
Abstract
Artificial intelligence (AI) has attracted much public interest, inspiring both hopes and fears. As countries define pathways for developing and implementing AI, healthcare is emerging as a priority sector. Sociotechnical imaginaries, which can mobilize public support and attract resources for realising sociotechnical visions, play an important role in the trajectories of emerging technologies. News media, in turn, are central to the negotiation, construction, and promotion of such imaginaries. We analyze how news media construct sociotechnical imaginaries of AI in healthcare in China, Germany, and the United States (US), three countries with differing healthcare and media systems, and sociopolitical and -cultural outlook on technologies. Drawing from a thematic analysis of articles from 15 newspapers, we find two powerful, cross-national, collectively held imaginaries: The first imaginary on enhancing healthcare with AI emerged across all three countries; the second imaginary on using AI to manage pandemics or epidemics was only fully developed in Chinese and US coverage, though present as an outlier in German news coverage. Lower-level divergences within each imaginary can be explained by systemic differences between the countries, such as the largely private US healthcare system, the mostly state-controlled Chinese media and healthcare systems, and the German hesitancy toward emerging technologies. This study provides evidence for how powerful imaginaries can emerge across very different sociopolitical and cultural contexts while accounting for contextual national factors.
Keywords
Introduction
Artificial intelligence (AI) has attracted much public interest, inspiring both hopes and fears (Cave & Dihal, 2019; Cools et al., 2024). As countries have started to define their preferred pathways for the development and implementation of the technology, healthcare has nearly universally emerged as a priority sector in AI strategies (Fatima et al., 2020; Galindo et al., 2021), with countries aiming to utilize the technology to tackle widespread challenges: Globally, there is a shortage of healthcare workers, their workloads and stress have intensified, the quality of healthcare is expected to sink, and health inequalities are expected to rise. Ageing populations and chronic diseases put further stress on healthcare systems (Bohr & Memarzadeh, 2020c, Hazarika, 2020; Jeddi & Bohr, 2020). AI has been discussed as part of the solution, with the World Health Organisation (2021) both “recogniz[ing] that AI holds great promise for the practice of public health and medicine” and cautioning of “potential serious negative consequences” if ethical challenges are not addressed.
The implementation of emerging technologies in critical parts of society, like AI in healthcare, is reflected in news media, which disseminate information, set public agendas, influence public perception and behavioral intentions (Brossard, 2013; Pjesivac et al., 2020; Schiff, 2024) and can shape the trajectory of technological developments by representing visions of socio-technical futures (Vicente & Dias-Trindade, 2021; Pentzold et al., 2020). Such visions have been conceptualized as sociotechnical imaginaries (SIs) (Jasanoff, 2015): “collectively held, institutionally stabilized, and publicly performed visions of desirable futures [or resistance against the undesirable], animated by shared understandings of forms of social life and social order attainable through, and supportive of, advances in science and technology” (Jasanoff, 2015, pp. 4, 19). SIs can mobilize public support and attract resources for realising socio-technical futures (Bareis & Katzenbach, 2022).
This paper analyzes news media imaginaries of AI in healthcare and compares how they are constructed in three countries striving for global leadership in AI: China, Germany, and the USA. The USA and China have invested heavily in the technology (Goldman Sachs, 2023; Shen et al., 2022), while Germany announced a national AI strategy to catch up with global leaders (Buck, 2018). But the three countries also have contrasting cultural and political outlooks on technology (Jasanoff, 1995; Simon & Goldman, 1989), dissimilar healthcare systems (Chen & Liu, 2023; Hennes et al., 2015), and different discursive opportunity structures (Ferree et al., 2002; Zhao, 2012) for the emergence and propagation of SIs. We assess to what extent these differences translate into imaginaries of AI in healthcare and who shapes their construction in news media.
Conceptual framework and literature review
Conceptual framework
This study is framed by the SIs concept (Jasanoff, 2015), complemented by scholarship on public communication about technologies (PCT) (see Figure 1). The SIs concept aims to explain how technologies develop depending on their socio-political and socio-cultural context. Hence, SIs are context-specific, “culturally particular,” “temporally situated,” materially bound, and spatially anchored (Jasanoff, 2015, p. 19). We derive several key elements from Jasanoff's (2015) conceptualization of SIs: the future role prescribed to the technology; the specific AI technology the vision surrounds; and a desirability evaluation, i.e., whether the vision is seen as (un)desirable, which entities are (un)desirably affected, and based on which rationale it is seen as (un)desirable.
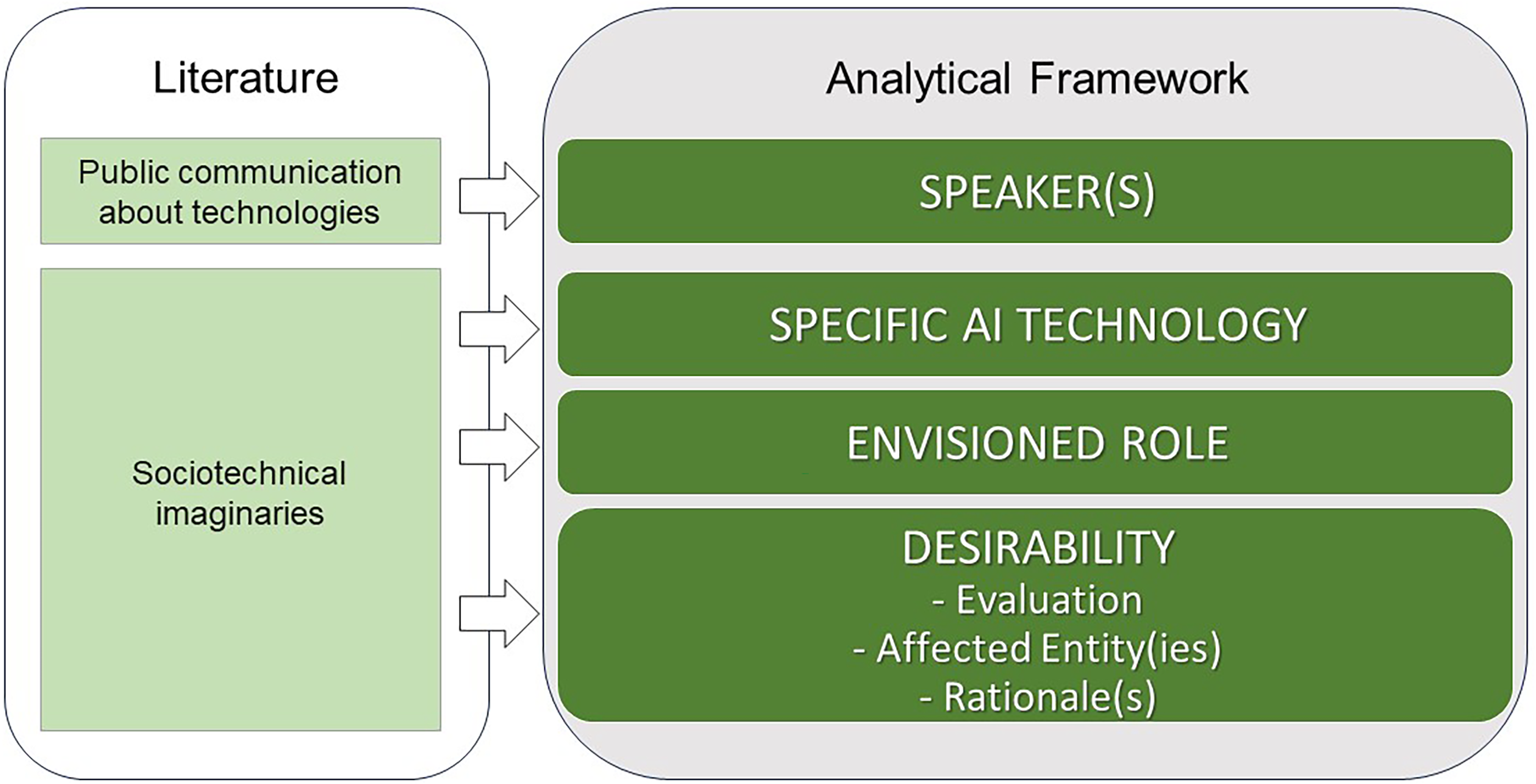
Conceptual framework.
We complement this with scholarship on PCT to account for the specificities of news coverage. While Jasanoff (2015) defines SIs as “publicly performed” (p. 4) and mentions their “expression in the mass media” (p. 27) as one facet of their performance, SI scholars often underestimate the role of news media as an arena of competition for public visibility and hegemony (Richter et al., 2023). PCT scholars have formalized this competition between different speakers, frames, and discursive positions about technologies in the public sphere (Ferree et al., 2002; Gerhards & Schäfer, 2006; Hilgartner & Bosk, 1988). We propose that imaginaries similarly emerge from this competition for visibility by speakers and their interpretations of emerging technologies. Therefore, drawing particularly from the concept of scientific public spheres (Ferree et al., 2002; Gerhards & Schäfer, 2009), we derive an additional speaker element to investigate who gets to express their views and contribute to the construction of AI healthcare imaginaries in Chinese, German, and US news.
Previous literature on AI in healthcare and related news coverage
AI in healthcare
Medical scholars have described the role AI can occupy in healthcare, the specific AI technologies involved, and their potential (un)desirability for different affected entities. They have also highlighted important stakeholders, which could be relevant speakers in public debates.
Scholars have discussed the potential role of AI in healthcare. Centrally, AI is described as increasing the speed and efficiency of healthcare processes with human-level or superior accuracy (Bohr & Memarzadeh, 2020a; Topol, 2019). This could enhance and facilitate both clinical and non-clinical healthcare processes, including diagnosis, prognosis, and treatment on the clinical side, and administration, patient communication, drug research and development, and remote patient monitoring on the non-clinical side (Bohr & Memarzadeh, 2020a; Saxena et al., 2023).
Research has considered various AI technologies involved. These can be broadly split into underlying technologies, medical AI applications, or applications adapted for medical use. AI-underlying technologies include machine learning, deep learning, machine vision, or natural language processing (Bohr & Memarzadeh, 2020a). Medical applications or applications adapted for medical use are, for instance, medical image recognition, clinical decision support systems, or health chatbots (Bohr & Memarzadeh, 2020b; Jeddi & Bohr, 2020).
Regarding the potential (un)desirability of AI in healthcare, literature has produced ambiguous assessments for patients and medical professionals, but also for the healthcare system. For patients, AI use could decrease risk of harm, improve treatment outcomes and patient autonomy, and enable cost savings and access to higher quality care (e.g., Jeddi & Bohr, 2020; Topol, 2019; Witkowski & Ward, 2020). However, risk of harm to patients could increase if the AI is faulty, and patients could experience discrimination and loss of agency due to an overreliance on AI (Morley et al., 2020; Topol, 2019). Similarly, for medical professionals, AI could improve working conditions, e.g., through reduced administrative and diagnostic workload and help reduce medical errors and negative outcomes (e.g., Hazarika, 2020; Tran et al., 2020; Witkowski & Ward, 2020). But AI use could also worsen malpractice and liability risks if the AI is faulty and bring about a deskilling and loss of agency of practitioners due to overreliance on AI, difficulties to interpret AI outputs, or conflicts between machine recommendations and human judgment (e.g., Hazarika, 2020; Morley et al., 2020; Topol, 2019). The healthcare system could benefit from cost savings and a greater ability to balance increasing demand with shrinking workforces, but potentially inaccurate measurements prompting unnecessary medical visits also introduce ambiguity (Topol, 2019; Tran et al., 2020).
Regarding speakers, research has highlighted several stakeholders regarding AI in healthcare. They include policy makers and regulators; healthcare providers, such as hospitals, physicians, and AI implementers and users; patients; and innovators, including incumbents like pharma and insurance companies, and disruptors like med-tech and IT companies including both Big Tech and start-ups (Hlávka, 2020; Landers et al., 2023). Notably, Ozalp et al. (2022) argued that Big Tech companies have “digitally colonized” healthcare, making them central players.
News coverage of AI in general and in healthcare
Scholarship on AI news coverage in general has shown an increase in coverage of AI over time (Chuan et al., 2019; Fast & Horvitz, 2017) and identified prevalent topics, frames, and evaluations of AI, as well as the most prominent speakers. It generally found a prevalence of business and economic themes (e.g., Chuan et al., 2019; Zeng et al., 2022), overwhelmingly positive sentiment and evaluations (e.g., Vergeer, 2020; Zeng et al., 2022) and a strong presence of industry actors (e.g., Chuan et al., 2019; Sun et al., 2020). It also identified healthcare as an important topic in large, AI-centric news corpora in the USA and UK (Cools et al., 2024; Nguyen & Hekman, 2022; Sun et al., 2020; Wang et al., 2023), China (Wang et al., 2023), the Netherlands (Vergeer, 2020), and Portugal (Canavilhas & Essenfelder, 2022).
Beyond such large-scale analyses, however, studies of news coverage about AI in healthcare are scarce. Duberry and Hamidi (2021) found that in April 2020, due to different peaks of pandemic risk perceptions internationally, the New York Times covered AI more positively and unrelated to COVID-19, while European newspapers balanced positive and negative reporting about the use of AI against the pandemic. Bunz and Braghieri (2022) found a representation of AI as outperforming doctors in the USA and the UK.
Analyses of news coverage of AI imaginaries are similarly scarce. Wang et al. (2023) merely used SIs as a sensitizing concept to analyze AI narratives in news. Hansen (2022) analyzed depictions of human-machine relationships in imaginaries in Danish AI-centric news and found the co-existence of a human-centric vision of AI as amplifying human abilities and a technology-centric vision of AI as replacing humans.
Research interest and questions
Hence, comprehensive analyses of SIs of AI in healthcare do not yet exist, particularly in a comparative perspective. We provide such an analysis, comparing AI healthcare imaginaries in three countries’ news: China, Germany, and the USA. We explore the following research questions (RQs):
Methodology
Research design
The article proposes a most-different-systems study (Mills et al., 2010), comparing imaginaries of AI in healthcare in China, Germany, and the USA. Hence, we explore whether similar imaginaries emerge in the news coverage of three countries despite their systemic differences in relevant aspects for the construction of AI healthcare imaginaries. Comparable outcomes within each country could mean that the vision of AI for tackling healthcare issues is “collectively held” (Jasanoff, 2015), reflective of its priority status in national strategies (Fatima et al., 2020; Galindo et al., 2021), and independent of systemic differences across the three countries. We propose that China, Germany and the USA differ in three relevant aspects for the construction of news media imaginaries of AI: their healthcare systems, outlooks on technology, and media systems (see also Table 1).
Characteristics of three country cases: USA, Germany, and China.
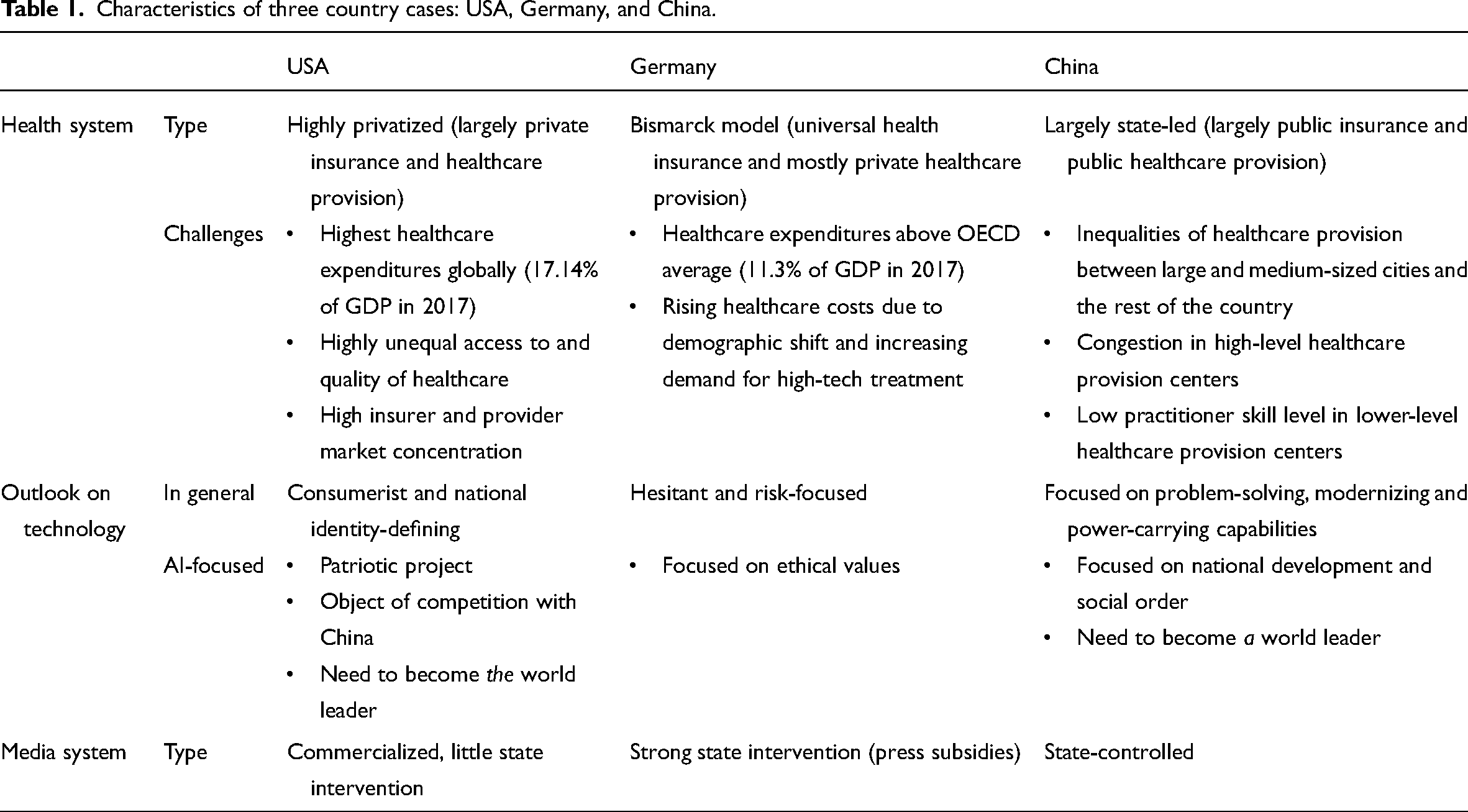
In terms of healthcare, the three countries differ in their level of privatization and the health systemic challenges. The USA represents a highly privatized system with largely private insurance and healthcare provision (Cacace, 2010; Hennes et al., 2015). Challenges include high healthcare expenditures, high market concentration among healthcare providers and insurers, and unequal access to and quality of healthcare (Fullman et al., 2018; Fulton, 2017; Hennes et al., 2015). Germany has universal health insurance and mostly private healthcare provision. Its system is threatened by rising costs from an ageing population, a shrinking workforce, and an increasing demand for high technological medical treatment (Hennes et al., 2015). China's largely state-led healthcare system hosts state-run insurance for 95% of its population and provides care chiefly through state-owned hospitals, but also urban community and rural township health centers (Chen & Liu, 2023; Wang, 2009). The government controls management and operation of state-owned hospitals (Wang, 2009). Challenges are the uneven distribution of high-quality care between larger cities and the rest of the country, congestion in high-level healthcare centers, and low practitioner skills in lower-level centers (Chen & Liu, 2023; Sun et al., 2016).
Regarding the sociocultural and sociopolitical outlook on technology, the USA has historically had a consumerist and national identity-defining relationship to technology (Nye, 1996), now re-enacted and amplified in its AI policies, where AI represents a patriotic project and an object of explicit competition with China, in which the USA needs to be the world leader (Bareis & Katzenbach, 2022; Hine & Floridi, 2022). In comparison, post-war Germany has been more hesitant toward new technologies, focusing strongly on risks (Jasanoff, 1995). German AI policy has focused on promoting ethical values under the “AI made in Germany” banner (Bareis & Katzenbach, 2022). China's post-Maoist approach to technology has centered on its potential for concrete problem-solving, and for bringing about modernity and global power (Greenhalgh, 2020; Simon & Goldman, 1989). This is reflected in its AI policies, which focus on national development, social order, and becoming a world leader (Bareis & Katzenbach, 2022; Hine & Floridi, 2022).
The countries’ media systems differ regarding the level of state involvement. The US system is strongly commercialized with little state intervention, the German system is shaped by strong state interventions through subsidies (Hallin & Mancini, 2004) and the Chinese system is largely state-controlled, containing both state party outlets and commercial outlets acting under political constraints (Lee, 2015; Zhao, 2012).
Data collection and analysis
We analyze five newspapers per country (see Table 2 for search strategy), selected for national scope in target audience and editorial focus, wide circulation, domestic headquarters, and viewpoint diversity (conservative vs. liberal for the USA and Germany, state-owned vs. commercial in China) (see Appendix 1 in the online supplementary materials). Where possible, we included print and digital editions. The timespan from 2012–2021 was selected to cover the years of increasing news interest in AI (Chuan et al., 2019).
Article Search Strategy.
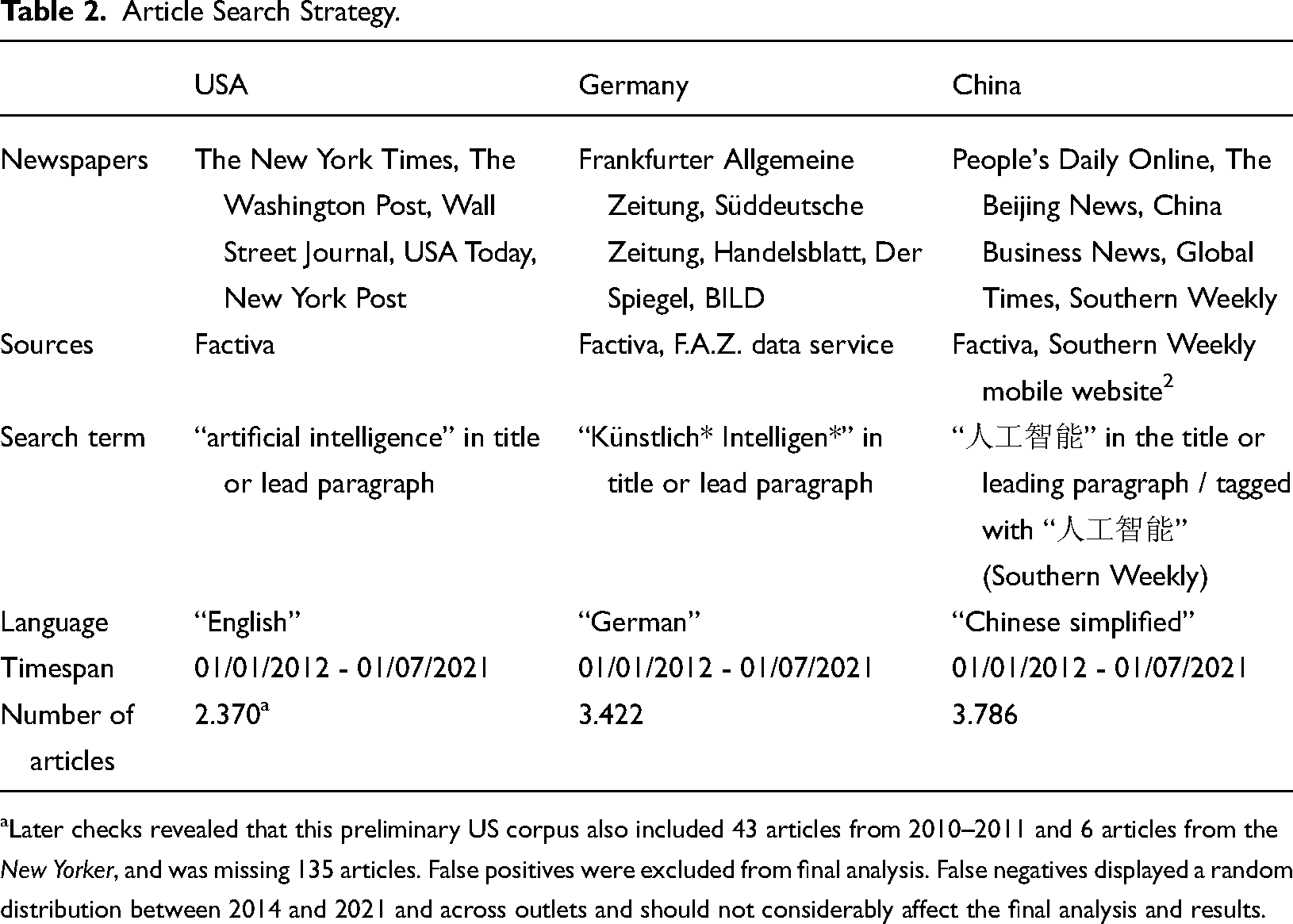
Later checks revealed that this preliminary US corpus also included 43 articles from 2010–2011 and 6 articles from the New Yorker, and was missing 135 articles. False positives were excluded from final analysis. False negatives displayed a random distribution between 2014 and 2021 and across outlets and should not considerably affect the final analysis and results.
To focus the qualitative analysis, each corpus was pre-analyzed through LDA-topic modeling (Blei et al., 2003). One healthcare topic emerged in each topic model, from which articles with a minimum 50% topic fit were selected for further investigation. Articles were further filtered for a strong focus on AI through a minimum keyword count (details in Appendix 2 in the online supplementary materials). The final corpora consisted of 26 articles for the US, 25 articles for the German, and 38 articles for the Chinese case, excluding duplicates and outliers. Articles from these corpora were sampled up to theoretical saturation starting from the articles with the highest topic fit.
Thematic analysis was performed in MaxQDA, taking the analytical framework's six elements as “analytical objectives” (Guest et al., 2012). US and German articles were coded by the first, Chinese articles by the second author. Coders also wrote summary memos for each article in English. Interpretation discrepancies were discussed and resolved between both.
Each article was first scanned for markers of future-orientation, such as “will,” “could,” “may,” “in the future,” and the existence of at least one “envisioned role” for AI. Sampling continued until themes for the “role” element emerged. Two “role” themes were identified for the US and Chinese, and one for the German case, with theoretical saturation reached at 14 articles in the USA, 16 in the German, and 15 in the Chinese case (Appendix 3 in the online supplementary materials). Duplicates and outliers were excluded from further analysis. Articles were regrouped according to these themes and thematic analysis was performed for the other analytical elements related to each “envisioned role.” Notably, while the number of articles underlying the results may seem small, a single article could contain more than one “role description” and typically included several different mentions of the other analytical framework's elements.
Results
We identified two imaginaries of AI in healthcare in the USA, two in China, and one in Germany, which shared similarities across countries, but also exhibited differences.
Imaginary 1: Enhancing healthcare
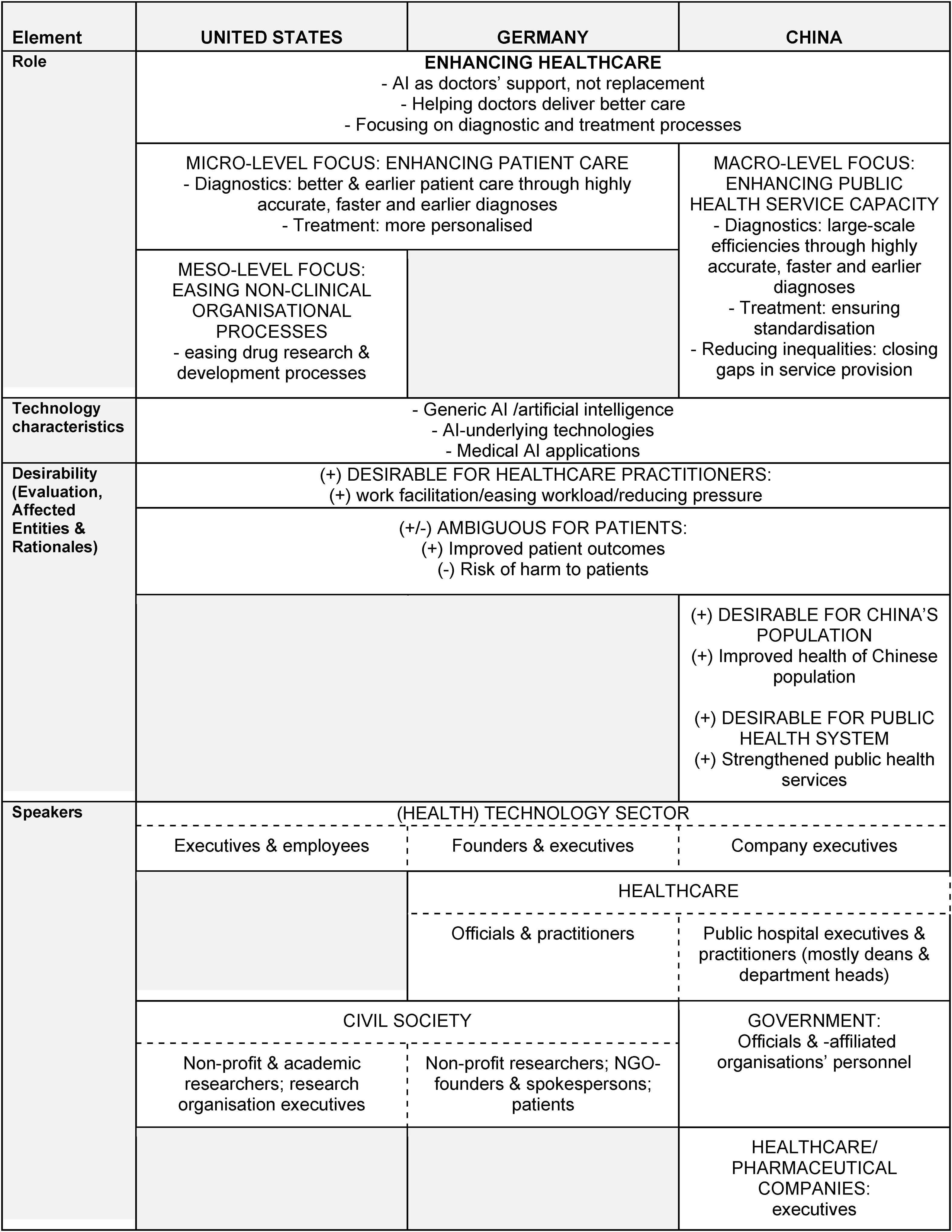
The first imaginary—found in all three countries—centered on enhancing healthcare (see Table 3). The imaginary emerged in a comparable timeframe across all three countries: Articles promoting the imaginary appeared from 2018 in the USA, and 2017 in Germany and China, and up to the end of our period of analysis in mid-2021. The vision evolved around “AI” in general, its underlying technologies, and specific medical applications for diagnostics and treatments, but also emphasized that doctors will remain irreplaceable. It was considered desirable for healthcare practitioners, but ambiguity was expressed regarding the vision's impact on patients. The US variant of the imaginary—constructed by technology sector and civil society speakers—linked the AI-enabled enhancements to individual patient care and included the possibility of using AI for drug research and development. The German version was promoted by technology sector, civil society, and healthcare sector speakers, and similarly emphasized the enhancements at individual patient level. The Chinese imaginary included speakers from the technology, healthcare, pharmaceutical, and government sectors and envisioned enhancements more in terms of service capacity and standardization across the country. Furthermore, the Chinese imaginary promoted the nation's population and public health system as expected beneficiaries.
Overview of the First Imaginary in US, German, and Chinese News.
Role
The envisioned role for AI in healthcare bore several similarities but differed in one crucial aspect between Germany and the USA on the one side, and China on the other. Similarities related to the overall vision of enhancing healthcare, the central role of doctors, and the focus on diagnostic and treatment processes. However, differences emerged regarding the societal level in focus. Indeed, US and German coverage emphasized the micro-level in terms of helping individual patients earlier and enabling more personalized care. The USA further included a meso-level and non-clinical aspect, envisioning facilitation of research processes for drugmakers. In contrast, Chinese coverage centered on macro-scale goals, focusing on increasing healthcare provision capacity, closing provision gaps, and standardizing care across the country.
Similarities
AI was envisioned as a means to enhance healthcare, described to “help” or “improve” healthcare, across US (e.g., Council, 2020b; Wang, 2020b), German (e.g., Klöckner et al., 2020; DPA, 2019), and Chinese (e.g., Chen, 2018; Feng, 2020) coverage alike. In addition, a particular spotlight was put on the diagnostic (e.g., Wang, 2020b; Klöckner et al., 2020; Li & He, 2019) and treatment steps of healthcare (e.g., Council, 2020b; Majorczyk, 2019; Lv, 2018). Furthermore, doctors were expected to remain central and irreplaceable, with AI technologies merely meant to “help” doctors in delivering better care (e.g., Wang, 2020b; DPA, 2019; Lv, 2018). More explicit examples included a speaker in US coverage emphasizing that “[t]he goal of using artificial intelligence in health care isn't to replace humans but rather to assist doctors” (Wang, 2020b), German news coverage describing AI as “tuned textbooks” for doctors and “not as a replacement, but as a promising support” (Klöckner et al., 2020), and Chinese coverage discussing AI as a “doctor's assistant” (Chen, 2018) and a “tool” because it was “impossible to replace doctors” (Lv & Wang, 2017).
Differences
The differences in terms of the micro-level focus (enhanced individual patient care) in US and German coverage and macro-level focus (large-scale enhancements) in Chinese coverage related both to diagnostics and treatment. Only US coverage additionally envisioned AI at a meso-level to facilitate drugmakers’ research processes.
Regarding diagnostics, the US and German imaginary versions linked AI-enabled highly accurate, early-stage diagnoses to more successfully treating or even preventing illnesses for individual patients. For example, in US coverage, doctors hoped to use AI for predicting adolescents’ schizophrenia risk, because “[d]rugs to treat schizophrenia may help those who are going to develop the disease, but the challenge is to identify who the patients will be” (Kolata, 2021). One German article argued that AI-enabled faster, more accurate diagnoses of rare diseases “could be crucial in order to help the patient early and improve their chances of recovery” (Telgheder, 2017). Regarding treatment, the German and US imaginary centered on more personalized care. For example, one US article described an AI platform to determine individually tailored blood cancer treatment, aiming “to reconstruct an individual patient and to stimulate how the disease progresses through each patient's body, and which types of therapies might treat the disease” (Castellanos, 2020). A German article similarly reported that AI could help “to fine-tune treatment to the individual patient” (Klöckner et al., 2020).
Adding a meso-level and non-clinical healthcare aspect to the US imaginary, AI was additionally envisioned to help drugmakers’ research and development because, for instance, it “could help drugmakers better understand the target population for specific drugs” (Castellanos, 2020).
In contrast, in the Chinese imaginary, regarding diagnostics, AI was envisioned to enable large-scale efficiency increases because it “can assist doctors in identifying and predicting the risks of more than 700 diseases, improving diagnostic accuracy and efficiency of clinicians” (Feng, 2020). Concerning treatment, the emphasis laid on standardized care for major diseases, especially cancer, as healthcare infrastructures were uneven between large cities and smaller primary medical institutions: “[AI technologies] … will bring a new solution to the standardized diagnosis and treatment in oncology” (Lv, 2018). Chinese news coverage of the imaginary explicitly linked these AI-enabled enhancements to structural challenges in the healthcare system, as they could help close gaps in public health service capacity and reduce inequalities between large hospitals and grassroots facilities. For instance, one article argued that AI in healthcare “will be conducive to making up for the shortcomings of grassroots diagnosis and treatment services” (Feng, 2020); and a hospital dean estimated that “[a]rtificial intelligence-assisted diagnosis can …solve the problem of insufficient medical service capacity to a certain extent” (Li & He, 2019).
Specific technology
The referenced AI technologies in this imaginary were broadly similar across all three cases, including “AI”/artificial intelligence,” AI-underlying technologies and medical AI applications.
Similarities
Beyond generic mentions of “AI”/“artificial intelligence,” AI-underlying technologies included, for instance, “machine-learning techniques” (Wang, 2020b), “Big Data” (Mewis, 2019), and “cloud computing” (Lv, 2018). Some, like “machine learning” or “algorithms,” appeared in the coverage of two or all countries (McConnon, 2018; Lv & Wang, 2017; Telgheder, 2017). Examples of medical AI applications were “AI-powered chatbots” (McConnon, 2018) and a patient simulation platform (Castellanos, 2020) in US coverage, a “smart hospital” (Majorczyk, 2019), and “AI-based decision support systems” (Hirsch, 2019) in German coverage, and “Intelligent Image Diagnostics” (Chen, 2018), and “Medical Knowledge Mapping” (Li & He, 2019) in Chinese coverage.
Desirability
Across all three countries, the vision was considered desirable for healthcare practitioners and ambiguous for patients. However, in contrast to the US and German versions, the Chinese imaginary also involved desirability for macro-structures, namely its population and the public health system.
Similarities
AI-enhanced healthcare was considered desirable for healthcare practitioners because it could ease their work and relieve pressure. For instance, one US article reported that AI “will make their [i.e., doctors’] lives easier” (Grady, 2019), one German article argued that it “can take over many of the doctors’ routine tasks and thus disburden them” (Klöckner et al., 2020) and a Chinese article asserted that AI can “bring convenience to medical workers” (Feng, 2020).
Perceived ambiguity for patients stemmed from a hope for improving patient outcomes, and a fear of increasing risks of harm. Anticipated improvements involved quality of life, cure and survival rates. For example, one US news article argued that AI-enabled earlier detection of dementia could help “preserving a patient's quality of life” (Wang, 2020b); one German article described the higher chances of curing a cancer patient thanks to AI: “Especially in the case of cancer, a quick diagnosis could be crucial in order to help the patient early and improve his chances of recovery” (Telgheder, 2017); and one Chinese article explained that enhanced healthcare provision capacity through AI could benefit patients because “more cancer patients can be diagnosed and treated early, and their survival years and quality of life can be improved” (Chen, 2018).
Fears of increased risks of harm were linked to potential misdiagnoses. For example, in US coverage an AI researcher questioned AI chatbot use in mental healthcare: ““If the app doesn't work, are people less likely to get the help they need?” (McConnon, 2018). One German article cited a survey which identified AI misdiagnosis as a perceived risk among 68% of the German population (Klöckner et al., 2020). In Chinese coverage, speakers even warned against the ultimate harm to patients: “AI's diagnosis can also be compromised, and that compromise can result in a patient's death” (Lv & Wang, 2017).
Differences
The emphasis on macro-level affected entities, namely the Chinese population and public health system in the Chinese imaginary mirrored the macro-level focus in its “envisioned role” element. The population was expected to benefit from the efficiency gains from AI use—especially from its introduction in cancer diagnostics: “Only then can the early screening for lung cancer, an action that benefits the country and the people, be carried out smoothly” (Chen, 2018). AI-enhanced healthcare was also described to help “build a healthy China” (Feng, 2020). The public health system was seen to gain from AI because it “will be conducive to …strengthening the efficiency of public health services, and helping to solve the structural problems of the relative scarcity of high-quality healthcare resources” (Feng, 2020).
Speakers
(Health) tech sector representatives were speakers in all three countries. However, differences emerged regarding other speaker groups, as civil society was only represented in US and German coverage, and healthcare sector speakers were only a substantial group in German and Chinese coverage. Government and health/pharmaceutical company voices were only promoted in Chinese coverage of the imaginary.
Similarities with small variations
While included in all three countries, speakers from the tech sector also displayed small differences: US news coverage featured executive and employee level, as well as both “Big Tech” and health technology start-up speakers, such as an IBM researcher (Kolata, 2021) and the CEO of start-up Aifred Health (McConnon, 2018). In the German imaginary, only health tech founders and executives like the Ada Health founder (Hoffmann, 2021) acted as speakers. In Chinese coverage, tech sector speakers were generally executives of Health Technology firms, particularly subsidiaries of larger groups, such as the president of Yitu Healthcare (Chen, 2018).
Differences
Civil society representatives in US and German news coverage differed in their range. In US coverage, this speaker group exclusively consisted of non-profit or academic researchers or research organization executives, like the director of the National Institute for Mental Health (McConnon, 2018). The German imaginary was constructed by a larger variety of civil society speakers, ranging from non-profit research, and NGO representatives to patients, such as the Hippo Foundation founder (Klöckner & Rybicki, 2020) and a cancer patient (Majorczyk, 2019).
Remaining an outlier in the US case, German healthcare sector speakers were a mix of executives and practitioners including, for instance, an oncologist at University Hospital Essen (Majorczyk, 2019), while in the Chinese case, they were generally deans or department heads of public hospitals such as a department director at Changzheng Hospital, Shanghai (Huang & Chen, 2021).
Only Chinese coverage included officials from government and governmental associations, as well as healthcare and pharmaceutical company executives, like the director of the Pinggu District Health Commission (Feng, 2020), the president of the Chinese society for clinical oncology (Lv, 2018), and the chairman of Baiyang Pharmaceutical (Lv & Wang, 2017).
Imaginary 2: Managing pandemics/epidemics
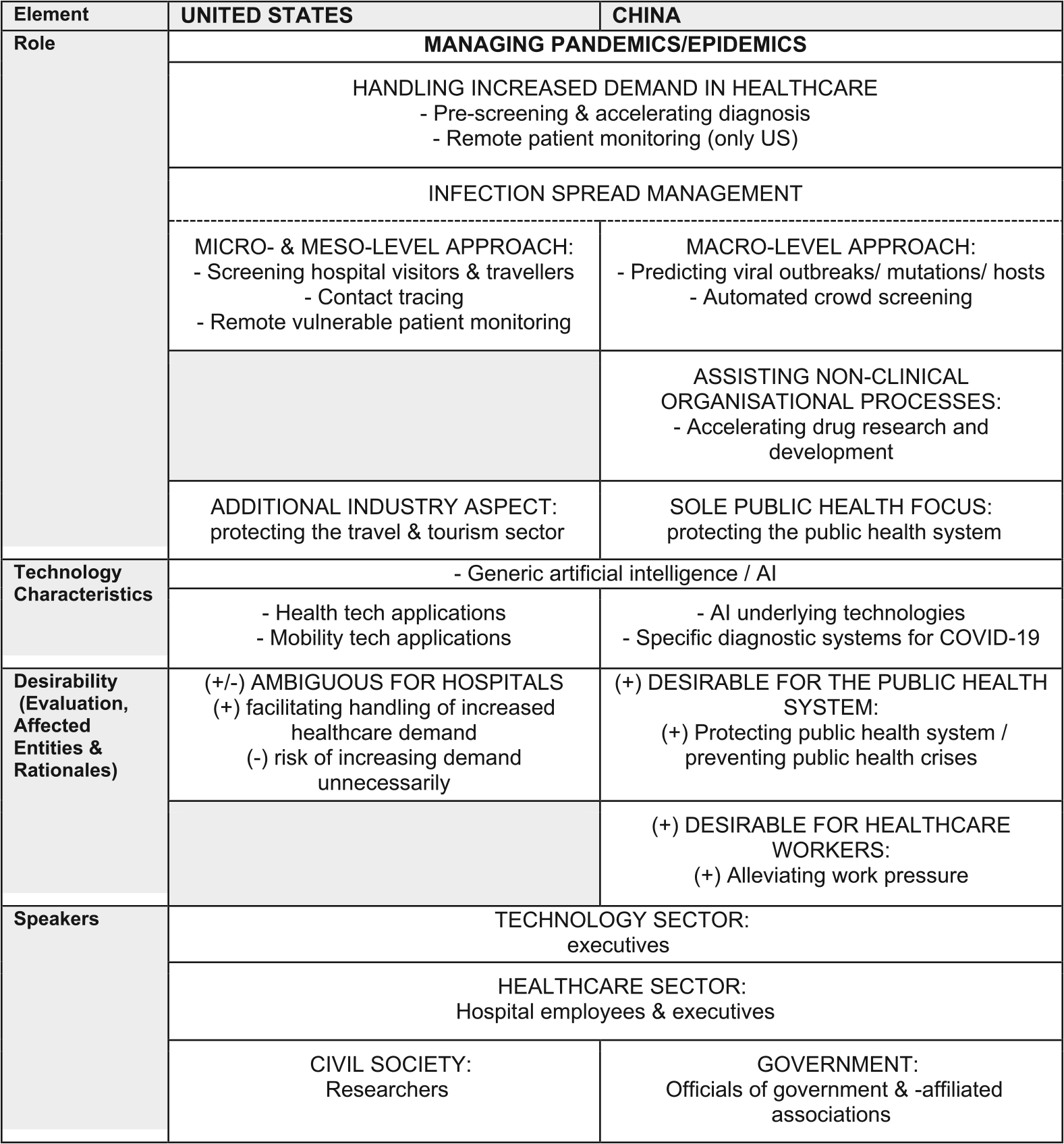
The second imaginary envisioned AI for managing pandemics and epidemics 1 (see Table 4). It was fully developed in the USA and China, but an outlier in Germany. Both in the USA and China, the imaginary was promoted with the first emergence of the COVID-19 crisis in 2020; the two German articles on this imaginary were published in 2020 and 2021. Essentially, AI was envisioned to help handle increased demand in healthcare services and to assist in infection spread. But the US version—constructed by technology, healthcare, and civil society sector speakers—referred to “AI” and AI-enabled health and mobility applications to envision pandemic management in both the healthcare and travel sectors. AI-enabled infection spread was imagined at the individual patient- and hospital-levels, yet the vision was considered ambiguous for hospitals. The Chinese version was promoted by technology, healthcare, and government sector speakers and referred to “AI,” AI-underlying technologies, and specific diagnostic systems for COVID-19. AI was centrally envisioned to help epidemic management in and for the healthcare system. AI-assisted infection spread was conceived of from a crowd- and top-down angle. AI was also devised to facilitate drug research and development. The Chinese imaginary was portrayed as exclusively desirable for both the public health system and healthcare workers.
Overview of the Second Imaginary in US and Chinese News.
Role
The envisioned role for AI in this imaginary showed similarities regarding the overarching goal of managing epidemics/pandemics across US and Chinese coverage and as an outlier in German coverage. Both US and Chinese coverage also centered on similar strategies, namely using AI to handle increased healthcare demand, and for managing infection spread. However, US coverage devised AI-enabled infection spread at the organizational and individual patient level, while Chinese coverage constructed it from a crowd- and top-down planning angle. The Chinese imaginary additionally placed AI into non-clinical healthcare processes in drug research and development. Furthermore, US coverage also included an additional industry aspect—envisioning AI for infection spread in tourism, not just healthcare—while strategies in Chinese coverage were solely linked to helping the public health system through the crisis.
Similarities
The imaginary in all three countries focused on using AI to manage the Covid-19 crisis, and in the USA and China also to manage future pandemics or epidemics. For example, one USA and one Chinese article titled that “Hospitals Tap AI to Help Manage Coronavirus Outbreak” (Council, 2020a), and “artificial intelligence is on the front line to ‘fight the epidemic’” (Qiu, 2020), respectively, and German articles reported on “Artificial intelligence in Covid diagnostics,” “in Covid progression monitoring” (Olk, 2021) and “to find a cure for Covid-19” (Rybicki, 2020). However, in the following, we only compare the fully developed US and Chinese imaginaries.
Both the US and Chinese coverage envisioned AI to help handle increased demand in healthcare through pre-screening and the acceleration of diagnoses; the US imaginary additionally involved remote patient monitoring. For example, one US article reported that “Faced with a burgeoning number of Covid-19 patients, hospitals are turning to AI to help with diagnoses and assessments” (Olson, 2020). Furthermore, AI-enabled remote monitoring of patients was envisioned to improve resource allocation because it could “predict which Covid-19 patients are likely to experience complications,” which “can help the hospital better allocate scarce resources, such as beds in its intensive-care unit” (Council, 2020a). Similarly, Chinese coverage explained that “[the combination of AI and CT] can help accelerate the identification of infected people in primary healthcare organisations” and that “AI is playing a role in the intelligent diagnosis of CT images of new coronavirus pneumonia, especially in alleviating the shortage of medical resources in core epidemic areas” (Tong, 2020).
Similarities with small variations
Regarding AI-enabled infection-spread management, the US imaginary involved a micro- and meso-level approach with individuals and organizations as the unit of management, while the Chinese imaginary centered on macro-level spread management across crowds and through top-down planning.
Concretely, US coverage emphasized infection control through monitoring vulnerable patients at home, stopping infected visitors at hospital entrances, and tracing individual contact. For instance, it reported on a hospital network which “this week plans to start using AI to remotely monitor high-risk cardiac patients at home to reduce their risk of exposure to the new coronavirus” (McCormick & Shah, 2020). And it described a hospital planning to block infected people at visitor entrances through an AI-powered screening system “[a]s part of an effort to curb the spread of any disease in its public gathering areas” (Council, 2020a). Furthermore, individuals could volunteer to use AI-enabled contact tracing (Hernandez, 2020).
In contrast, in the Chinese imaginary, AI was expected to “provide a great boost to crowd screening” (Zeng & Sun, 2020). Furthermore, AI-enabled planning for “epidemic prevention and control” was envisioned top-down across the population, as AI technologies were described as able to “predict potential outbreaks of the new coronavirus” and “predict potential hosts” and envisioned to help “tracking the mutation of the new coronavirus” (Zeng & Sun, 2020), thus assisting policymaking because they can “help public health decision-makers formulate models of epidemic development … thereby helping decision-makers to implement precise policies” (Qian, 2020).
Differences
The Chinese imaginary included AI for drug research and development, while this non-clinical healthcare aspect was absent in this second US imaginary. For example, Chinese coverage highlighted that “artificial intelligence can also help figure out the structure of the virus and screen a large number of previous drugs” (Qian, 2020).
Furthermore, the US and Chinese imaginary notably differed because the US version also included an economic aspect, envisioning AI for infection spread prevention in the travel and tourism industry, highlighting that AI products “aim to make travel safer during the pandemic” and that “A.I. could also serve as an ounce of prevention when the next health crisis hits the travel industry” (Kamin, 2020). In contrast, public health was the sole focus of the Chinese imaginary. For instance, one speaker believed that “artificial intelligence technology plays an important role in early warning of the public health system” (Qian, 2020). Even the use of AI in the drug industry was envisioned as a means “to effectively support epidemic protection and control” (Li, 2020), rather than help, for instance, the drug industry itself.
Specific technology
The envisioned technologies in this imaginary, beyond generic references to “AI”/ “artificial intelligence,” differed vastly. In the US version, referenced technologies reflected the imaginary's parallel focus on the travel industry and healthcare by involving both health and mobility technology applications. Cited technologies in the Chinese imaginary more closely resembled the technologies in the first imaginary, including AI-underlying technologies, but more specific diagnostic systems for COVID-19 in terms of medical AI applications.
Differences
In US coverage, AI-enabled health technologies included, for instance, symptom-checking smartphone apps (Fitch, 2020) or a remote patient monitoring system (Council, 2020a), and examples of mobility technology applications were smart health cards or artificial tour guides for travelers (Kamin, 2020).
In contrast, the Chinese imaginary referenced AI-underlying technologies like algorithms, big data analytics, or machine learning (Zeng & Sun, 2020) and diagnostic-focused systems based on AI imaging technology such as pneumonia AI image-assisted diagnostic products (Wang, 2020a), and a COVID-19 intelligent CT image evaluation system (Tong, 2020).
Desirability
Desirability descriptions of this imaginary in both countries’ versions were connected to the increased demand for healthcare during the pandemic, but otherwise differed considerably regarding the assessments and imagined affected entities. Indeed, the US imaginary was constructed as ambiguous for hospitals, while the Chinese imaginary was promoted as purely desirable for the public health system and healthcare workers.
Differences
Desirability of the imaginary in US coverage, in line with the envisioned “role,” was centered on meso-level affected entities—hospitals—and considered ambiguous, because AI solutions could either help hospitals manage demand, or induce unnecessary demand when faulty. For example, one article explained that “[u]sing AI to process data for remote patients helps facilities focus resources on more severe cases” (McCormick & Shah, 2020), while sceptics of cough screening apps cautioned in another that reliability issues could be “sending healthy individuals to overloaded hospitals” (Fitch, 2020).
In the Chinese imaginary—similar to the first—the public health system was again described as positively affected as AI would help protect it and prepare it for public health emergencies. For instance, one article titled that “AI builds a firewall for the public health system” (Qian, 2020), while a speaker in another article argued that the next step for AI is to “contribute to our country's realisation of “early detection, early reporting, early isolation, early diagnosis, and early treatment” of major public health emergencies” (Wang, 2020a).
Notably, only Chinese coverage constructed the imaginary as desirable for healthcare workers, which were struggling under the pressure of quickly diagnosing increasing numbers of suspected COVID patients. AI was seen as an opportunity to ease this pressure. For example, one article explained that an AI model for image-based diagnoses of COVID “will alleviate the situation of strained medical diagnostic resources” (Wang, 2020a).
Speakers
In both countries’ news coverage, mirroring the influence of the technology sector in the first imaginary, speakers again included executives from the technology sector, but also representatives from the healthcare sector. Civil society speakers were only represented in US coverage, while government speakers were only referenced in Chinese news coverage.
Similarities with small variations
From the technology sector, only tech sector executives from start-ups and mid-sized specialist IT companies like the CEO of RADLogics (Olson, 2020) contributed to this second US imaginary, whereas in Chinese coverage, they were again executives of large technology firms, their health technology departments, or subsidiaries like the product development head at SenseTime (Qiu, 2020).
From the healthcare sector, speakers included hospital employees and executives, like, for instance, the president of Tampa General hospital (Council, 2020a) for the US imaginary and the vice president of the Shanghai Public Health Clinical Centre (Tong, 2020) for the Chinese imaginary. While this was similar in the coverage of the first Chinese imaginary, it was a notable difference in the US coverage, where this speaker group had been only an outlier.
Differences
Bearing strong similarities to speaker representation in the first imaginary, civil society speakers in US coverage again consisted exclusively of researchers, yet from various disciplines, including “sociologists” (Kamin, 2020), a medical researcher (Olson, 2020), a computational linguist, a bioethicist-anesthesiologist, and “AI researchers” (Fitch, 2020), and government voices in Chinese coverage included government officials and directors of associations under the government, such as the president of the China Academy of Information and Communication Technology (Wang, 2020a).
Conclusion and discussion
Our analysis of AI imaginaries in US, German, and Chinese news media revealed two cross-national imaginaries, albeit with some differences. The first imaginary on enhancing healthcare with AI emerged across all three countries; the second imaginary on using AI to manage pandemics or epidemics was fully developed in China and the USA, but less developed in Germany. Differences appeared in terms of the approaches and structures in focus, which we broadly qualified as representing micro- versus macro-levels of society: The first US and German imaginaries envisioned AI to enhance patient care at the individual level, whereas the Chinese imaginary positioned AI as a means for large-scale efficiency gains, treatment standardization and reduction of service provision gaps across the country. Similarly, the second US imaginary envisioned AI to help manage the pandemic at individual patient and hospital-level, while the Chinese imaginary anticipated it to help in top-down epidemic control and planning at national level. Notably, both US and Chinese coverage included a vision for AI to help with non-clinical processes in drug research and development organizations, an aspect absent from German coverage. Overall, Chinese imaginaries showed less ambiguity: China's first imaginary included more positively affected entities compared to the other two countries, and the second Chinese imaginary on AI-enabled epidemic control was considered exclusively desirable. Regarding speakers contributing the imaginaries, the technology sector was the only one represented across all five imaginaries, whereas healthcare sector representatives were notably missing from the first US imaginary. Civil society speakers only appeared in US and German coverage, whereas Chinese coverage promoted government voices.
In light of previous literature, the results indicate well-established, cross-national imaginaries for AI in healthcare, particularly regarding the enhancement of healthcare through AI. The understanding of healthcare as a priority area for AI development and use seems to be reflected, promoted, further shaped, and sharpened by the news media, despite the systemic differences between the USA, Germany, and China. This suggests that the imaginaries can be considered “collectively held” (Jasanoff, 2015, p. 4) across national borders. Moreover, not only was AI seen as a means to enhance healthcare across all three countries, but this imaginary was also supported across different stakeholder groups within each country. Additionally, across all three countries, the imaginaries emerged around the same time. Findings on investments in medical AI as compared to healthcare or AI ventures in general seem to confirm that the imaginaries are sufficiently powerful to impact the development of the technology in this area (Jairath et al., 2024).
Yet, some finer differences can be explained by their sociocultural and sociopolitical outlook on technology and healthcare systems. First, the imaginary of managing pandemics did not fully emerge in Germany. This could reflect Germans’ more risk-fixated outlook on new technologies (Dogruel & Joeckel, 2019; Jasanoff, 1995), and may have been compounded by the timespan of our study stopping in mid-2021. Additionally, German coverage exclusively devised clinical roles for AI in healthcare, disregarding its potential in non-clinical processes (Bohr & Memarzadeh, 2020a). This may be similarly grounded in a hesitancy toward a broad application of AI in Germany. Second, the Chinese imaginaries focused particularly on alleviating shortages and inequalities in public health and top-down infection control and highlighted affected collective entities like the population and public health system. On the one hand, this reflects the nation's view of technology as a solution for socio-economic and political challenges (Greenhalgh, 2020; Hine & Floridi, 2022). On the other hand, it underscores the unique demographic and developmental context in China, with a large population, limited healthcare resources, and large regional disparities in health indicators (Fang et al., 2010), which has been an issue of governmental focus for reforms (Jia et al., 2022). The US imaginaries reflect its largely privatized healthcare system and market concentration therein (Cacace, 2010; Fulton, 2017; Hennes et al., 2015), as they focused on individual (patient) and organizational (hospital) levels and envisioned AI to enhance the quality of individual healthcare rather than to cut costs. Realising the US imaginaries would therefore likely increase, rather than reduce accessibility issues in US healthcare (Fullman et al., 2018; Hennes et al., 2015).
While the envisioned roles and affected entities generally fell into micro-and meso-level approaches and structures in the USA and German cases, and macro-level approaches and structures in the Chinese case, one notable exception was the focus of Chinese coverage on healthcare practitioners in the Covid-related imaginary. In particular, this aspect was absent in the correspondent US imaginary. We suggest that this might be explained by different diagnostic strategies in China and the USA. China heavily relied on CT imaging—and its related radiologist workforce—for first diagnosing Covid-19. In contrast, in the USA, diagnosis was recommended through lab studies, while lung CT imaging was reserved for monitoring severe cases (Greenspan et al., 2020).
While the ambiguity for patients of using AI to enhance healthcare seems in line with scientific research on AI in healthcare, the representation of the imaginaries as exclusively desirable for healthcare workers notably disregarded potential downsides. Indeed, for patients, coverage across all countries described both the potential benefits in health outcomes and the potential risk of harm to patients (see e.g., Jeddi & Bohr, 2020; Topol, 2019). For healthcare practitioners, however, only AI's potential to ease their work and alleviate work pressure was addressed (see e.g., Tran et al., 2020), and no exposure was given to potential downsides, such as risk of deskilling, of agency loss in decision-making, of medical errors and negative outcomes, and of malpractice and liability resulting from an overreliance on AI or faulty AI (e.g., Hazarika, 2020; Morley et al., 2020; Topol, 2019). However, at least in the first imaginary, this could be explained by the emphasis in the imaginary on the central, irreplaceable role of doctors, whose work will merely be supported and supplemented by AI. If doctors remain in charge, they are less likely to suffer the consequences of an overreliance on AI or errors from faulty AI. This doctor–centric finding contrasts with findings by Bunz and Braghieri (2022) in US and UK news, where AI was represented as soon-to-be outperforming doctors, and by Hansen (2022) in Danish coverage of AI, where the human-centric and human-replacing visions of AI co-existed.
Regarding the speakers cited, we found an omnipresence of technology sector speakers, mirroring prior studies on AI news coverage in general (e.g., Chuan et al., 2019; Sun et al., 2020). Additionally, our findings provide further evidence for the argument of a “digital colonization” of the healthcare sector by Big Tech (Ozalp et al., 2022) in the case of the first imaginary in US coverage. Indeed, not only did coverage feature executives and employees from Big Tech companies, but health sector speakers remained an outlier in the media coverage of the imaginary. This could be interpreted as a form of marginalization of healthcare professionals in favor of a stronger influence of Big Tech as healthcare is being transformed by AI technologies. Nevertheless, we also identified speakers from health tech start-ups, suggesting that this phenomenon could reflect a more general rapprochement of the two sectors as AI becomes integrated into healthcare, not limited only to Big Tech expanding its reach into new realms.
The Chinese case was the only one to feature government voices. Furthermore, since Chinese public hospitals are themselves part of China's political system (Wang, 2009), the remarks of medical practitioners holding administrative positions therein are likely to also reflect the government's attitudes toward AI in healthcare, essentially further imagining the technology from a government perspective. Overall, this multiple representation of government-related voices could be anticipated given the largely state-controlled Chinese media and healthcare sector (Wang, 2009; Zhao, 2012)
This study contributes to scholarship on sociotechnical imaginaries of AI in several ways. First, it provides the first analysis of news media imaginaries of AI in healthcare, using a fine-grained operationalization of the SIs concept. Second, it includes in its comparison a non-Western and two non-anglophone countries, which are typically underrepresented in research on media coverage of AI (Brause et al., 2023). Finally, it illustrates ways in which imaginaries of AI in healthcare can be considered as “collectively held” as they are “publicly performed” in news media (Jasanoff, 2015, p. 4): the overarching visions are well-established across the news coverage of several countries, while accounting for contextual factors in each country; their construction in the news media involves speakers from multiple parts of society, including private, public and third sector stakeholders; the different versions of the first imaginary even reproduce certain aspects at a more detailed level across countries, including the ambiguity and desirability of the vision for patients and healthcare practitioners; finally, the second Chinese imaginary contained no ambiguity about the desirability of the vision, as it was constructed as purely desirable for both the healthcare system and healthcare workers, giving it a better chance of convincing relevant stakeholders to support and advance its real-world implementation.
Future research could expand on these contributions, broadening the country and media samples or period of analysis. For instance, the news article sample in this paper did not include the phase after the introduction of Large Language Models (LLMs), such as ChatGPT, to the public. Yet this development reinvigorated news discussions of AI (Gilardi et al., 2024) and preliminary research has identified healthcare as an important topic therein (Xian et al., 2024). In addition, a recent analysis of (mostly) US digital news reporting on ChatGPT in healthcare identified themes mirroring our findings: ChatGPT use is reported to enhance healthcare and to particularly benefit doctors and the healthcare system while reporting remains highly ambiguous about the potential impact on patients (Xu & Wang, 2024). We therefore expect that our findings would hold true in the phase since the introduction of LLMs. Further research could also expand the focus to understand what other imaginaries of AI these healthcare imaginaries are competing with in the news media. Finally, research could probe whether and how these imaginaries succeed or fail to emerge in other public arenas, such as social media, policy debates, and documents, or in surveys among the public.
Supplemental Material
sj-docx-1-emm-10.1177_27523543241300185 - Supplemental material for News Media Imaginaries of Artificial Intelligence in Healthcare: A Qualitative Analysis Across China, Germany, and the United States
Supplemental material, sj-docx-1-emm-10.1177_27523543241300185 for News Media Imaginaries of Artificial Intelligence in Healthcare: A Qualitative Analysis Across China, Germany, and the United States by Saba Rebecca Brause, Heng Yang, Mike S. Schäfer and Jing Zeng in Emerging Media
Supplemental Material
sj-docx-2-emm-10.1177_27523543241300185 - Supplemental material for News Media Imaginaries of Artificial Intelligence in Healthcare: A Qualitative Analysis Across China, Germany, and the United States
Supplemental material, sj-docx-2-emm-10.1177_27523543241300185 for News Media Imaginaries of Artificial Intelligence in Healthcare: A Qualitative Analysis Across China, Germany, and the United States by Saba Rebecca Brause, Heng Yang, Mike S. Schäfer and Jing Zeng in Emerging Media
Supplemental Material
sj-docx-3-emm-10.1177_27523543241300185 - Supplemental material for News Media Imaginaries of Artificial Intelligence in Healthcare: A Qualitative Analysis Across China, Germany, and the United States
Supplemental material, sj-docx-3-emm-10.1177_27523543241300185 for News Media Imaginaries of Artificial Intelligence in Healthcare: A Qualitative Analysis Across China, Germany, and the United States by Saba Rebecca Brause, Heng Yang, Mike S. Schäfer and Jing Zeng in Emerging Media
Footnotes
Acknowledgments
The authors gratefully acknowledge Xiaoyue Yan (University of Zurich) for her contributions to data collection and technical editing of the manuscript.
Data availability statement
The data that support the findings of this study are available from Factiva database, Frankfurter Allgemeine Zeitung data service and the Southern Weekly mobile website but restrictions apply to the availability of these data, which were used under license for the current study, and so are not publicly available.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical statement
Based on the analysis of news coverage in different countries, there are no human participants involved in this article. Informed consent and ethical approval are therefore not required in this study.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work is part of the project “Imaginaries of Artificial Intelligence: The Communicative Construction of AI in China, Germany and the US” funded by the Swiss National Science Foundation (SNSF) and German Research Foundation (DFG) (Grant number 100017L_197552).
Supplemental material
Supplemental material for this article is available online.
Notes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.