
Abstract
This article explores the extent to which healthcare interpreting can be considered “relational practice.” It describes an interactional sociolinguistic study conducted in Australia, based on video recordings of two naturally occurring interpreted general practice consultations. Participants were hearing Australian Sign Language (Auslan)/English interpreters, deaf patients, and hearing doctors. Analysis of these recordings was supplemented by reflective interviews with participants. The study examines the ways in which interpreters facilitate good working relationships between participants, and to explore the extent to which their decision-making is driven by relational considerations. The analyses presented in this article provide evidence that relational work is an important aspect of the healthcare interpreter’s role. Some of the ways in which it is achieved, however, may challenge our ideas about “appropriate” interpreter behaviour. Thus, the skilled and experienced interpreters in the study were seen to modify face threats, directly influence the flow of interaction, and actively facilitate social talk and humour, occasionally even engaging in it themselves. It is argued that interpreters’ decisions can only be understood within the discursive context in which they occur, and such behaviour can highlight interpreters’ attentiveness to the maintenance of good rapport.
1. Introduction
In the healthcare setting, we know that good practitioner–patient rapport is a crucial element of communication. Researchers have suggested that when practitioners and patients get on well with each other, this can improve accuracy and efficiency, and it can positively affect health outcomes for patients (Allison & Hardin, 2020; Leach, 2005; Ross, 2013; J. Silverman et al., 2005). Good rapport in this setting can help practitioners draw out important clinical details from patients, which helps them to treat patients more effectively (Ross, 2013), and it may also encourage better treatment compliance (Leach, 2005).
Rapport is largely established and maintained through speakers’ engagement in “relational work,” this being “the ‘work’ individuals invest in negotiating relationships with others” (Locher & Watts, 2005, p. 10). It is a broad concept that encompasses any and all strategies used in the negotiation of relationships, be they positive and supportive relationships, confrontational relationships, or anything in between. Leach (2005) suggests that practitioners wishing to create good rapport with patients should focus on strategies including, but not limited to, being friendly, sincere, engaging, and empathetic. Cassatly (2010) suggests that the success of this relationship relies on mutual trust, which is built through effective communication, empathy, and the practitioner viewing the patient as “a ‘whole’ human being and not just a person with a malady” (p. 229). We also know that seemingly “irrelevant” conversational acts such as small talk can support positive rapport-building and the achievement of clinical goals (i.e., reassuring patients, minimising pain; Álvaro Aranda & Lázaro Gutiérrez, 2022; Holmes & Major, 2002; Macdonald, 2016).
When patients and healthcare practitioners do not share a common language, their interaction—and any attempts at relational work—are often mediated by an interpreter. Yet, there is relatively little focus on rapport and relational work within healthcare interpreting research and pedagogy. This article aims to bolster this line of research with a detailed qualitative description of Australian Sign Language (Auslan)/English interpreters’ relational work in a general practice setting in Australia.
2. Context for the study
The role of interpreters in facilitating relational work is an emerging area of research. We need rich description of what experienced interpreters actually do in situated practice, so that we are better equipped to teach interpreting students the skills that they will need for effective professional practice. This section briefly outlines current understandings of health interpreter role, particularly with regard to relational work.
2.1 The interpreter’s role
Recent studies of (spoken and signed) interpreted interaction based on naturally occurring data have shown that interpreters have an active “visible” role in interaction, through managing discourse and co-constructing the meaning of talk with the primary participants (e.g., Angelelli, 2004; Bolden, 2000; Major, 2014; Major & Napier, 2019; Mapson & Major, 2021; Metzger, 1999; Napier, 2007; Wadensjö, 1998). By their very presence, interpreters are key players in the construction and shape of interaction (Angelelli, 2004; Davidson, 2002; Metzger, 1999). A key part of understanding how and why interpreters impact upon interaction, and how this relates to their role in facilitating relational work, is acknowledging that they make interpretation decisions based on more than just a message equivalence level. That is, despite a pervasive misperception that interpreters convey only messages (i.e., discrete units of information) between languages, the actual moment-by-moment decisions they make are far beyond this level (Major & Napier, 2019).
Metzger’s (1999) study of American Sign Language-English interpreting in a paediatric setting highlights the interpreter’s active role in discourse management, including clarifying information with participants and using attention-getting strategies to ensure clear communication. Some instances of documented interpreter visibility have also included disempowering behaviour on the part of interpreters. Angelelli (2004), for example, discusses an example where an interpreter reprimands a patient for her narrative speaking style, which does not match the short answers expected by the doctor. Bolden (2000) found evidence of an interpreter pursuing clinically relevant information with his own questions, while omitting what he perceived as irrelevant topics.
Examples like these have prompted scholars such as Hale (2007) to call for researchers to problematise such instances of visibility. At some point, Hale (2007) claims, it must be acknowledged that agency exhibited by interpreters surpasses communication brokering to become gate-keeping. Tebble (1996) states categorically that “all turns at talk should be interpreted” (p. 44). Although this perspective is a useful reminder that interpreters must constantly reflect on the impact of their decision-making, and not take ownership of the talk of participants, it may risk not accounting for the fluidity of interpreter role in context (Major & Napier, 2019). As Llewellyn-Jones and Lee (2014, p. 61) remind us,
what is “right” in one context and one interaction between one set of participants with one combination of language/communicative skills and with one or several shared goal(s), is unlikely, if only one of those parameters changes, to be “right” in another.
To this end, this article seeks not to generalise, or prescribe what interpreters should do, but rather to develop a richer understanding of what skilled and experienced interpreters actually do in context. The focus of this study goes beyond interactional management to explore the effect of relational dynamics on the interpreter’s decision-making process.
2.2 “Face” and rapport work by interpreters
A concept central to relational work is the notion of “face.” Face relates closely to a person’s sense of self-worth and dignity, and has been described as “the positive social value a person effectively claims for himself by the line others assume he has taken during a particular contact” (Goffman, 1967, p. 5). To redress or mitigate a potential face-threatening act (e.g., confrontational talk), speakers engage in “facework” (a term originally from Goffman, 1967), which is “the construction of our own concept of self and the work we do in social interaction to enable others to construct, reproduce and maintain their self-concepts” (Watts, 2003, p. 131). We each bring our own “frames” to an interaction, through which we make judgements about what is and is not polite within the social and cultural context we are in (Holmes, 2008), and when facework is necessary.
Spencer-Oatey’s (2000) “rapport management theory” focuses on the concept of face and highlights the linguistic and non-linguistic tools (e.g., including gesture and intonation) used by participants to do facework and negotiate rapport in interaction. In recent years, researchers have begun to explore interpreters’ active involvement in such relational work, particularly in the medical and mental health fields (see, for example, Allison & Hardin, 2020; Chang et al., 2021; Delizée & Michaux, 2022; Hemingway, 2023; Mapson & Major, 2021; Rodríguez-Vicente, 2021), as well as other settings including police and intelligence (Goodman-Delahunty & Howes, 2019; Skinner, 2020), and employment (Dickinson, 2014; Harrelson & Nicodemus, 2022).
Within the health setting, evidence is emerging that relational work should be considered a vital part of the interpreter’s role. Delizée and Michaux (2022), for example, explored this through thematic analysis of interview data and discourse analysis of a French-Russian interpreted psychotherapeutic consultation. They show how the interpreter mitigated both face-threatening and face-flattering speech acts, and therefore engaged in co-constructing the rapport work and the supportive relationship between participants. They found that the interpreters, therapists, and patients in their study were all very aware of the interpreter’s role in facilitating positive and trusting relationships in this setting (see also Rodríguez-Vicente, 2021). Hemingway (2023) explored the complexity of relational work based on the experiences of signed language interpreters in Canada, highlighting the adaptability needed by interpreters to navigate and negotiate challenges specific to each interaction. Hemingway also describes how aspects that allow interpreters to better attend to rapport (such as small talk in the waiting room) tend to be unpaid labour and are therefore undervalued.
Other studies have discussed the consequences of inadequately conveying rapport work. In a family medical clinic in the United States, Allison and Hardin (2020) found that over 80% of clinicians’ attempts at rapport work were not conveyed to Spanish-speaking patients by interpreters at all. It is important to note that the interpreters in their study were untrained. As Hsieh (2022, p. 2) notes, “. . . when interpreters focus on medical information and ignore clinicians’ rapport-building talk, clinicians may appear emotionally detached.” At the other end of the spectrum, Tebble (1999) illustrates how an interpreter’s decision to change the affect of a message can be misleading. In one excerpt from her data, for example, a patient has high blood pressure, something which the practitioner has stated categorically. The interpreter, however, mitigates the seriousness of this by referring to “a little raised blood pressure” (Tebble, 1999, pp. 193–194), thereby reducing the force of the original statement and somewhat changing its meaning (see Hale, 2002; Jacobsen, 2008; Mason & Stewart, 2001, for discussion of similar actions within the courtroom setting).
Trained interpreters have been observed making decisions based on existing relationships between participants. In a health setting, Mapson and Major (2021) show how interpreters’ familiarity with participants and context can reduce cognitive load and allow interpreters to better attend to relational goals (see also Hemingway, 2023). From the perspective of health professionals, interpreter familiarity also helps to build trust and reduce the intrusiveness of the interpreter as an extra person in the room (Schofield & Mapson, 2014). Interpreters in naturally occurring data have also been seen to occasionally engage in rapport-oriented talk themselves. Álvaro Aranda and Lázaro Gutiérrez (2022), for example, examined real-life interpreted health interactions in Spain, based on observations by researchers rather than recordings. The trained interpreters in their study were attuned to health practitioners’ use of small talk to achieve relational and clinical goals, conveying it and even participating it at times (see also Major & Napier, 2019; Wadensjö, 1998).
Beyond the healthcare setting, interpreters have been observed negotiating cultural gaps too. In New Zealand, McKee and Awheto (2010) describe how a Māori New Zealand Sign Language interpreter in a Māori setting took on a “cultural broker” role, because the Māori deaf people in the interaction did not have the necessary cultural knowledge to assume a leadership role they had been given. The interpreter actively monitored and mediated potential cross-cultural tensions to facilitate a successful outcome. Similarly, Roy (2000) observed an American Sign Language interpreter actively helping a university student to behave appropriately, by giving a cue that his first response to his Professor had not been appropriate. Roy suggests that the interpreter was engaging in facework, because the student could lose face by demonstrating a lack of awareness of the cultural norms and the interpreter in her study assumed responsibility for preventing this.
Building on these examples of decision-making beyond the “message” level, this article examines some ways in which doctor–patient (and interpreter) relationships are negotiated and maintained through interpreted talk. Specifically, the analysis focuses on interpreters’ decision-making in instances of rapport-threatening talk (an accusation and a complaint) as well as more global rapport-oriented talk (empathy and humour).
3. Data collection and analysis
The study takes an interactional sociolinguistic (IS) approach (Gumperz, 1982, 1999, 2001) to analysing interaction data at a detailed turn-by-turn level, to understand the processes through which participants convey and understand relational work. An IS description of naturally occurring data allows us not only to understand the interactional and linguistic choices made by all participants, including interpreters, but also to understand the impact of these decisions upon the way relationships are negotiated through the flow of talk.
3.1 Auslan and Auslan/English interpreting
Australian Sign Language (Auslan) is the visual-gestural language used by an estimated 6,500-strong Deaf community (Johnston, 2006). Signed language interpreting in Australia has been established and recognised as a profession since the 1980s (Napier et al., 2010), and interpreters are now employed in a wide variety of settings, including employment, social services, conference, education, courtroom, and healthcare. Interpreters are expected to be qualified and hold a credential from the National Authority for the Accreditation of Translators and Interpreters (NAATI 1 ). There are different levels of NAATI credentials available to test for, depending on the interpreter’s level of skill and experience.
3.2 The participants and the data
The two interactions recorded and analysed for this study were naturally occurring; that is, the consultations would have happened whether or not they were filmed for this study, allowing us the closest possible observation of how people actually interact in real life (D. Silverman, 2006). The study was granted ethical approval by both the Macquarie University Human Research Ethics Committee and the Royal Australian College of General Practitioners National Research and Evaluation Ethics Committee.
To find suitable recording opportunities, I first shared information about the planned study and invited local deaf people and interpreters to express their interest in participating. Deaf people generally took the lead and contacted me when suitable opportunities arose, after which I then approached the general practitioner (GP), the practice manager, and the interpreter. Two opportunities were declined at this stage as the health staff were not interested in participating. Informed consent was given by participants after they had had an opportunity to read/watch information about the project (available in both Auslan and English) and to ask any questions. Digital video cameras were set up in the GPs’ rooms and, to reduce the intrusion of recording as much as possible, I left the room for the duration of the appointment.
The nature of each recording, as well as the participants and their existing relationships, is quite different to each other. This provides a useful comparison in exploring how interpreter decisions are inextricably bound to context, including participant goals and their existing relationships. Recording 1 involves a professional interpreter who is also the daughter of the patient, and Recording 2 involves an interpreter who has only a prior professional relationship with the other participants. Although one interpreter has a dual role, both interpreters are skilled, experienced, and NAATI-credentialed.
3.2.1 Recording 1
The first interaction involves a male deaf patient (Frank 2 ), a female interpreter (Lauren), a female general practitioner (Dr Curtis), and a female nurse (Naomi). Frank is a native signer of Auslan who is aged over 60. He has a variety of health problems and is a regular visitor to the practice; however, Frank has recently changed GPs and has been seeing Dr Curtis for only 2 months, so the relationship is fairly new. Lauren has more than 18 years of experience as a NAATI-credentialed interpreter. She is also the (adult) daughter of the patient, and her dual role is seen clearly throughout the interaction. It is the patient’s own preference that she interprets for him because he relies on her ability to make contextual links clear (e.g., relating a procedure to a prior experience); he had previously tried other interpreters but could not understand them, nor they him.
The consultation begins as a routine check-up; Frank has come to see Dr Curtis because of cellulitis, a bacterial infection of the skin. Dr Curtis examines his legs, as well as his ankles which are swollen, and also asks about a skin irritation on Frank’s face. In consultation with the nurse, Dr Curtis decides Frank will need IV antibiotics, which he is not happy about, but eventually accepts. They also discuss the results of other tests, and how Frank’s medication is going.
3.2.2 Recording 2
This interaction involves a female deaf patient (Pamela), a female interpreter (Sarah), and a female GP (Dr Taylor). Pamela is aged between 40 and 49 and is a fluent but non-native Auslan signer, having migrated to Australia and learnt Auslan as a child. She has diabetes and regularly visits this doctor for diabetes-related check-ups. Sarah is aged between 30 and 39 and has been working as a NAATI-credentialed interpreter for 8 years prior to participating in this study. Unfortunately, little background information about Dr Taylor is available, as she agreed to be recorded on the condition that she did not have to fill in a questionnaire or answer interview questions, because she did not have the time.
Recording 2 represents a unique opportunity to examine interaction within a doctor–patient–interpreter relationship that exhibits a high level of rapport. Pamela reports to have been a patient of Dr Taylor for more than 7 years, and Sarah has interpreted for them for more than 2 years. It is evident that the three participants have already established a good working relationship and get along extremely well.
This interaction centres on routine monitoring of Pamela’s diabetes. They begin by discussing Pamela’s blood sugar results and diabetes medication. There is confusion and subsequent clarification by all participants with regard to the two types of medications starting with a “D.” They discuss an upcoming blood test, prescriptions, and Dr Taylor explains that the dose of one of Pamela’s tablets has changed. Pamela explains about a news story she heard about, compliments the GP’s skirt, and also asks her to explain what causes strokes. There is a humorous exchange about an insurance company, and Dr Taylor reminds Pamela about an upcoming blood test.
3.2.3 Reflective interviews
Interviews were conducted individually with both interpreters and one patient (Pamela) in the weeks following the recordings. The other three participants (two doctors and one patient) were happy to have their consultation recorded but declined to participate in an interview. Interviews were semi-structured and lasted between 25 and 37 min. Questions included asking about existing relationships (e.g., “how long have you been visiting this doctor? Do you have a good relationship with them?”) as well as other specific points of interest arising from the recording (e.g., “I noticed the interpreter laughed at a joke, what did you think of this?”). Strict ethical requirements meant that video clips could not be shown to the participants, so discussions were based on transcript excerpts as well as my descriptions of what had happened. Without being able to share the primary data, it was important to conduct interviews quite soon after the appointments, while everything was fresh in participants’ minds. The trade-off was that participants did not have the opportunity to comment on detailed points of analysis, as this occurred later on. Nonetheless, they were able to provide their perspectives on preliminary findings and share their insights on the consultation, as well as relational work and interpreter role generally. Interviews were video recorded and later transcribed/translated into written English.
3.3 Analysis
All excerpts involving relational work were identified in the recordings and analysed in greater detail using IS techniques. IS has much in common with conversation analysis (CA) (Ten Have, 2007), but also attempts to “bridge the gap” between bottom-up and top-down approaches by combining micro-analytical detail with broader social contextual information (Stubbe et al., 2003). Within this analysis, particular attention was paid to the negotiation of relational work in general (Locher & Watts, 2005; Watts, 2003), as well as a focus on rapport management seen in response to face threats (Spencer-Oatey, 2000). It is acknowledged that a certain level of subjectivity is inherent in this type of approach. However, the fine-grained level of analysis also provides a much richer description of participants’ turn-by-turn moves, and their responses within the interaction provide evidence of their interpretation of others’ contributions to talk. The analysis was therefore a cyclic process that involved repeatedly watching the video data, amending transcriptions, and making analytical observations based on interactional evidence as well as insights provided in the interview data.
Both the English and Auslan were then transcribed, with Auslan signs represented in written form using CAPITAL LETTERS (a process referred to as glossing; see Johnston & Schembri, 2007). 3 The technical transcription system used in this study was built on existing transcription systems such as CA (e.g., Drew et al., 2001; Ten Have, 2007), and the system developed by the Language in the Workplace project (Vine et al., 2002). Non-linguistic features such as pausing, laughter, gesturing, and body movements were also noted; please see Appendix 1 for transcription conventions.
4. Healthcare interpreting as relational practice: results and discussion
4.1 Managing relational difficulties
Healthcare interpreters frequently encounter challenging talk such as disagreements, criticisms, complaints, or the breaking of bad news. These situations can be difficult to manage and therefore present an opportunity to examine the extent to which interpreters take responsibility for managing relationships at a local (discourse-internal) level. In potentially difficult exchanges, we might expect that speakers are more likely either to engage in face-threatening behaviour, or to mitigate actual or potential threats to face.
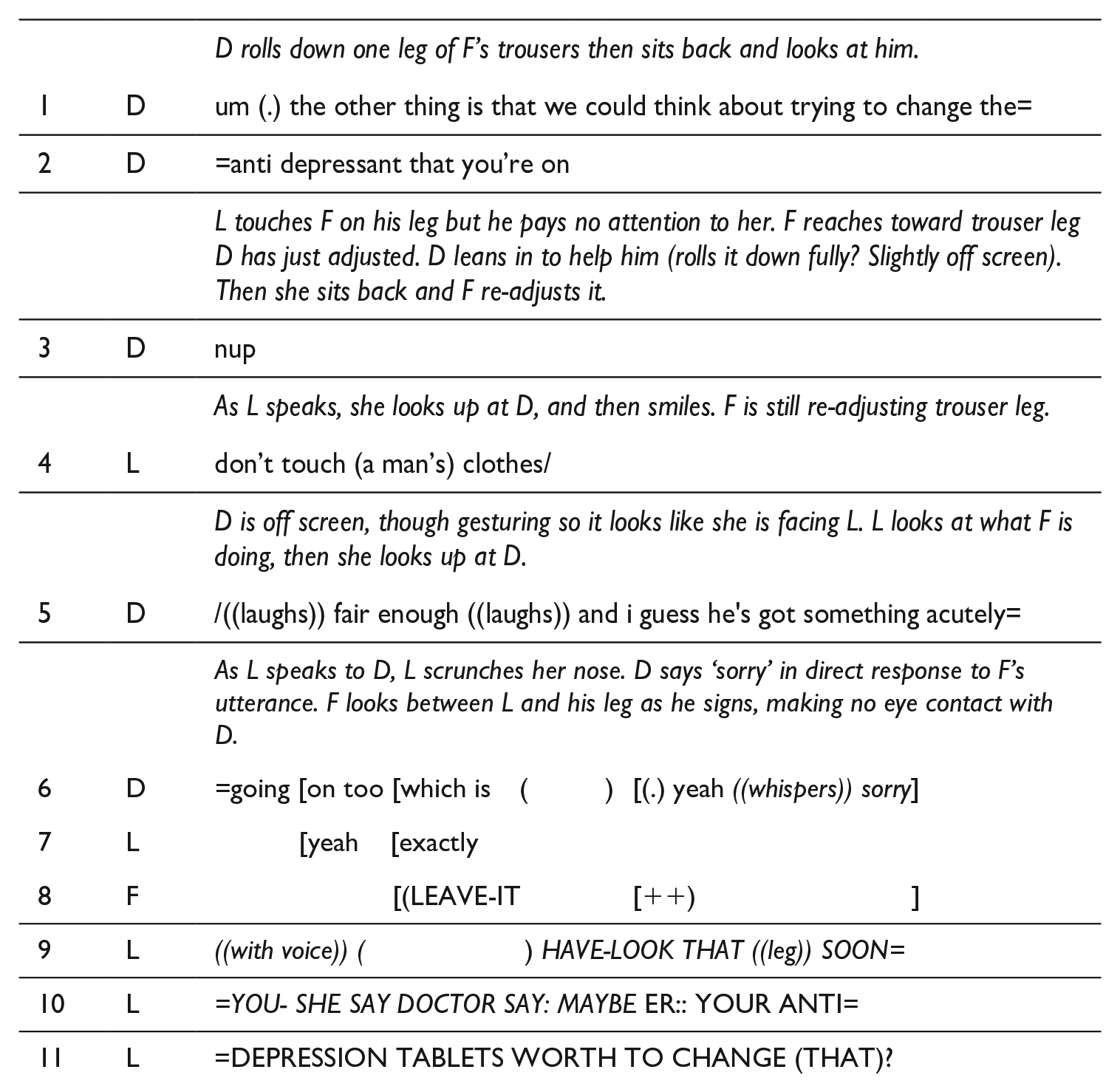
There were at least four potential face threats in Recording 1 and five in Recording 2. Excerpt 1 (from Recording 1) involves a blatant complaint from the patient, Frank, after the GP touches his clothes in a way that he is not happy with. The excerpt begins as Dr Curtis has finished examining Frank’s ankles; she leans forward to roll his trouser legs back down, while beginning a new topic of talk. First, an easy-to-read simplified version is provided so readers can understand the content. Here, the overlap is removed and the Auslan has been translated into English (indicated by underlined text). This is followed by the technical version of the transcript, which includes non-linguistic information and shows overlap (indicated by square brackets). The reader should pay particular attention to the non-linguistic information provided in the technical version, which is essential to understanding how the talk unfolds.
D = Dr Curtis, F = Frank (patient/father), L = Lauren (interpreter/daughter)
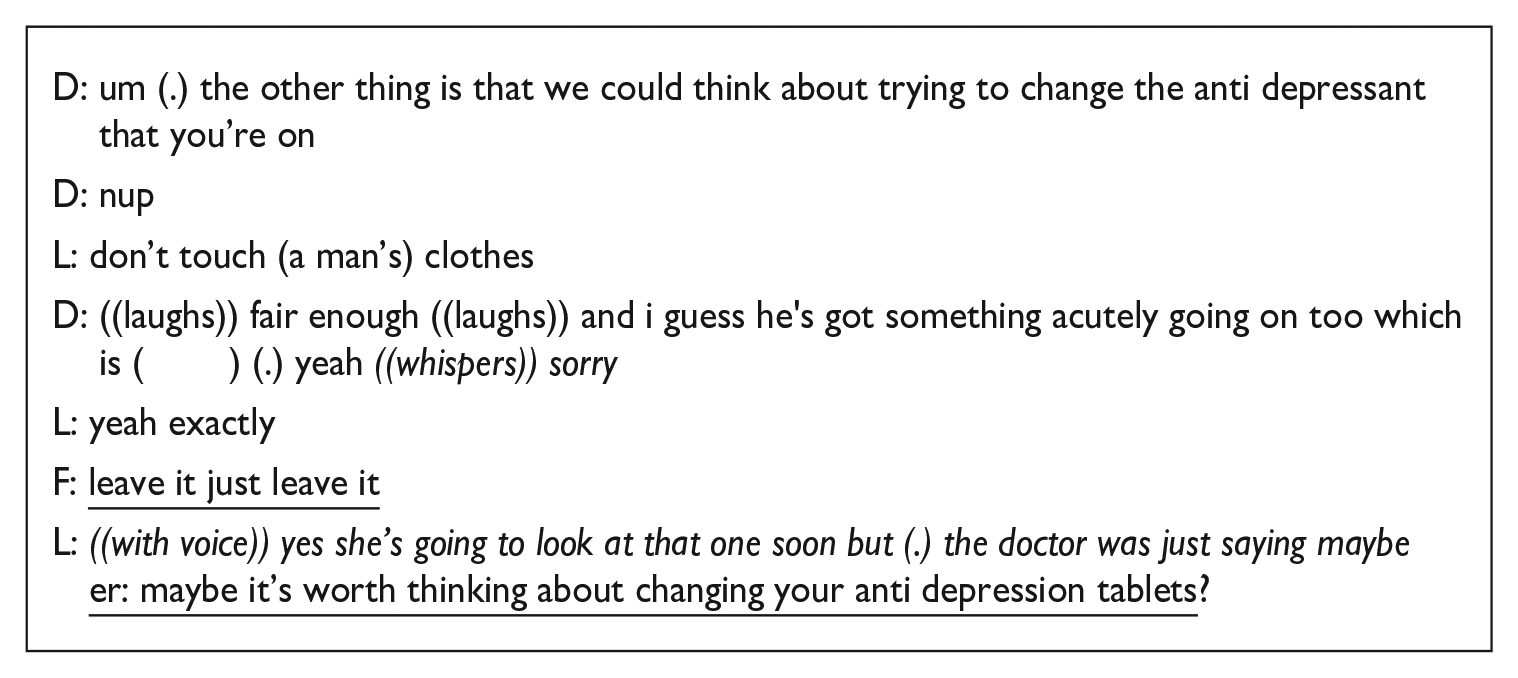
As noted in the non-linguistic information, Dr Curtis rolls down one leg of Frank’s trousers, then sits back and looks at him as she changes the topic. Frank then reaches towards the trouser leg she had adjusted, and, perhaps thinking he is in need of assistance, Dr Curtis again leans in to help him. Although we cannot see exactly what happens next, Dr Curtis has clearly made a faux pas, because she pulls back immediately and says “nup” (line 3). This self-repair shows that she is already oriented to a complaint: What-ever has happened, it is clear to her that Frank is unhappy with her actions.
Rather than conveying Dr Curtis’ self-repair to Frank, who in any case is not looking and is busy re-adjusting his trouser leg, Lauren says to the GP “don’t touch (a man’s) clothes.” While this may look on the surface like she is reprimanding the GP, a speech act that would be inherently threatening to the GP’s face, the utterance is heavily mitigated by smiling and a friendly tone of voice. Presumably her comment here is in her role as daughter rather than interpreter.
Dr Curtis appears to be doing further facework in lines 5 and 6 as she attempts to account for Frank’s complaint. She may be protecting her own face by asserting that the patient has other issues that account for his grouchiness. In addition to this, or alternatively, she could be protecting Frank’s face by acknowledging that he is in pain. In line 8, Frank makes his complaint more explicit. At this point, he is still leaning down to re-adjust his trousers, and the sign LEAVE-IT is made with a brusque and repeated sweeping motion away from him. Although Frank’s complaint is not interpreted by Lauren, it arguably does not need to be as we can see from the GP’s whispering “sorry” (line 6) right after Frank’s complaint that she understands it clearly herself. This is evidence that both interpreter and doctor are engaging in relational work.
In line 9, it is interesting to see that Lauren takes responsibility for moving the interaction forward, by re-introducing the issue of Frank’s anti-depression medication, and moving the interaction past the complaint. It is possible that she has changed the topic to further protect the GP’s face, given that that the situation has become a bit awkward. Alternatively, past experience may suggest to her that pursuing a line of apology will not progress the interaction in a productive manner, although without further evidence it is impossible to be certain. We now examine similar features in Recording 2, involving an interpreter who does not have a dual interpreter/daughter role.
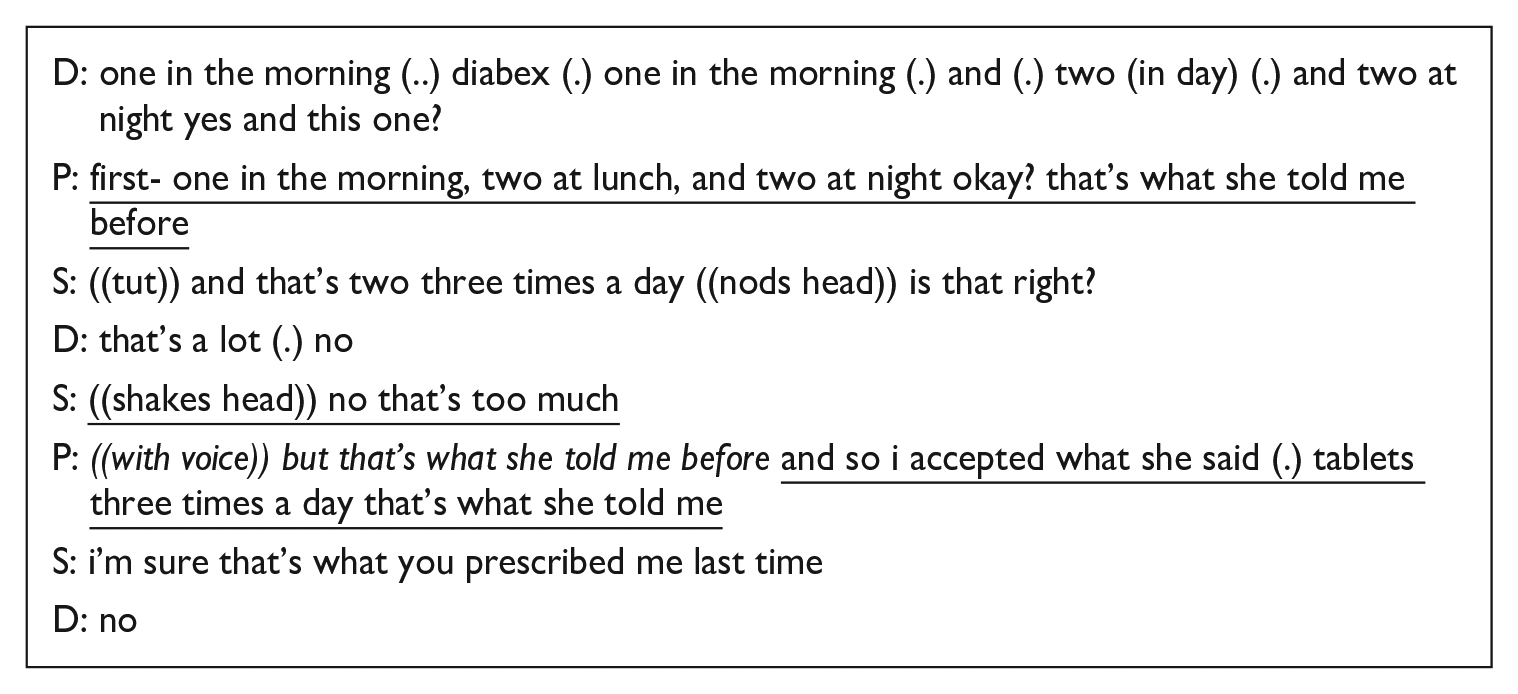
Excerpt 2 below is an exchange in which the patient directly accuses the GP of being wrong. This occurs as part of a lengthy clarification sequence in which all three participants are working together to solve confusion over Pamela’s medication doses. Here, Pamela accuses Dr Taylor of having given her wrong information. The accusation is blatant and can be considered a threat to the GP’s face.
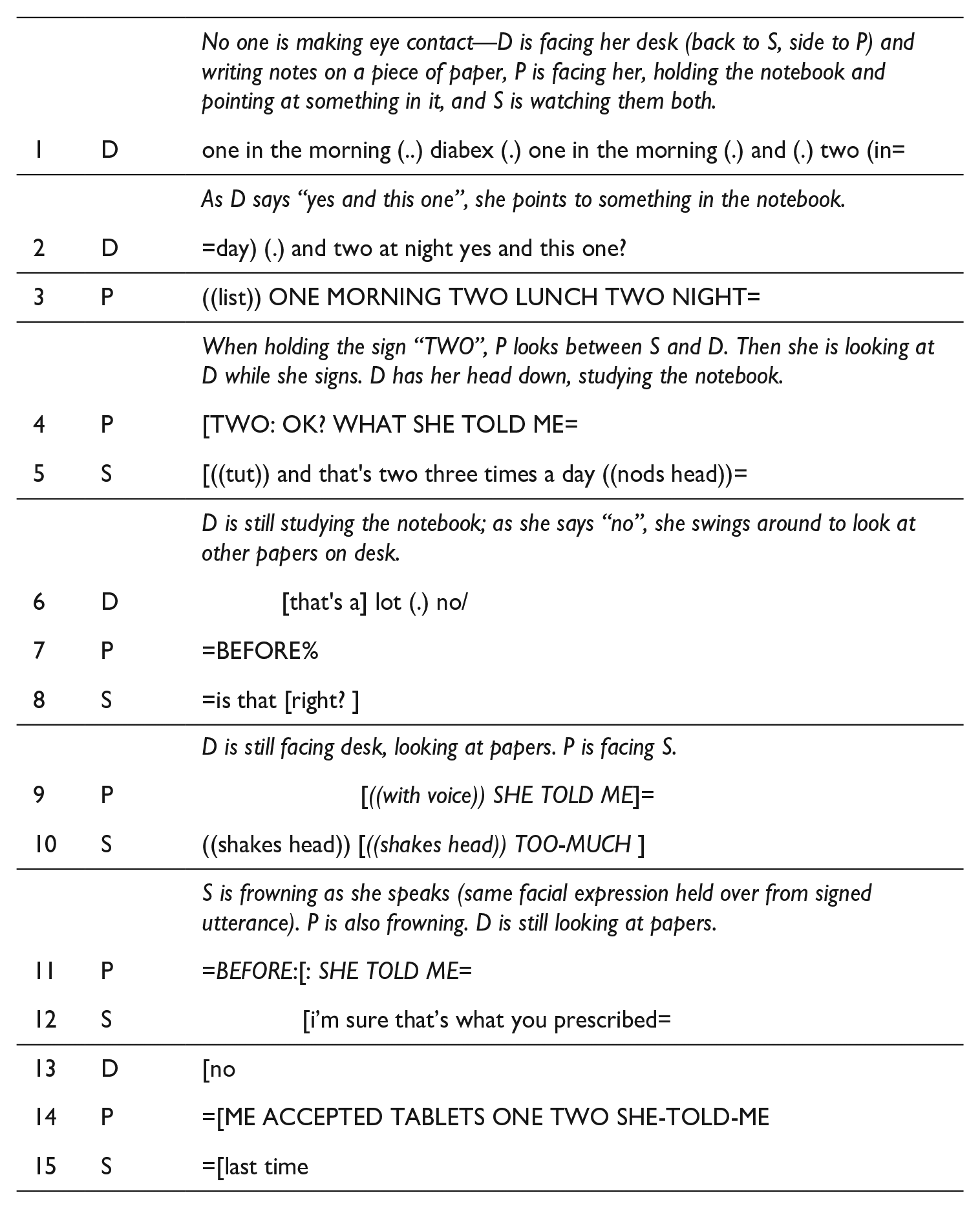
D = Dr Taylor, P = Pamela (patient), S = Sarah (interpreter)
In this excerpt, the patient directly confronts the GP, and the interpreter adds to, omits information from, and effectively changes the deaf patient’s utterance in response. This type of change can be considered unfaithful to the original message. A detailed discourse analysis, however, allows us to explore why this might have happened and consider situational factors influencing the interpreter’s response.
The excerpt begins with Dr Taylor turning to the topic of the second medication (Diamicron) in line 1. Interestingly, Pamela’s answer (lines 3, 4, 7) is already slightly defensive and may be a claim for face. That is, if she has already sensed there may be a problem, then placing the responsibility for dosage instructions on the GP (“that’s what she told me before”) allows Pamela to maintain her identity as a good and compliant patient. This also has the potential to threaten the GP’s identity face if interpreted literally, but in line 8 we can see that Sarah interprets this as “is that right?,” a question in which no potential blame is directed at the GP. This is consistent with previous research which found that interpreters sometimes tone down hostility or aggression (Dickinson, 2014; Jacobsen, 2008).
At this point, Dr Taylor is studying the notebook, not facing or making eye contact with Sarah or Pamela, and she responds “that’s a lot (.) no” (line 6). Pamela’s response, starting in line 9, is quick (before the interpretation is finished), and it is a bald and emphatic accusation: “((voice)) but that’s what she told me before and so i accepted what she said. . . .” Sarah’s interpretation of this is markedly softened. She softens the actual accusation both with the soft tone of her voice and her choice of words: “i’m sure that’s what you prescribed last time” (lines 12, 15). She further minimises a potential threat to the GP’s identity face by omitting the consequence reported by Pamela (“so i accepted what she said”). Sarah’s interpretation still holds an element of challenge, but the accusation has been heavily mitigated.
One possible explanation for her behaviour is that she is doing facework on Pamela’s behalf. If indeed deaf people are more direct than hearing people, as Hoza (2007) suggests, it is possible that Sarah is toning down Pamela’s directness to mitigate a threat that she perceives to Dr Taylor’s face. Alternatively, the interpreter could be protecting her own face: Sarah may not be prepared to convey such a bald accusation to Dr Taylor given that she also has an established working relationship with the GP.
A further explanation is that perhaps the full linguistic content of Pamela’s accusation does not need to be interpreted. While the words spoken in English by Pamela may not be articulated clearly enough for the GP to understand them (and at this point the GP is facing away from Pamela and Sarah), the tone of Pamela’s voice clearly conveys the affect of her utterance. It is possible then that the interpreter is adding only the necessary information; more would arguably be redundant, or would overemphasise Pamela’s tone, and create far more of a confrontation than originally intended.
After this (not shown in the excerpt above), Dr Taylor disagrees with Pamela and clarifies her previous instructions. There is no marked relational work in the GP’s response, suggesting that she does not view the accusation as a face threat. At the end of this sequence, Pamela realises that she has been wrong and we then see a burst of redressive rapport-oriented work; that is, a lot of apologising and explaining.
It is important to note that the two excerpts presented here are not one-off examples. Both interpreters made decisions to add to, omit information from, and change utterances during rapport-threatening exchanges. Lauren’s dual role of interpreter and daughter helps us to understand some of her decisions; at times, she takes a level of control that can be regarded as visibility at the high end of the spectrum (Angelelli, 2004). However, it is striking to see the non-family interpreter also making similar decisions. Both interpreters are very skilled and experienced practitioners, so it is unlikely these changes were a result of mistakes. Instead, they give us a detailed insight into the ways relational considerations can drive interpreter decision-making.
4.2 Maintaining positive relationships
In addition to local interactional demands, “global” factors underpin the choices participants make in interaction. This includes the desire to maintain good social relationships generally, not only as warranted by localised instances of challenging talk.
It is useful to remember here the very different characteristics of each interaction. Recording 1 is more serious in nature with the discovery of a health problem that will require a hospital visit. Two instances of humour and four instances of empathy were identified in that recording. In Recording 2, the participants get along very well and the appointment is more routine in nature. Three sections of small talk and five instances of humour were identified in this recording. The analysis below focuses on an excerpt of empathy from Recording 1, followed by an example of humour from Recording 2.
In Excerpt 3 below, Lauren produces a signed interpretation that has an empathetic tone, where none was explicit in the original utterance. This occurs approximately 3 min after the doctor has stated the need for IV antibiotics, and the patient Frank has been very clear he is not happy about a hospital visit.
D = Dr Curtis, F = Frank (patient/father), L = Lauren (interpreter/daughter)
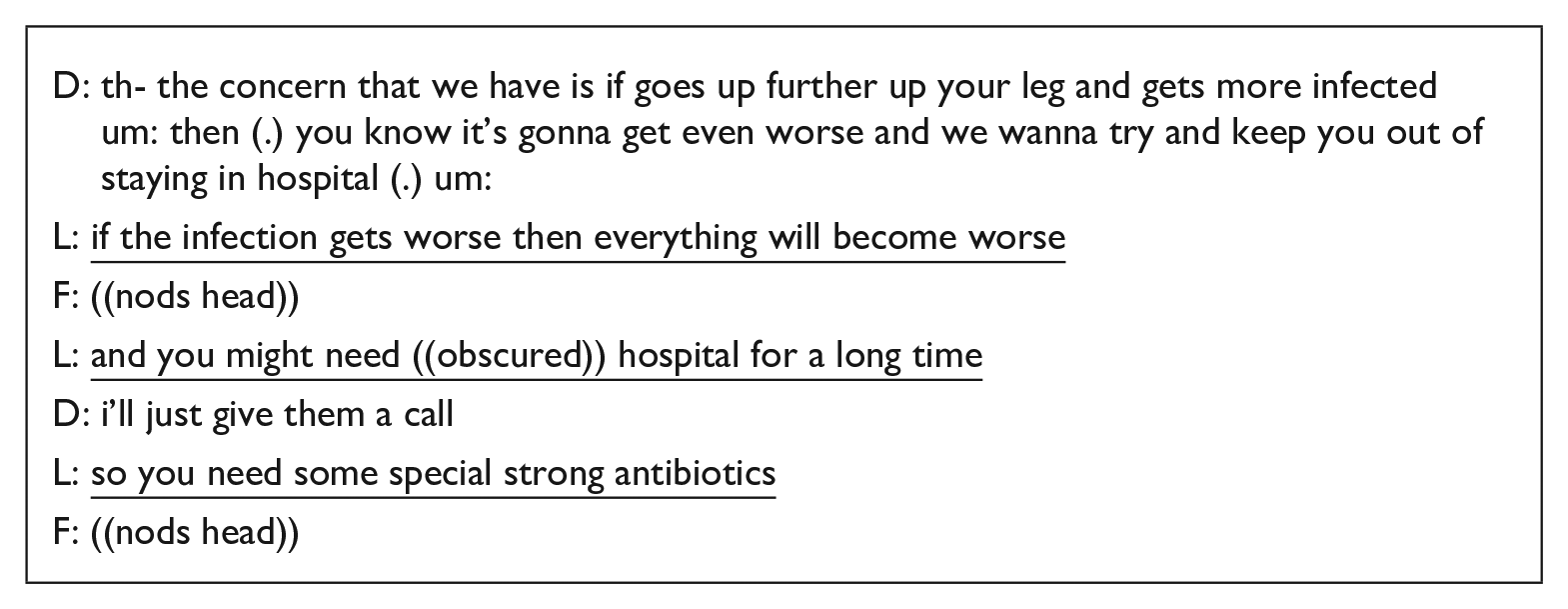
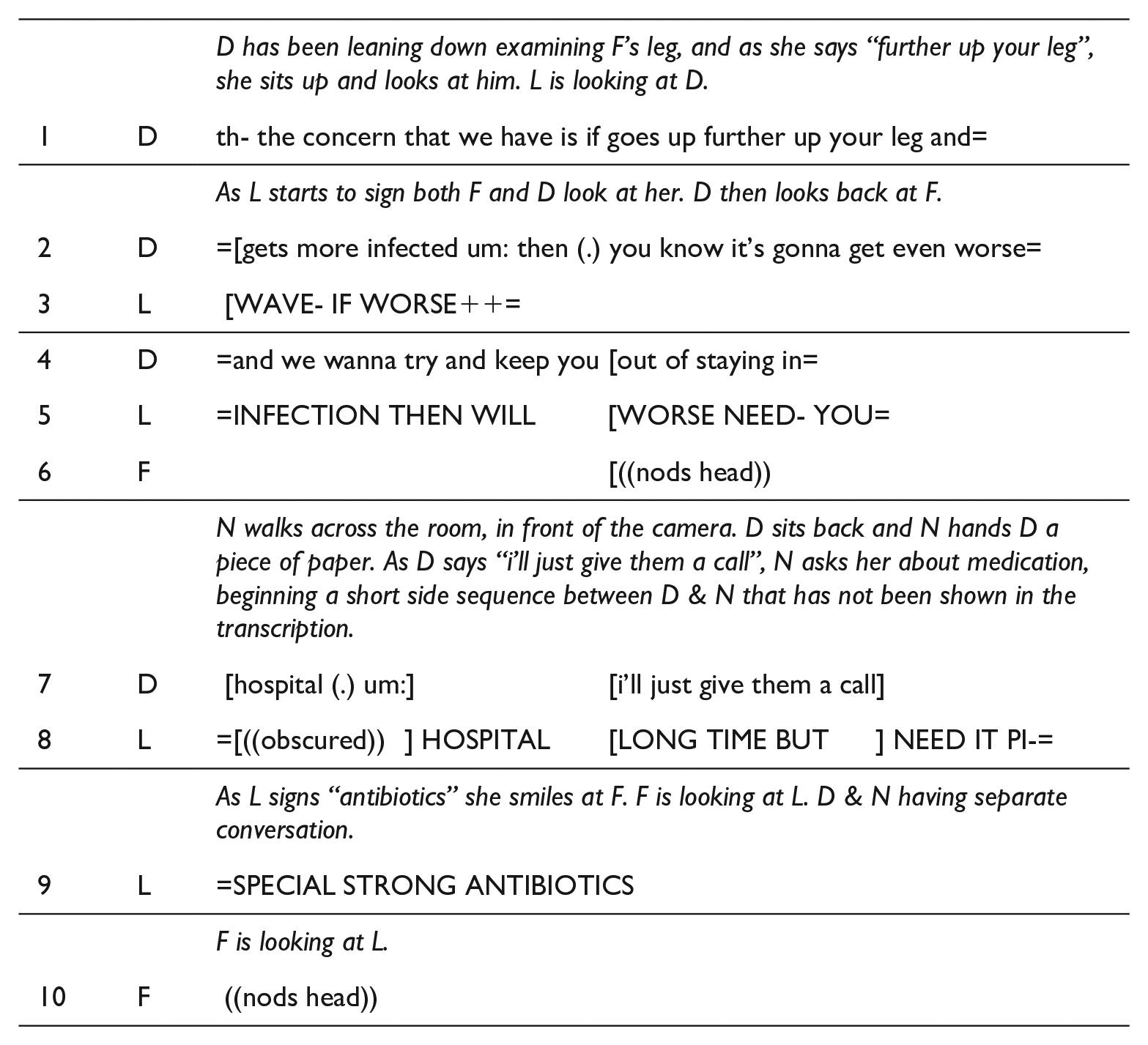
In this excerpt, Dr Curtis provides some justification for the need for IV antibiotics. Lauren’s interpretation makes an additional reference to “special strong antibiotics” (line 9). As she signs “antibiotics” she smiles at Frank, conveying empathy about the need for treatment, as everyone present is aware that he is not happy about this. There is not enough interactional evidence to know whether this empathy is solely from Lauren or whether it also captures the audibly friendly tone of Dr Curtis’ prior talk. Later on in the exchange (not shown above), Lauren continues to show empathy with the non-linguistic strategies of smiling and shrugging, and also by explicitly saying “BAD-LUCK” to him.
This example of relational work could be viewed from both a local and a global level. At a global level, Lauren’s empathetic and reassuring justification for antibiotics helps to paint Dr Curtis in a caring light, which ultimately promotes a good GP–patient relationship. Similarly, it contributes towards maintaining a good father–daughter relationship. At a local level, Lauren is likely responding to the fact that Frank is not especially happy about the prospect of more antibiotics. In a retrospective interview, she explained that she believes the GP–patient relationship is the “overall goal” and that the interpreter–patient and interpreter–GP relationships have to be strong to optimise the “most important one.” It would be interesting to know whether Lauren ever expresses this much empathy when working with other, unrelated, deaf clients or only to her father with whom she has a close relationship. There is no comparable example of empathy in Recording 2, although this would be an interesting line of enquiry for a future study with a larger dataset.
Excerpt 4 shows a humorous exchange from Recording 2 about the patient’s insurance company. This excerpt illustrates Sarah both interpreting and subtly engaging in the exchange herself. To provide some context to this humour: Sarah and Pamela both later explained that there had been an ongoing issue with Pamela’s insurance company in relation to a medical claim. The insurance company’s lack of action had become an in-joke, with frequent references to whether the insurance company has a pulse or not. This excerpt occurs near the end of the consultation as Dr Taylor is preparing prescriptions and organising her paperwork.
D = Dr Taylor, P = Pamela (patient), S = Sarah (interpreter)
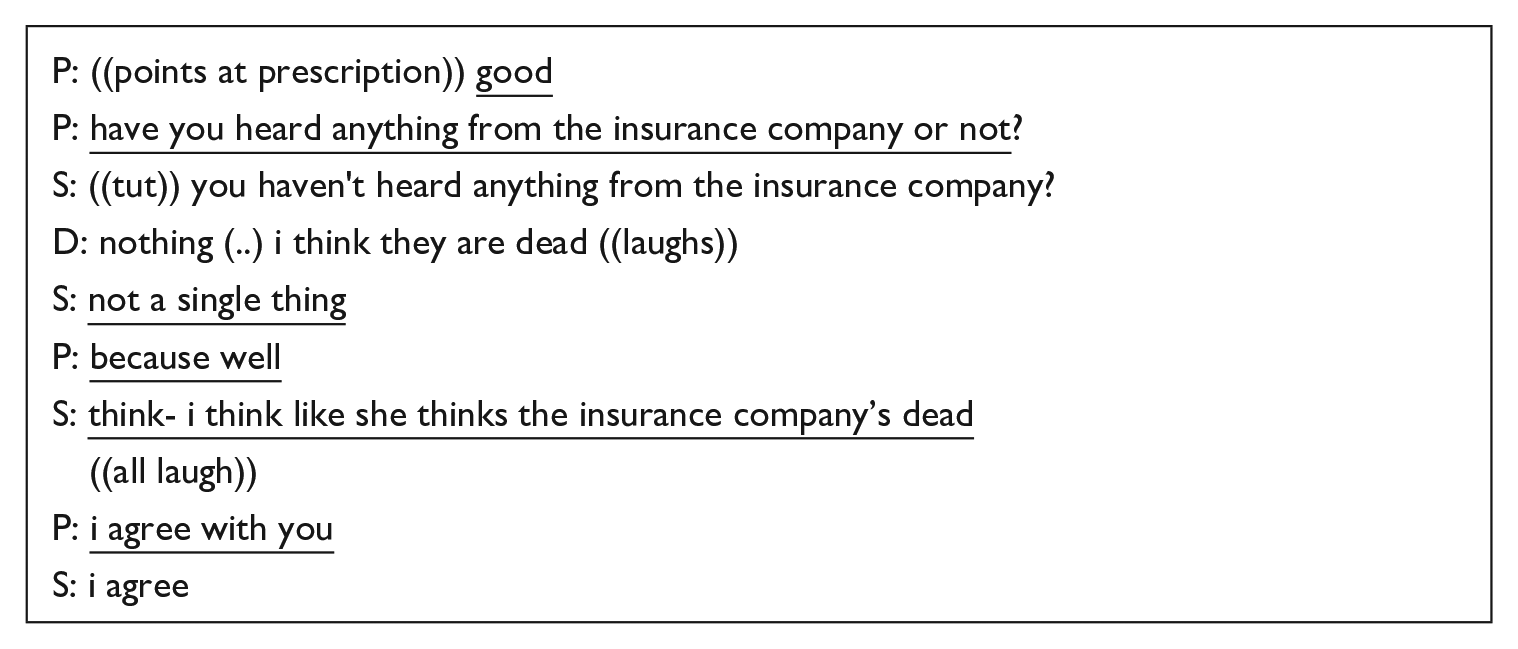
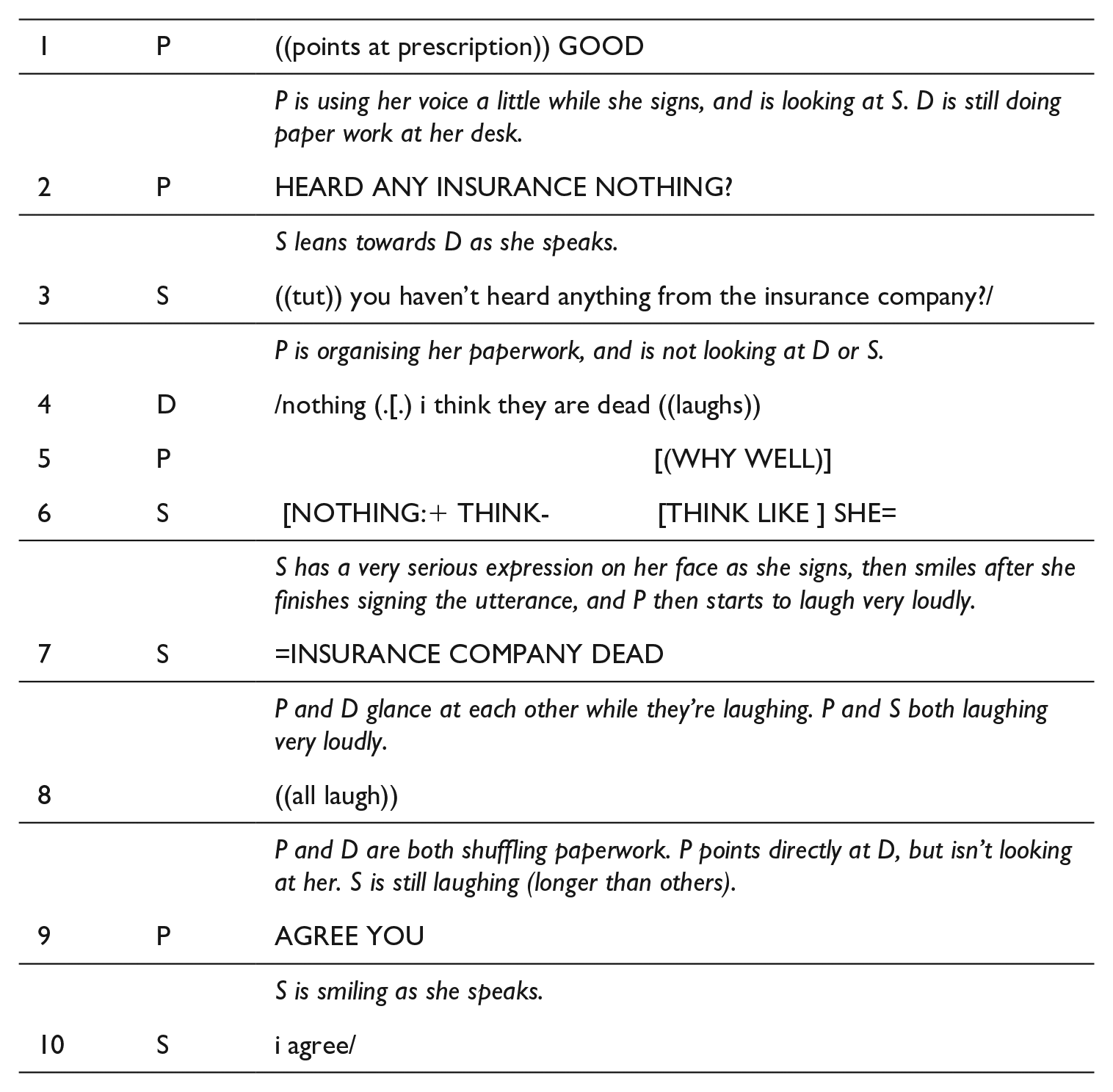
As Pamela is packing up her paperwork, she asks if the GP has heard anything from the insurance company (line 2), which is interpreted. Dr Taylor immediately responds with a negative answer to Pamela’s question, followed by a joke: “nothing (..) i think they are dead” (line 4). She also then laughs very loudly. At this point, Pamela is again focused on organising her paperwork and so she is not alerted to the humorous tone by seeing Dr Taylor’s laughter. This also accounts for Sarah’s “NOTHING:+” (not a single thing) (line 6). While it may look as if Sarah has missed the humour, she is simply waiting to get Pamela’s attention before delivering the joke. Sarah’s signing attracts Pamela’s attention and then the joke is conveyed (lines 6, 7). Sarah conveys the irony with a very serious look on her face as she signs, followed by a smile at the end of her utterance. Her facial expression is an important cue in alerting the patient to a shift of tone or “frame.”
All three participants then laugh. Sarah is clearly engaging in the humorous exchange herself as an individual, which is similar to Wadensjö’s (1998) study in which an interpreter was seen to engage in humour by laughing at a nurse’s joke. It is important to note, however, that Sarah delays her own laughter until the joke has been conveyed to Pamela. In an interview with Sarah afterwards, she stated that this is an important part of maintaining her own ongoing relationship with the patient and the GP. She explained, “I think they would think it’s strange if I didn’t laugh, you know I think they want me to be as much of a participant as I want to be.” Pamela also felt strongly that humour and small talk are a very important part of her appointments: “That kind talk stops people griping or feeling uneasy and without it I would feel uncomfortable. It’s good when deaf people can talk to their doctor like that.”
5. Summary and implications
The excerpts analysed in this article highlight the high value participants place on positive relationships and some of the ways skilled interpreters facilitate this aspect of communication in a health setting. The analysis supports Merlini’s (2013) assertion that politeness is not only about responding to face threats; in some settings the overall aim is supportive, and interpreters are attuned to this (see also Mapson, 2016; Mapson & Major, 2021). Both interpreters in this study were seen to influence the flow of the interaction and mitigate face-threatening utterances. They actively encouraged others’ attempts at relational work and participated in it to a small degree. Both interpreters were aware of their involvement in relational work and were clear about their reasons for engaging in it. As a consequence, “relational practice” was an integral part of their role in these interactions.
A limitation of this study was that interviews were conducted prior to the more fine-grained analysis. In a future similar study, it would be ideal to re-present the more detailed findings to participants and explore the extent to which they align with participant perceptions. It would also be valuable to examine health interactions where participants are meeting for the first time. The analysis presented here suggests that familiarity plays an important part: Although a different and unfamiliar interpreter’s involvement would unlikely have compromised Pamela’s ability to understand information about her own health, the nature of relational work surely would have changed. The humorous exchange seen in Excerpt 2, for example, relied heavily on all participants’ background knowledge of the long-running joke about the insurance company.
The study supports others’ claims that interpreters in this setting align to and balance clinical, linguistic, and interpersonal goals (Bolden, 2000; Davidson, 2002; Major & Napier, 2019), and actively facilitate and to some degree engage in relational work (e.g., Allison & Hardin, 2020; Chang et al., 2021; Delizée & Michaux, 2022; Hemingway, 2023; Mapson & Major, 2021; Rodríguez-Vicente, 2021). This study provides further evidence that interpreters can be very powerful agents in the decisions they make and their ability to drive the direction of an interaction.
Hale (2007) and Tebble (1996) have claimed that interpreters should convey every turn at talk in the tone it was expressed. There are sound ethical reasons for this being our starting point; participants must be able to trust that they can fully and accurately access talk that is mediated by a professional interpreter. However, it must be acknowledged that skilled, experienced interpreters do at times diverge from “faithful” interpretations in this context, and not because of a lack of skill (at least in the excerpts shown here), but for reasons that relate directly to the maintenance of relationships. This aspect of the healthcare interpreter’s role cannot be ignored, particularly in a context where real health outcomes can rely on good rapport between participants.
That is not to say that modifying others’ talk is always appropriate or acceptable in this setting. Interpreters must constantly reflect on their own behaviour, questioning whether their actions empower service users and are in line with the values of their professional Code of Ethics. To engage in these discussions, we need more analyses of naturally occurring data, so that we can continue to develop our understanding of the context-bound reasons behind such decisions. If we continue to focus solely on interpreting as a pursuit of message equivalence, then we are severely limited in preparing interpreting students for real-world challenges and the complexity of interpreter role. We need to acknowledge that relational work is not just a lovely and optional extra factor, but rather an integral part of the healthcare interpreter’s role.
Footnotes
Appendix
Acknowledgements
The study reported here was undertaken as part of my doctoral research at Macquarie University in Sydney. I would like to express my gratitude to all participants as well as my supervisors Jemina Napier and Maria Stubbe, my Auslan advisor Stef Linder, and Janet Holmes for her feedback on an earlier version of this article.
Declaration of conflicting interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was financially supported by an Australian Postgraduate Award (Industry) from the Australian Research Council. The study was granted approval by the Macquarie University Human Research Ethics Committee (HE28NOV2008-D06201 and 5201000559) on 6 February 2009 and the Royal Australian College of General Practitioners National Research and Evaluation Ethics Committee (RACGP NREEC 09/010) on 19 October 2009.