
Abstract
Objective:
To establish normative nasalance scores for the Nasometer II for children speaking Quebec French.
Design:
Prospective study using a randomly selected sample of children with typical speech.
Setting:
Two children’s hospitals in the province of Quebec, Canada.
Participants:
Eighty-eight children with typical speech, language and hearing development, aged between 6;00 and 11;11 years, were enrolled at the Centre hospitalier universitaire Sainte-Justine in Montreal and the Centre hospitalier universitaire de Québec-Université Laval in Quebec City, Canada.
Outcome Measure:
Mean nasalance scores.
Results:
Mean nasalance scores were obtained for oral vowels, nasal vowels, repeated syllables, oral sentences, a nasal sentence, mixed sentences as well as a short text. While there were no meaningful significant effects of sex and age on the nasalance scores, most nasalance scores obtained at the hospital site in Montreal were statistically significantly higher than in Quebec City. Mean nasalance scores, standard deviations and theoretical critical threshold values are provided and can be used for clinical assessment and research.
Conclusions:
Nasalance scores differences according to hospital sites may be attributable to dialectal differences, to differences between the nasalance scores obtained by the nasometers in the 2 clinics, or to a combination of the 2. In future research, diagnostic cutoff scores for different nasal resonance disorders can be developed based on these normative scores.
Introduction
In the field of Speech-Language Pathology, resonance refers to our perception of the vibration of sound through the oral, pharyngeal and nasal cavity.1,2 The sound frequencies generated by the vocal folds are modified by the shape and size of the air space of the vocal tract, which in turn are modified by articulatory settings such as the position of the tongue, the opening of the mouth and the opening and closing of the velopharyngeal valve. 3 The velopharyngeal valve is responsible for coupling and decoupling the oral and nasal cavities during speech. During velopharyngeal closure, the velum elevates and the nasopharynx narrows. 4 Velopharyngeal closure is important for the production of oral speech sounds, while nasal and nasalized speech sounds are produced with an open velopharyngeal sphincter. The proper functioning of the velopharyngeal sphincter is essential for intelligible and acceptable speech.
In Speech-Language Pathology, the term resonance disorder is used to refer to imbalances of oral and nasal resonance in speech. 5 There are different resonance disorders, or types of oral-nasal imbalances, that may arise as a result of anatomical and functional differences. 6 Hypernasality is defined by excessive nasal resonance on voiced oral vowels and consonants. The cause is velopharyngeal dysfunction (VPD), which may be due to anatomical defects (eg, cleft palate), motor impairment (eg, dysarthria) or velopharyngeal mislearning (eg, compensatory articulation error despite adequate anatomical structures). Hyponasality manifests when there is not enough sound transmitted through the nasal cavity on nasal sounds. This results from nasal airway obstruction, such as hypertrophic adenoids and tonsils or septum deviations. Mixed resonance manifests when there is hypernasality present on oral sounds together with hyponasality on nasal sounds. This phenomenon may arise in cases of combined velopharyngeal dysfunction and partial nasal obstruction. 5 Individuals affected by a resonance disorder may experience differing levels of impact on the intelligibility and acceptability of their speech. This may lead to social challenges and poorer psychosocial outcome. 7
Auditory-perceptual assessment performed by a trained speech-language pathologist is considered best practice to assess for speech and resonance disorders. 6 To supplement listeners’ auditory-perceptual evaluations, the nasometer enables a non-invasive, quantitative assessment of nasalance, which is a proxy measure for the balance of oral and nasal resonance. The nasalance score is the ratio of nasal acoustic energy to the sum of nasal and oral acoustic energy. Nasometers have been used in clinical practice and research for over 30 years.5,8-10 In addition to providing a quantitative measure, nasalance assessment can help determine the effectiveness of speech therapy or surgical intervention and may assist clinicians in judging the degree of severity of a nasal resonance disorder by comparing a patient’s results with the norms established for children of the same age and region. This measure adds a distinctive feature to speech results and is complementary to other objective measures that can be obtained using videofluorosocopy or nasoendoscopy. Nasalance can be an important component of the comprehensive diagnosis of nasal resonance disorders in speakers with cleft lip and palate.
Normative nasalance scores can vary between different languages10,11 and even dialects.12,13 There are also effects of age14-18 and possibly of sex.17-21 Finally, different speech stimuli will result in different nasalance scores.22-24 While standard stimuli for nasalance testing have been developed for many different languages, the situation is still more heterogeneous when it comes to French. Stimuli and normative nasalance scores have been developed for adult25,26 and pediatric speakers of Swiss French. 11 In Canada, stimuli and reference scores have been established for minority French-speaking children and young adults in the Canadian West.12,27 However, there are currently no well-researched test materials and normative scores for children in Quebec, which is a majority French-speaking province in Canada. Quebec French has a different pronunciation for vowels than European French.28-32 It is also characterized by longer nasal vowels. In addition, these tend to become diphthongized in closed stressed syllables.33,34
Therefore, the primary objective of this study was to obtain nasalance norms for French-speaking children in Quebec aged 6;00 to 11;11 years. The secondary objective was to explore the possible differences between mean nasalance scores according to sex, age and research sites. These research objectives were explorative, and explicit research hypotheses were not considered necessary or helpful in this context.
Methods
Participants
Research ethics were obtained for a multi-site data collection (#MP-21-2017-1357). The data collection took place between 2017 and 2020. A total of 104 children with typical speech were screened for participation in the study at 2 academic children’s hospitals in Quebec. Sixty-nine children were screened at the Centre Hospitalier Universitaire Sainte-Justine (CHUSJ) in Montreal and 35 at the Centre Hospitalier Universitaire de Québec-Université Laval (CHU de Québec-UL) in Quebec City. For inclusion, patients had to be between 6;00 and 11;11 years old, speak age-appropriate Quebec French as their first and dominant language as well as pass a hearing screening (1000, 2000, and 4000 Hz). Exclusion criteria included craniofacial and dentofacial differences, speech and language disorders, developmental disorders and attentional or behavioral problems. Sixteen participants failed the initial screening. The resulting study group was composed of 88 children (44 girls and 44 boys). Of these participants, 59 were recruited at the CHUSJ (24 girls and 35 boys) and 29 at the CHU de Québec-UL (20 girls and 9 boys). The mean age was 8.75 years (SD = 1.68). All children spoke Quebec French as their first language, but 11 also spoke English and 5 spoke Arabic at home.
Speech Stimuli
A short protocol consisting of a variety of stimuli has been developed and pre-tested 35 for the assessment of nasalance in Quebec French. The stimuli were chosen to capture a variety of phonetic features and to enable comparison with already existing research data for French, namely those of Leeper et al, 12 Garnier 25 and Tourmel. 26 Some of these stimuli are part of a recently published list of sentences in Quebec French for the auditory-perceptual assessment of resonance and speech related to velopharyngeal function. 36 The protocol includes 28 stimuli in various contexts: 6 prolonged isolated vowels, 13 repeated syllables, 8 sentences and 1 reading passage with 73 words. The reading passage was limited to participants aged 8 to 12 to ensure fluent reading. Table 1 shows the stimuli included in the assessment protocol.
Stimuli. Table 1 Shows the Stimuli Included in the Assessment Protocol.
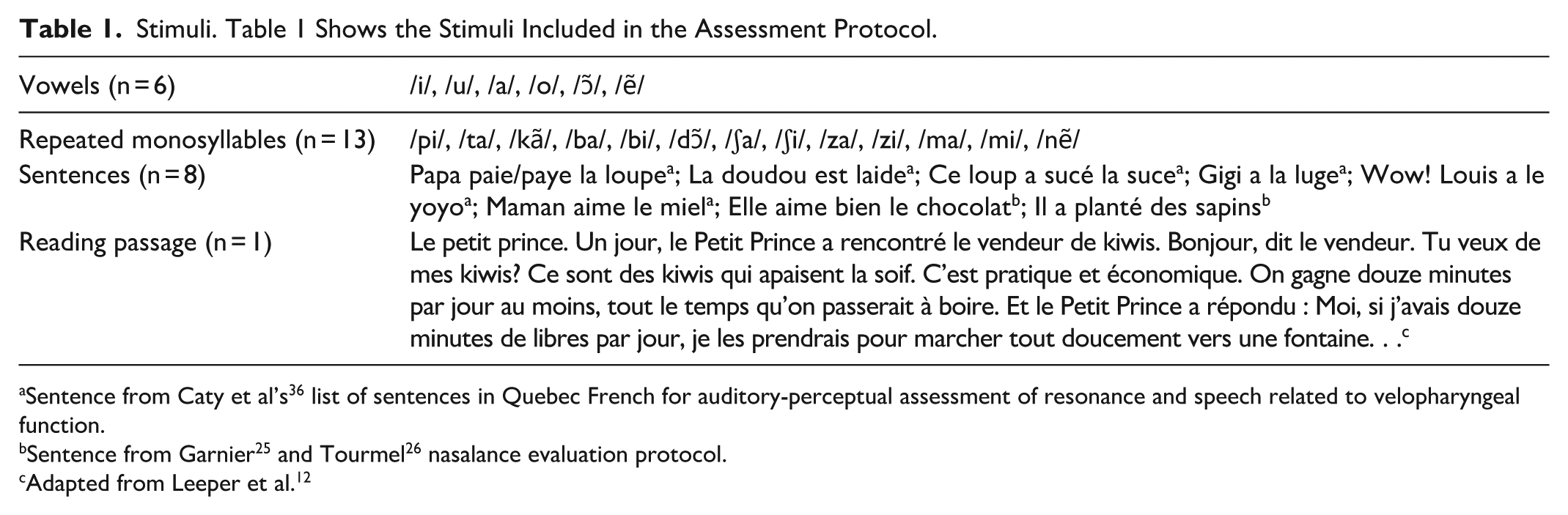
Sentence from Caty et al’s 36 list of sentences in Quebec French for auditory-perceptual assessment of resonance and speech related to velopharyngeal function.
Adapted from Leeper et al. 12
Materials
Hearing screening was performed using an Interacoustics AA222 portable audiometer at CHUSJ and a MAICO MA25 ANSI S3.6 Class 4 audiometer at CHU de Québec-UL. Nasalance data were collected using the PENTAX Medical Nasometer II (model 6450). Each site had its own nasometer. Following the manufacturer’s recommendations, each device was calibrated at the start of the day. An additional calibration was carried out in the middle of the day.
Procedure
The assessments were conducted in the offices of the Speech-Language Pathology department at each site, providing a calm and noise-free environment. Speech and hearing were screened first. For the speech screening, the task was a spontaneous conversation, with informal assessment tasks such as a picture description, if necessary. Nostril patency was screened using a nasal mirror. Screening was considered successful when the speech-language pathologist judged that there were no speech anomalies or signs of nasal obstruction. A hearing screening was then performed. Following the guidelines of the American Academy of Audiology, 37 3 frequencies were tested at an intensity of 20 dB for each ear: 1000, 2000 and 4000 Hz. Screening was considered successful when the child had detected 2 out of 3 signals for each frequency tested, for each ear.
Once a child was deemed eligible to take part in the study, the nasometer assessment could begin. The nasometer headset was placed on the participant’s head according to the manufacturer’s recommendations. Monitoring was carried out throughout the assessment to ensure that the headset remained properly positioned. Once the headset was positioned, the participant was asked to repeat the various stimuli of the assessment protocol. The order of the stimuli was counterbalanced to ensure that each participant experienced the stimuli in a different sequence, minimizing any potential bias or order effects.
Breaks were allowed whenever a participant needed them. If the child made a mistake, he or she was asked to repeat the stimulus until it was produced correctly. Nasalance scores for each stimulus were recorded for later analysis.
Data Analysis
To establish the nasometry norms for children speaking Quebec French, the data were analyzed descriptively with mean nasalance scores and standard deviations. In the diagnosis of resonance disorders, elevated nasalance scores for oral speech stimuli are considered an indication of hypernasality while excessively low nasalance scores on speech stimuli loaded with nasal sounds are an indication of hyponasality. 1 Kummer 38 estimated that the borderline region for hypernasality begins 2 standard deviations above the mean score of an oral test stimulus. For hyponasality, the same author estimated the borderline region more conservatively 1 standard deviation below the mean for a nasal speech stimulus. In the present study, this method was used to estimate the critical thresholds for nasalance scores that could be considered too high for oral speech stimuli and too low for nasal speech stimuli.
The nasometric norms for Quebec French were created with a data collection that was carried out with young female and male speakers ranging in age from 6;00 to 11;11 years. The data were also collected at 2 sites, with different nasometers. As a result, it was important to investigate possible effects of speaker sex, age and sites. To investigate the possible effect of age on the nasalance scores, the group was divided into 1 group of 51 children aged 6;00 to 8 ;11 years (24 girls and 27 boys) and a second group of 37 children aged 9;00 to 11;11 years (20 girls and 17 boys) for statistical testing.
Not all children were able to complete all recordings of the test materials. Based on the data distribution for each stimulus, statistical testing was carried out either with Student T-tests or non-parametric Mann-Whitney U-tests, as appropriate. While this resulted in a relatively large number of 84 2-sided comparisons, the significance level was not Bonferroni-adjusted to avoid type II false-negative errors. 39 Exact P values were recorded so that the plausibility of the described differences could be better appreciated. The significance level was set at P < .05. The statistical analyses were carried out in SAS 9.4 and NCSS 8.
Results
The combined statistical results from the 2 sites can be found in the respective columns in Tables 1 to 4. Together with the means and standard deviations, the theoretical critical threshold (CT) of 2 standard deviations above the mean for oral stimuli and of 1 standard deviation below the mean for nasal stimuli, as suggested by Kummer, 38 are also reported.
Mean Nasalance Scores for Vowels. The Descriptive Reporting in Tables 2 Breaks Up the Results by Center for the Vowel Stimuli.
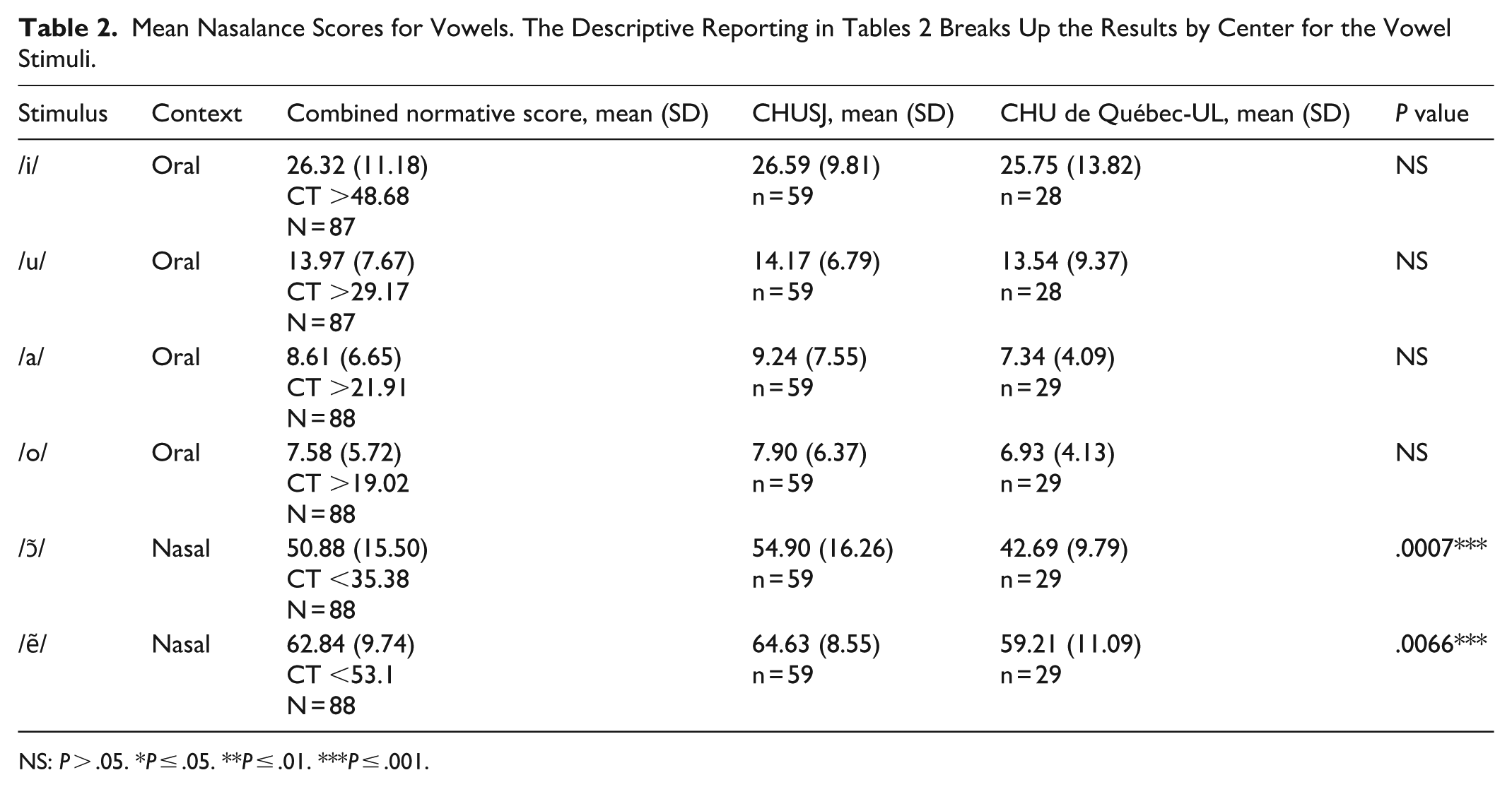
NS: P > .05. *P ≤ .05. **P ≤ .01. ***P ≤ .001.
Mean Nasalance Scores for Repeated Syllables. The Descriptive Reporting in Tables 3 Breaks Up the Results by Center for the Repeated Syllables Stimuli.
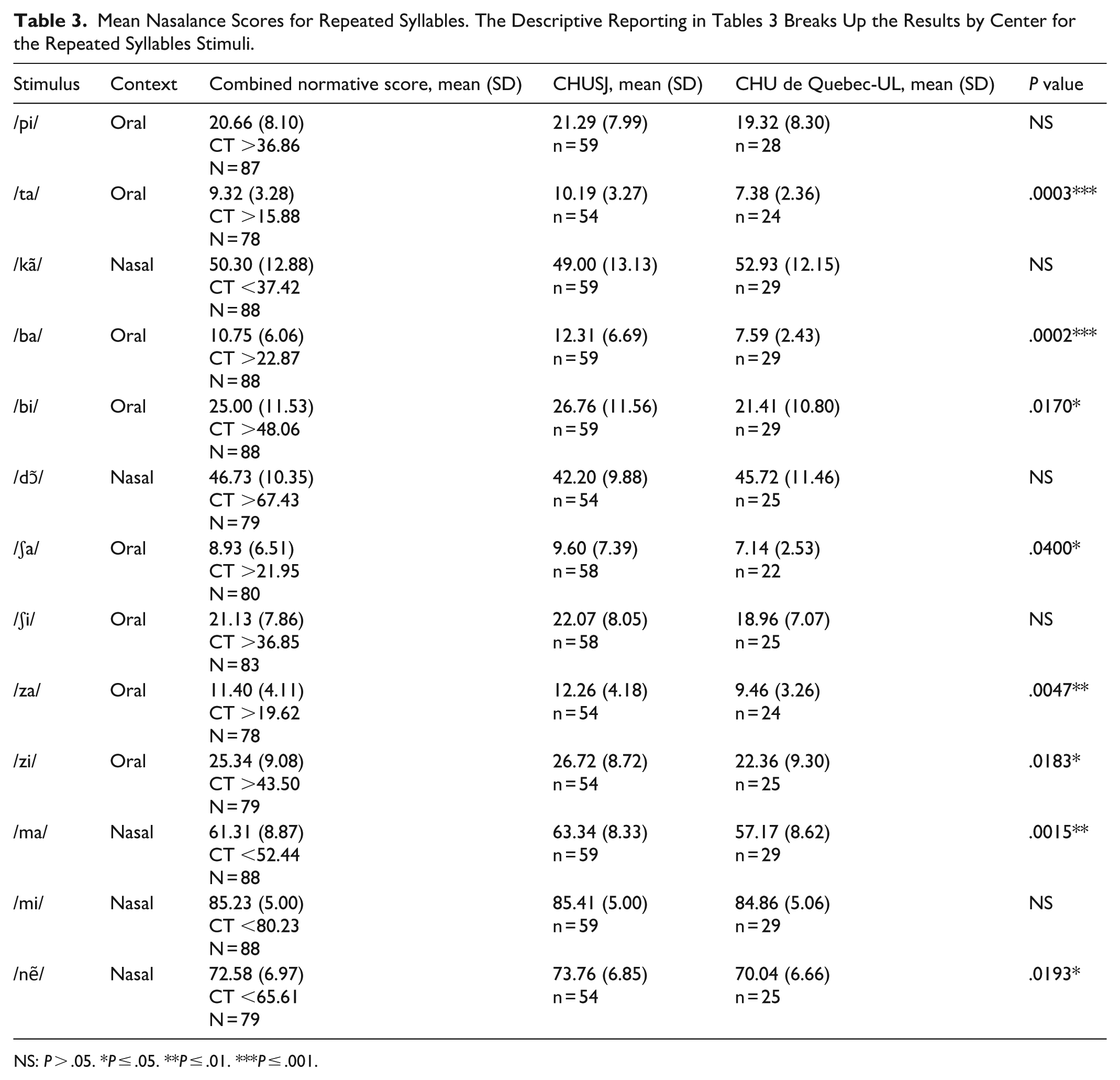
NS: P > .05. *P ≤ .05. **P ≤ .01. ***P ≤ .001.
Mean Nasalance Score for Sentences. The Descriptive Reporting in Tables 4 Breaks Up the Results by Center for the Sentences Stimuli.
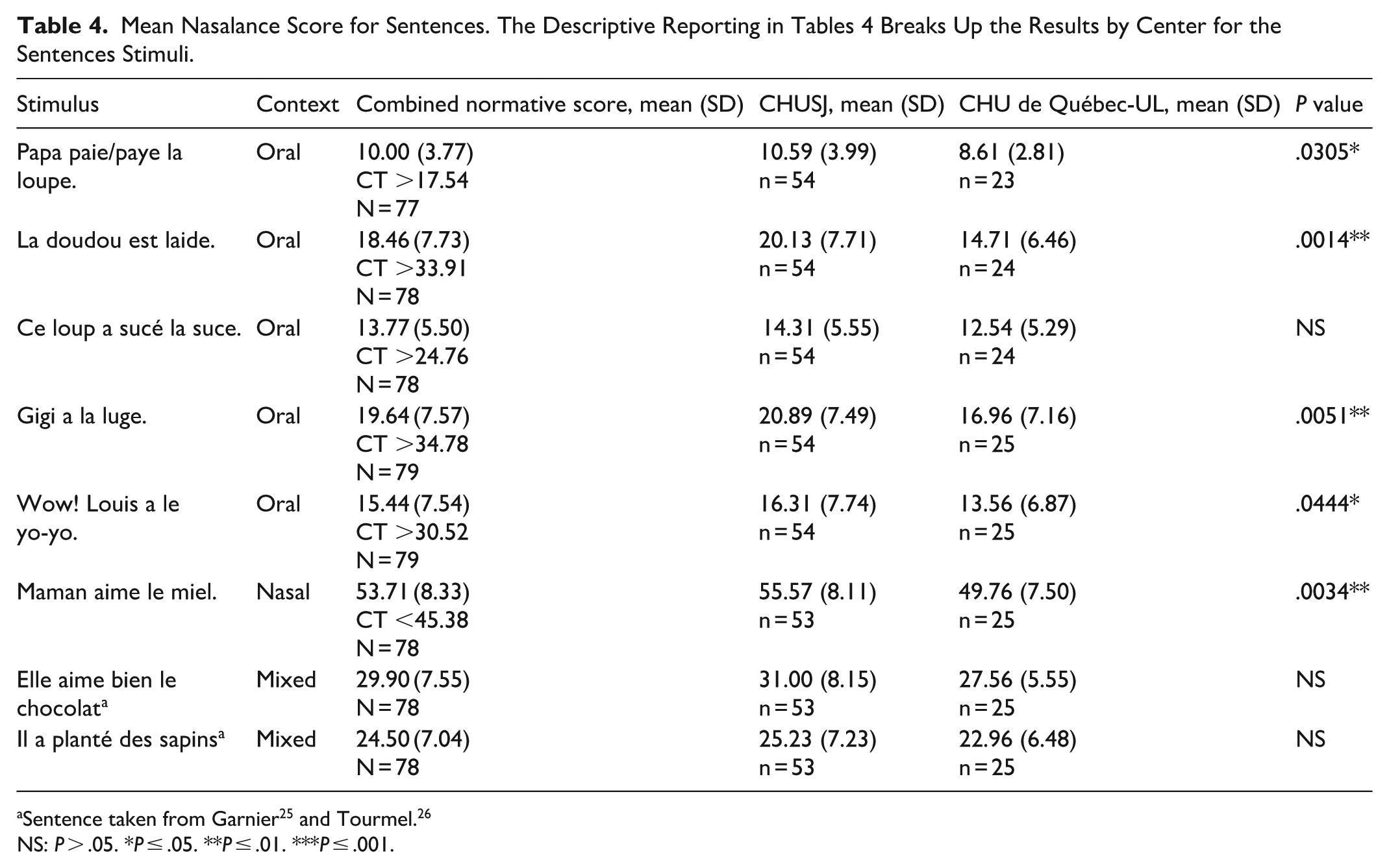
NS: P > .05. *P ≤ .05. **P ≤ .01. ***P ≤ .001.
The average nasalance score for all oral vowels was 14.12%. The highest nasalance score was obtained for the vowel /i/ (26.32%) and the lowest for the vowel /o/ (7.58%). For nasal vowels, the average nasalance score was 56.86%. The highest nasalance score was obtained for the vowel /ẽ/ (62.84%) and the lowest for the vowel /ɔ̃/ (50.88%). For repeated monosyllables, the average nasalance score was 34.95%. The highest nasalance score was obtained for the /mi/ (85.23%) and the lowest for the /ʃa/ (8.93%). In general, the highest nasalance scores were obtained for monosyllables that contained a nasal consonant. For the oral sentences, the average nasalance score was 15.46%. The phrase “Gigi a la luge” had the highest nasalance score (19.64%) while the phrase “Papa paie la loupe” had the lowest (10.00%). The nasalance score for the nasal sentence was 53.71%. For the phonetically mixed sentences, the average nasalance score was 27.20%. The sentence “Elle aime bien le chocolat” had the highest nasalance score (29.90%) and the sentence “Il plante des sapins” the lowest (24.50%). Finally, for the mixed text (“Le petit prince”), the nasalance score was 30.25%.
Statistical testing showed no significant differences between boys and girls, with the exception of the phonetically mixed sentence “Elle aime bien le chocolat” (girls mean 28.12, SD 7.56 vs boys mean 31.86, SD 78,13; P = .0100).
When the data for children in the age group 6;00 to 8;11 were compared to the age group 9;00 to 11;11, there were no significant differences except for the repeated syllable /mi/ (children 6;00-8;11 mean 84.39, SD 5.04, vs children mean 9;00-11;11 86.38, SD 4.76; P = .0465).
When the data for the speakers were compared by center, it was found that the nasalance scores for stimuli recorded at the Montreal site (CHUSJ) were always numerically higher than at the Quebec City site (CHU de Québec-UL), except for the 2 repeated syllables /kã/ and /dɔ̃/. Statistical testing showed that the nasalance scores for 15 out of the 28 stimuli (53.60%) were significantly higher at the CHUSJ. Therefore, the descriptive reporting in Tables 2 to 5 breaks up the results by center.
Mean Nalasance Scores for the Text. The Descriptive Reporting in Tables 5 Breaks up the Results by Center for the Text Stimulus.
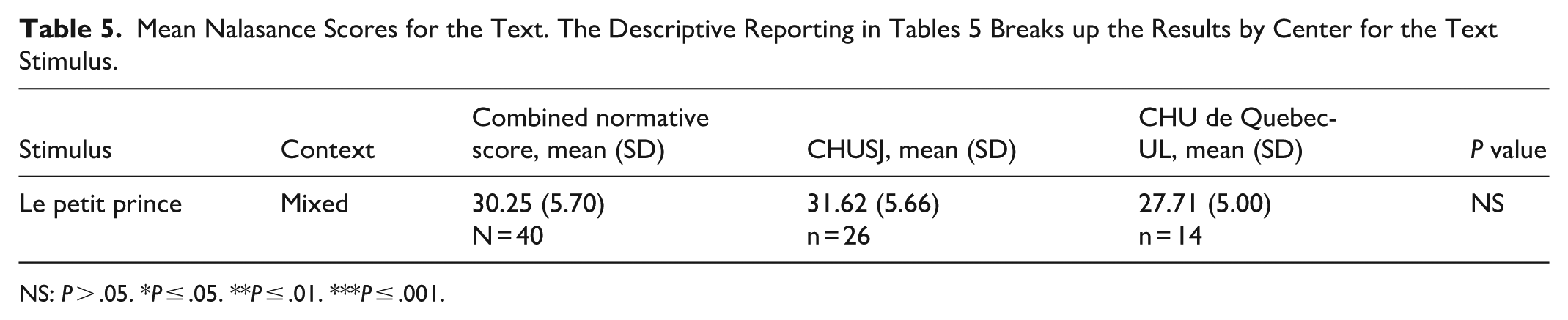
NS: P > .05. *P ≤ .05. **P ≤ .01. ***P ≤ .001.
Discussion
The present study established new stimuli as well as the first norms for nasalance scores for French-speaking children in Quebec aged 6;00 to 11;11 years. These can now be used by speech-language pathologists to assess children with resonance disorders who speak Quebec French. The overall results demonstrated that the stimuli worked as intended, with high nasalance scores for items loaded with nasal sounds, low scores for non-nasal stimuli and nasalance scores in-between the extremes for the phonetically balanced materials.
Together with the mean scores, theoretical critical threshold values were reported for each item according to the method suggested by Kummer. 38 However, these authors also emphasized that such thresholds are only approximate and that occasional normal speakers may straddle these boundary areas. While many of the reported estimated critical threshold scores appeared plausible, items such as the repeated syllables /ma/ and /mi/ had high mean scores with low standard deviations, so that the resulting theoretical critical thresholds were unrealistically high. The same observation could be made about the oral sentence “Papa paie la loupe,” which had the lowest nasalance scores of all the sentences. As a result, the estimated critical threshold was still lower than the mean nasalance scores of some of the cognate oral test sentences in this collection. Future research will be needed to determine more accurate cut-off scores for the test stimuli.
A direct comparison of the present data set with other previous data collections in French11,12,25-27 was not possible because of the differences in testing materials, French dialects and generations of nasometers used. Watterson 23 argues that, in general, nasalance scores lower than 20% for oral test sentences or texts can be considered typical. Dalston et al 40 first suggested a cut-off of 32% for hypernasality but then revised the cut-off to 28% in a later study. 41 Hardin et al 42 argued for a lower threshold of 26%. Based on a review of different studies, Watterson 23 suggested 30% as the cut-off for hypernasality, a range of 31% to 45% for mild to moderate hypernasality and over 45% for severe hypernasality. For sentence- or text-level speech stimuli loaded with nasal sounds, a threshold lower than 50% nasalance has been suggested as the diagnostic limit for hyponasality.42,43 Future research will have to demonstrate whether the cutoff scores for Quebec French would fall into similar ranges.
With the collection of the normative nasalance scores, it was also important to investigate possible effects of speaker sex, age and research sites. Between boys and girls, only 1 mixed sentence out of the 28 (3.6%) test items showed a significantly higher nasalance score for the boys. When the data for children in the age group 6 to 8 were compared to the age group 9 to 11, only 1 nasal syllable out of 28 (3.6%) test items had significantly higher nasalance scores for the group of older children. In both cases, the mean scores for the 2 groups were still within a few nasalance points of each other, so it is difficult to attach a particular meaning to these 2 isolated findings.
There were more systematic differences between the 2 centers. Almost all (26 out of 28, or 93%) nasalance scores for the stimuli recorded at the CHUSJ were numerically higher. For the 15 out of 28 (53.6%) items where significant differences were found, many of the P values were small, so these differences can probably be considered meaningful despite the large number of statistical tests.
The differences in nasalance scores between the 2 sites may be attributable to dialectal differences between the cities of Montreal and Quebec, to differences between the nasalance scores obtained by the nasometers in the 2 clinics, or to a combination of the 2. It is possible that dialectal differences could explain the differences between the 2 centers. In previous research, dialectal differences have been found to affect nasalance scores in different varieties of North American English (19) and Flemish (20). Canadian French has many regional dialectal varieties. The interested reader may listen to audio examples from the 2 regions in the publicly available “Atlas sonore des varietes de francais au Canada.” 44 The differences between Montreal and Quebec City French are subtle. While they may be recognizable to speakers of Quebecois French, the distinction may be more difficult to make for speakers of other varieties of French. The main differences relate to features such as vocabulary or vowel length differences. 45 French in the Province of Quebec is known for its phonological opposition between intrinsically short and intrinsically long vowels. For some words, this difference may even signal that the speaker comes from a specific region: French in the Montreal area generally has longer vowels, while that of the Quebec City area has shorter vowels. 45 Given that the nasometer measures nasalance mainly through vowels because of its bandpass filtering characteristics, 8 then longer nasalized vowels in 1 dialect could presumably lead to higher nasalance scores. This could explain the higher nasalance scores recorded at the CHUSJ located in Montreal.
The observed differences may also result from the nasometers itself. The study was conducted at 2 different sites, and with 2 different nasometers of the 6450 type. When Bressmann and Tang 46 compared nasalance scores obtained with 4 different nasometer headsets, they found that between 56.1% and 98.9% of measurements were within 3 nasalance points for the different pairs of headsets. The largest difference observed was 8 nasalance points. Unfortunately, the nasometers in the current study had been retired and the headsets could not be compared to verify whether the higher scores at the CHUSJ site were attributable to the specific characteristics of the microphones in the headset used at this site.
Limitations
The present study had several limitations that should be considered when interpreting the findings. Some of the test sentences were quite short. This was done deliberately to ensure that they could be read or repeated even by very young or preliterate children. In general, the nasalance scores obtained with short stimuli can be equivalent to those obtained with longer text passages. 47 However, a few sentences were shorter than the minimum length of 6 syllables as recommended by Watterson et al. 24 This could potentially increase the variability of the nasalance scores obtained with these test stimuli.
In the statistical analysis, numerous inferential tests were computed. This was considered a prudent approach because of differences in the number of speakers and the nature of the data distributions for the different test items. The statistical findings showed that many of the nasalance data recorded at the CHUSJ in Montreal were significantly higher than at the CHU de Québec-UL in Quebec City, which was considered a plausible finding. For the 2 isolated findings for sex and age, it was more difficult to decide whether these were meaningful differences or spurious statistical effects. Finally, it could not be conclusively resolved whether the higher nasalance scores at the CHUSJ site were the result of dialectal differences or of measurement differences between the nasometers used. However, it was also important to ensure that the norms represented pediatric speakers of Quebec French from different geographical regions.
Conclusion
This study developed normative nasalance scores data for French-speaking children in Quebec aged between 6;00 and 11;11 years old. These normative scores can now be used by speech-language pathologists working with French-speaking pediatric patients with craniofacial conditions such as cleft palate, as well as with children with speech disorders related to velopharyngeal dysfunction of other origin. With normative scores, the nasometer can be better used to corroborate clinicians’ auditory-perceptual assessments, to support the team in making treatment decisions for the patient, and to measure a patient’s progress following speech therapy or surgery.
The variety of test items with normative scores presented here provides the clinician with a range of options for testing clients with different linguistic or developmental abilities. The assessment can be adapted to the clinician’s needs and the child’s characteristics.
In future research, the assessment protocol will be used with speakers with resonance disorders – that is, oral-nasal imbalances – in order to establish reliable diagnostic cut-off scores for hypernasality and hyponasality for children speaking Quebec French.
Footnotes
Acknowledgements
This project was made possible through the support of the speech-language pathologists who are members of the Community of Practice in Velopharyngeal Dysfunction and Orofacial Malformations in Quebec. The authors would like to thank Luc Ostiguy, retired professor, for his important intellectual contribution to the project, Jérémie Duval, audiologist, for her advice on audiological screening procedures, Farzane Youssefi, speech-language pathologist, for her dedicated involvement in data collection and Narcisse Singbo for his assistance with the statistical analysis. We are also grateful to the families and the children who gave their time to participate in this study.
ORCID iDs
Ethical Considerations
This multi-site study protocol was reviewed and approved by Comité d’Ethique de la Recherche, CHU Sainte-Justine (approval number #MP-21-2017-1357).
Consent to Participate
Written informed consent was obtained from the parents of the children participating in the study.
Author Contributions
All authors contributed to the research and preparation of this manuscript. Marie-Ève Caty was instrumental in the conceptualization, methodology development and supervision of the study, in collaboration with all the other authors. Annie Salois, Andréanne Mayrand and Ericka Beaudoin obtained funding, collected the data together with their team members and administered the project at their respective sites. Tim Bressmann helped with the analysis and interpretation of the study findings. All authors contributed to the writing and editing of the manuscript.
Funding
The authors disclosed receipt of the following financial support for the research, authorship and/or publication of this article: This research has been supported by funding granted by Association francophone pour le savoir (ACFAS), the Fondation du CHU de Québec-Université Laval and the Conseil Multidisciplinaire du CHU Sainte-Justine. The funders had no role in the design, data collection, data analysis, and reporting of this study.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Data Availability Statement
The data supporting the findings of this study are available from the corresponding author upon reasonable request.