
Abstract
Purpose:
The present study compares lower eyelid complication rates between preseptal and retroseptal transconjunctival approaches for orbital fracture repair.
Methods:
MEDLINE, Embase, Cochrane, and Web of Science were searched from inception to November 2024 in accordance with PRISMA 2020 guidelines. Studies were included if they reported original data (n > 1) on orbital or peri-orbital fracture repair using either preseptal or retroseptal transconjunctival approaches, with at least 1 postoperative lower eyelid complication. Both comparative and single-arm studies were included due to limited available evidence. Risk of bias was assessed using RoB 2.0, ROBINS-I, and MINORS tools as appropriate. Pooled proportions and risk ratios were calculated using random-effects meta-analysis.
Results:
Three hundred studies were screened and 39 studies (n = 2665 patients) met inclusion criteria. Of these, 1976 patients underwent preseptal and 689 underwent retroseptal approaches. For isolated orbital floor fractures, a retroseptal approach was used more often (59.9%) than a preseptal approach (34.9%). Scleral show was the most frequent complication overall (1.4%) and was more common in retroseptal cases (2.9%) than in preseptal cases (0.9%). Entropion occurred in 0.8% of preseptal and 0.9% of retroseptal cases; ectropion occurred in 0.4% and 0.7%, respectively. The pooled proportion of total eyelid complications was 2% (95% CI: 1-5) for preseptal and 3% (95% CI: 1-9) for retroseptal approaches. Meta-analysis of 5 comparative studies (n = 556) demonstrated no significant difference in complication risk (RR 0.80; 95% CI: 0.26-2.41). GRADE certainty of evidence was moderate.
Conclusions:
Both transconjunctival approaches associated with low complication rates, but they are not clinically interchangeable. Retroseptal access may be preferred in older patients or isolated fractures requiring minimal dissection, while preseptal incisions may benefit younger patients or complex fractures requiring broader exposure. Until stronger comparative evidence emerges, patient anatomy and fracture pattern should guide approach selection.
Keywords
Introduction
Facial fractures, particularly orbital fractures, are a common injury that often requires surgical intervention. Approximately 1 in 3 facial fractures have orbital involvement, and about 10% of all facial fractures are isolated orbital wall fractures, the most common type of which is the orbital floor fracture.1,2 To access the infraorbital rim and orbital floor, several surgical approaches through the lower eyelid can be used. 3 The transconjunctival approach is favored by many surgeons because it avoids leaving externally visible scars, an important consideration for esthetic outcomes. However, this approach carries potential risks of ocular and lower lid complications, such as corneal abrasion, ectropion, entropion, and scleral show, which can significantly affect both visual function and the esthetics of the lower lid postoperatively. 4 While existing literature highlights the esthetic benefits of the transconjunctival approach, recent literature indicates that this technique may also carry an increased risk of lower lid complications compared to external approaches. 5
Two commonly used variations of the transconjunctival approach are the preseptal and retroseptal techniques. The preseptal approach, which involves dissecting from the conjunctiva to a surgical plane that is superficial to the orbital septum, is thought to better preserve the peri-orbital fat and structural elements of the lower eyelid in order to reduce complication rates, though it is technically more demanding. 6 In contrast, the retroseptal approach is simpler and quicker but is thought to theoretically increase risk of lower lid complications via disruption of lower lid structural integrity, though this has not been reliably demonstrated in the literature. 7 No consensus has been reached regarding which transconjunctival variation is the superior technique for minimizing complications. Thus, a systematic review comparing the 2 techniques was performed to inform surgical decision-making, all with the aim of improving patient outcomes.
Research Question
In patients undergoing surgery for orbital fractures (population), does the preseptal transconjunctival approach (intervention) decrease the risk of lower lid complications (outcome) compared to the retroseptal transconjunctival approach (comparison)?
Methods
Search Strategy
This systematic review protocol was formulated adhering to the 2020 Preferred Reporting Items for Systematic reviews and Meta-Analyses (PRISMA) Checklist. 8 The original search occurred in November of 2024, including 4 databases (Embase, MEDLINE, Cochrane, and Web of Science) from 1946 to 2024. The following search terms were used: “exp Orbital fractures/or exp Orbital floor fractures/or exp Orbital wall fractures/ or (facial trauma* or orbital trauma* or orbital fracture* or maxillofacial injur*)) and ((Preseptal* or preseptal approach* or transconjunctival* or preseptal orbital* or preseptal eyelid*)) and ((Retroseptal* or Retroseptal approach* or transconjunctival* or Retroseptal orbital* or Retroseptal eyelid* or Retroseptal* or retroseptal approach* or transconjunctival* or retroseptal orbital* or retroseptal eyelid*)) and limit to (english language and humans).” Complete strategy is described in Figure 1. This systematic review was prospectively registered with PROSPERO (CRD42024520816).
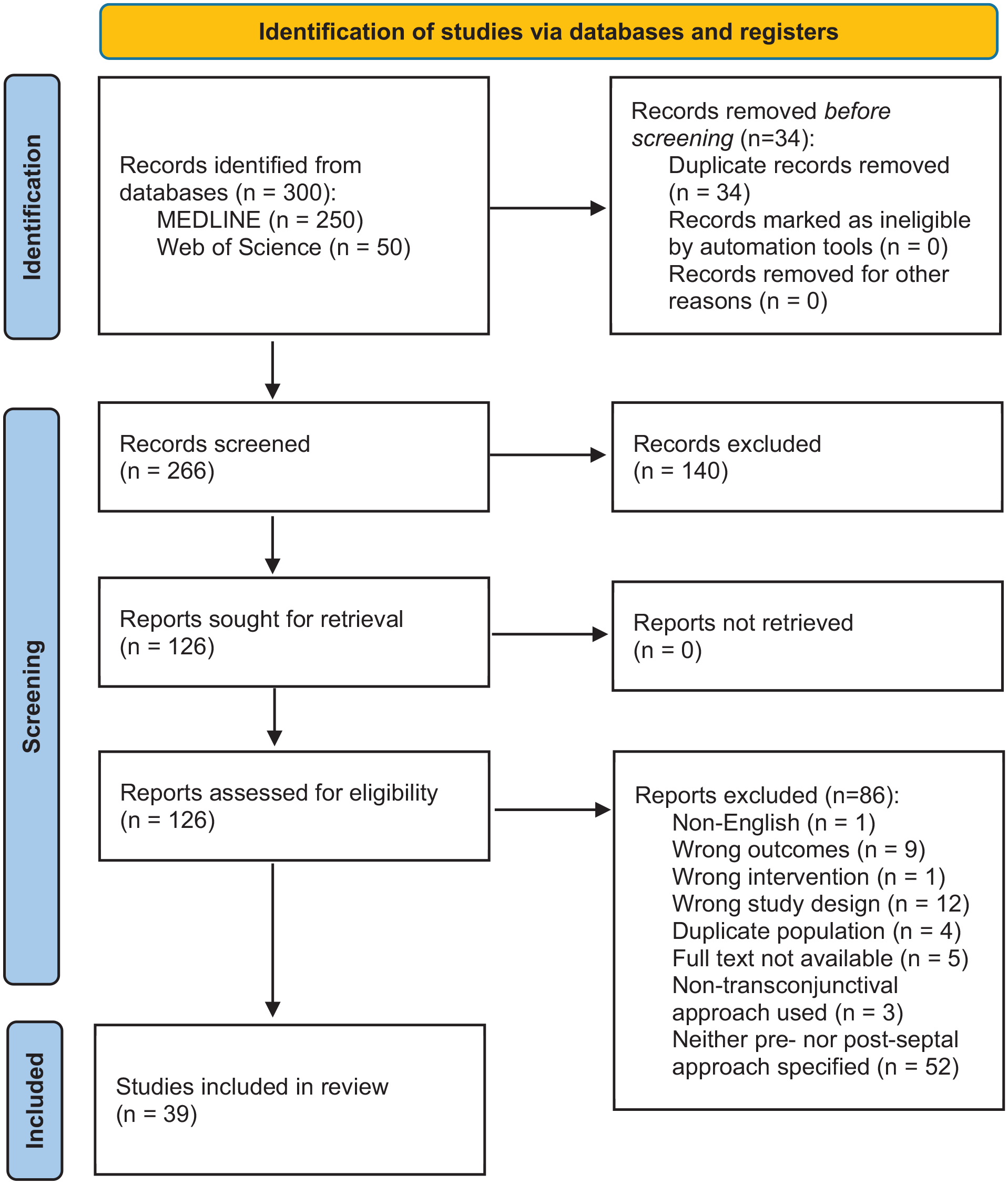
PRISMA 2020 flow diagram for study selection. The process of identifying, screening, and including studies in the systematic review following the PRISMA 2020 guidelines is outlined above. 7 A total of 300 records were identified through database searches (MEDLINE, Web of Science, and Cochrane) and 39 studies were included in review.
Inclusion Criteria
Inclusion criteria were as follows: patients who have undergone surgery for orbital or peri-orbital fractures using a transconjunctival approach, with either the preseptal or retroseptal approach clearly identified and/or described. All patient ages, genders, and geographic locations were included. Studies must have reported original patient data (n ≥ 2), including at least one postoperative lower lid complication (ectropion, entropion, or scleral show). Both randomized controlled trials and non-randomized studies (eg, cohort studies, case series) were included from all years to capture as much relevant data as possible. Given the scarcity of direct comparative studies, non-comparative studies were included. Any comparative studies identified were reported separately from non-comparative studies to mitigate resultant bias.
Exclusion Criteria
Studies were excluded if they exclusively reported on surgeries that were unrelated to orbital fractures, such as ophthalmologic procedures. Patients undergoing revision procedures were excluded, to minimize the confounding effect of an increased risk of complications with multiple lower lid procedures. Additionally, studies that reported fewer than 2 patients were excluded due to insufficient data for meaningful analysis. Reviews, meta-analyses, commentaries, and animal or cadaveric studies were excluded as they lack original human data. Studies that did not specify whether the preseptal or retroseptal approach was used were excluded to maximize the validity of comparative analysis. Finally, studies involving concurrent eyelid procedures or modifications of the transconjunctival technique beyond simple pre- or retroseptal variations were excluded to avoid confounding factors in assessing complication rates.
Study Selection and Assessment
In the first step of the review, establishment of agreement between 2 reviewers (JH and PK) was undertaken. This involved scanning the titles and abstracts of articles. Selected articles were then screened at the full text level (JH and PK) and assessed for eligibility based on the inclusion and exclusion criteria. The 2 reviewers discussed any discrepancies that arose, with a third reviewer (JR) available for final resolution.
Data Extraction
A standardized data collection form was developed and included relevant variables to extract data from the selected articles. Based on our study objectives, the form included the following variables: study information (title, author, year, country, journal, study design), demographic information (number of eyes operated on, sex, age, orbital fracture (isolated orbital fracture vs other), comorbidities, history of surgery to the orbital area), intervention information (preseptal or retroseptal transconjunctival approach, time following fracture), and outcomes/outcome measures (postoperative lid complications, operative time, time to followup (max followup and time at which the complication was identified)).
The risk of bias for included studies was assessed by 2 independent reviewers (PK and CW) using the recommendations of the Cochrane Handbook for Systematic Reviews of Interventions. 9 Disagreements were resolved through discussion and by consensus. As such, for randomized control trials, the tool used was the Risk of Bias 2.0 Cochrane tool (RoB 2.0), 10 and for each included study, the domains assessed by reviewers were: bias due to deviations from intended interventions, bias due to deviations from the intended intervention, bias in measurement of outcome, and bias in selection of the reported result. A RoB 2.0 version for crossover (matched) trials was used for studies with within-subject design. For each study, a decision regarding the risk of bias for each domain was judged to be “low,” “some concerns,” or “high,” informing a decision about the overall risk of bias for each study based on these domains. For non-randomized studies, the ROBINS-I (Risk of Bias in Non-randomized Studies of Interventions) tool from Cochrane was used to assess the risk of bias. 11 This tool evaluates potential biases across domains including: confounders, selection, deviations from intended interventions, missing data, selection of the reported result, and measurement of outcomes, with judgments similar to the RoB 2.0 tool, indicating low, moderate, serious, or critical risk of bias for each study. Lastly, non-comparative case series were assessed using the Methodological Index for Non-Randomized Studies (MINORS). 53
Statistical Analysis
Descriptive statistics were calculated for study characteristics, patient demographics, operative details, and reported complications. Continuous variables were summarized as weighted means where appropriate, using study sample sizes to account for differential contributions. Proportion meta-analyses were performed to estimate pooled event rates for eyelid complications using a generalized linear mixed model (GLMM) with logit transformation. Pooled proportions are reported with 95% confidence intervals (CIs), and heterogeneity was assessed using the I2 statistic.
For studies directly comparing the preseptal and retroseptal transconjunctival approaches, a random-effects meta-analysis was conducted to calculate pooled risk ratios (RRs) with 95% CIs for total eyelid complications. Between-study heterogeneity was evaluated using the I2 statistic and Cochran’s Q test. An I2 value greater than 50% was considered indicative of substantial heterogeneity. 12 The certainty of evidence for the main outcome (total eyelid complications) was assessed using the Grading of Recommendations, Assessment, Development and Evaluations (GRADE) framework. 13 All analyses were conducted using R version 4.4.1 with the meta and metafor packages. 14
Results
Study and Patient Characteristics
A total of 300 studies were identified through database searches, and 66 full-text articles were assessed for eligibility. Ultimately, 39 studies were included in the analysis6,7,15 -51 (Figure 1). Study characteristics are summarized in Table 1. Most studies were either case series (Level IV, 30/39; 76.9%) or prospective cohort studies (Level III, 6/39; 15.4%), while 3 were lesser-quality randomized controlled trials (Level II, 3/39; 7.7%). The majority were published between 2010 and 2020 (21/39; 53.8%). The most frequent countries of publication were the United States (9/39; 23.1%), India (5/39; 12.8%), Italy (5/39; 12.8%), Japan (4/39; 10.3%), and South Korea (4/39; 10.3%).
Characteristics of Included Studies.
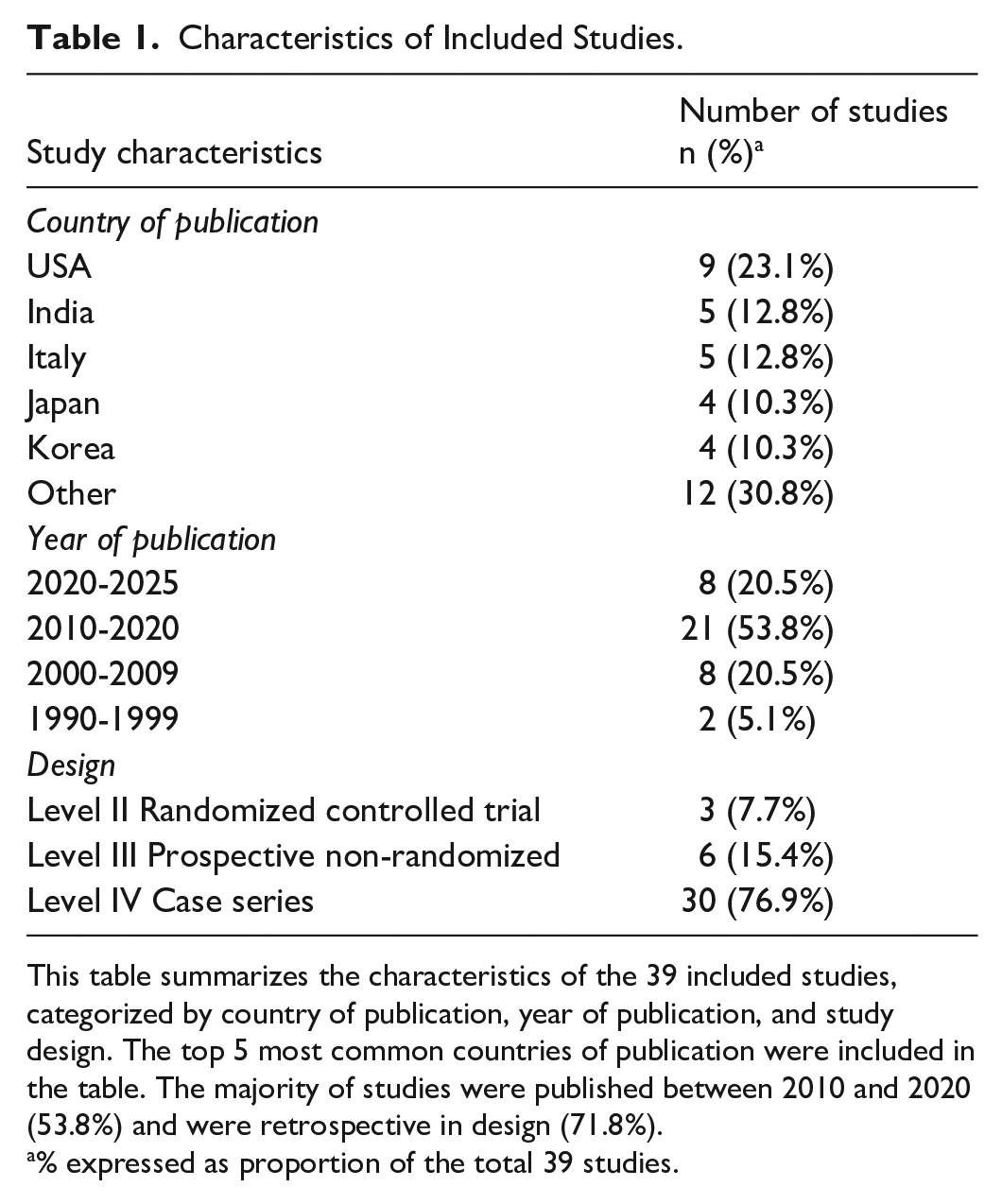
This table summarizes the characteristics of the 39 included studies, categorized by country of publication, year of publication, and study design. The top 5 most common countries of publication were included in the table. The majority of studies were published between 2010 and 2020 (53.8%) and were retrospective in design (71.8%).
% expressed as proportion of the total 39 studies.
In total, 2665 patients were included: 1976 underwent preseptal transconjunctival approaches and 689 underwent retroseptal approaches (Table 2). The weighted mean age was 38.5 years (SD 4.91) in the preseptal group and 39.1 years (SD 7.38) in the retroseptal group. Mean time from injury to surgery was 9.8 days for preseptal and 11.1 days for retroseptal patients. The most common fracture type in both groups was isolated orbital floor fracture (preseptal: 689/1976; 34.9%; retroseptal: 414/689; 59.9%).
Patient and Operative Characteristics of Included Studies.
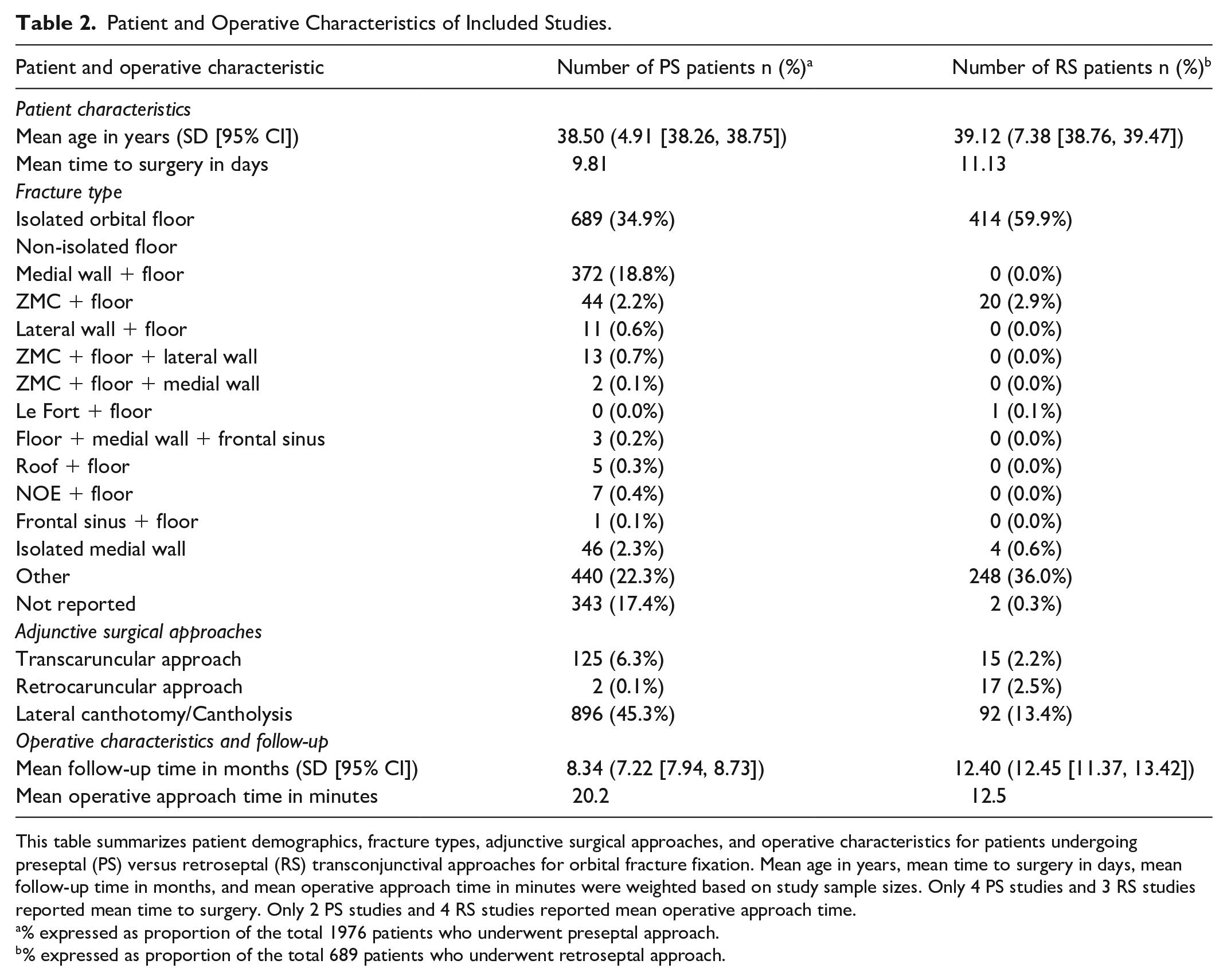
This table summarizes patient demographics, fracture types, adjunctive surgical approaches, and operative characteristics for patients undergoing preseptal (PS) versus retroseptal (RS) transconjunctival approaches for orbital fracture fixation. Mean age in years, mean time to surgery in days, mean follow-up time in months, and mean operative approach time in minutes were weighted based on study sample sizes. Only 4 PS studies and 3 RS studies reported mean time to surgery. Only 2 PS studies and 4 RS studies reported mean operative approach time.
% expressed as proportion of the total 1976 patients who underwent preseptal approach.
% expressed as proportion of the total 689 patients who underwent retroseptal approach.
Intervention Characteristics
Operative details are presented in Table 3. Alloplastic materials were the most commonly used for orbital floor reconstruction in both groups (preseptal: 13/15 studies; 86.7%; retroseptal: 6/8 studies; 75.0%). Closure was most often performed with absorbable sutures (preseptal: 13/20; 65.0%; retroseptal: 6/10; 60.0%), with sutureless techniques used less frequently (preseptal: 4/20; 20.0%; retroseptal: 2/10; 20.0%). Frost sutures were used in only a minority of studies (preseptal: 4/18; 22.2%; retroseptal: 2/9; 22.2%). Lateral canthotomy/cantholysis was more frequently performed in the preseptal group (896/1976 eyelids; 45.3%) compared to the retroseptal group (92/689 eyelids; 13.4%).
Operative Characteristics Stratified by Study.
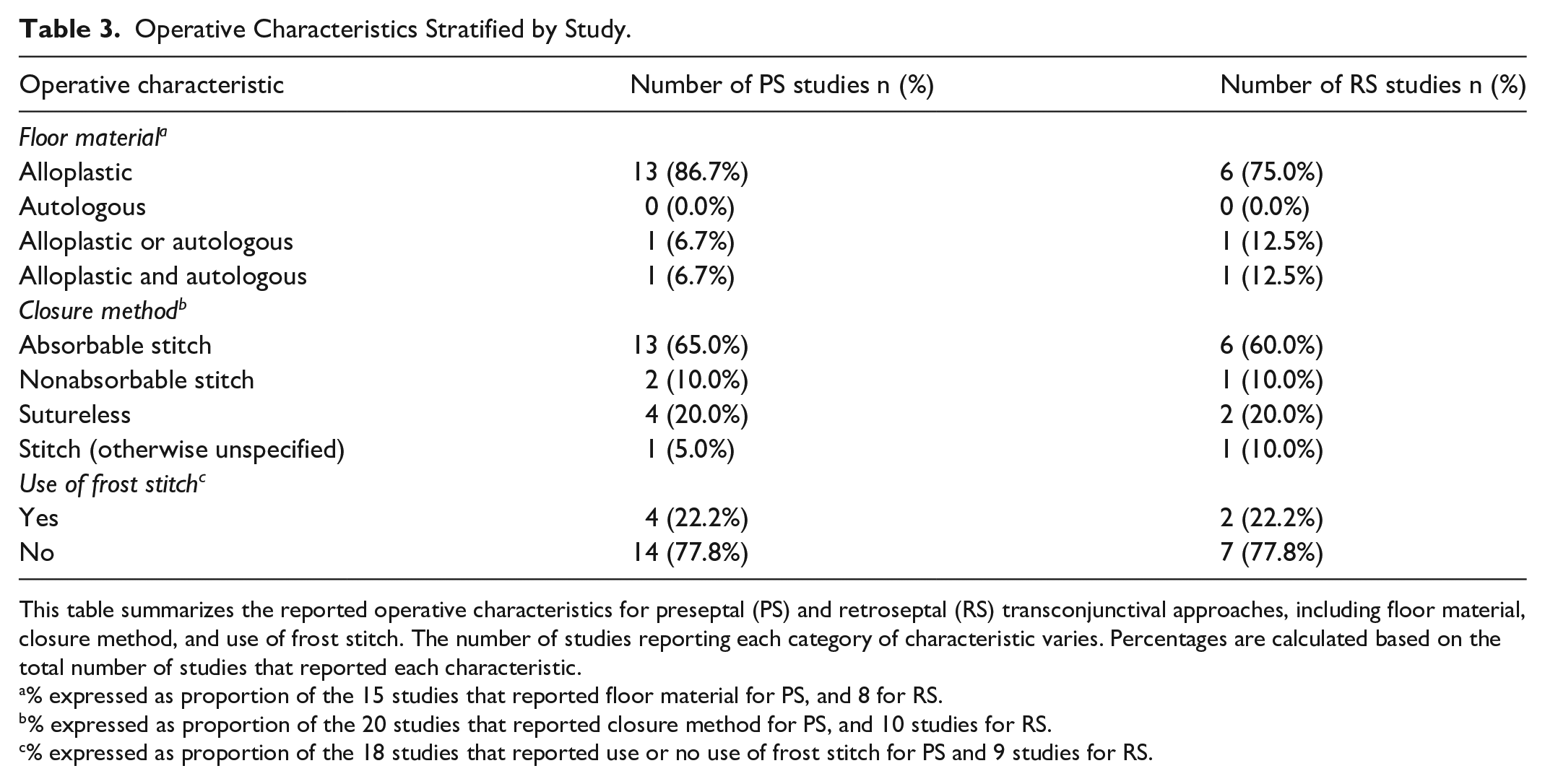
This table summarizes the reported operative characteristics for preseptal (PS) and retroseptal (RS) transconjunctival approaches, including floor material, closure method, and use of frost stitch. The number of studies reporting each category of characteristic varies. Percentages are calculated based on the total number of studies that reported each characteristic.
% expressed as proportion of the 15 studies that reported floor material for PS, and 8 for RS.
% expressed as proportion of the 20 studies that reported closure method for PS, and 10 studies for RS.
% expressed as proportion of the 18 studies that reported use or no use of frost stitch for PS and 9 studies for RS.
Mean operative time for the lower lid approach was 20.2 minutes for the preseptal approach (reported in 2 studies) and 12.5 minutes for the retroseptal approach (4 studies). Mean follow-up duration was 8.3 months (SD 7.2) for preseptal patients and 12.4 months (SD 12.5) for retroseptal patients.
Outcomes and Outcome Measures
Pooled complication rates are shown in Table 4. The pooled proportion of total eyelid complications was 2% (95% CI: 1-5; I2 = 69.2%) in the preseptal group and 3% (95% CI: 1-9; I2 = 19.7%) in the retroseptal group. Scleral show was the most common specific complication (preseptal: 18/1976; 0.9%; retroseptal: 20/689; 2.9%), followed by entropion (preseptal: 16/1976; 0.8%; retroseptal: 6/689; 0.9%) and ectropion (preseptal: 7/1976; 0.4%; retroseptal: 5/689; 0.7%). Eyelid revision was reported only in the preseptal group (13/1976; 0.7%).
Complications Summary and Pooled Proportions of Patients in Included Studies.
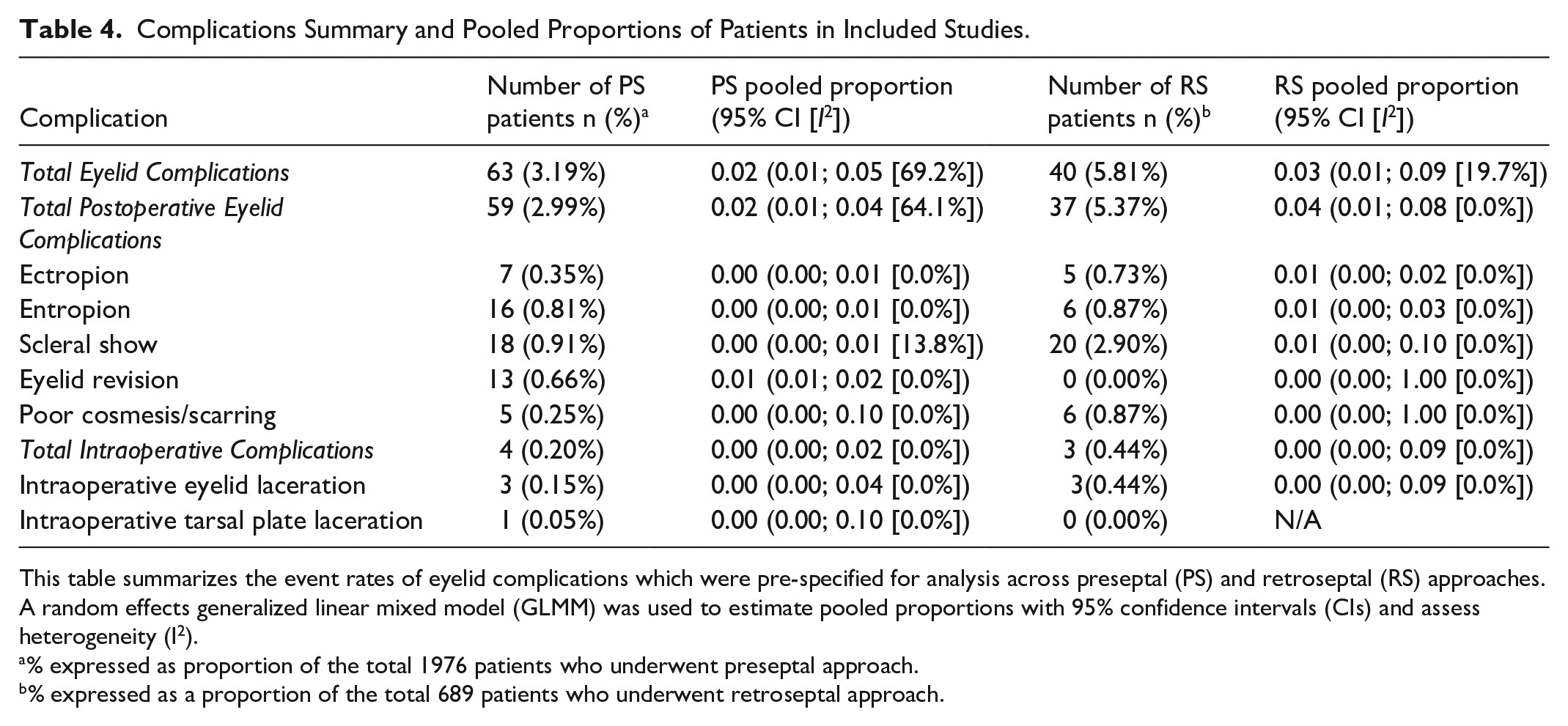
This table summarizes the event rates of eyelid complications which were pre-specified for analysis across preseptal (PS) and retroseptal (RS) approaches. A random effects generalized linear mixed model (GLMM) was used to estimate pooled proportions with 95% confidence intervals (CIs) and assess heterogeneity (I2).
% expressed as proportion of the total 1976 patients who underwent preseptal approach.
% expressed as a proportion of the total 689 patients who underwent retroseptal approach.
Intraoperative complications were rare in both groups (Table 4), with only 3 intraoperative tarsal plate lacerations reported among preseptal cases (3/1976; 0.15%) and 3 intraoperative eyelid lacerations in the retroseptal group (3/689; 0.44%).
Other non-predefined complications were infrequent (Supplemental Figure 3). Trichiasis occurred in 8 preseptal patients (0.4%) and 4 retroseptal patients (0.6%). Granulomas were seen in 3 preseptal patients (0.15%) and 1 retroseptal patient (0.15%), and epiphora in 2 preseptal patients (0.1%).
Meta-analysis of 5 comparative studies (n = 556 patients) showed no statistically significant difference in the risk of total eyelid complications between approaches (RR 0.80; 95% CI: 0.26-2.41; I2 = 0%; Figure 2). GRADE assessment rated the certainty of evidence as moderate due to imprecision in the pooled risk estimate (Supplemental Figure 4).
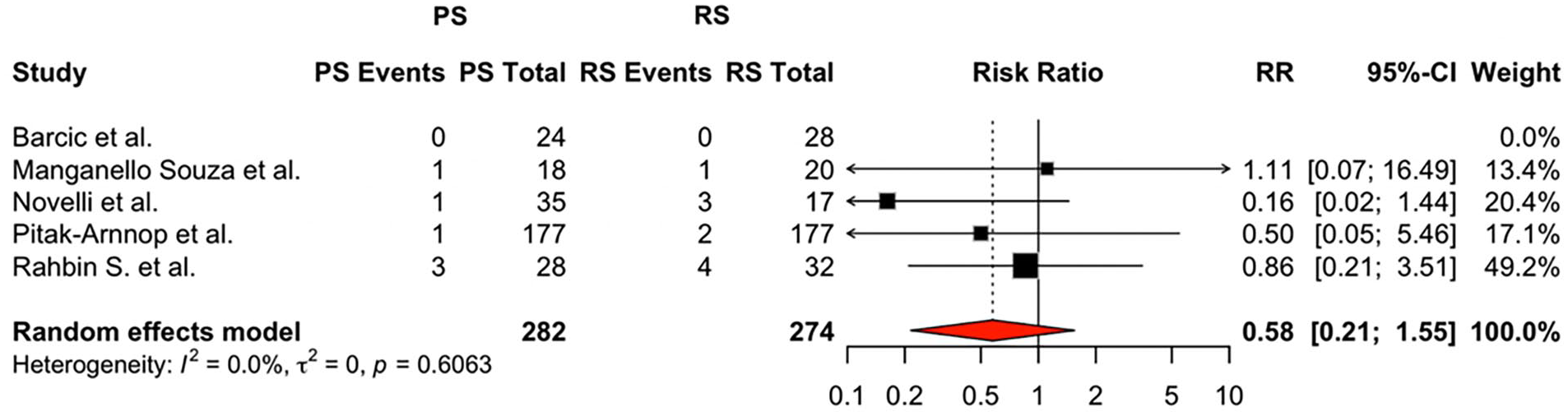
Forest plot comparing postoperative eyelid complications between PS-TCA and RS-TCA. This plot shows the risk ratios (RR) with 95% confidence intervals (CIs) for postoperative eyelid complications across 5 comparative studies, created on R. Counts represent the number of patients experiencing eyelid complications (PS Events, RS Events) relative to the total number of patients in each surgical approach group (PS Total, RS Total). A random-effects model was used for meta-analysis, as clinical and methodological variability was expected across studies. The pooled RR was 0.80 (95% CI: 0.26-2.41), suggesting no significant difference between preseptal (PS) and retroseptal (RS) transconjunctival approaches. Heterogeneity was assessed using Cochran’s Q test and I2 statistic, with I2 = 0.0%, indicating no observed between-study variability.
Risk of Bias
Risk of bias was assessed using 3 established tools, selected based on study design and intent to evaluate treatment effects. Each tool assessed relevant domains as per its framework and is summarized in Supplemental Figures 3 and 4.
Randomized controlled trials (RCTs) were evaluated using the Cochrane Risk of Bias 2.0 (RoB 2.0) tool. 52 Three RCTs (Giraddi et al, 20 Mohamed et al, 29 and Pitak-Arnnop et al 36 ) were included. Of these, one study (Giraddi et al 20 ) was judged to be at high overall risk of bias, largely due to serious concerns in outcome measurement. The other 2 were rated as having “some concerns,” either due to unclear randomization procedures or limited outcome blinding29,36 (Supplemental Figure 1). Sixteen non-randomized interventional studies were assessed using the ROBINS-I (Risk Of Bias In Non-Randomized Studies of Interventions) tool. 11 This tool is appropriate for studies that aim to estimate the effect of an intervention, regardless of whether they included a concurrent comparison group. Two of these studies were formally comparative (ie, evaluated both preseptal and retroseptal approaches), and the remaining 14 reported outcomes following a single surgical approach but inferred treatment effects—aligning with the intended application of the ROBINS-I tool. Across these studies, most were judged to have moderate overall risk of bias, typically due to confounding, unclear selection methods, or lack of adjustment for baseline differences. A subset showed serious or critical risk of bias due to missing data or poor outcome measurement (eg, De Riu et al, 18 Cortese et al, 17 and Neovius et al 30 ), and were downgraded accordingly (Supplemental Figure 2).
The remaining 20 studies were non-comparative case series, assessed using the Methodological Index for Non-Randomized Studies (MINORS). 53 This validated instrument is designed for non-randomized studies reporting clinical outcomes, and includes 8 domains for non-comparative studies such as clearly stated aim, consecutive inclusion, prospective data collection, and appropriate endpoints. Across these studies, the mean MINORS score was 14.3 ± 2.6 (out of a maximum of 24), indicating moderate methodological quality. Domains with the lowest scores included blinding of outcome assessors and prospective sample size calculation, both of which were either absent or not reported in nearly all studies. Conversely, most studies scored well in domains related to aim clarity and endpoint appropriateness.
Discussion
This systematic review is the only systematic review to date that assesses lower eyelid complications following preseptal and retroseptal transconjunctival approaches in orbital fracture repair. While a range of lower eyelid incisions remain in use—including subciliary and subtarsal incisions—the transconjunctival approach has garnered increasing favor due to its avoidance of visible scarring and potential for improved esthetic outcomes. 54 As such, interest has grown not just in whether to use a transconjunctival incision, but in how best to execute it. This study synthesizes over 2600 patients from 39 studies and evaluates both approaches in the context of complication profiles, technical variations, and reporting quality.
Although both approaches were associated with low complication rates, subtle differences in complication profiles emerged that may have clinical relevance. The most notable disparity was in scleral show, observed in 2.9% of retroseptal cases compared to 0.9% of preseptal cases (Table 4). This finding may reflect a greater risk of vertical lid malposition when dissecting through deeper planes and manipulating orbital fat. In contrast, eyelid revision procedures occurred exclusively in preseptal patients (0.7%), potentially due to anterior lamellar contracture or orbicularis scarring from more superficial dissection. Rates of entropion (0.8% vs 0.9%) and ectropion (0.4% vs 0.7%) were nearly identical between groups. These differences, while not statistically significant, highlight that there is likely importance in matching dissection plane to patient anatomy. In older patients, or those with lower lid laxity, prior blepharoplasty, or reduced orbicularis tone, the retroseptal approach may be advantageous, as it preserves anterior lamellar attachments and avoids additional tension on already weakened structures. In contrast, younger patients with firm lower lids and robust soft tissue tone may tolerate preseptal dissection well, particularly when anterior exposure (ie, the orbital rim) is prioritized. Surgeons should interpret these trends not as deterministic risks, but as patient-modifying factors to guide approach selection during preoperative planning.
Intraoperative data from the included studies offer further insight into when and why each approach is chosen. The retroseptal technique had a shorter mean operative approach-to-floor time (12.5 vs 20.2 minutes for the preseptal approach), reinforcing its appeal in settings where procedural efficiency is prioritized or exposure is straightforward (Table 2). That said, total operative time for procedures was sparsely reported and therefore not analyzed, and so whether a preseptal approach truly lengthens the entire procedure is not known. Somewhat unexpectedly, lateral canthotomy—a maneuver often used to expand access in tight or complex surgical fields—was performed in 45.3% of preseptal cases but only 13.4% of retroseptal cases. This finding contradicts the conventional belief that retroseptal access may be more restrictive and may reflect publication patterns, surgeon comfort, or case selection bias. Additional intraoperative details—such as similar rates of absorbable suture closure (65.0% preseptal vs 60.0% retroseptal) and sutureless techniques (20% in both)—suggest that closure method may be driven more by institutional or surgeon preference than by approach (Table 3). Frost sutures were rarely used in either group. Collectively, these findings imply that preseptal approaches may be more frequently selected in challenging cases where adjunctive maneuvers like canthotomy are anticipated, while retroseptal incisions may serve as the workhorse for routine orbital floor access.
The predominance of preseptal reports in the literature (1976 vs 689 retroseptal patients) likely reflects more than just clinical frequency. Publication and selection bias almost certainly play a role. Preseptal techniques are sometimes perceived as more anatomically conservative or technically elegant, making them more attractive to authors and reviewers alike. In contrast, the simplicity of the retroseptal approach may render it less frequently published despite likely widespread use. As such, the skew in reported cases may not mirror real-world practice, and care must be taken not to conflate publication volume with clinical preference or superiority. This observation reinforces the notion that broader, registry-based reporting to ensure equitable representation of all standard approaches in the surgical literature should be pursued.
The quality of included studies was variable and, in many cases, limited. Only 3 randomized controlled trials were identified, published in 2012, 2021, and 2024.20,29,36 Two were judged to have “some concerns” and one was rated high risk due to deficiencies in outcome measurement (Supplemental Figure 1). Sixteen non-randomized studies were assessed using the ROBINS-I tool and most (10 studies) were judged to have moderate risk of bias, frequently due to lack of adjustment for fracture complexity, unclear patient selection, and inconsistent outcome definitions (Supplemental Figure 2). Several studies (eg, De Riu et al 18 , Cortese et al, 17 Neovius et al 30 ) had serious or critical risk of bias and were downgraded accordingly. The remaining 20 case series were assessed using the MINORS instrument and demonstrated an average score of 14.3 ± 2.6, consistent with moderate methodological rigor. Common deficiencies included the absence of sample size calculation, prospective enrollment, and blinded assessment. Importantly, the inclusion of these single-arm studies was intentional and necessary to maximize the completeness of this review in light of the paucity of well-controlled comparative studies. Nevertheless, these limitations reduce the precision of pooled estimates and reinforce the need for more structured research designs in future work.
Despite these limitations, our findings suggest that preseptal and retroseptal transconjunctival approaches are not likely functionally interchangeable, and that patient selection should be informed by both anatomical considerations and operative goals. In our dataset, the retroseptal approach had a shorter mean exposure time (12.5 minutes vs 20.2 minutes) and was used in fewer cases requiring lateral canthotomy (13.4% vs 45.3%), suggesting it may be favored for isolated orbital floor fractures with straightforward access. While traditionally considered more limited in exposure, the retroseptal approach avoids dissection along the anterior lamella and may better preserve orbicularis and skin attachments, making it a rational choice in older patients, or those with preexisting eyelid laxity, prior lower lid surgery, or diminished orbicularis tone—features that heighten the risk of vertical lid malposition. 7 In contrast, the preseptal approach was more commonly reported (1976 vs 689 patients) and appeared to be selected in more complex cases, such as non-isolated orbital fractures (65.9% of cases in the pre-septal group vs 40.1% of cases in the retroseptal group), where broader exposure and enhanced access are often necessary. Therefore, a preseptal approach may be advantageous in younger patients with firmer anterior lamellar support, where the sequelae of orbicularis contracture is reduced, and in situations where preservation of orbital fat is desired, such as in patients with shallow orbits or those at risk of postoperative hollowing. Conversely, some may argue the opposite—that the preseptal route, being anterior and more superficial, should be reserved for those who are older to avoid direct fat manipulation; however, our data did not show higher rates of scleral show or ectropion in the preseptal group, and revision procedures occurred only in that cohort (13/1976; 0.7%), suggesting that contracture affecting the anterior lamella may be a more relevant risk than intraorbital fat disruption in this setting. Ultimately, our review demonstrates that the literature does not currently support the notion that 1 approach should be considered universally superior over the other. Instead, the the selection of a preseptal versus retroseptal approach should account for the anatomical demands of the fracture, the patient’s soft tissue characteristics, and the surgeon’s familiarity with the relevant dissection planes.
Lastly, the finding of no statistically significant difference in total eyelid complication rates (RR 0.80; 95% CI: 0.26-2.41) may reflect true clinical equivalence—or it may more likely reflect insufficient power and heterogeneity in the underlying data. Statistically null results in this context do not confirm equivalence unless studied through a design explicitly powered for non-inferiority. Our findings instead underscore a lack of clear evidence favoring one approach over the other, which is not the same as demonstrating that they are identical in risk. The trends noted in this review across complication types, operative time, and intraoperative choices, however, suggest that there are likely practice distinctions between how preseptal and retroseptal approaches are being used by surgeons.
In conclusion, while this review provides a broad summary of outcomes following preseptal and retroseptal transconjunctival approaches, the field remains constrained by study design limitations, reporting variability, and possible publication bias. There is no strong evidence to suggest that 1 technique is universally superior. However, there is ample evidence to suggest that they serve different purposes in the hands of different surgeons. Future studies must move beyond retrospective case aggregation and toward rigorously designed, prospective, and ideally randomized studies that stratify outcomes by fracture type, surgical objective, and patient-level risk factors. Only with such data can the field evolve from preference-based practice to truly evidence-guided decision-making.
Conclusion
In summary, this systematic review and meta-analysis demonstrates that both preseptal and retroseptal transconjunctival approaches are associated with low rates of lower eyelid complications in orbital fracture repair. While no significant difference in total complication risk was identified, important trends in complication profile, intraoperative technique, and patient selection indicate that these approaches are not functionally equivalent. We therefore advocate for surgeons to select an approach to the orbit that is tailored to patient anatomy, fracture complexity, and surgeon expertise until higher-quality comparative data become available.
Supplemental Material
sj-docx-1-fac-10.1177_27325016251364229 – Supplemental material for Evaluating Lower Lid Complications in Preseptal Versus Retroseptal Transconjunctival Approaches for Orbital Fractures: Systematic Review and Meta-Analysis
Supplemental material, sj-docx-1-fac-10.1177_27325016251364229 for Evaluating Lower Lid Complications in Preseptal Versus Retroseptal Transconjunctival Approaches for Orbital Fractures: Systematic Review and Meta-Analysis by Justin Haas, Patrick Kim, Carolyn Wang, Mohamed El-Rabbany and Jennifer Redwood in FACE
Footnotes
Ethical Considerations
Institutional Review Board approval was not required.
Consent to Participate
Ethics approval and consent to participate were not required for this study, as it is a review of previously published literature and did not involve the collection of original patient data.
Author Contributions
1. Justin Haas (corresponding author): conceptualization, methodology, investigation, formal analysis, writing, project administration. 2. Patrick Kim: methodology, investigation. 3. Carolyn Wang: investigation, formal analysis, writing. 4. Mohamed El-Rabbany: Supervision, conceptualization, methodology, writing, project administration. 5. Jennifer Redwood (principal investigator): Supervision, conceptualization, methodology, writing, project administration.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.