
Abstract
This interdisciplinary scoping review addresses the involvement of spoken and signed language interpreters in statutory mental health assessments. Specifically, this inquiry seeks to identify and review pre-existing literature concerning the barriers to and facilitators of effective practice in interpreter-mediated statutory mental health assessments, and the extent to which interpreter mediation supports or impedes a person’s legal rights and best interests in this context. An interdisciplinary team applied the revised Joanna Briggs Institute scoping review framework to review 44 items, including empirical and grey literature covering relevant aspects of the available body of knowledge across the fields of social work, mental health, and interpreting studies. The review concludes that there is a lack of direct evidence on interpreting practice in the context of statutory mental health assessments, which is significant considering the high-stakes scenarios that may lead to the deprivation of liberty. The findings suggest that there is insufficient evidence regarding necessary modifications to standard interpreting practices for such assessments, as well as how assessors should adapt their own practice in response to the need for interpreting. This work highlights the need for more focused research on good practices for interpreting within this context and calls for guidance to facilitate effective interprofessional collaboration between interpreters and other professionals engaged in these assessments.
1. Introduction
This article concerns statutory mental health assessments potentially leading to involuntary detention in a psychiatric facility, whether for further assessment and/or mental health treatment. In England and Wales, the statutory instrument governing this is the Mental Health Act 1983 (henceforth MHA), and similar legislation is present worldwide (Fistein et al., 2009). Specifically, the focus of this work is on understanding the practice of assessments in circumstances where an interpreter is required. We present the results of an international and interdisciplinary scoping review that sought to identify and examine pre-existing literature concerning the barriers to and facilitators of effective practice in interpreter-mediated statutory mental health assessments or Mental Health Act Assessments (henceforth MHAAs). We also explore the extent to which interpreter mediation supports or impedes the legal rights and best interests of those being assessed within this context. 1 It is important to note that statutory assessments related to mental capacity, as opposed to mental illness, are outside the scope of this work.
2. Background
2.1 Topic and significance
MHAAs that may lead to involuntary detention and treatment differ significantly from those conducted within a clinical diagnostic process or during ongoing treatment and therapy. In the latter scenarios, there is a substantial body of existing literature in the field of interpreting and translation (e.g., Boyles & Talbot, 2017; Costa, 2022; Rolland et al., 2021). MHAAs are distinct in that they usually occur in emergency or urgent circumstances where all parties are unlikely to have a pre-existing working relationship which shapes dynamics.
In addition, the assessment process is explicitly bound by Mental Health legislation and holds significant authority. Its powers can, for instance, supersede an individual’s rights under Human Rights legislation. MHAAs require the cooperation of several doctors and non-medical professionals at a time when an individual is experiencing a serious mental health episode that may even potentially pose a risk to themselves or others. These are high-stakes circumstances in which an individual’s communication, language, behaviour, and understanding are likely to be altered and/or impaired because of their mental state. As a result, the performance of interpreters, their collaboration with other professionals, and the impact of interpreter mediation on the outcomes for the individual undergoing assessment emerge as significant areas of concern. This concern is the subject of Interpreters for Mental Health Act Assessments (INForMHAA; see Young et al., 2023), a project investigating professional practice and outcomes in interpreter-mediated assessments in the context of the Mental Health Act (MHA, 1983). The scoping review presented here serves as a precursor to this study. INForMHAA particularly focuses on how Approved Mental Health Professionals (AMHPs) jointly work with interpreters when conducting assessments under the MHA. Even though the AMHP role is open to mental health nurses, occupational therapists, and psychologists, 95% of AMHPs are qualified social workers (Skills for Care, 2024). Their role is distinct from that of the (usually) two doctors responsible for undertaking a medical recommendation. Instead, the AMHP is responsible for undertaking an assessment based on all the circumstances including an interview. The AMHP must consider all the relevant factors surrounding a person’s context, such as their family circumstances and social relationships, to determine whether detention is necessary.
The AMHP role is predicated on effective interpersonal communication with the assessed person to discern their views and understanding of what is happening to them. For this reason, a specific clause was added in statutory guidance, requiring that the interview conducted as part of the assessment be conducted “in a suitable manner” Section 13 [2] MHA, 1983. In fact, statutory guidance that accompanies the MHA explicitly highlights the need to ensure appropriate communication for groups who might have difficulties in communicating effectively (Department of Health, 2015, paragraphs 4.4, p. 36). The guidance recognises that factors hindering effective communication include language differences, challenges comprehending technical terminology or sustaining attention, hearing or visual impairments, difficulties in literacy or numeracy, learning disabilities, as well as cultural differences. In the case of language differences, the guidance states that “every effort should be made to identify an interpreter who is appropriate to the patient” (Department of Health, 2015). This provision was originally inserted to safeguard the rights of individuals whose first language may not be English and to prevent the possibility of unlawful detention based on ineffective communication (Jones, 1991, p. 48).
Despite this emphasis on meeting communication needs, there is no requirement to systematically report the language used in a MHAA, in contrast to the recording of gender and ethnicity. In addition, there is no evidence gathered as part of the UK minimum data set used to analyse the outcomes of MHAAs (NHS Digital, 2022b) indicating whether an interpreter was involved in an assessment. At the moment, there is uncertainty about how the presence of an interpreter may affect the process and outcome of an MHAA. This uncertainty is particularly concerning given that those from ethnic minority communities are far more likely to be subject to compulsory powers under the Act, whether in hospital or in the community (UK Government, 2018). Although the majority of individuals from diverse ethnic backgrounds would not necessarily use languages other than English in an MHAA, it is important to acknowledge that there are some who may, particularly among new arrivals as well as refugees and asylum seekers (Migration Observatory at Oxford University, 2019). According to the UK Office of National Statistics (ONS, 2022) census data for England and Wales, “8.9% (5.1 million people) did not report English as their main language.” Within this group, “43.9% (2.3 million) could speak English very well,” “35.8% (1.8 million) could speak English well,” “17.1% (880,000) could not speak English well,” and “3.1% (161,000) could not speak English at all.” Given that in 2020–2021, there were over 53,000 detentions under the MHA in England and Wales (Statista, 2023) and considering the diverse language abilities within this population, it seems reasonable to assume that a number of MHAAs may require the assistance of an interpreter.
In MHAAs, as is the case in other forms of psychological assessments, effective communication serves as a key tool for gaining insights into the individual’s mental state, identifying potential underlying factors contributing to their distress and symptoms, and interpreting the significance of their behaviour (Weber et al., 2022). This involves actively considering the language used by the individual and how it may be affected by, or linked to, the individual’s mental health condition (Cambridge et al., 2012). Furthermore, developing a meaningful relational understanding between the mental health professional and the person being evaluated is key to enable a comprehensive understanding of the person’s mental state (Rodríguez-Vicente, 2021). This not only facilitates a meaningful assessment but also ensures that the person feels heard, understood, and supported throughout the process, which ultimately contributes to more effective communication, a key factor in achieving equitable outcomes (Tribe & Thompson, 2022). Studies on mental health interpreting outside the specific context of MHAAs have shown that when communication in a person’s preferred language is not facilitated, it can result in a distorted or incomplete understanding of their mental state (Casas et al., 2012). In addition, an extensive body of literature on interpreter-mediated encounters across health and social care settings highlights the critical role of collaborative working dynamics between service providers and interpreters in ensuring effective communication (Geiling et al., 2021). Nevertheless, although collaborative working dynamics are promoted as a fundamental principle, their implementation may vary depending on the specific needs and characteristics of each setting (Hsieh et al., 2013).
2.2 Approach: Why a scoping review?
In seeking to assemble and review existing evidence concerning interpreter-mediated MHAAs as a precursor to the wider INforMHAA study, there were three considerations. First, the topic constitutes a specialised field within the broader discipline of public service interpreting distinct from more established domains of mental health interpreting, such as psychological therapy. Nonetheless, some of the literature concerning interpreter practice in mental health assessments more generally may be of relevance even if not formally linked to this specific context. Thus, the boundaries of the field under study and review are not strictly clear-cut. Second, practice knowledge may not be confined solely to formal literatures, with empirical studies on this specific topic likely to be rare; consequently, a broad and inclusive approach was deemed necessary to identify and consider a potentially fragmented body of work. Third, the study for which the review was a precursor was firmly associated with practice under one specific legislation, the MHA, and in one geographical context (England and Wales). Yet, valuable insights, evidence sources, and potentially best practices were anticipated from an international context where similar legislation and practices exist. Given these considerations, a scoping review was chosen as the most appropriate approach to address the questions outlined in Section 3.1.
Scoping reviews have gained increasing prominence as a robust evidence-based methodology within various literature domains, particularly in the fields of medicine, health care, and social work/social care practice (Bradbury-Jones et al., 2022). They find their most valuable application in situations where the existing research literature is limited, rendering systematic reviews less insightful, and where professional practice knowledge exists but may be more commonly found outside of the empirically driven literatures (Grant & Booth, 2009). The approach adopted in scoping reviews stands in contrast to systematic reviewing and meta-analyses, which primarily focus on assessing the quality and depth of existing research evidence, as illustrated in the interpreting field in the works of Brisset et al. (2013), Krystallidou et al. (2020), and Theys et al. (2020). In contrast, a scoping review aims to gather a wide range of available knowledge, including grey and informal literature, often addressing questions related to professional uncertainty (Arksey and O’Malley, 2005). Considering all these factors, the incorporation of a scoping review into the field of interpreting studies is anticipated to make a contribution by mapping information from diverse sources across various domains pertaining to the under-researched area of statutory mental health assessments.
3. Method
The review method followed the revised scoping review framework, as presented by the Joanna Briggs Institute (Peters et al., 2020), which consists of “title and review questions, inclusion criteria, participants, concept, context, types of evidence sources, search strategy, evidence screening and selection, data extraction, data analysis and presentation of results.” This framework builds upon the works of Arksey and O’Malley (2005) and Levac et al. (2010) and adheres to the PRISMA-ScR reporting guidelines (Tricco et al., 2018). The scoping review protocol has been pre-registered on the international platform INPLASY under the reference number INPLASY20220086.
3.1 Defining the research questions
The Population Interest Context (PICo) approach (Richardson et al., 1995) guided the formulation of the research questions (Table 1).
PICo Process for Formulation of Research Questions.
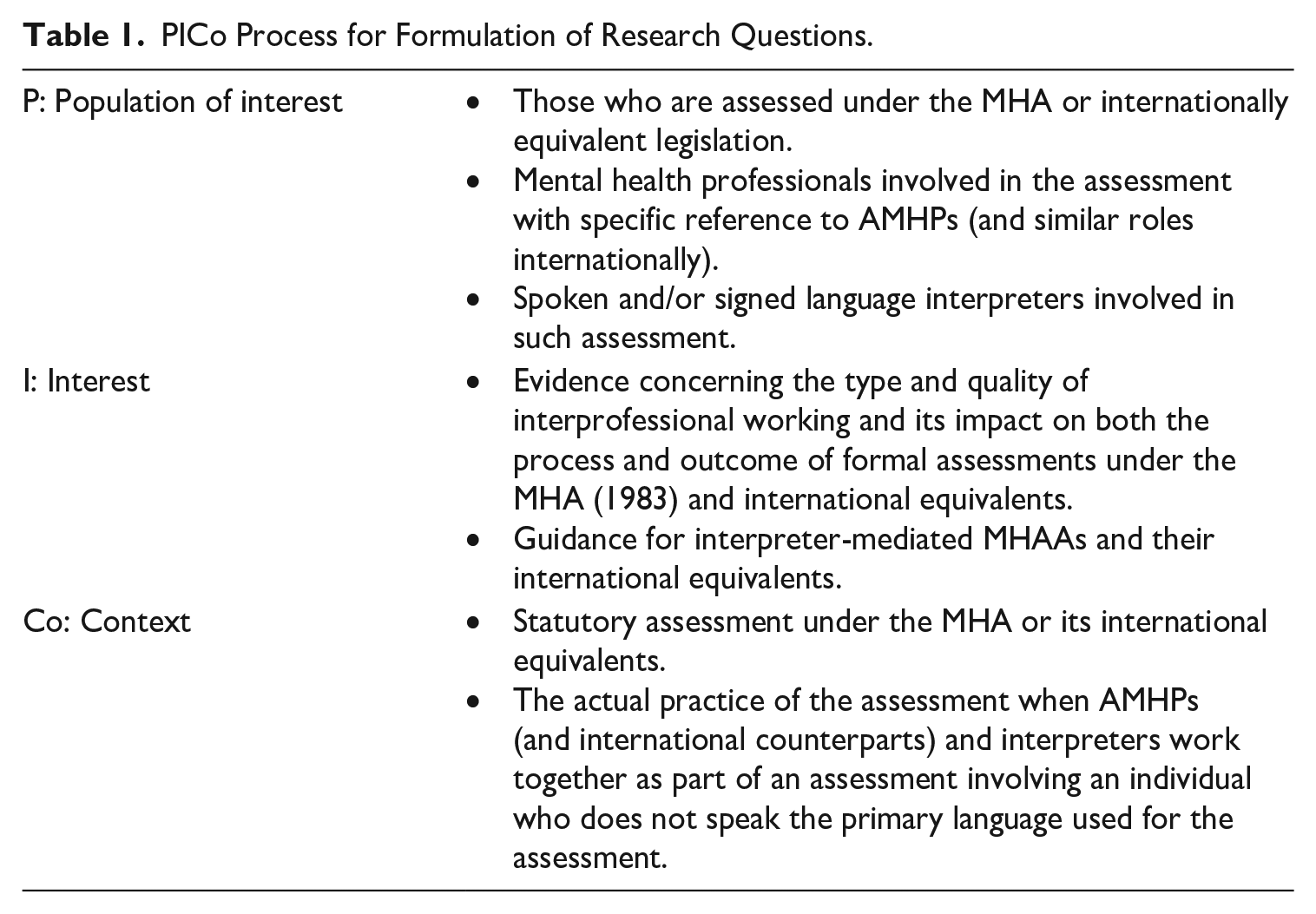
In the specified context of interest, namely, the professional practice involving AMHPs (and their international equivalents) and interpreters within the non-medical interview, and components of the MHA assessment (and its international equivalents), the guiding research questions of the scoping review are:
Research Question 1. What are the enablers and barriers to good practice in interpreter-mediated MHA (1983) assessments (and their international equivalents)?
Research Question 2. To what extent and how might interpreter mediation support or impede the legal rights and best interests of those assessed under the MHA (1983) (or its international equivalents)?
3.2 Definition of terms for the purposes of scoping review
To conduct the scoping review effectively, it was crucial to establish precise definitions for the key terms used in the literature search. The term “MHA (1983)” refers to the formal legislation in England and Wales governing the compulsory assessment, treatment, and potential detention of individuals experiencing mental illness, either for their own safety or for the protection of others. This legislation undergoes periodic review, as demonstrated by the release of a “draft Mental Health Bill” in June 2022 (HC/HL, 2023), outlining proposed reforms to the existing MHA. However, none of the recommendations made by the Joint Consultative Committee have been accepted by the current government (Department of Health and Social Care, 2024) and any reform remains on hold.
“International equivalents” refer to parallel pieces of legislation for the same purpose and with the same or similar powers that exist in other countries, although the exact details of the provisions contained within them may not be identical (Fistein et al., 2009).
“Translation” is understood in this study as a superordinate term used to refer to the process of conveying meaning across languages (Baker, 2011). In this article, we refer to interpreting a “a form of translation in which the source-language text is presented only once and thus cannot be reviewed or replayed, and the target-language text is produced under time pressure” (Pöchhacker, 2004, p. 10: citing Otto Kade); and this definition applies for working between spoken and signed texts. This differs from how translation is typically perceived as a text-based event which is not produced in real time and can be edited. Despite this distinction in the translation and interpreting literature, the word “translator” is commonly and incorrectly used in the fields of health and social care to refer to interpreters working in live-mediated events, so we have considered the use of both terms in this review.
In addition, in this review, our focus is on the role of professional interpreters. This excludes bilingual individuals who interpret or mediate informally without formal training, on an ad hoc basis, and/or without remuneration for their interpreting services (Napier, 2021).
3.3 Search criteria
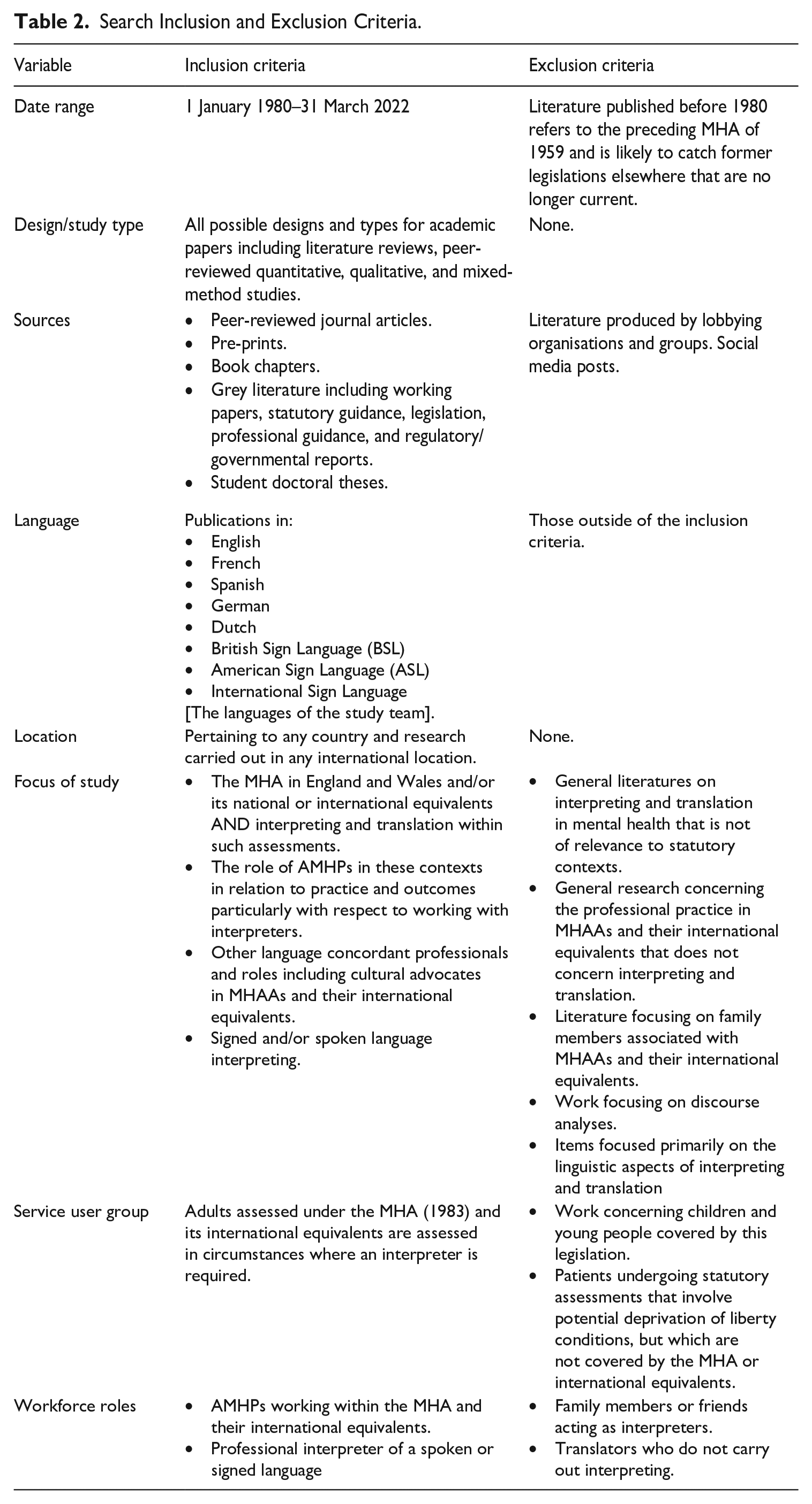
For inclusion/exclusion criteria applied to the initial search of the literature see Table 2.
Search Inclusion and Exclusion Criteria.
3.4 Search terms and strategy
We entered keyword synonyms using database thesauri (MeSH entry terms in PubMed) and search terms with database-appropriate syntax, parentheses, Boolean operators AND/OR for search strings, and field codes were specified. We also incorporated equivalents of these terms in the languages specified in our inclusion criteria. The key concepts and synonyms are listed in Table 3; search terms and the Boolean operators used in Table 4.
Concepts and Descriptors.

Search Terms with Database-Appropriate Syntax, Parentheses, Boolean Operators, and Field Codes.

The databases searched were: PubMed, ASSIA (Applied Social Sciences Index and Abstracts), PsycINFO (American Psychological Association), Web of Science (Clarivate), CINAHL (Cumulative Index to Nursing and Allied Health Literature), Social Care Online, and EThOS. In addition, we searched the online indices of 26 journals where publications on this topic were likely to be placed across the disciplines of social work, allied health professions, translation and interpreting and sign language/deaf studies as well as subject-specific publisher websites using key terms so that we could capture book chapters (see Appendix 1 in Supplemental Material alongside this article for a full list). A targeted search focused on grey literature was largely based on the research team’s own professional knowledge encompassing NHS Digital, NHS England, the Care Quality Commission, legislation and statutory guidance in mental health, professional resources, and publications for public sector spoken language interpreters and signed language interpreters.
3.5 Identification and selection of relevant studies
The online systematic review software Covidence facilitated the importation and screening of citations. The selection process involved two stages: (1) initial screening of titles and abstracts conducted by three reviewers (AY, JN, SV). Items categorised as “maybe” or where reviewer disagreement occurred underwent discussion to achieve consensus (“yes” or “no”); (2) full-text screening performed by reviewers (AY, RT), with a third reviewer (NRV) acting independently to resolve any “maybe” items or conflicts requiring further discussion for consensus. Screening at both stages required the involvement of a team member with expertise in interpreting and another member with a background in social work specialised in mental health. Their professional and academic judgement was crucial in ensuring that the selected literature was relevant to the questions guiding the review even if not directly addressing statutory mental health assessment. It also allowed for the inclusion of work that addressed the statutory context from the perspective of mental health professionals, where interpreting/translation was highly pertinent but may have been overlooked. The emphasis on identifying “silences” within existing research was crucial when selecting studies. A scoping review, aimed at mapping out areas with limited pre-existing work, offers the flexibility to adopt this approach, which may not be feasible in a systematic review.
Exclusion criteria were documented at each stage of the study selection process. After duplicates were removed, 279 items were identified at stage one screening; 131 were excluded and 148 progressed to full-text screening; 104 studies were excluded at this point leaving 44 items which were retained for review (Figure 1).
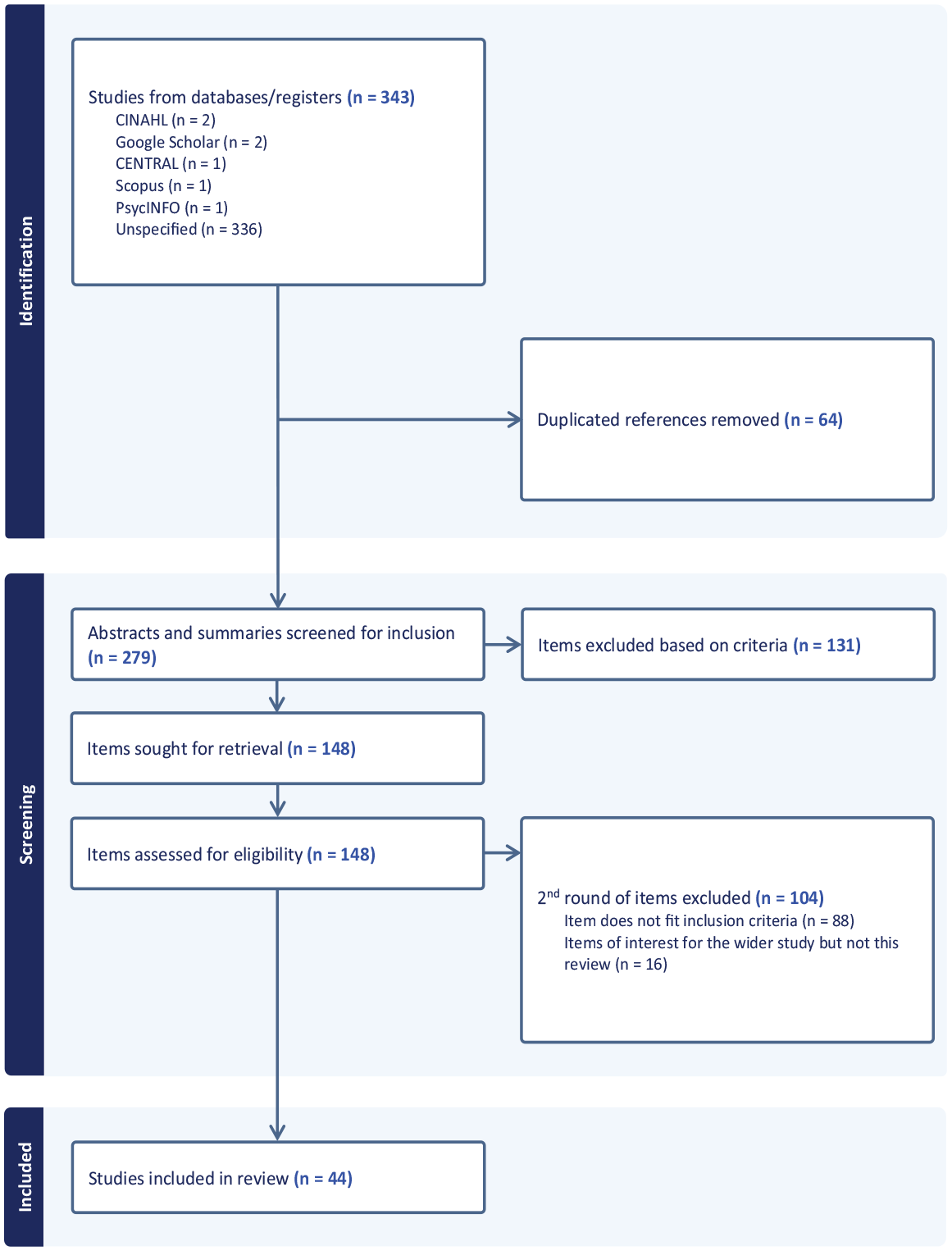
Prisma ScR Flowchart of Results.
3.6 Charting and tabulation
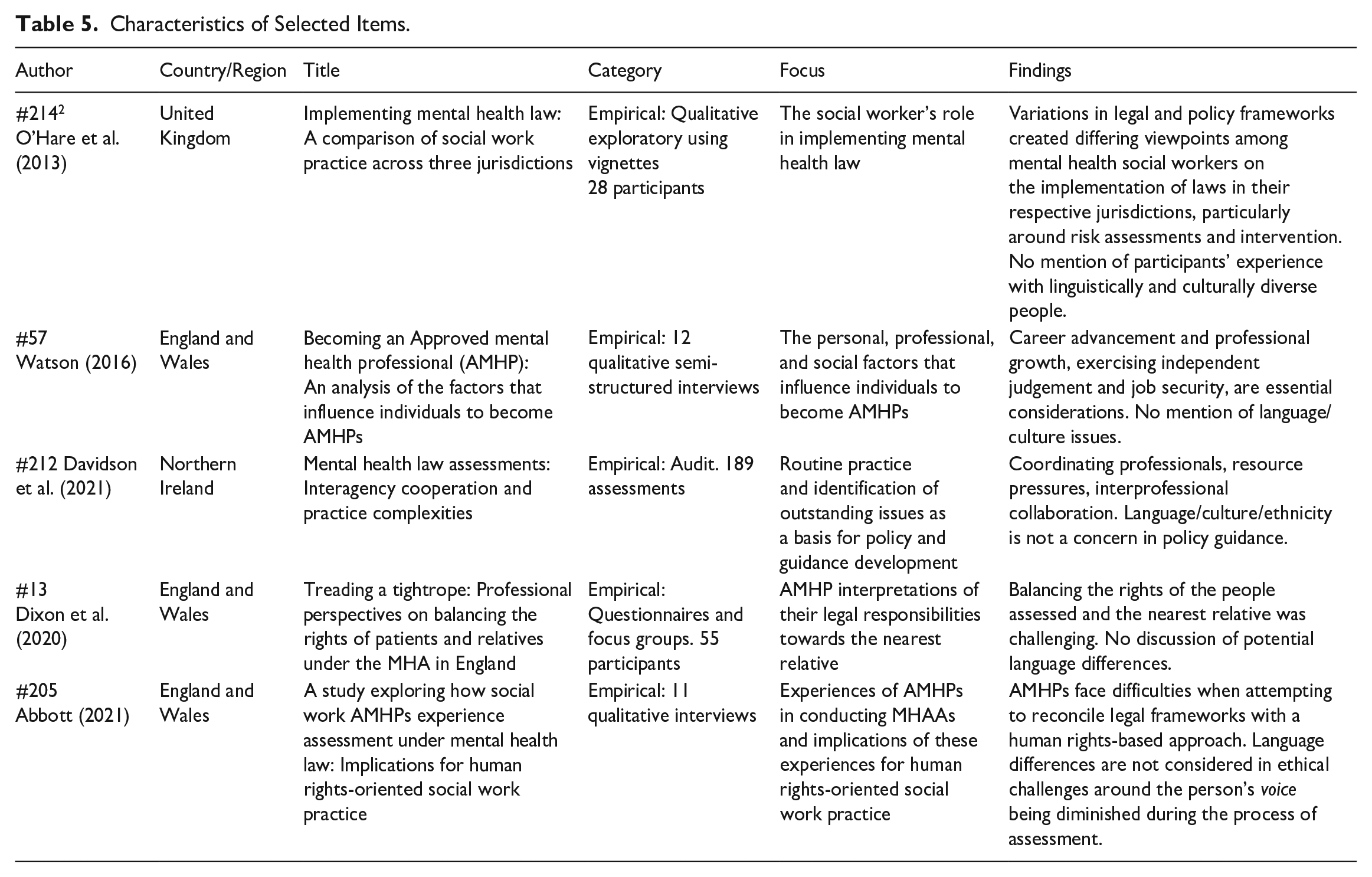
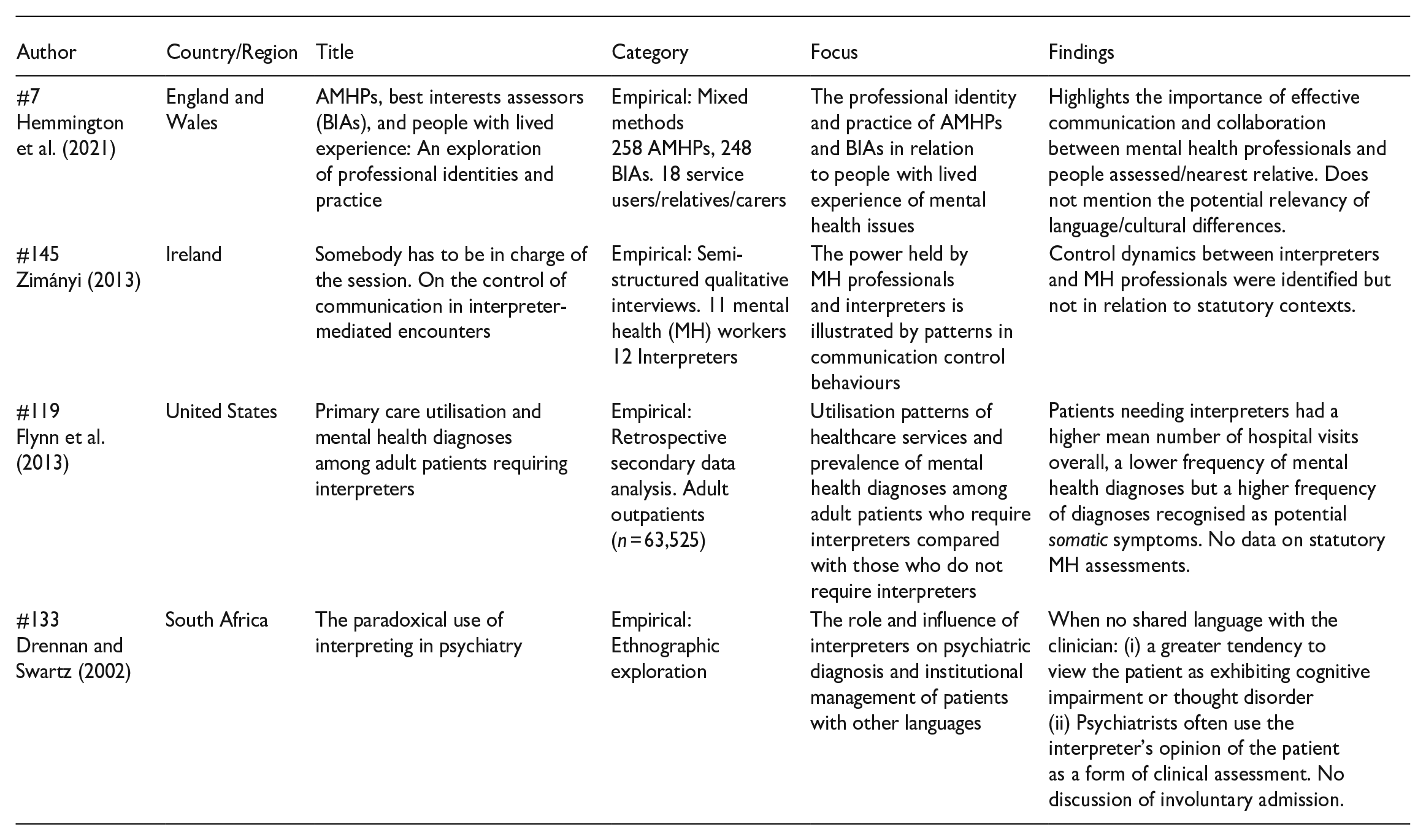
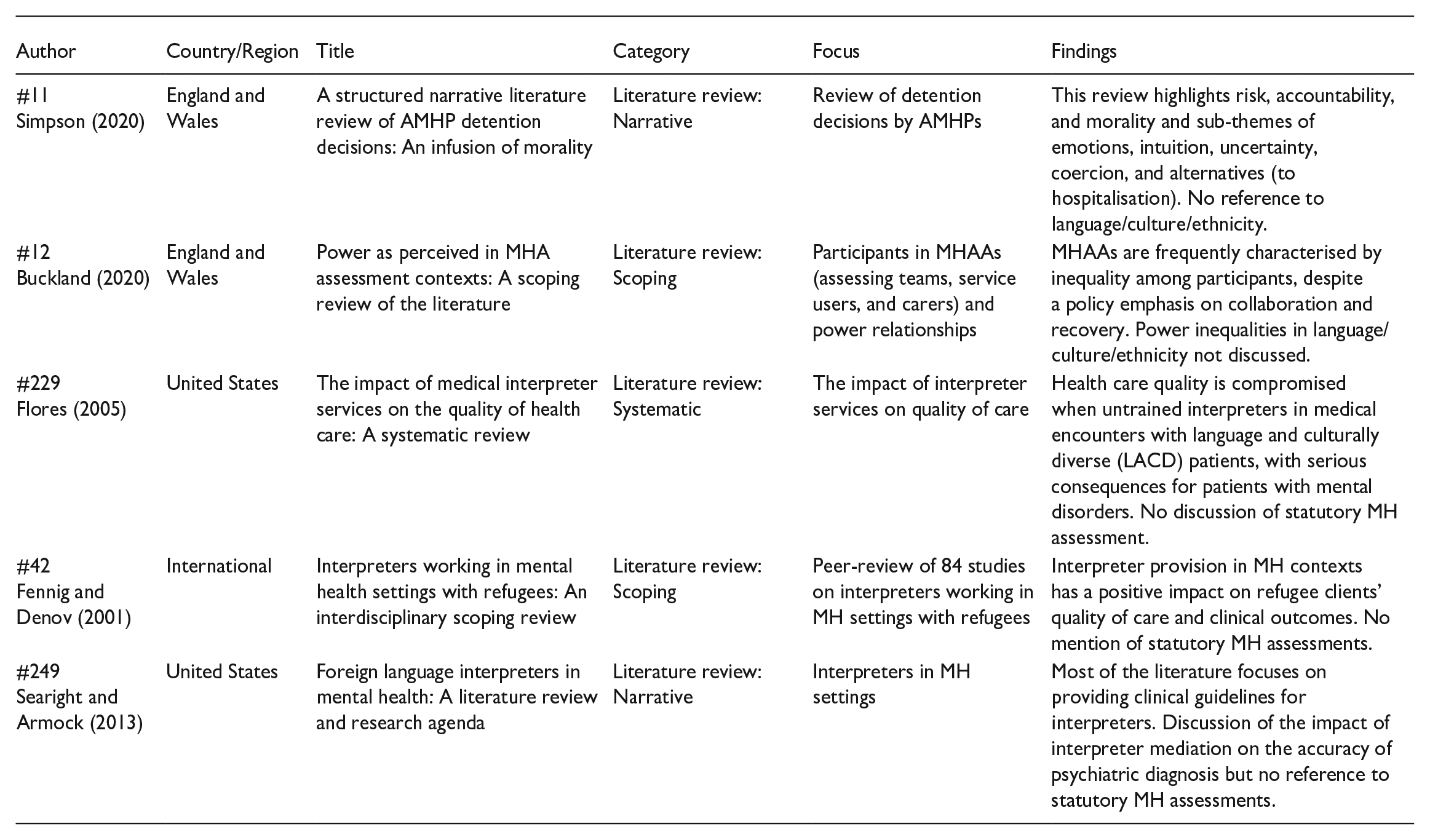
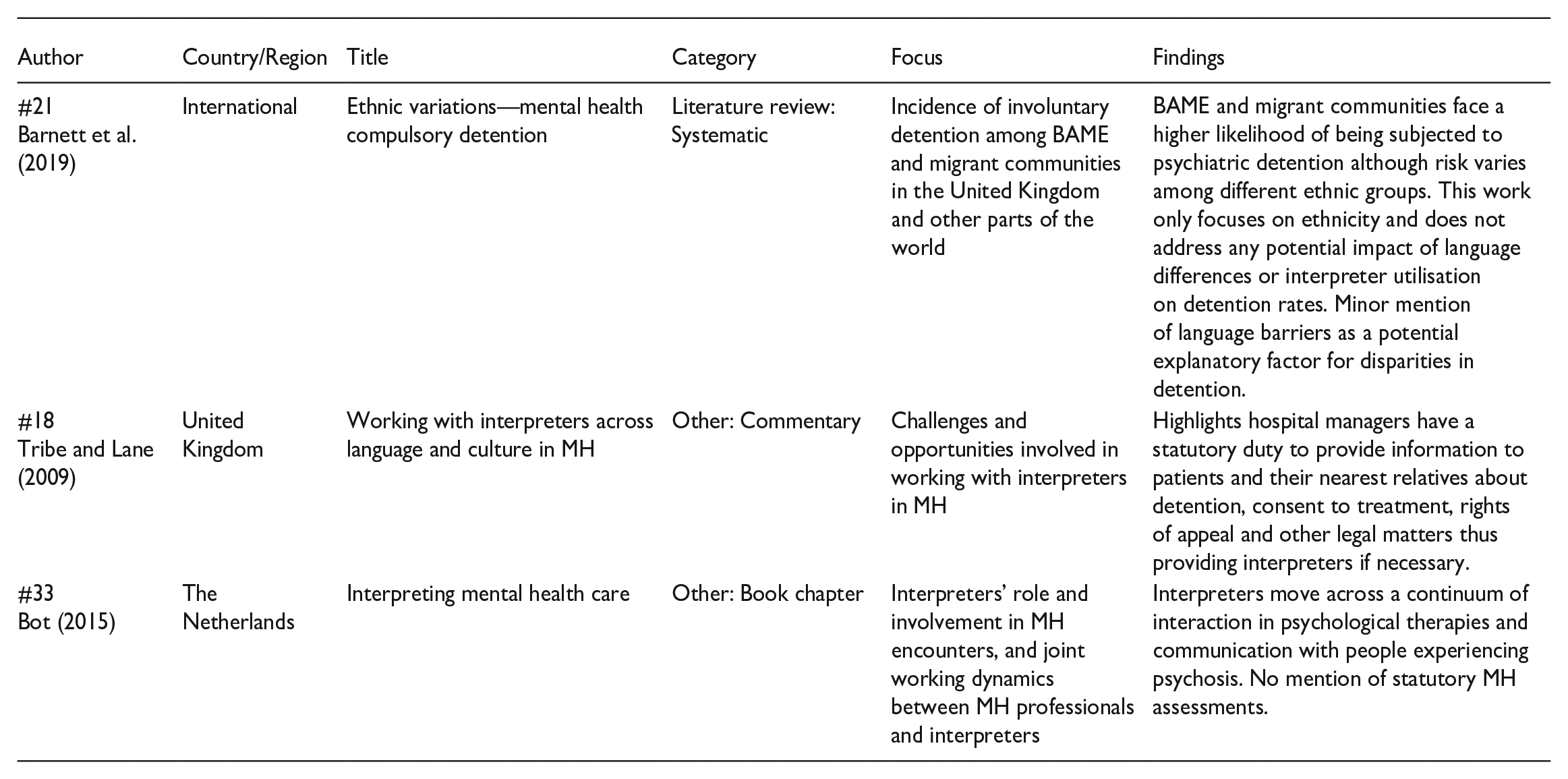
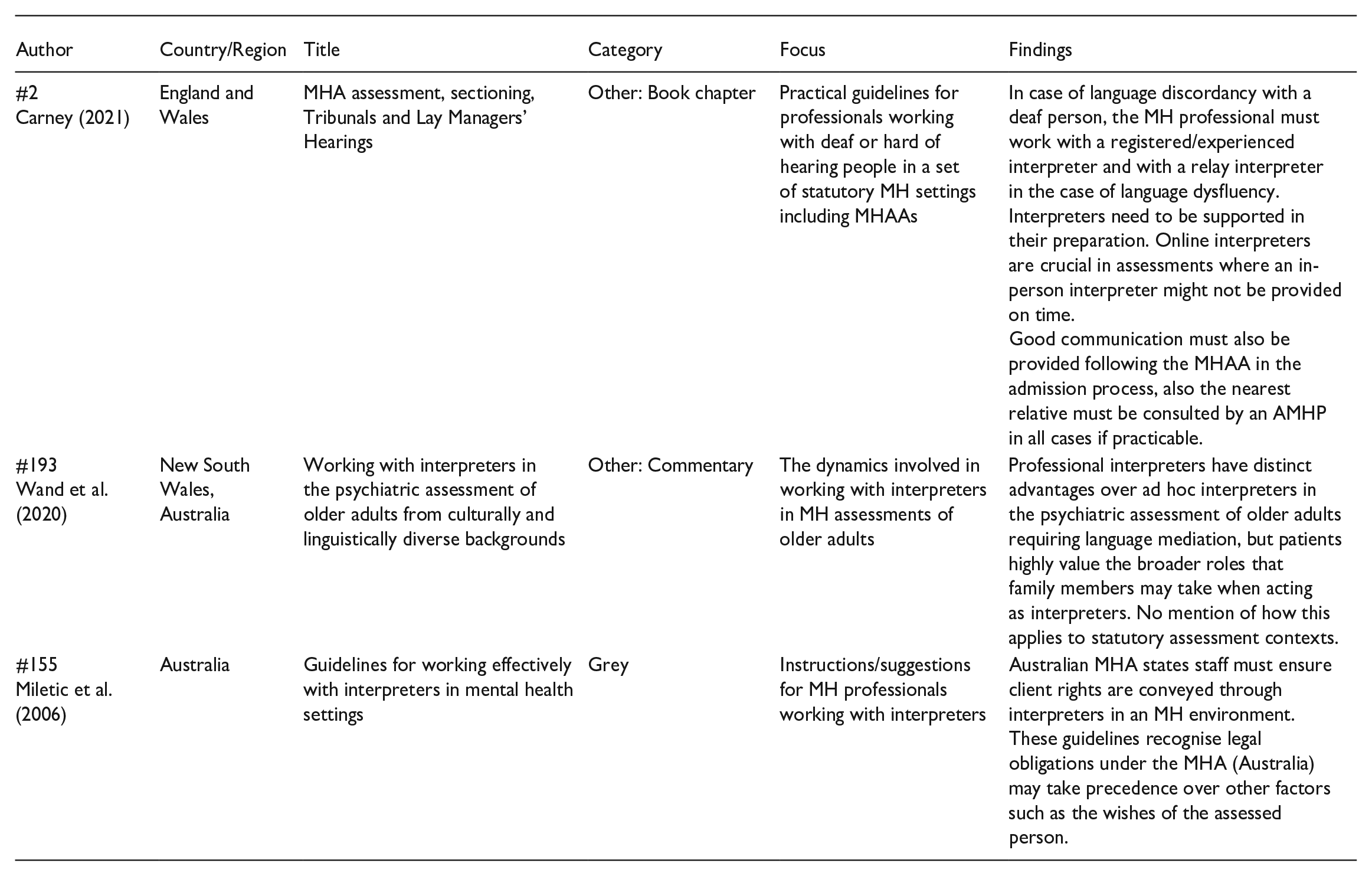
A bespoke charting template was created in Microsoft Excel combining elements of the charting template available in Covidence, which is more suitable for intervention studies, and one available through the Joanna Briggs Institute (Evans et al., 2019), which encompasses a wider range of study designs and types of literature. The study characteristics chart included: (1) authors, year of publication; (2) category of publication: empirical study, literature review, grey literature, book chapters/book; (3) country of relevance; (4) key findings or main patterns relevant to the review. These categories are reflected in Table 5.
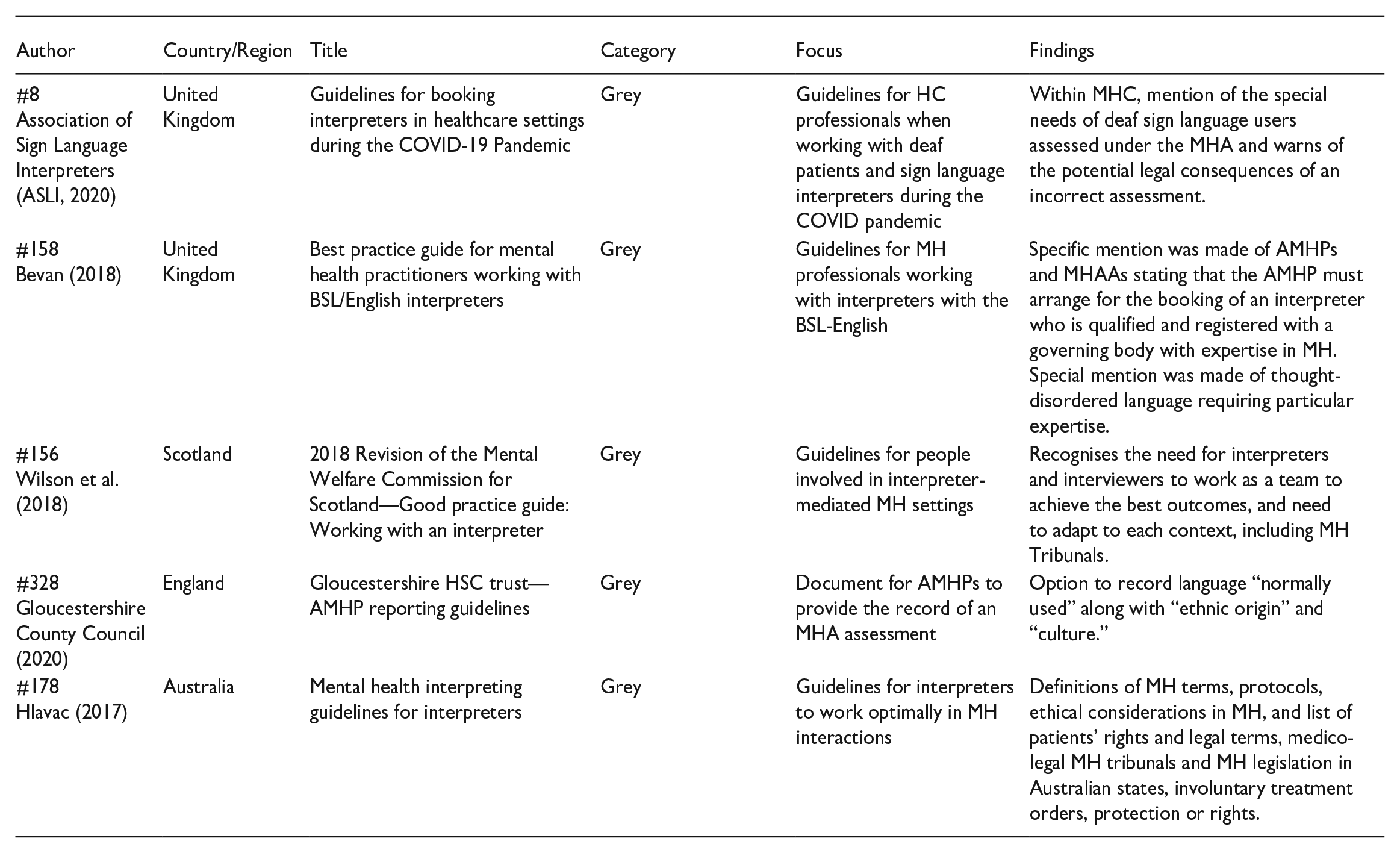
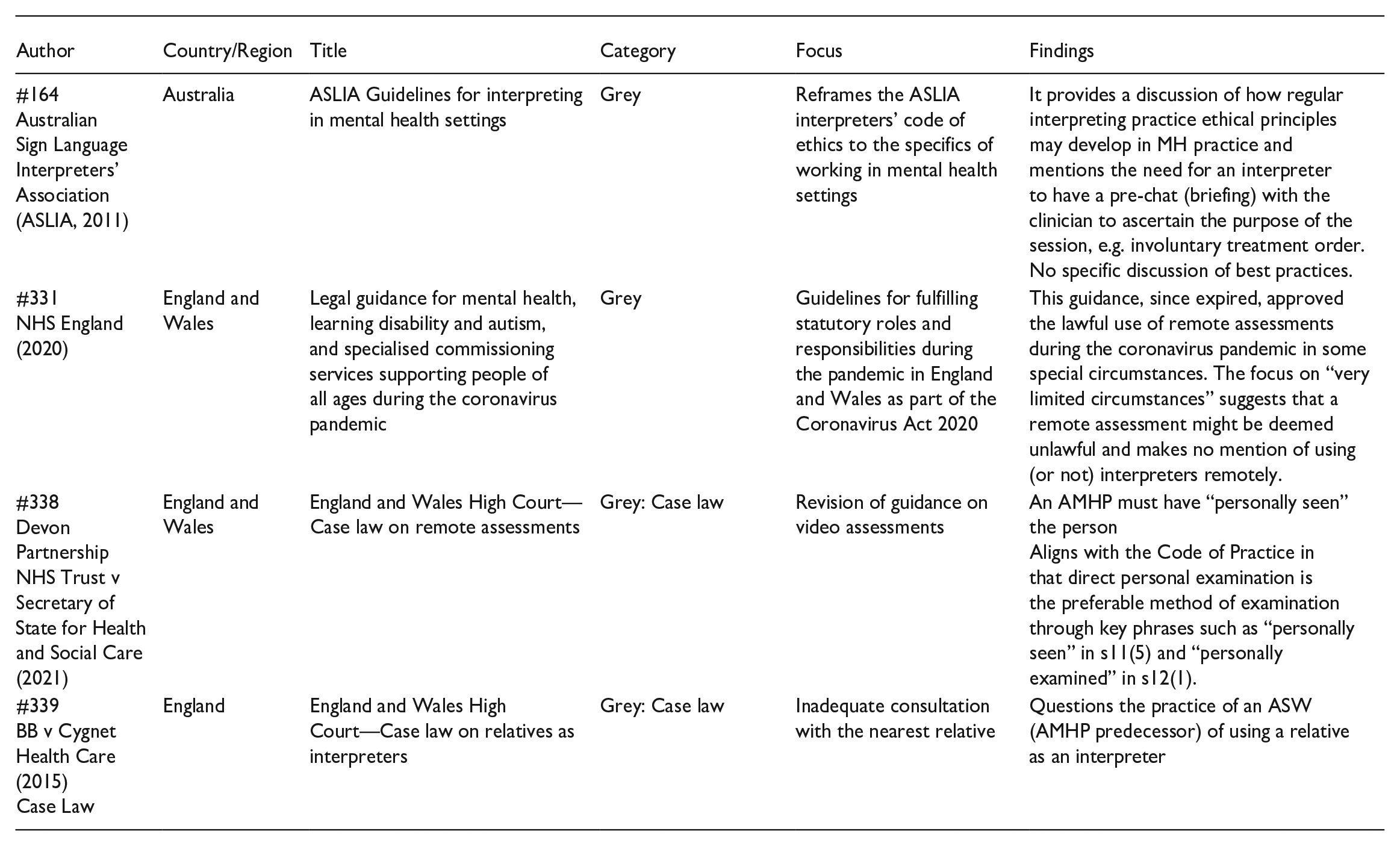
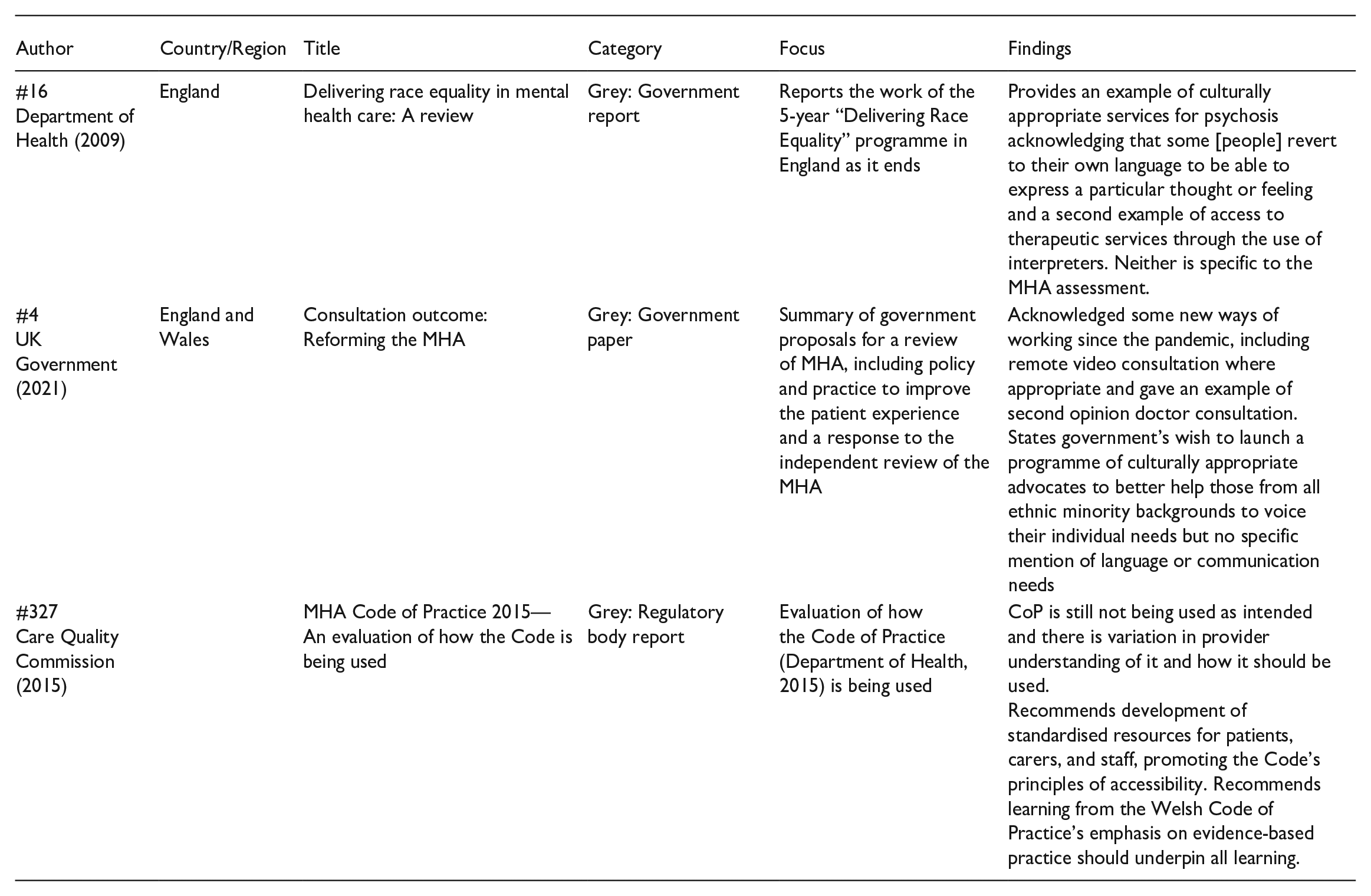
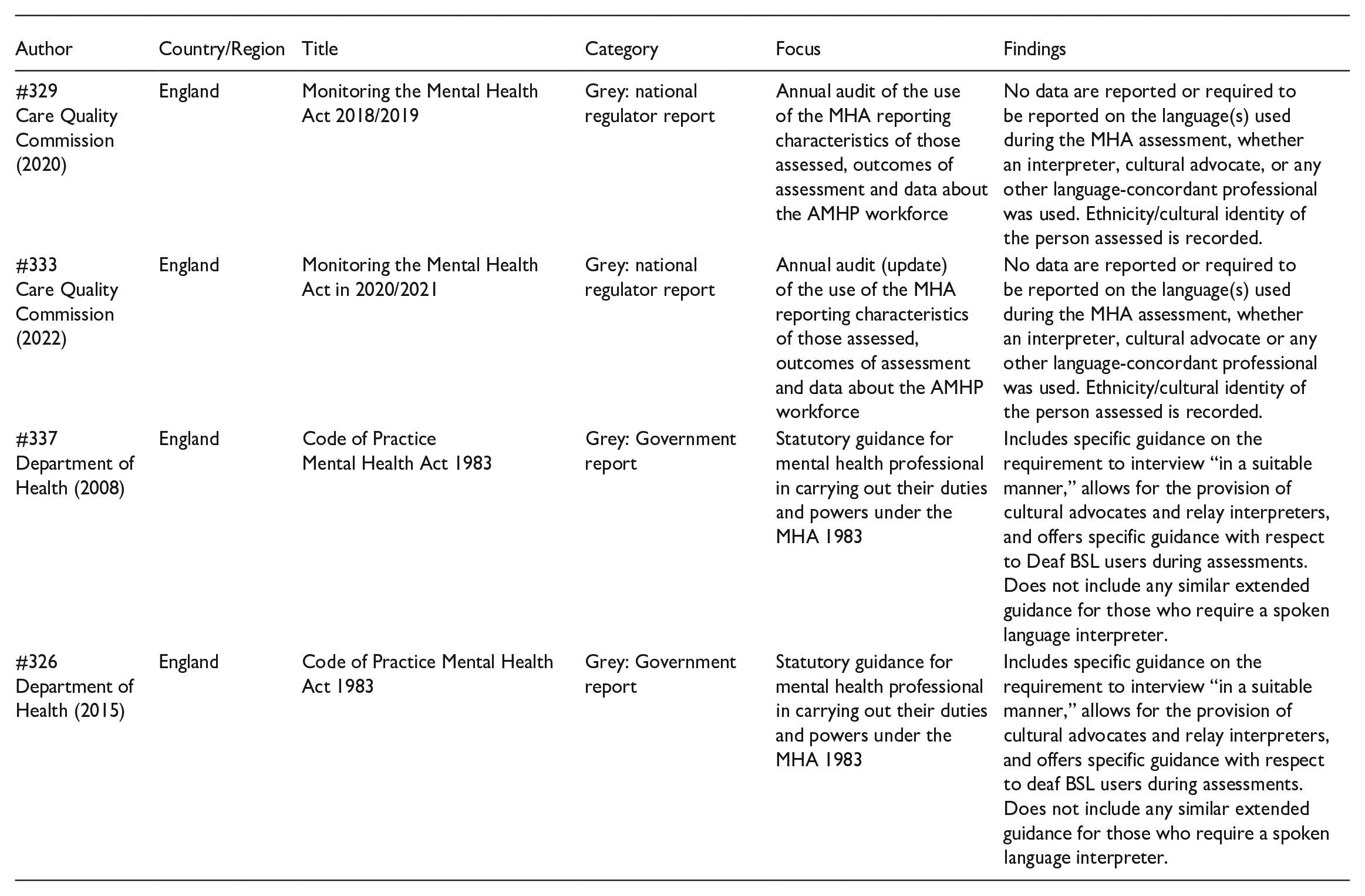
Characteristics of Selected Items.
4. Results
Characteristics of included items
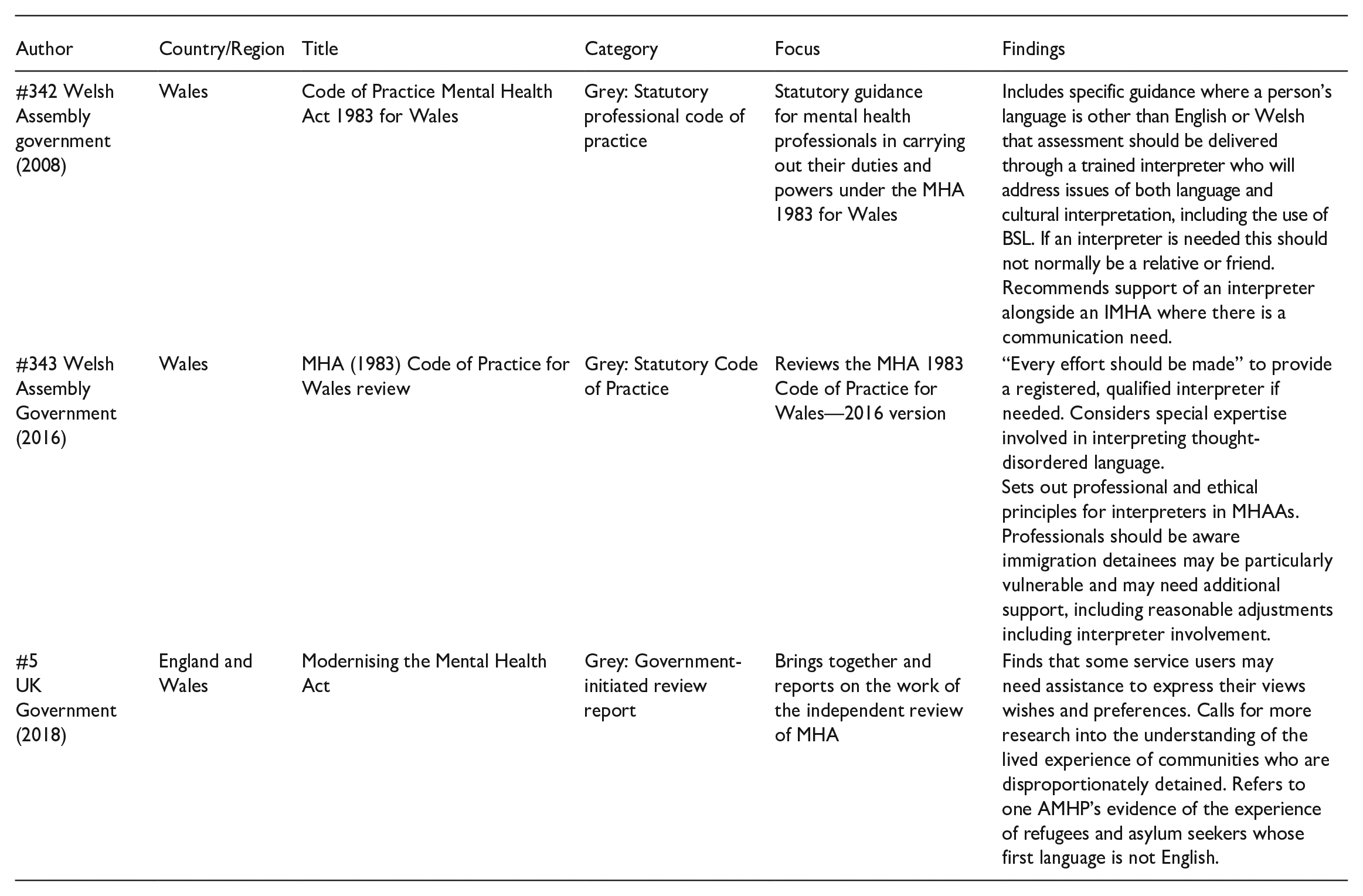
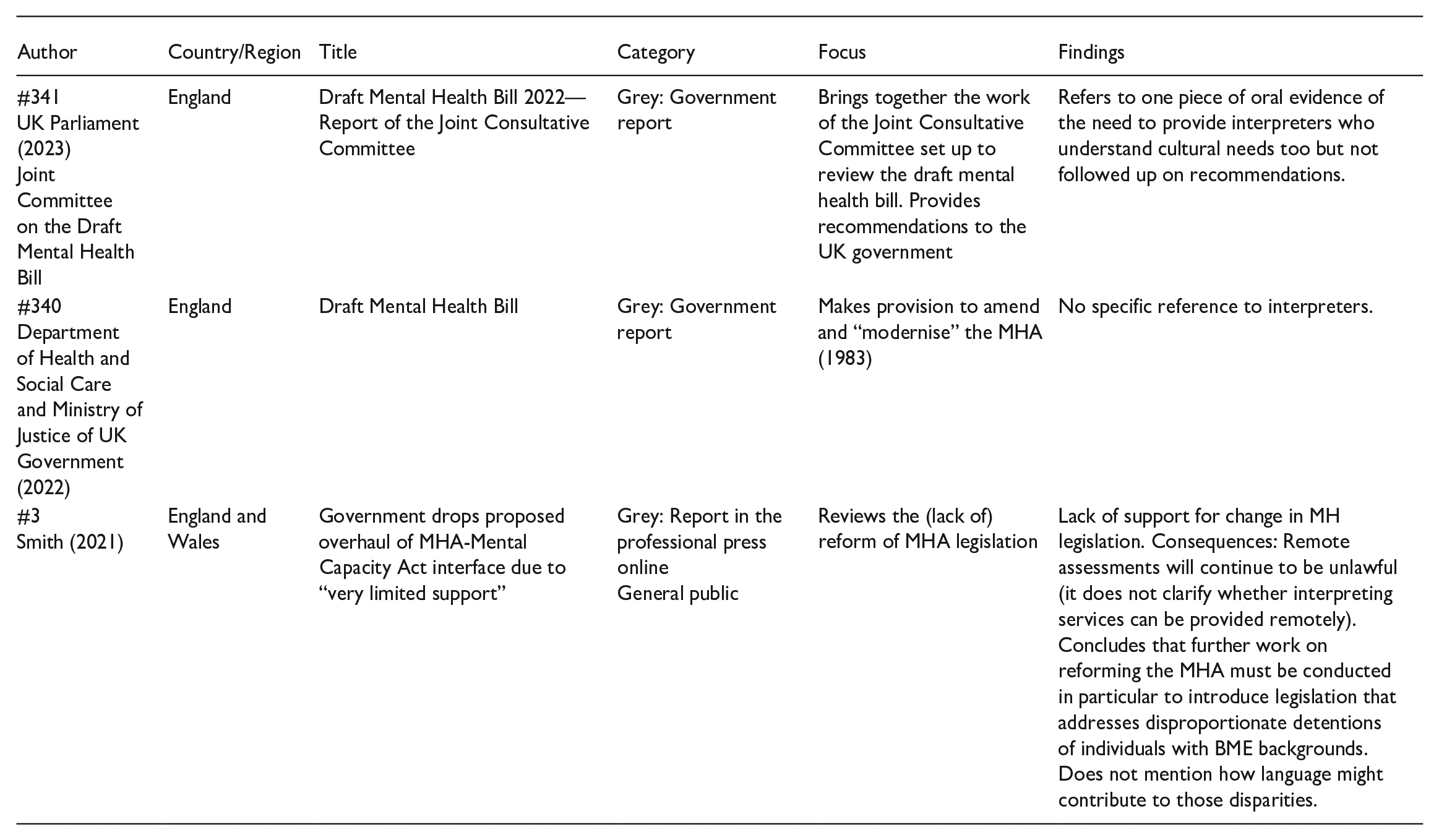
The results of the charting phase are presented in Table 5. This includes a statement about whether issues of language/communication/interpreting were explicitly included within the article’s focus given the relevance of the topic addressed.
4.1 Type of literature
Of the 44 items reviewed in the final stage, 24 are grey literature items, 10 are empirical studies, 6 are literature reviews, and 4 are classified as “other.”
Among the grey literature items, three sub-groups can be differentiated. The first sub-group consists of 15 items, which are publications by government and statutory bodies such as the Care Quality Commission. The second sub-group consists of seven professional guidelines documents, with five targeting mental health professionals and two targeting interpreters. The third sub-group consists of two online reports on legal matters by experts in the matter.
Out of the ten items featuring empirical data, seven concern aspects of AMHP professional practice, and three concern interpreters working in mental health contexts. Among these empirical items: one is quantitative in design, one is a retrospective study of patient visits, and two are mixed methods, combining surveys, interviews, and focus groups. The remaining six empirical studies follow a qualitative methodology involving interviews with sample sizes ranging from 10 to 33 participants.
Out of the six literature reviews: two are narrative reviews, two are scoping reviews, and two are systematic reviews. Regarding their thematic scope, two of the reviews concern AMHP practice, and three reviews are about the involvement of interpreters in statutory mental health. Finally, one review concerns ethnic variations in compulsory detention under the MHA.
4.2 Geographical coverage
Among the ten empirical items, seven were generated by UK-based universities, one in Ireland, one in the United States, and one in South Africa. Regarding the six literature reviews, two had a UK focus, two had a US focus, and two had an international focus. Of the seven professional guidelines, four originated in the United Kingdom, and three in Australia. The remaining grey literature items, comprising government and statutory bodies’ reports, have a UK focus. No items in languages other than English were retrieved.
5. Narrative synthesis of findings
We adopted the PAGER framework (Bradbury-Jones et al., 2022) to assist in the narrative synthesis of findings and their presentation. This tool was designed as a structured approach for synthesising and articulating the findings of a scoping review. PAGER offers a clear structure whereby each item is considered under the headings of: “
The complete PAGER table can be found in Appendix 2 in the Supplemental Material alongside this article. The elements in this table assisted in the articulation of the main findings, set out below, where three main patterns concentrated around: (a) interpreter-mediated MHAAs as a missing focus; (b) implications of interpreting in statutory circumstances not being recognised; and (c) a lack of consideration of the impact of language mediation in contemporary AMHP practice. A descriptive narrative was constructed around these three main patterns to map out the key themes and represent their prominence in the literature. By articulating these patterns in detail, nuances highlighting advances or gaps in the field were identified, providing an overview of the current state of research and practice in interpreter-mediated statutory mental health assessments.
5.1 Interpreter-mediated MHAAs as a missing focus
A major finding of this review is that there is the absence of pre-existing literature specifically investigating interpreter-mediated Mental Health Act assessments or their international equivalents, regarding either practice or their impact on outcomes.
The articles that have a broad focus on mental health interpreting do not generally include extensive, if any, references to the involvement of interpreters in situations of compulsory detention or emergency practice under the law. Even when such references are made, they are usually brief and peripheral; for example, Tribe and Lane’s (2009) reference to duties to provide linguistically accessible information to those detained. Articles focusing on issues of AMHP practice, for example, Leah (2019), Vicary, et al. (2019), Abbott (2021), and Karban et al. (2021) fail to include any consideration of how linguistic or cultural mediation might be relevant to their key findings. The absence of research evidence on the practice of interpreter-mediated MHAAs creates a misleading perception that all MHAAs take place within a monolingual context with shared language usage.
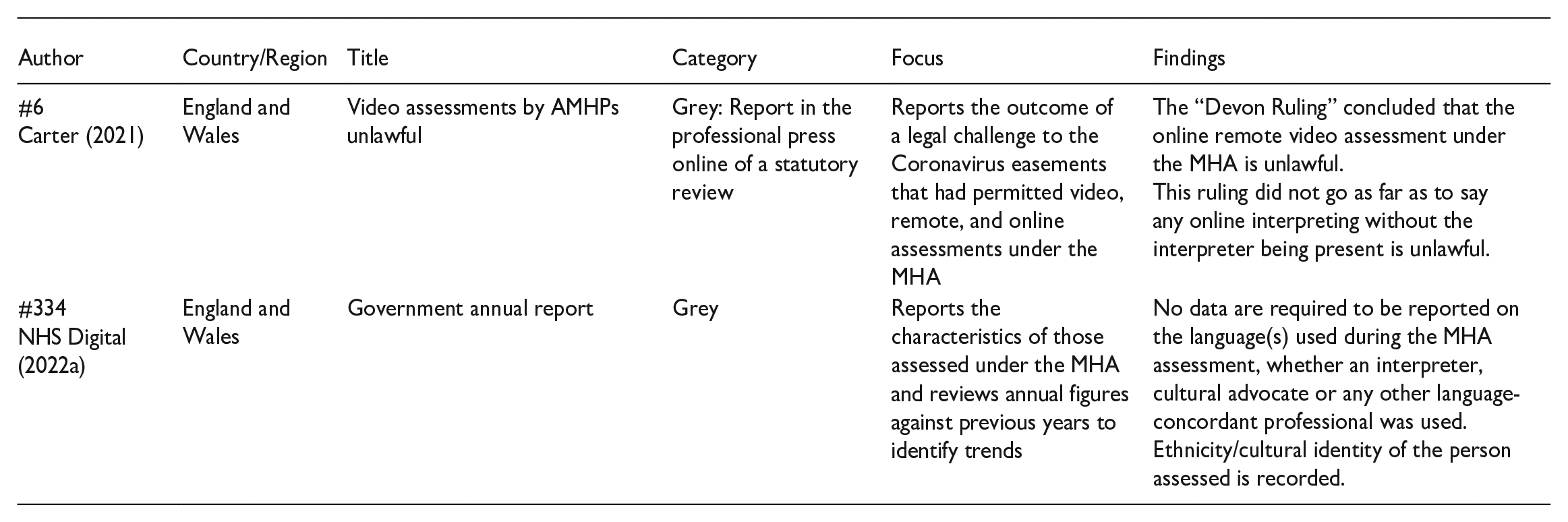
The failure to recognise the effects and potential influence of language on MHAA practice and outcomes, separate from those of cultural and/or ethnic identity, is widespread. The lack of regular reporting data on the language identities and language use of those assessed (NHS Digital, 2022a), and whether interpreters or other language-concordant professionals were required is stark. It could be argued that this illustrates a lack of emphasis on considering the language preferences of the person being assessed and the assessment process as potential sources of inequality within the MHA assessment process. This failure to attend to language differences is reinforced in the literature surrounding the reforms to the MHA with language considerations only featuring with respect to translations of written texts/information for patients or special considerations for those who are deaf (UK Parliament, 2023). In the most recent report from the Joint Consultative Committee on the Draft Mental Health Bill (2023), the body set up to scrutinise the draft mental health bill, the brief mentions of interpreting are subsumed under considerations of advocacy for the person assessed, rather than identified in their own right (UK Parliament, 2023).
The diminishment of the potential impact of interpreter mediation on the process and outcomes of MHAAs is systemic. For example, the temporary allowances under the Coronavirus Act 2020 in the United Kingdom that briefly permitted remote MHAAs were eventually judged unlawful in part because of the negative impact on judgements, interaction, and communication (see NHS England, 2022). Remote interpreting is still widely practised in MHAAs (Young et al., 2023). However, the impact of a “disembodied voice” during an assessment on someone already experiencing mental health distress, which could result in the deprivation of liberty, remains unquestioned: Why are questions regarding the legality of remote assessments not being extended to remote interpreting? This is an area of practice research that clearly requires further work. The gap in the evidence-based practice literature, practice guidance and statutory reporting is not limited to the United Kingdom alone. This lack of attention extends internationally, making the scarcity of research directly in this area a matter of global concern.
A second aspect related to “interpreter-mediated MHAAs as a missing focus” concerns the characteristics of the available literature and the clear scarcity of empirical studies relating to interpreter mediation in MHAAs and their equivalents. Empirical research plays a vital role in advancing knowledge and the absence of it limits the ability to draw evidence-based or evidence-informed recommendations for practice. Although numerous guidance documents, both statutory and non-statutory, emphasise the need for best practices, including proper assessments as required by legislation, the preference for professionally qualified interpreters, and the duty to make provisions for them (ASLIA, 2011; Carney, 2021; Department of Health, 2008, 2015; Hlavac, 2017; Welsh Assembly Government, 2008), these documents do not constitute an evidence base for practice, neither for interpreters nor for AMHPs.
5.2 The implications of interpreting in statutory circumstances not being recognised
This review concludes that the prevailing body of research in interpreting studies does not adequately distinguish research, guidelines, or practice recommendations that apply in mental health statutory contexts, such as the MHA, from general work on interpreting mental health. Most of the literature available refers to interpreter mediation in psychotherapeutic (Bot, 2015) or psychiatric (Drennan & Swartz, 2002; Wand et al., 2020) practice whether in assessment, evaluation, or treatment, and therefore does not recognise distinctive issues at stake in statutory assessments. This applies both to empirical studies and professional guidelines. Some of the issues prevailing in existing mental health interpreting literature include (1) the interpreters’ role, agency and visibility including ethical dilemmas in relation to those, (2) links between language, culture, and mental health, (3) challenges around ensuring accuracy in mental health, for example, in the case of cross-cultural equivalents, (4) the impact of language mediation on mental health practice including assessments, and (5) interpersonal dynamics. In the literature reviewed, none of these issues is addressed in the context of MHAAs and the special conditions that may pertain to emergency or statutory practice under the law. As a result, this scoping review highlights the need for research that explores how long-standing debates and current expertise in the field of interpreting studies, particularly mental health interpreting, apply to statutory mental health assessments and, by extension, to other statutory practices. Such research would lead to generating new insights and perspectives on the topic which would, in turn, advance the field of interpreting studies. The contribution of this area of work to interpreting studies lies in the unique challenges presented by interpreting within statutory mental health, such as interpreting complex legal terminology, the role, responsibilities, and powers of professionals conducting MHAAs, and the interpreting of potentially disordered language output of people severely affected by mental health conditions, all within the context of potential involuntary detention under the law.
This lack of recognition of the particular nature of mental health interpreting in relation to statutory mental health contexts such as MHAAs is also present in existing guidance for interpreters. Some do mention special legal considerations and associated concepts, or ethical considerations that might be pertinent to MHAAs (ASLI, 2020; ASLIA, 2011; Hlavac, 2017), however, they do not comprehensively address the unique considerations, procedures, and challenges encountered in statutory mental health assessment under whatever jurisdiction. The absence of detailed guidance for interpreters in situations of mental health crises and collaboration with professionals under legal obligations poses a challenge. The scarcity of explicit practice frameworks may affect interpreters, given that there is not sufficient guidance to support their decision-making in this context, thus compromising the overall quality of the assessment process, particularly in relation to legal aspects. In addition, the lack of existing literature raises concerns regarding the preparation, training, and support provided to interpreters working in statutory mental health contexts, including the absence of these matters within generic interpreter training programmes. Building on this point, when discussing the need for interpreters to have knowledge and skills that extend beyond conventional interpreting competencies to effectively work in specialised mental health contexts, it is worth acknowledging recent developments in the area of trauma-informed interpreting. This approach calls for recognition of the impact of trauma on individuals’ behaviour and linguistic output, including thought-disordered language, and encourages interpreters to apply trauma-informed principles to their work (Bancroft, 2017; González-Campanella, 2022).
This scoping review also identified a lack of literature on the need for collaborative working practices between AMHPs (or equivalents) and interpreters in MHAAs (or equivalents). This is important because there is some evidence (from non-statutory mental health services) to suggest that interprofessional collaboration between mental health practitioners and interpreters can lead to positive outcomes (Gryesten et al., 2023). However, there is a gap in the existing literature on the specific strategies and techniques that AMHPs and interpreters can use to effectively collaborate during MHAAs, in which the legal aspect is especially salient. Moving beyond academic literature and guidelines, statutory documents paint a similar picture: while the statutory code of practice accompanying the MHA (Care Quality Commission, 2015; Department of Health, 2008, 2015; Welsh Assembly Government, 2008, 2016) does offer certain guidance regarding situations that call for the involvement of an interpreter, it falls short of providing specific instructions on how AMHPs can effectively collaborate with interpreters. The existing guidance primarily focuses on determining when interpreter assistance is required, rather than offering specific guidance on optimising the working relationship between AMHPs and interpreters. The lack of guidance that AMHPs may experience when conducting assessments through an interpreter, and assumptions that might be made regarding the interpreters’ level of knowledge about core legal concepts and their implications, for instance, will require carefully considered practice responses. Guidance that supports AMHPs to jointly navigate the complexities of meaning-making in MHAAs as opposed to viewing interpreting as a bolt-on mechanism, or a “conduit,” would not only enhance AMHP confidence in interviewing “in a suitable manner” and reaching a decision on outcomes but would also have associated benefits for the experience of people assessed.
5.3 Lack of consideration of impact of language mediation in contemporary AMHP practice
The parameters of the scoping review include available empirical research on the challenges involved in AMHPs’ professional practice, to identify the extent to which challenges associated with language mediation might be recognised. It was notable to find that challenges associated with the need for language mediation have been largely overlooked in the existing body of research that focuses on contemporary AMHP practice.
The current literature predominantly focuses on various challenges that AMHPs encounter in their work, such as effectively managing risks (Simpson, 2020), navigating complex legal frameworks (Abbott, 2021; Fish, 2022), safeguarding the rights and autonomy of individuals undergoing assessment and rights of the nearest relative (Dixon et al., 2020), and fostering collaborative relationships with other professionals during the coordination of MHAAs (Davidson et al., 2021). These studies shed light on AMHPs’ awareness of the ethical dilemmas inherent in wielding statutory powers, including striking a balance between autonomy and safety, managing power dynamics, managing the complexities of their coordinating role, and grappling with time constraints.
It was notable that in all these studies, which admittedly had a different focus than our topic of interest, there was not even a passing consideration given to whether and how the points being made might be affected by practice that is not monolingual. This absence is notable, especially considering previous research indicating that language mediation can disrupt standard communicative practices in social work, presenting challenges that practitioners may not have the resources to effectively address (Tipton, 2016). The specific challenges faced by AMHPs in such interpreter-mediated assessments are multifaceted. The presence of interpreters introduces a layer of complexity for AMHPs that can affect the accuracy and reliability of information exchanged. A higher potential for misinterpretations, omissions, or misunderstandings can occur, potentially compromising the overall assessment process and subsequent decision-making. This is particularly salient in the case of acute mental health: for example, the MHA Code of Practice (Department of Health, 2015: 36) states that the AMHP should be responsible for “booking registered qualified interpreters with expertise in mental health interpreting.” This includes recognising that “the interpretation of thought-disordered language requires particular expertise” (Department of Health, 2015: 133). However, the specific skills and expertise required to effectively interpret thought-disordered language, particularly in the context of an MHAA, are not thoroughly examined in the existing body of knowledge. Thought-disordered language, occasionally observed in individuals with severe mental health conditions (Caplan, 2009), is likely to pose unique challenges for interpreters because of the complex and sometimes fragmented nature of the language use. Understanding and accurately conveying the meaning and intent of such language calls for specialised expertise that goes beyond general language interpretation skills and beyond generic AMHP training. However, the literature lacks a comprehensive exploration of the specific competencies, training, and qualifications that interpreters and AMHPs need to possess to jointly address thought-disordered language within the context of MHAAs. By addressing this gap in the literature, further research could expand on the practical implications of the MHA Code of Practice’s provisions related to interpreter selection and utilisation with a focus on effective collaborative practice.
Although some of the AMHP-related practice research focuses on power inequalities in MHAAs (Buckland, 2020), this is only considered in monolingual contexts, which itself is not acknowledged in the literature. The AMHP, as the primary decision-maker in the assessment, is identified as holding a position of power. However, how the presence of an interpreter introduces an additional layer of complexity to the assessment process, influencing the distribution of power among the various participants involved, remains unaddressed. This is important because power is connected to the notion of “voice,” understood to mean the expression of one’s wishes and feelings and that might have an influence on a person’s mental state and behaviour. Interpreter mediation introduces an additional layer of communication that either enables or constrains the service user’s “voice” and how it may be understood in the assessment. Surprisingly, this crucial aspect has not been comprehensively explored in the existing literature concerning one of the most profound civil law powers, which allows the deprivation of an individual’s liberty. Attention to the availability and proficiency of interpreters and the challenges these pose for AMHPs is also absent. This is salient because, in accordance with the MHA Code of Practice, AMHPs are responsible for organising interpretation. AMHPs are also charged with engaging with an assessed person’s Nearest Relative to ascertain whether they have an objection to the person’s detention under the MHA. The available literature that discusses this role does not mention any complexities that might arise if the AMHP and nearest relative or wider family do not share the same language (Dixon et al., 2020; Hemmington et al., 2021). However, previous research on social work with interpreters has identified difficulties that social workers might have in liaising with families of service users who use a language other than English, even when interpreters are involved (Pollock, 2023). In sum, the way in which interpreting adds further complexity to current practice concerns is largely absent from the current body of knowledge.
6. Concluding remarks
This scoping review set out to answer two research questions about the state of knowledge concerning interpreter-mediated statutory mental health assessments, specifically MHAAs. The first question concerned the enablers and barriers to good practice for AMHPs and interpreters in MHAAs. The main finding of this review is the almost total absence of the consideration of interpreter mediation in empirical research on MHAAs and the lack of evidence-based guidance for practice. Building on this idea, the absence of evidence highlights the potential catalysts for improving practice, which may include a focus on fostering collaborative interprofessional teamwork, jointly involving interpreters and mental health professionals. In addition, exploring how and why the unique circumstances of statutory work within the mental health field may differ from conventional mental health interpreting practice is essential. Finally, it is crucial to examine how key considerations in AMHP practice, such as power dynamics and voice, can adapt to, or be influenced by, the additional layer of working with interpreters.
The second question for this review set out to explore how interpreter mediation supports or impedes the legal rights and best interests of individuals assessed under the MHA or its international equivalents. Our principal finding is that none of the literature items we identified addressed this as an issue in its own right beyond guidance of when interpreters should be provided, and the rights of the individual to have access to high-quality interpretation. There is no direct evidence from practice and no clarity that evidence from related contexts, including mental health interpreting more generally, is adequately relevant to the very particular practice circumstances of MHAAs.
When considering the characteristics of the literature items identified, an unanticipated finding is the lack of transdisciplinary approaches across the fields of interpreting studies and health/social care in this context. This literature review has brought together relevant literature items from the fields of social work and interpreting studies that address overlapping points in the context of MHAAs or equivalents. By synthesising the insights from both disciplines, this review sought to highlight the interconnections and shared perspectives that can contribute to a more comprehensive understanding of interpreter-mediated MHAAs. The findings suggest that while both fields have valuable perspectives to offer, both bodies of knowledge appear to operate separately. The lack of cross-fertilisation hinders the development of a comprehensive understanding and approach to interpreter-mediated MHAAs. This gap in interdisciplinary research likely points to limited opportunities for interprofessional collaboration and training. Social workers and interpreters typically work in separate organisational structures, with little opportunity for collaboration or joint training. This can result in social workers and interpreters having limited knowledge of each other’s roles and responsibilities, leading to potential misunderstandings and challenges in completing effective MHAAs or failure to conduct them in a suitable manner.
This review marks the initial phase of the INForMHAA project and serves as the foundational step towards addressing the identified gap in practice-based research and aims to offer tailored guidance and training resources for AMHPs and interpreters in this field. This review makes several contributions to interpreting studies: it draws attention to a highly specialised area of mental health interpreting; it exemplifies the value of scoping reviews in cross-disciplinary studies on interpreting; it encompasses both signed and spoken language interpreting within a common focus of inquiry and it lays the groundwork for a systemic exploration of this topic in different national contexts, thereby facilitating future cross-national comparisons across countries with different legislative frameworks and health care systems, thus increasing understanding on mental health interpreting practices globally.
Having acknowledged its contribution, it is also important to recognise the limitations of this scoping review to guide future reviews on interpreter-mediated statutory mental health assessments or similar topics. For instance, the breadth-over-depth approach of this scoping review means that nuanced aspects of interpreter-mediated MHAAs may have been overlooked. In addition, an exhaustive quality assessment of the selected items was not provided, potentially limiting the ability to critically evaluate the quality of the evidence base. Addressing these limitations could enhance the robustness of future literature reviews in this field or similar ones.
Supplemental Material
sj-docx-1-isy-10.1177_27523810241279010 – Supplemental material for Interpreter mediation in statutory mental health assessments: A scoping review
Supplemental material, sj-docx-1-isy-10.1177_27523810241279010 for Interpreter mediation in statutory mental health assessments: A scoping review by Natalia Rodríguez-Vicente, Alys Young, Sarah Vicary, Jemina Napier, Rebecca Tipton and Celia Hulme in Interpreting and Society
Supplemental Material
sj-docx-2-isy-10.1177_27523810241279010 – Supplemental material for Interpreter mediation in statutory mental health assessments: A scoping review
Supplemental material, sj-docx-2-isy-10.1177_27523810241279010 for Interpreter mediation in statutory mental health assessments: A scoping review by Natalia Rodríguez-Vicente, Alys Young, Sarah Vicary, Jemina Napier, Rebecca Tipton and Celia Hulme in Interpreting and Society
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was funded by the NIHR School for Social Care Research grant number REF# P172. The views expressed in the article are not necessarily those of the funder.
Supplemental material
Supplemental material for this article is available online.
Notes
Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.