
Abstract
Introduction
The International Consortium for Health Outcomes Measurement (ICHOM) has developed the ICHOM Standard Cleft Set (ICHOMSCS), a set of standardized outcome measures for Cleft Lip and/or Palate (CL/P) treatment. 1 The current set contains short-term outcome measures for secondary alveolar bone grafting (SABG), like excessive bleeding or infections, dehiscence, fistula or necrosis within 30 days after surgery and it contains long-term Patient Reported Outcome Measures (PROMs) regarding function and esthetics of the jaw. However, ICHOMSCS currently does not contain long term clinician reported SABG outcome measures. 1
Alveolar bone grafting (ABG) is commonly applied to correct the alveolar defect in patients with CL/P. This surgical procedure addresses a variety of goals; oronasal fistula closure, a continuous and stable dental arch, a bone environment that facilitates eruption and orthodontic movement of permanent teeth adjacent to the cleft, an increased bone attachment to the teeth adjacent to the cleft, and eventually it supports, in combination with orthodontic treatment, to facial symmetry, dental rehabilitation and prosthodontic reconstruction.2,3 Various bone grafts can be used to fill the alveolar defect, including autografts, allografts, xenografts, and synthetic grafts. The ABG can be performed in 3 different stages of tooth development: primary, secondary, or tertiary. Secondary ABG (SABG) is the golden standard for many cleft surgeons and is performed during dental transition and before eruption of the permanent canine, between the ages of 8 and 11 years.4-9
Clinician reported assessment methods for the long-term evaluation of SABG of patients with CL/P can be either non-radiographical, like probing and intra-oral inspection, or radiographic assessment. Occlusal, periapical and panoramic radiographs are commonly used for 2- dimensional (2D) radiographic evaluation. Computed tomography (CT) and cone-beam computed tomography (CBCT) provide a 3-dimensional (3D) radiographic assessment of SABG. Not only are the assessment methods diverse, different scoring scales are also available.
While there is a large variety of techniques used in SABG surgery by cleft teams worldwide, no long-term outcome measure is yet included in the ICHOMSCS. A uniform, straightforward, accurate, and reliable approach to assess the SABG outcome at the end of the complete cleft treatment, would be useful to promote informed decision-making in cleft care. But also has the potential to improve the quality of cleft care and to reduce costs. Therefore, this scoping review aims to provide an overview of the available methods for long-term evaluation of SABG of patients with CL/P. The secondary aim is to evaluate the reliability of the available long-term SABG assessment methods as the obtained assessment method should be suitable for use in the multiple centers worldwide that are using ICHOMSCS.
Material and Methods
This scoping review followed the guidelines of the Preferred Reporting Items for Systematic reviews and Meta-Analyses extension for Scoping Reviews (PRISMA-ScR). 10 There were no human participants in this study and informed consent was not required.
Eligibility Criteria
The studies included in this review were selected according to the participants, concept, and context (PCC) criteria. 11 The inclusion criteria were defined according to Participant (P): patients with uni- or bilateral non-syndromic cleft lip and alveolus (CLA) and/or cleft lip, alveolus and palate (CLAP); Concept (C): patients who underwent SABG surgery; Context (C): >3 months evaluation of the SABG outcome assessed with a well-defined assessment method and scoring scale, that was tested on reliability.
Included study designs were controlled clinical trials (CCTs) and both retrospective and prospective observational studies. There were no restrictions regarding the appearance and location of the cleft (uni- or bilateral, left, or right), preoperative status of orthodontic treatment and type of graft used. Only English written studies were included. Animal studies, systematic reviews, meta-analyses, cross-sectional studies, case reports, and in vitro studies were excluded.
Information Sources and Search
A literature search was conducted in the following databases: Medline ALL, EMBASE, Web of Science and Cochrane Library. The first search was conducted on August 25, 2021 and was updated on April 7, 2023. The complete search strategy was prepared with the support of the librarians Wichor Bramer and Christa Niehot of the Erasmus Medical Center, Rotterdam, The Netherlands. The search focused on synonyms and related terms for cleft, alveolar bone grafting, and treatment outcomes, the full search strategy is shown in Supplemental Table 1. The final search results were exported into EndNote, and duplicates were removed by the library technician.
Selection of Sources of Evidence
Two reviewers (L.S.K.K. and A.E.V.) independently screened the publications from the literature search based on titles and abstracts. The Rayyan web application was used to facilitate independent record selection by the scoping team. 12 Publications selected by both reviewers based on title and abstract were included for full text review. Subsequently, full-text articles were retrieved and evaluated for eligibility based on the inclusion and exclusion criteria by both reviewers. In case of discrepancy, a third reviewer was consulted (N.C.W.K.).
Data Charting and Synthesis
Data charting was performed independently by 2 reviewers (L.S.K.K. and A.E.V.). The following data were extracted from the included studies: study design, year of publication, sample size, number of patients, age, cleft type, follow-up time, type of graft used, assessment method, scoring scale, and information on reliability.
Data Analysis
Data were descriptively summarized and analyzed. Additionally, the study characteristics were discussed in the text using a narrative approach. The results about assessment methods were categorized into non-radiographic, 2D radiographic or 3D radiographic. Inter-/intra-rater reliabilities and/or intra-class coefficients (ICC) and/or dice coefficient from the different studies were summarized for each assessment method with mean and range.
Results
Selection of Studies
The study selection process was presented in the PRISMA flow diagram in Figure 1. Initially, a total of 3222 records were identified after duplicate records had been removed. After the title and abstract screening, 75 articles were selected for full text screening. Among these, 46 articles were excluded because no full-text was available (n = 4), no information on reliability of the assessment method was provided (n = 33), Primary ABG or Tertiary ABG was performed (n = 4), different study design was used (n = 2), or the follow-up period was less than 3 months (n = 3; Figure 1). Finally, 29 articles were eligible for inclusion in the study.
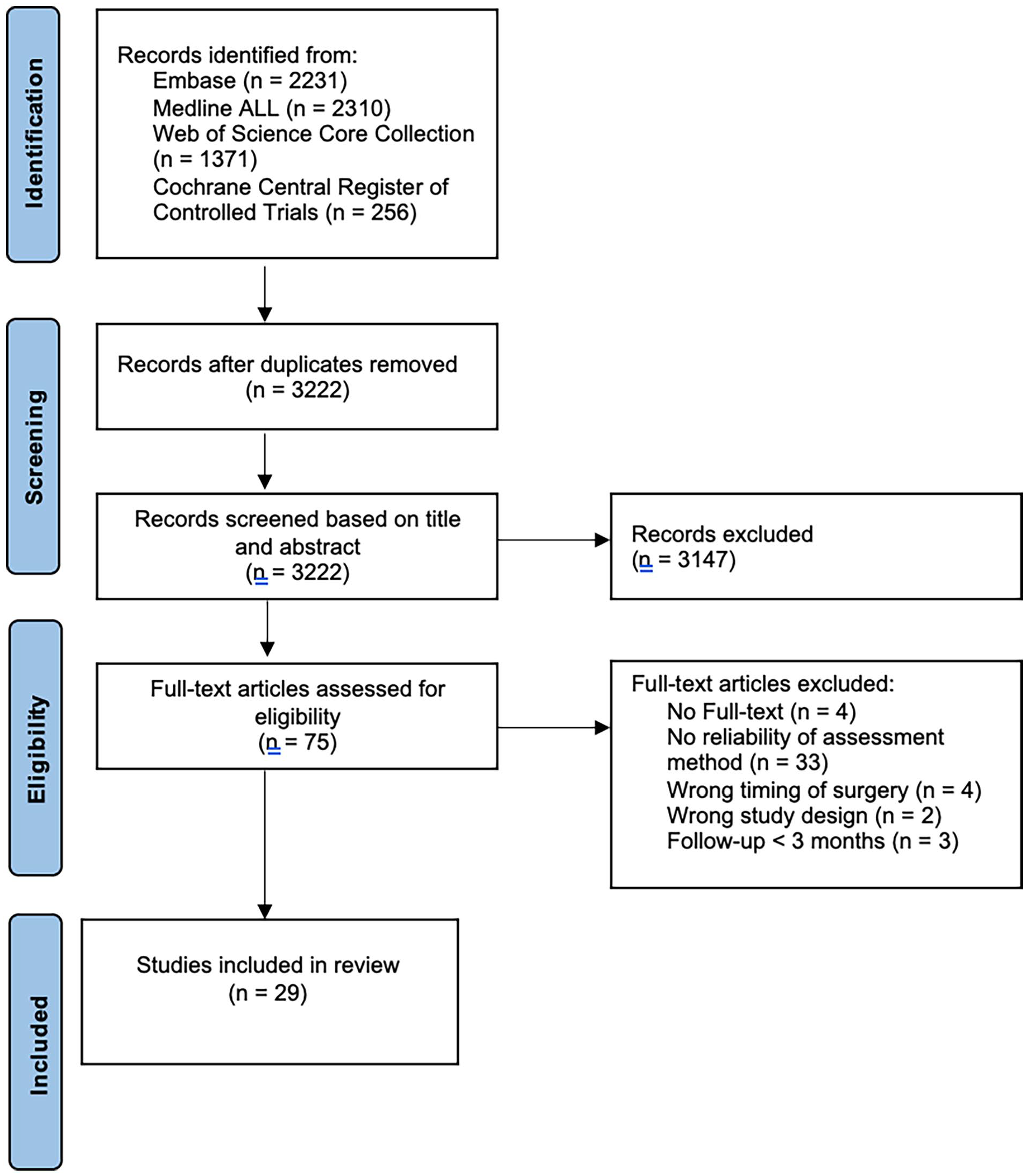
PRISMA (preferred reporting items for systematic reviews and meta-analyses) flow diagram.
Study Characteristics
A summary of the included studies is presented in Tables 1 and 2. The dates of publication ranged from 1997 to 2023. The 29 included studies had a follow-up time ranging from 3 months to 6 years postoperatively. The total number of participants per included study varied between 10 and 618 patients. The included studies identified 20 different scoring scales among various non-radiographic, 2D and 3D radiographic assessment methods.
Characteristics of Included Studies.
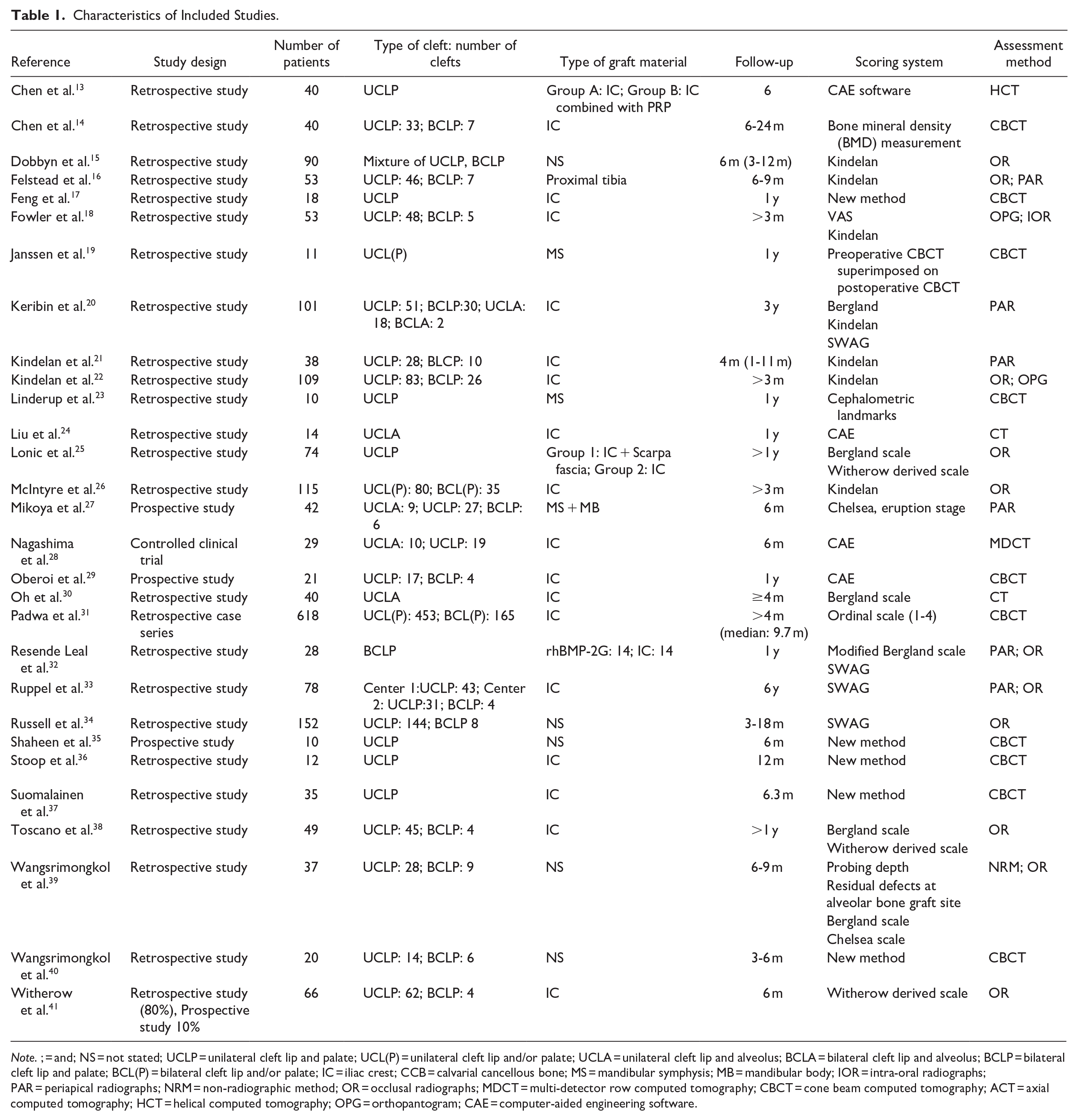
Note. ; = and; NS = not stated; UCLP = unilateral cleft lip and palate; UCL(P) = unilateral cleft lip and/or palate; UCLA = unilateral cleft lip and alveolus; BCLA = bilateral cleft lip and alveolus; BCLP = bilateral cleft lip and palate; BCL(P) = bilateral cleft lip and/or palate; IC = iliac crest; CCB = calvarial cancellous bone; MS = mandibular symphysis; MB = mandibular body; IOR = intra-oral radiographs; PAR = periapical radiographs; NRM = non-radiographic method; OR = occlusal radiographs; MDCT = multi-detector row computed tomography; CBCT = cone beam computed tomography; ACT = axial computed tomography; HCT = helical computed tomography; OPG = orthopantogram; CAE = computer-aided engineering software.
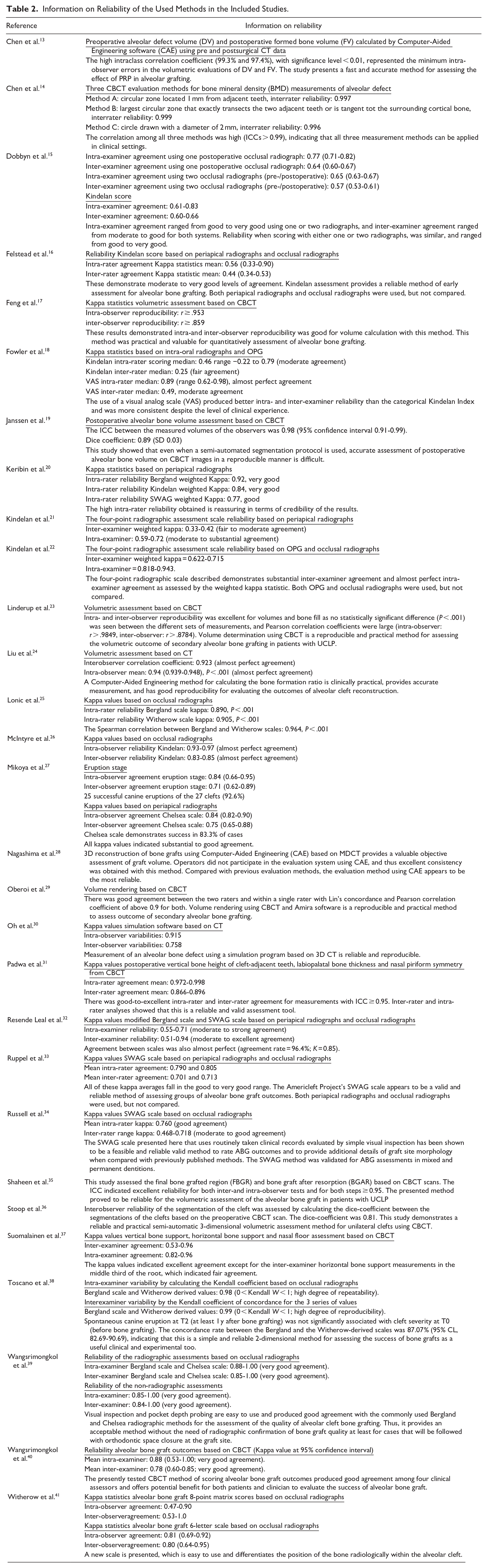
Information on Reliability of the Used Methods in the Included Studies.
Non-radiographic Assessments
In 1 included study a non-radiographic assessment method was used to evaluate SABG. 39 Wangsrimongkol et al. evaluated probing depth of the teeth adjacent to the cleft (ICC in both mesial and distal teeth ranging from 0.88 to 1.00) and a visual inspection of residual defects at the alveolar bone graft site (ICC ranging 0.89-1.00) as non-radiographic methods for assessing the SABG results 6 to 9 months post SABG. 39
Radiographic Assessments
In 15 of the included studies,
Short Description of Scoring Scales Applied to 2D Radiographs.
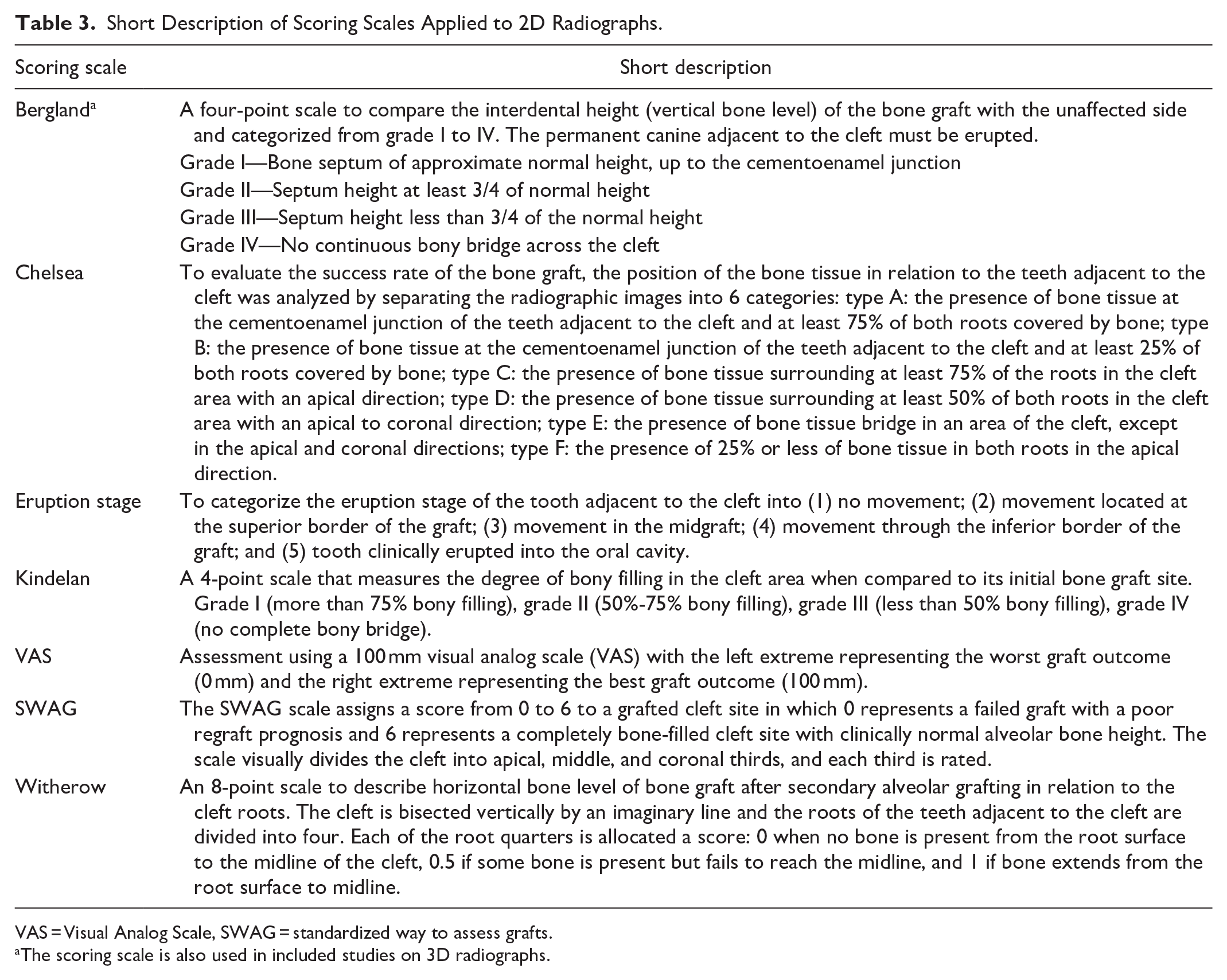
VAS = Visual Analog Scale, SWAG = standardized way to assess grafts.
The scoring scale is also used in included studies on 3D radiographs.
In 14 of the included studies,
For CBCT, 10 scoring scales were described to assess SABG outcome. Chen et al. 14 reported a high correlation of 3 methods of Bone Mineral Density (BMD) measurement by the same scorer with ICC > .99. Janssen et al. 19 used a superimposition technique revealing an ICC between observers of 0.98 and a dice coefficient of 0.89. Linderup et al. 23 examined cephalometric landmarks based on CBCT and discovered strong correlation coefficients (inter-observer: r > .88, intra-observer: r > .98). Padwa et al. 31 evaluated SABG outcomes using an ordinal scale based on CBCT with an inter- Κ = 0.87 and intra-rater reliability Κ = 0.98. Oberoi et al. 29 performed CAE on CBCT with an inter- rater reliability Κ = 0.97 and intra-rater reliability Κ = 0.98. The following authors did research on new CBCT assessment methods evaluating SABG with reliability ranging from fair to excellent: Wangsrimongkol et al. 40 (mean inter-rater reliability Κ = 0.78 (range: 0.60-0.85) and a mean intra-rater reliability Κ = 0.88 (range: 0.53-1.00)), Feng et al. 17 (intra-observer reproducibility: r > .953, inter-observer reproducibility: r > .859), Shaheen et al. 35 (inter-and intra-observer tests ≥ 0.95), Stoop et al. 36 (dice-coefficient = 0.81), and Suomalainen et al. 37 (inter-examiner agreement: 0.53-0.96, intra-examiner agreement: 0.82-0.96).
Discussion
In this scoping review 29 studies were analyzed to provide an overview of the available methods for evaluating the outcome of SABG in patients with CL/P from a clinician point of view. Additionally, information on reliability was provided. The 3D assessment method was most consistent between examiners, but it has his drawbacks. The higher costs, increased radiation exposure, the need to have either a medical CT or CBCT scanning device, and the need for specialized training and expertise to handle the device and interpret the scans make this method less accessible and potentially even harmful for the patient. As for the higher radiation levels, the European guidelines on CBCT state that the radiation dose from a single CBCT scan is equivalent to 3 to 30 times the dose from an OPG. 42 Further, the costs for a CBCT examination are approximately 4 times the costs for panoramic imaging. 43 The radiation and price ratio’s can vary depending on the specific machine used, the settings, and the area being scanned. 44 For 3D evaluations, the included studies used several scoring scales to calculate volume. Although the scoring scales differed, the majority was digitalized, which explains the high reliability compared to the non-automated non-radiographic and 2D radiographic assessments. BMD is calculated with the highest reliability, suggesting this is the most reliable technique for evaluation after SABG. 14
The least described assessment method in the included studies is the non-radiographic assessment of SABG. The downside of the non-radiographic assessment, is that it seems less accurate and more subjective. However, it is the least invasive technique, due to low costs, easy accessibility and no potential negative side-effects and reliability scores are still notable. Wangsrimongkol et al. 39 found that both probing depth as visual inspection correlated well with the Bergland method and Chelsea method on 2D radiographs. They suggest that the non-radiographic evaluation can be a viable alternative, reducing the need for radiographic confirmation.
Most frequently used in the included studies were the 2D radiographic assessment methods. For 2D radiographic assessments, the primary limitations are their inability to provide depth information and the potential for distortion and overlapping of anatomical structures, compared to 3D radiographs. Moreover, the performance of 2D radiograph to assess the SABG outcomes on the long term, also depends on the scoring scale applied to the images. The Bergland and the Kindelan scale were most frequently used, but the Bergland resulted in higher inter- and intra-rater reliability than the Kindelan. With this finding, the Bergland scale is suggested to be a valuable, accessible, and cost-effective scoring scale for evaluating SABG outcomes. However, the Bergland scale does have its shortcomings, it is only applicable when the permanent canine has fully erupted, making earlier evaluations unfeasible. Further, the Bergland scale cannot evaluate vertical bone loss or the lack of bone in the cleft’s most apical region. 45 Consequently, cases with an apical bone defect but normal interdental bone height could be incorrectly judged as successful.
Seven included studies combined different assessment methods and/or scoring scales within their resea-rch.18,20,25,27,32,38,39 These comparisons generally did not result in conflicting evaluations of SABG outcomes, nor was there consensus on 1 method being superior to another.
Limitations
A scoping review is a suitable research technique for providing an overview, however there are some limitations to consider in the current study. Within the 2D radiographic assessment group, several types of 2D radiographs were available: occlusal, peri-apical or OPG, but this was often not exactly described and never actually compared, making it impossible to provide conclusions on a preference for a specific type of 2D radiograph. Then, a follow-up period of at least 3 months was chosen in the inclusion criteria, but the actual length of follow-up was not further evaluated in the current study. Feichtinger et al. 46 observed that 1 year after SABG the volume of the bone might be enlarged due to the eruption of the lateral incisor or canine. This implies that evaluating SABG before eruption of the teeth adjacent to the cleft might be too soon for certain assessment methods and/or scoring scales and may lead to false indications for additional surgeries. Feichtinger indicated that the best time for postoperative assessment is still uncertain. 46 Finally, the included studies only provided reliability scores regarding the raters that used the assessment methods, validity of methods to assess success of SAGB has not been described yet, most likely because there is no consensus about when SAGB can be considered successful. However, inter and intra-rater reliabilities are indeed important for a set like ICHOMSCS, as a long-term assessment method after SABG needs to be applicable on many different places worldwide and a high reliability also indicates that a method might be simple to be adopted.
Future Research
Though the goals of SABG seem to be clear, no strict requirements are available that define when these goals are successfully accomplished. Moreover, the criteria for defining the success of SABG have not yet been consistently established. Future research is required to define success of SABG, for example via a DELPHI study. Only then, validation of the several long-term assessment methods is possible. Future research should also be done on evaluating and comparing the different assessment methods and scoring scales on costs effectiveness, patient burden, accuracy and accessibility worldwide, which will require high quality longitudinal research. Finally, future research should be done on ideal timing of SABG evaluation.
Interpretations
The current scoping review showed that the 3D radiographic automated assessment method for the evaluation of SABG of patients with CL/P is most reliable. However, in our opinion, 3D radiographs should only be considered in difficult cases as costs are higher, radiation load is higher and accessibility is lower. Further, we think that 2D radiographs are indispensable during the treatment process. However, the non-radiographic assessment method, with a visual inspection and probing depth of the teeth adjacent to the cleft, appears to address the primary objectives of SABG with the smallest burden, highest accessibility, has still notable reliability and might be verysuitable for long-term evaluation purposes in ICHOMSCS. We could imagine a yes/no checklist that is filled out by a clinician in the final phase of ICHOMSCS, at the end of the complete cleft treatment around age 20. The checklist should at least consider canine eruption, periodontal health and fistula within the dental arch.
Conclusions
The ABG addresses a variety of goals; oronasal fistula closure, a continuous and stable dental arch, a bone environment that facilitates eruption and orthodontic movement of permanent teeth adjacent to the cleft, an increased bone attachment to the teeth adjacent to the cleft, and eventually it supports, in combination with orthodontic treatment, to facial symmetry, dental rehabilitation and prosthodontic reconstruction.2,3 Within this list of diverse goals, it remains difficult to strictly define success of SABG. However, to assess the long-term outcome of SABG in ICHOMSCS these goals should be taken into consideration. There is a wide variety of available assessment methods and scoring scales provided in the current scoping review, none of them obtained low scores on reliability. But unfortunately, none of the provided assessment methods seems to be able to evaluate all goals in 1 method. Future research is necessary to determine a suitable assessment method and timing for long-term clinician reported evaluation of SABG in ICHOMSCS.
Supplemental Material
sj-docx-1-fac-10.1177_27325016251338530 – Supplemental material for A Scoping Review on Long-Term Assessment Methods After Secondary Alveolar Bone Grafting of Patients with Cleft, Lip and/or Palate
Supplemental material, sj-docx-1-fac-10.1177_27325016251338530 for A Scoping Review on Long-Term Assessment Methods After Secondary Alveolar Bone Grafting of Patients with Cleft, Lip and/or Palate by Laura S. van der Knaap-Kind, Nicoline C.W. van der Kaaij, Anne E. Verkolf, Eppo B. Wolvius and Lea Kragt in FACE
Footnotes
Acknowledgements
We thank Wichor Bramer and Christa Niehot, information specialists from the Erasmus MC Medical Library, for developing and updating the search strategies.
Data Availability Statement
All data is accessible upon request.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
Institutional Review Board approval was not required.
Informed Consent
Informed consent was not required.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.