
Abstract
The historical example of World War I demonstrates that immense volumes of complex reconstructive defects, which surpassed the available medical capabilities, presented a unique opportunity for the development of plastic and reconstructive surgery. We aim to demonstrate how the current conflict in Ukraine has become a catalyst for medical progress and innovation by describing the first case of microsurgical free flap reconstruction of a large palatal defect in a child in Ukraine. This procedure and perioperative care were made possible by the combined efforts between surgeons from a U.S.-based academic pediatric cleft center and adult microsurgical center in collaboration with a local pediatric hospital surgical and anesthesia teams. This report showcases the feasibility of performing such complex reconstructive procedures and presents: (1) a model for surgical education, (2) a model for global surgery, and (3) an important step in advancing cleft care in Ukraine, which could ultimately be game-changing for building a sustainable, effective healthcare system.
Keywords
Patients and Methods
After the onset of the current full-scale conflict, Ukraine found itself in a critical need for comprehensive reconstructive surgery assistance for both adult and pediatric populations. This traditionally requires efforts of microsurgical, cleft, and craniofacial disciplines. However, the cohesive collaboration has been precluded in the past by the culturally driven lack of direct communication between these specialties. Additionally, the reserve of pre-conflict specialists able to perform free tissue transfers cannot fully cover the existing volume of defects requiring reconstruction. Thus, the need for rapid training of young surgeons and enhancing existing specialists’ skills becomes urgent.
The onset of war, however, drew humanitarian effort from many surgical specialties, in particular microsurgery, to share their expertise. Ukrainian hospitals welcomed the visitors, jump-starting the rapid progress in complex procedures that require multiple teams which were hard to accomplish before. This also made it possible for our pediatric plastic surgery team to successfully perform a technically difficult reconstruction on a patient in the setting of limited resources. This collaboration could have occurred under more peaceful conditions, but the urgency of the conflict accelerated the process and the sharing of expertise.
The patient was an 11-year-old male, who presented to the surgery department at a regional Ukrainian pediatric hospital with complaints of regurgitation of food and liquid into the nasal cavity during meals and severe hypernasality. To alleviate his symptoms, the patient used a palatal obturator. Based on his medical history, the child underwent 5 surgeries, including primary palate repair and unsuccessful palatal fistula correction in different hospitals of the country. Genetic evaluation for cleft predisposition was not conducted due to limitations at the treating hospital, thus the presence of a syndrome remains uncertain. On physical examination, a large fistula encompassing the majority of the hard palate was identified (Figure 1). Given the patient’s previous surgical challenges and failures with local tissue repairs, a decision was made to proceed with a free tissue transfer.

Preoperative palatal defect (above, left), radial forearm flap, immediate postoperative result (above, right), postoperative recurrent fistulae (below, left), final result after revision (below, right).
This patient’s presentation was not the direct result of the war, but the lack of available care that was exacerbated by the conflict. While there was already a lack of microsurgeons, the shift in surgical focus to trauma care only increased the care gap. Many surgeons capable of performing such a procedure were serving on the front lines, leaving a significant void that we aimed to fill by providing expertise and training to attending surgeons and trainees in children’s hospitals.
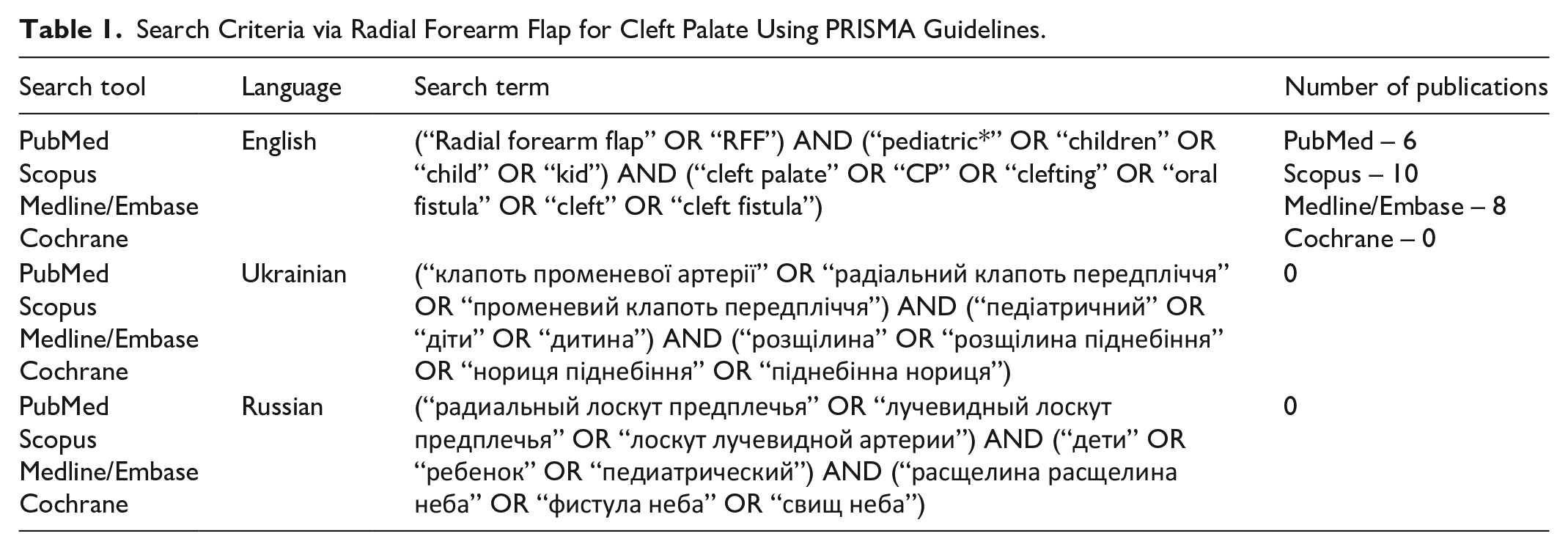
To date, free-tissue transfer has been considered a “last chance” means of repair in palatal reconstruction.1-5 The use of radial artery flaps for covering defects in both the hard and soft palate is not a new concept, as they are widely utilized in palate tumor reconstruction, trauma cases, narcotic-related, and cleft-related oronasal fistula reconstructions for both adult and pediatric population.6-8 No reports of radial forearm flap for cleft lip and palate were identified via a literature review in Ukraine (see Table 1). To the best of our knowledge, the case described in this study was the first of its kind in this country. The concept of conducting international humanitarian surgical missions in countries experiencing crisis has existed for decades, and there are numerous organizations involved in conducting reconstructive operations worldwide.9,10
Search Criteria via Radial Forearm Flap for Cleft Palate Using PRISMA Guidelines.
The Center for Global Health of a U.S. academic institution began work in the field of plastic and reconstructive surgery in Ukraine in April 2022, following the start of the full-scale invasion in Ukraine. The initial format of collaboration between the U.S. representatives and Ukrainian surgeons involved online consultations on the management of complex reconstructive cases. 11 In collaboration with a U.S. pediatric hospital the first joint surgical mission to Ukraine was organized in March 2023. Three American surgeons participated in the mission – 1 pediatric cleft lip and palate plastic surgeon and 2 microsurgeons.
From its inception, the team’s approach not only factored in the direct execution of microsurgical procedures on patients by mission participants, but also the simultaneous on-site training of Ukrainian surgeons, surgical residents, anesthesiologists, and medical teams. Thus, Ukrainian participants were involved in every stage of preoperative preparation, surgical procedures, and postoperative care. They provided regular patient follow-ups to receive further recommendations and maintained constant communication with the U.S. team – which became a key component in achieving optimal surgical outcomes.
Preoperative preparation began with standard laboratory tests and Allen’s test with Doppler assessment of vascular dominance. The patient was right hand dominant and Allen’s test revealed the dominant artery to be the radial artery on the left forearm donor site, which factored into the surgical planning. The decision was made to proceed with the left forearm, intraoperatively assess ulnar flow and perform a radial artery graft if needed. The plan also included donor site skin grafting from the same upper arm which would then be closed primarily. Preoperative markings and closure on the patient’s non-dominant forearms are shown in Figure 2. Distally, markings for the standard radial forearm are marked. Proximally, the skin graft donor site is marked which is then closed primarily.
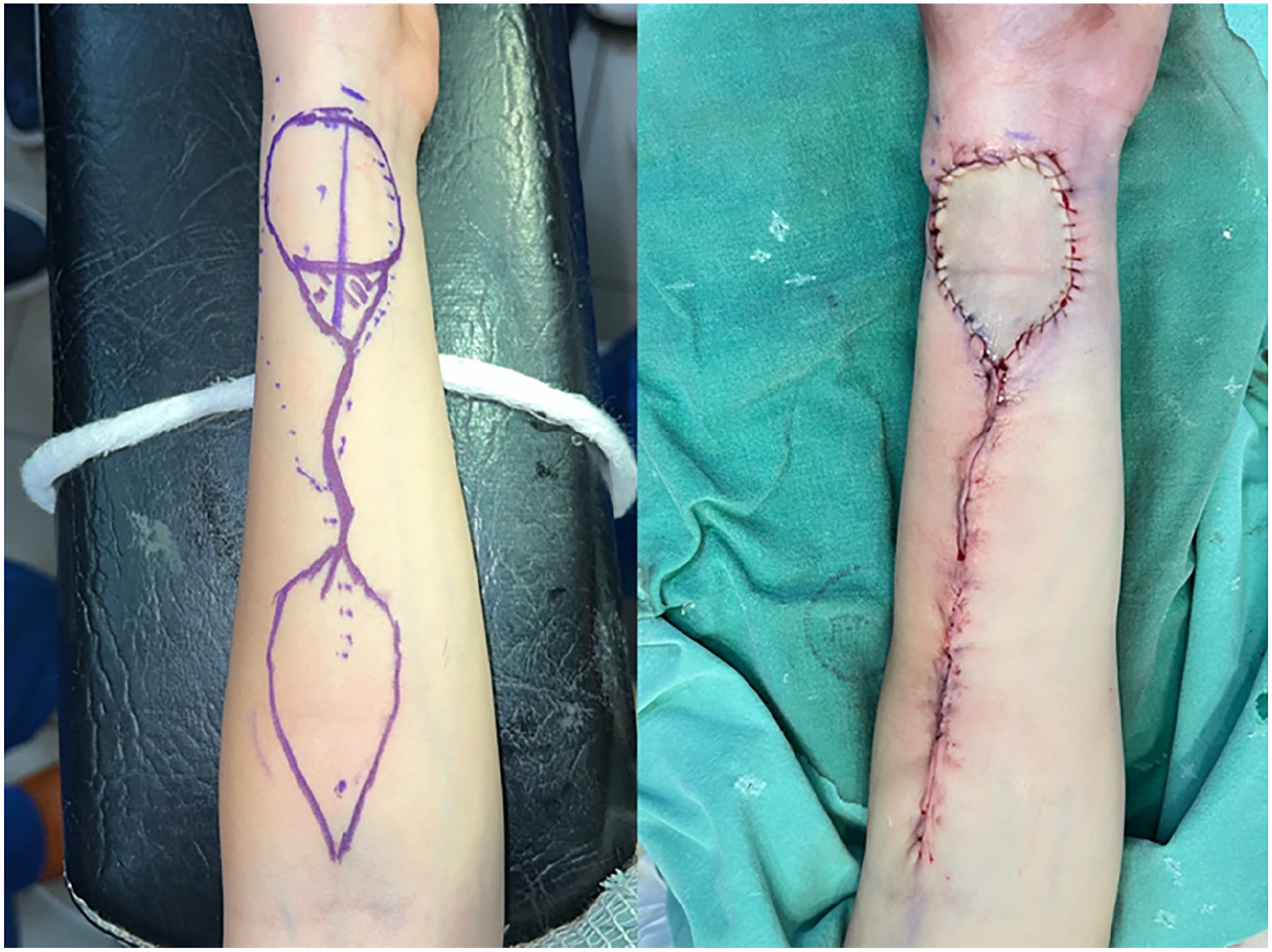
Preoperative donor-site markings on the non-dominant forearm (left). Post closure forearm (right).
Preparation also included education of anesthesia, nursing, and critical care teams to highlight the important aspects of flap care including visual and Doppler assessment of flap perfusion, blood pressure, fluid maintenance and postoperative oral care, etc. To achieve effective communication with the patient’s family, our institution developed a postoperative care guideline complemented with culturally tailored illustrations and translated into Ukrainian in a non-medical format accessible to the general population. We demonstrate an example of culturally tailored guidelines as it pertains to feeding and post op care for patients from infancy to adults (Figure 3) below. The guidelines include instructions for feeding and post operative care for infants and school aged children alike based on post operative day, such as progressing diet from liquids to soft to full in the top part of the instruction sheet. Additionally, we included recommendations about not touching the surgery site and returning to the hospital with fever, bleeding, or severe pain. We have found these instructions to be new effective tools for the families for successful postoperative care. Patients’ parents repeatedly have commented on the usefulness of the simple, illustration-heavy instructions.

Example of culturally tailored guidelines for postoperative oral care created by our team and translated into Ukrainian language. Top part lists feeding instructions for school aged children and infants based on postoperative day going from liquids to soft to normal diet. Bottom part of instructions includes information on the surgery site care and the indications for returning to hospital in case of fever, bleeding, or severe pain develops post-operatively.
The procedure was performed by a team of 4 surgeons, including 1 Ukrainian pediatric surgeon, along with a dedicated Ukrainian anesthesia team. Flap harvest and inset was conducted in standard fashion with vascular anastomosis to the facial vessels under 3.5× loupe magnification, as the hospital lacked the technical capability for a microscope.12,13 This underscores the benefit of prior surgical loupes training and challenges that can be significant in lower recourse settings. The patient was managed in the intensive care unit with Doppler flap perfusion assessments every half hour for 3 days, as well as daily pediatric dose of Aspirin for 30 days. Over 18 months of continued monitoring, the flap required 1 fistula revision operation at 6 months mark to correct 2 fistulas that became apparent at 4 to 8 weeks as the flap healed. First fistula was located at the anterior border just behind the incisors where there was no palatal shelf, only the vertical alveolar margin. This fistula was repaired with a gingival turndown flap which healed with help of protective palatal splint for 2 weeks. The second fistula was located at the posterior lateral border opposite of the pedicle. Direct 2 layer oral and nasal closure with a collagen membrane inlay between layers was used to repair this fistula (see Figure 1 for end result). The speech was normalized and all preoperative complaints were resolved as the result.
Conclusions
This study demonstrates that the Ukrainian conflict has become a catalyst for medical progress, particularly for complex reconstructive procedures. While the war did not directly cause the patient’s condition, it facilitated collaboration between Ukrainian and international teams, enabling the first successful free radial forearm flap surgery in Ukraine. Following Gillies’s steps after World War I, Ukraine has an opportunity to leverage the current medical crisis, effectively advancing the fields of cleft care and microsurgery. The war accelerated this collaboration and the transfer of knowledge that would have taken longer under normal circumstances.
The relationships established between Ukrainian and international medical institutions continue to support both on-site and remote efforts. This collaboration, while starting with 1 case, has laid the foundation for future training programs and autonomous surgical capabilities in Ukraine. In the long term, this enables the establishment of advanced multidisciplinary standards of care for pediatric and adult reconstruction, the creation of academic residency training programs, and the establishment and enhancement of centers of excellence in the future. While 1 case alone does not establish full autonomy, it marks a significant step toward sustainable microsurgical practices, as well as efforts towards creation of plastic surgery residency programs in Ukraine driven by this need and collaboration that made this case possible.
Performing the first radial forearm free flap surgery on a child in a country with no prior experience of this procedure, during a state of martial law, in a lower resource setting is a notable achievement. During the martial law that involves the lack of post-operative follow up or long term care, we have set this patient up for success post-operatively through the developed relationships with Ukrainian colleagues, improved training and resources that have been introduced as the result of this collaboration. Overall, this case demonstrates Ukraine’s ability to implement complex microsurgical techniques for cleft and related complications in the future.
Footnotes
Ethical Considerations
No IRB approval was required for a case report.
Consent to Participate
Consent to participate was obtained from participant’s legal guardians in writing.
Consent for Publication
Consent for publication of de-identified patient-related information was obtained from participant’s legal guardians in writing.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Data sharing is available upon request from the corresponding author.