of treatment or poor quality of care results in prolonged suffering, further disability and injury, and premature mortality.
Limitations
This study is limited in its generalizability, and the results may therefore not be applicable to other geographic settings, organizations, and groups. The data collected in the needs assessment survey was cross-sectional, self-reported, and from a small sample size. Self-reported and cross-sectional data are known to have biases such as social desirability bias and recall bias. The snapshot, point-in-time nature of cross-sectional data does not provide information about causation and oftentimes lacks representativeness. This study’s exclusion of individuals with SCI who are not members of Living Hope may also be a limitation, as the excluded individuals may have different needs and be disconnected from care and community.
Because many SCI studies also do not sample immigrants or undocumented persons, there is a notable dearth of research about the needs of immigrants with disabilities, and this study provides meaningful insight for community programs, policy makers, and clinicians. It provides a foundation for future research to further understand the experiences of and explore the needs of immigrants with disabilities.
Conclusion
To the best of our knowledge, this study is among a few conducted with undocumented Latinx immigrants with SCI in the U.S. The study points to the multiple and overlapping factors including legal status, discrimination, and disability that impact immigrant health for this population. Systemic changes to promote access to transportation, food, housing, mental and physical health care, among other factors are needed to advance health equity and improve health outcomes. It also suggests the utility of community-based research to foster understanding of immigrant health as well as the need to further explore immigrant-based initiatives in support of their own health. Further study is needed to document and assess the impact of public health policies that exclude marginalized groups such as undocumented immigrants from access healthcare and other public resources. Future studies are also needed to explore evidence-based interventions and health promotion programs for undocumented Latinx with SCI in order to determine what results in the best health outcomes for this community. The structural barriers at the root of the inequities faced by undocumented immigrants with SCI must be addressed in community health promotion programming, public health intervention, and public policy in order to improve their health outcomes and quality of life.
Footnotes
Acknowledgements
We are tremendously thankful to the members of the Living Hope Wheelchair Association who participated in the study and shared their time and insight; special thanks to Lionel Santibáñez for his editorial assistance.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Albert Schweitzer Fellowship-Houston/Galveston and the Health Policy Research Scholars (HPRS), a leadership development program of the Robert Wood Johnson Foundation (RWJF).
Anonymized Text
The present study was approved by the Institutional Review Boards (IRBs) of the University of Texas Health Science Center at Houston (UTHealth) School of Public Health and the University of Houston-Clear Lake. This study was also authorized and approved by the board and leadership team of Living Hope.