
Abstract
Background:
Spring-assisted cranioplasty and successful long-term outcomes for sagittal synostosis has been well described in recent literature. However, there is a paucity of data regarding the application of springs to unicoronal synostosis. Unicoronal synostosis (UCS) presents unique challenges in its causation of skull base scoliosis and orbital asymmetry. Many surgeons feel that the fronto-orbital advancement and vault remodeling is the most effective and reliable strategy to counteract these changes. Here we present our experience and outcomes with spring cranioplasty for unicoronal synostosis.
Materials and methods:
A retrospective review of non-syndromic unicoronal synostosis patients undergoing spring-assisted cranioplasty was performed. Preoperative and postoperative intracranial volume (ICV), orbital volume (OV), orbital height (OH), orbital width (OW), midface twist (MFT), and skull-base twist (SBT) were measured from DICOM CT data. Analysis was performed with Materialize software (Leuven, Belgium). Paired t-tests were performed using Excel.
Results:
Ten patients (5 females, 5 males) had springs placed at 100.1 days (avg). Average ICV: preop: 608.2 ± 101.4 cc, postop: 995.2 ± 166.1 cc. Differences in orbital volume and height in the preop affected orbit versus non-affected orbit was significant (P = .01, P ≤ .001 respectively) whereas no significant difference between the two sides postoperatively was observed (P = .19, P = .58 respectively). Average preop MFT was 81.1 ± 2° and postop was 87.6 ± 2.6° and preop SBT was 171.9 ± 2.7° and postop was 177.6 ± 2.6°; both showing significant improvement after spring cranioplasty (both P ≤ .001).
Conclusion:
Our experience and early outcomes with spring cranioplasty for UCS demonstrates that when used in younger patients (<5 months) cranial springs can be a safe and effective strategy to minimize skull base scoliosis, facial scoliosis, and orbital asymmetry, as well as increase intracranial volume. Although long-term data needs to be assessed, we are optimistic that early correction of cranial base scoliosis will translate to stable results as patients reach dentoskeletal maturity.
Introduction
Craniosynostosis occurs in 1 in 1700 to 2500 births and presents as the premature fusion of 1 or more cranial sutures. This results in a restriction of growth perpendicular to the affected suture and a compensatory growth expansion by the non-affected sutures.1,2 When a single suture is affected there is typically a predictable head shape morphology and the diagnosis of synostosis can be verified using CT imaging. Coronal craniosynostosis accounts for approximately 15% to 25% of all craniosynostosis cases and can be seen unilaterally or bilaterally. 3 Unilateral coronal synostosis (UCS) is characterized by skull base and midface twist with a range of severity. This presents clinically as ipsilateral forehead and frontoparietal flattening with varying degrees of contralateral bossing, as well as ipsilateral nasal root deviation, temporal fossa bossing, superior brow displacement (Harlequin eye deformity), vertical orbital dystopia, and anterior displacement of the ear and temporomandibular joint; chin point and nasal tip deviation are toward the unaffected side.1,2,4
The goals of treatment for craniosynostosis should aim for long-term correction of craniofacial dysmorphologies and allow for adequate brain growth and development.2,5,6 Surgical treatment has evolved from the early report by Lane 7 in 1892 to “unlock the brain” with suturectomy to the more invasive cranial vault remodeling.2,8 The most common surgery to address UCS is a bilateral frontal orbital advancement and cranial vault remodeling (FOAR) at around 5 to 10 months of age. 6 Timing of surgery must balance the operative risk of blood loss in a young patient where even a small volume is significant compared to their total blood volume against the observed benefits of early intervention on brain development and improved craniofacial morphology.1,4,9-13
Studies reviewing long-term results of FOAR for treatment of UCS have reported this technique successfully mitigates the risk of increased intracranial pressure, however the esthetic outcomes can be suboptimal.8,14,15 Taylor et al reported long-term follow up over 5 years in UCS patients yielded a 5 times increased likelihood of being classified as Whitaker III or IV; noting the presence of supraorbital retrusion and temporal hollowing. With FOAR there is reported immediate postoperative improvement (<1 year postop) in craniofacial appearance, however it is believed that because the cranial base asymmetry is not addressed during surgery there is a relapse toward the preoperative state in the long-term. 16 This observation has led many authors to advocate for overcorrection to improve long-term FOAR outcomes, which poses a challenge to achieve when trying to overcome the soft tissue envelope.5,15
An alternative to FOAR is endoscopic assisted craniectomy with postoperative cranial orthosis (ESC). Surgery is typically performed under 4 months of age, which takes advantage of the pliability of the infant skull and the rapidly growing brain. 17 Jimenez and Barone 4 reported their 16 year experience with this technique and found compared to FOAR, ESC was safe and resulted in shorter operative times, less blood loss, and a shorter hospital stay. Previous results of suturectomy alone for UCS had yielded poor esthetic outcomes leading to modifications of the techinique with postoperative cranial orthosis4,18,19 or endoscopic assisted frontal-orbital advancement. 20 With these modifications, endoscopic suturectomy has shown improved esthetic and ophthalmologic outcomes compared to FOAR.
Recently, distraction osteogenesis (DO) for correction of UCS has been more widely described.21-23 DO involves a 4 stage process to promote new bone growth and soft tissue expansion: (1) initial osteotomy and distractor placement; (2) latency period; (3) active distraction phase; and (4) consolidation phase. 24 Craniofacial applications of DO was first described clinically in 1992 by McCarthy et al 25 to address mandibular hypoplasia and it’s application has evolved to uses throughout the entire craniofacial skeleton. DO is appealing compared to FOAR due it’s ability to form new bone, slowly expand the soft tissue envelope, and preserve blood supply of the bone. UCS patients treated with DO had improved Whitaker outcomes compared with FOAR patients, improved orbital symmetry, and improved skull base scoliosis correction.21,22,26
Spring cranioplasty has become a widely accepted treatment for sagittal synostosis however it’s reported use to treat UCS is lacking. There is only a recent case report of 2 UCS patients treated with spring cranioplasty. Interestingly, there was a significant improvement of facial scoliosis and cranial base deviation, which was maintained over 3 years postop. 27 For the past 5 years, we have employed spring cranioplasty in UCS patients around 3 to 4 months old. Although we are in the process of collecting long-term data (5+ years postop), our early outcomes suggest spring cranioplasty for UCS can be an effective and safe strategy to improve cranial base scoliosis, facial scoliosis, and orbital asymmetry, as well as increase intracranial volume.
Methods
Patients
A retrospective study was conducted on our patients with non-syndromic unicoronal craniosynostosis who underwent spring cranioplasty from July 2019 to January 2023. The study was approved by the Institutional Review Board at our institution under IRB # STUDY00002700.
Clinical Data and Statistical Analysis
Patient demographics and clinical data were collected from the medical record (Table 1). In addition to data shown in Table 1, estimated blood loss (EBL), packed red blood cells (pRBC) given, length of surgery, hospital length of stay, and complications for both the spring placement and separate spring removal surgeries were recorded. CT DICOMs were obtained and preoperative and postoperative (time near spring removal) intracranial volume (ICV), orbital volume (OV), orbital height (OH), orbital width (OW), midface twist (MFT), and skull-base twist (SBT) were measured using Materialize software (Leuven, Belgium) and the open source software ImageJ (https://imagej.net/ij). Following the techniques outlined in the paper by Liu et al OH was measured from the supraorbital notch to the zygomaticomaxillary suture on the inferior orbital rim. OW was measured from the frontozygomatic suture to the dacryon. The MFT angle was calculated at the intersection on the affected side of a line along the infraorbital rim at the bilateral zygomaticomaxillary sutures and a line from nasion to prosthion. The SBT angle was obtained on the affected side between a line from the nasion to sella and a line from the sella and opisthion 5 (Supplemental Material 1).
Patient Demographics and Clinical Data.
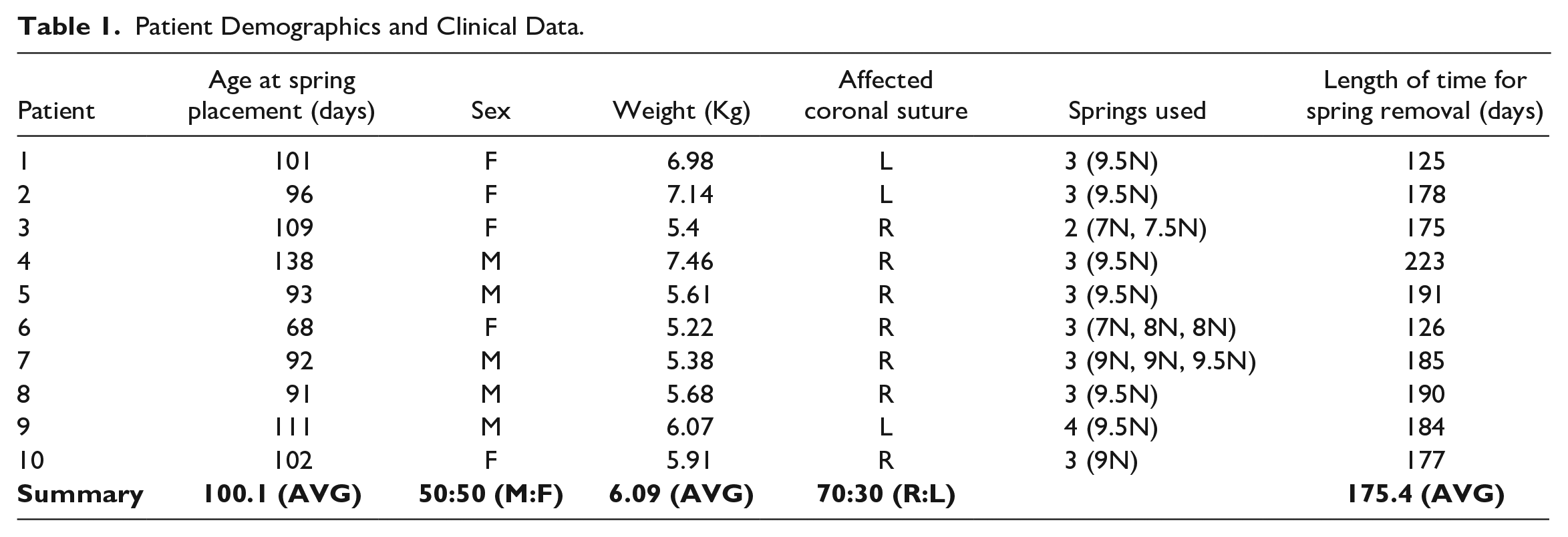
Statistical analysis was executed through Microsoft Excel version 16X. Calculations for averages, standard deviation, and paired t-tests were performed.
Surgical Technique
Spring placement
A hemicoronal zig-zag incision was made and dissection carried out in the subgaleal plane. The pericranium was dissected off the affected suture. The dura was carefully dissected free from the margin of the fontanelle. To expose the junction of the coronal and squamosal sutures, the temporalis muscle was dissected from the anterior temporal fossa and lateral orbit. A bur hole was made with a matchstick at this junction so that the dura could be dissected free along the entire length of the intended suturectomy. Then the suturectomy was performed with a side-cutting bur with a footplate from the anterior fontanelle to the squamosal suture; width of suturectomy was approximately 5 to 10 mm. Under direct visualization, a lateral orbitotomy was performed using a matchstick to osteomize the sphenoid wing and lateral orbit, which directly connected to the suturectomy (Supplemental Material 2A). The dura was assessed for injury and hemostasis. Cranial springs (Osteomed, Addison, TX) were placed. The number and strength of the springs were determined by assessing bone thickness and amount of initial suturectomy distraction upon placement with the intent of using as many and the most forceful springs that the bone could tolerate without cheese wiring. Small notches using a Kerrison Rongeur were placed along the suturectomy to help prevent migration of the spring footplates (Figure 1). The vectors of distraction were determined intraop and depended on the patient’s degree and vectors of deformity; the goal was a downward and anterior movement of the supraorbital rim and forehead (Supplemental Material 2B-C). The surgical site was irrigated out copiously with saline and a single drain placed. The temporalis was resuspended and pericranium repaired. The scalp was closed with 4-0 Vicryl and 4-0 Chromic.
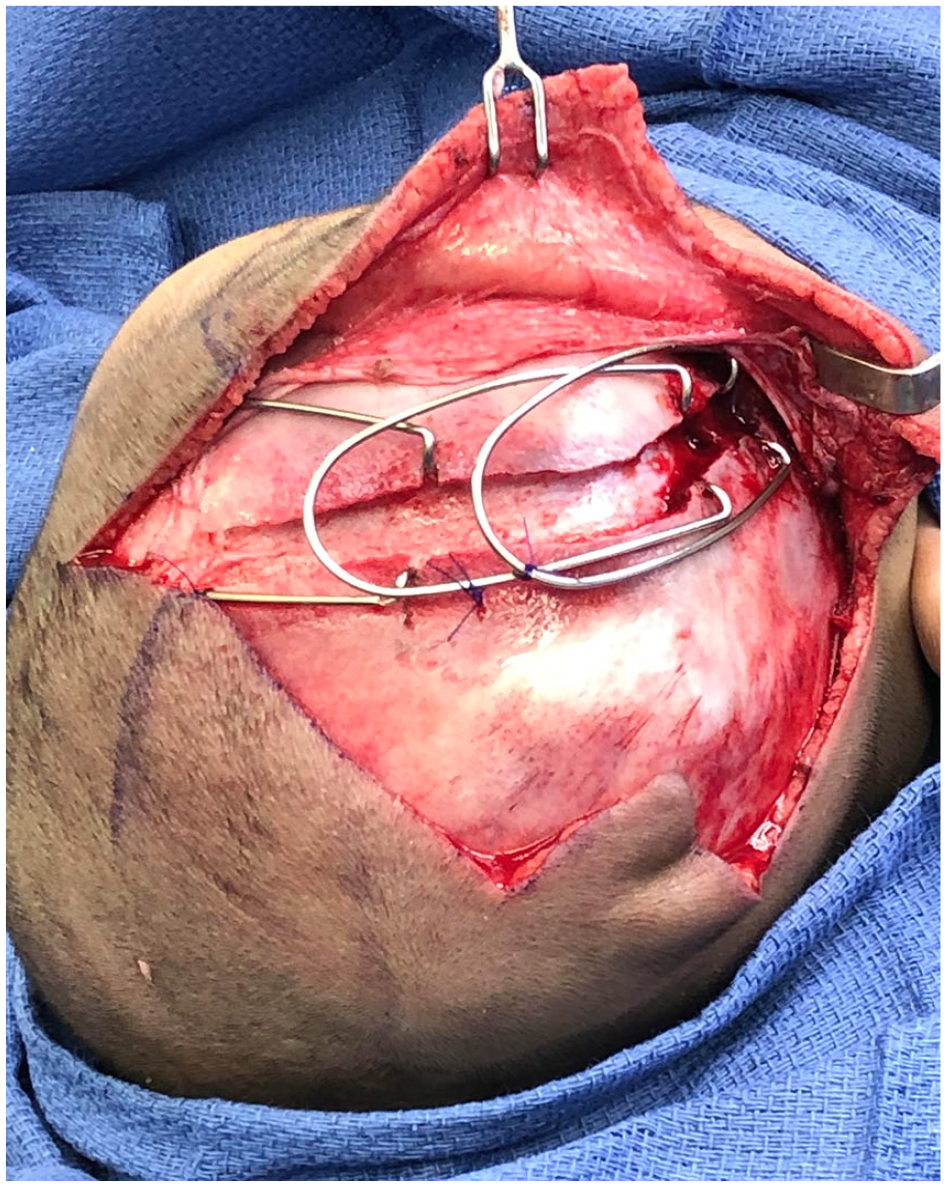
Right coronal suturectomy and intraoperative spring placement. Note the notching along the suturectomy to prevent spring footplate migration.
Spring removal
Cranial spring removal was performed using the previous incision. The springs were exposed and split at the midpoint to faciliate easier removal. The footplates were carefully freed from the bone and rotated out of place. Bleeding and dural injury were assessed. The surgical site was irrigated with saline and the scalp closed with 4-0 Vicryl and 4-0 Chromic over a drain.
Postoperative Care
Spring placement
Patients were admitted postoperatively to the ICU overnight. Drain output was recorded and drains removed when <30 cc/24 hours. Patients were discharged home and seen for evaluation weekly in clinic in the early postop period and then monthly. Spring footplate excursion was measured as well as bone formation. When spring footplates were at maximal excursion (>50 mm) and there was adequate bone bridging, the patient was scheduled for cranial spring removal. A low radiation dose craniofacial CT was obtained after spring placement on postoperative day 2 and before spring removal surgery.
Spring removal
Patients were admitted postoperatively to the surgical floor. Drain output was recorded and drains removed when <30 cc/24 hours. Patients were discharged home after drain removal. Patients were seen 1 week post-spring removal, 4 to 6 weeks postop, and then annually. Our protocol is to obtain a low radiation dose craniofacial CT when the patients are 5 years old.
Results
Patient Demographics and Clinical Data
As described in Table 1, our case series included 10 patients with a 50:50 ratio of male to female and 7 of the 10 affected coronal sutures were on the right side. Average age at time of spring cranioplasty was 100 days (range 68-138). For spring placement and removal, EBL was on average 21.7 ± 7.6 cc and 17.8 ± 7.1 cc, respectively; PRBC given was on average 14 ± 29.5 cc and none, respectively; length of surgery was an average of 83.1 ± 20.1 minutes and 75.4 ± 22 minutes, respectively; and hospital length of stay (LOS) averaged 2.9 ± 1 days and 1.2 ± 0.8 days, respectively. Typically, 3 springs were placed and 9.5N was the most common strength used. Average length of time between spring placement and removal was 175 days (range 125-223).
There were no sagittal sinus injuries, durotomies, CSF leaks, infections, or bleeding complications. None of the patients had spring exposure or malposition. One patient presented with a hypertrophic scar at the temporal portion of the incision, which was revised during spring removal and did not recur. Two patients were noted to have small (1.5 cm) temporal bone defects at the 2 year postop visit. One patient needed a FOAR for residual deformity, which was performed at the time the cranial springs were planned to be removed (Supplemental Material 3A-N).
Clinical Results and Analysis
Intracranial volume and craniofacial morphology analysis
Average preop and postop ICVs were 608.19 ± 101.4 cc and 995.22 ± 166.13 cc, respectively, with an average 64.3 ± 14.4% volume increase. When stratified by sex, preop and postop ICVs for males was 648.33 ± 128.26 cc and 1058.7 ± 216.1 cc respectively, and for females 568.05 ± 51.52 cc and 931.74 ± 72.97 cc respectively. Average percent ICV increase for males and females was 63.61 ± 13.95% and 64.99 ± 17.96% respectively.
On clinical exam (Figures 2A -F and 3A -F) there was qualitative improvement of orbital morphology, nasal positioning, and forehead and brow position when comparing preop with postop photos. Midface twist preop and postop was on average 81.07 ± 1.97° and 87.58 ± 2.57° respectively with significant improvement (P ≤ .001).
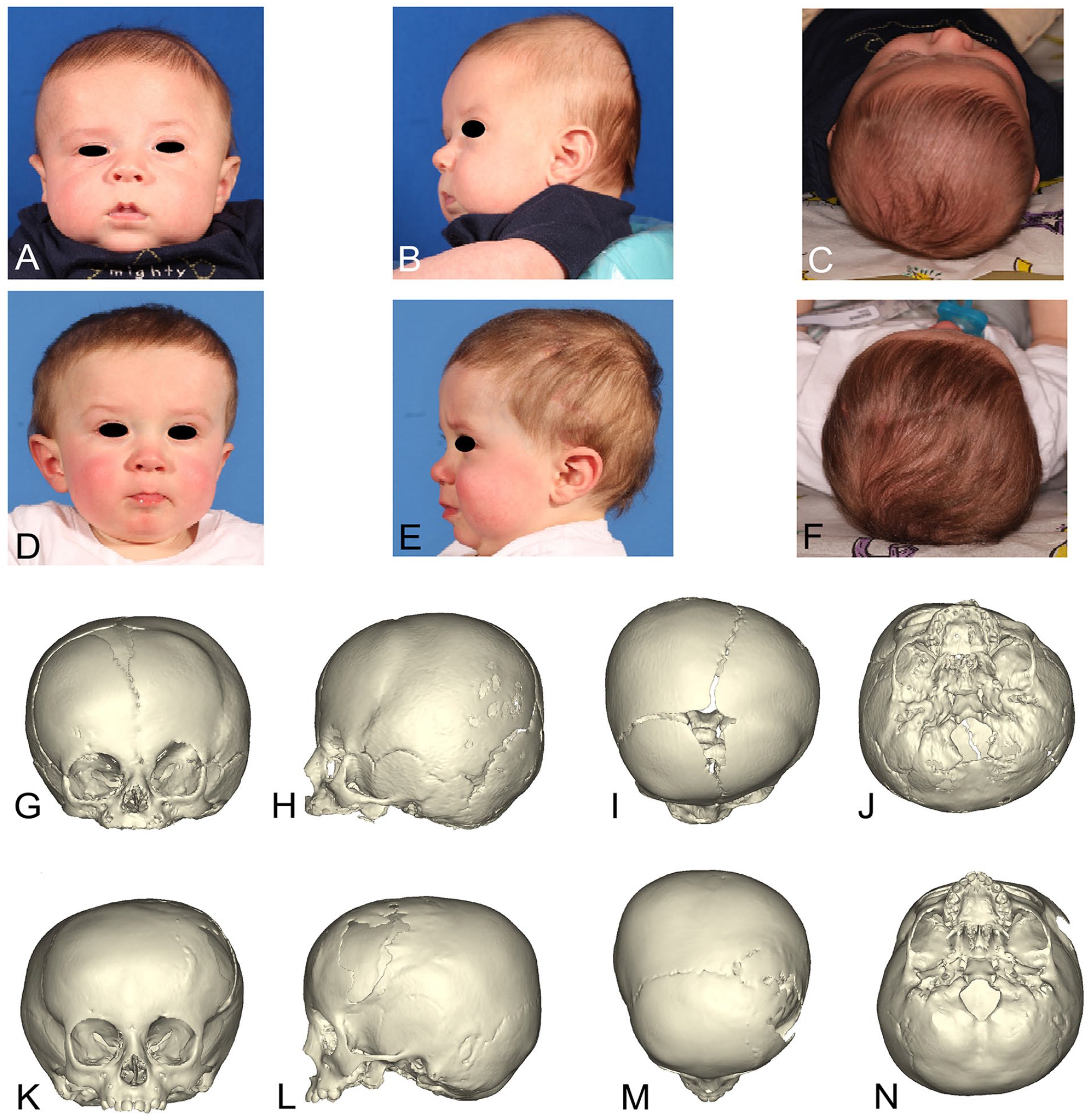
Patient 10 clinical photos preop ((A) Front; (B) Left lateral; (C) Top) at 100 days old and 13 months and 12 days old ((D) Front; (E) Left lateral; (F) Top). CT scan preop at 100 days old ((G) Front; (H) Left lateral; (I) Top; (J) Base) and postop at 22 months and 12 days old ((K) Front; (L) Left lateral; (M) Top; (N) Base).

Patient 11 clinical photos preop ((A) Front; (B) Right Lateral; (C) Top) at 86 days old and 296 days old ((D) Front; (E) Right lateral; (F) Top). CT scan preop at 57 days old ((G) Front; (H) Right lateral; (I) Top; (J) Base) and postop at 210 days old ((K) Front; (L) Right lateral; (M) Top; (N) Base).
3D reconstructions of preop and postop CT scans (Figures 2G -N and 3G -N) correlate with clinical photos demonstrating improvement of the Harlequin eye deformity, nasal root deviation correction, and improved positioning of the forehead and superior orbital rim. Additionally, preop and postop cranial base twist can be demonstrated with significant improvement (P ≤ .001); average 171.9 ± 2.75° and 177.55 ± 2.63° respectively.
Orbital analysis
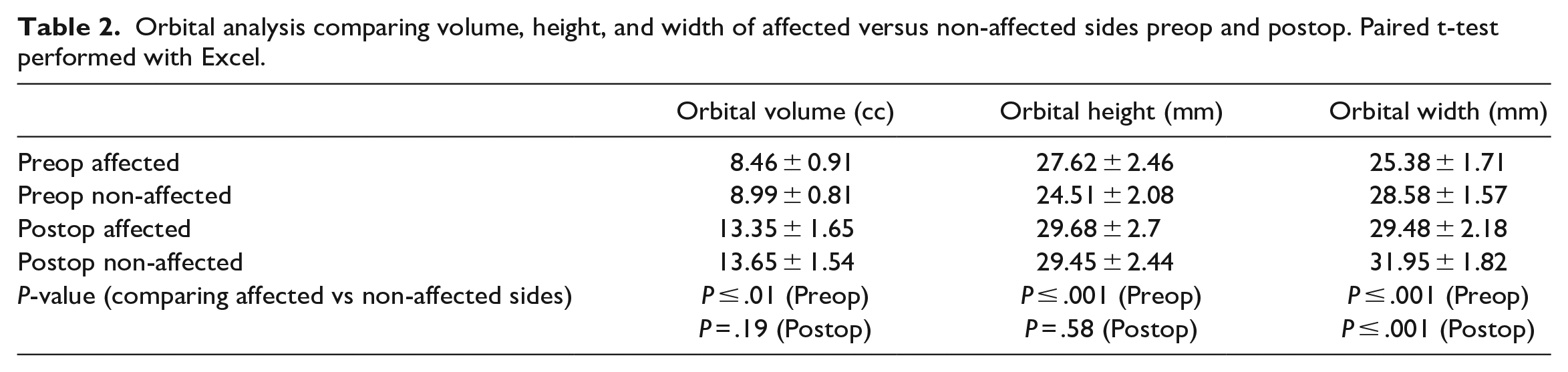
Table 2 provides a summary of the orbital analysis comparing the affected and non-affected orbits before and after spring cranioplasty. The preop affected and non-affected orbital volume, height, and width were on average 8.46 ± 0.91 cc and 8.99 ± 0.81 cc, 27.62 ± 2.46, 24.51 ± 2.08, 25.38 ± 1.71, and 28.58 ± 1.57 mm respectively. There were significant differences seen between the preop affected and non-affected orbital volumes, height, and width (P ≤ .01, P ≤ .001, and P ≤ .001, respectively) which highlight the preop orbital asymmetries. The postop affected orbit and non-affected orbital volume, height, and width were on average 13.35 ± 1.65 cc and 13.65 ± 1.54 cc, 29.68 ± 2.7, 29.45 ± 2.44, 29.48 ± 2.18, and 31.95 ± 1.82 mm respectively. Postoperatively there was no significant difference between the affected and non-affected orbits for volume and height (P = .19 and .58 respectively), suggesting an improvement in orbital symmetry. However, the postop orbital width of the affected and non-affected side remained significantly different (P < .001). Figure 4 provides an example from 1 patient of the overall morphologic changes seen in the orbits after spring cranioplasty; there is improved symmetry with reduction of orbital height and distribution of the orbital volume from superiorlateral to posterior and medially.
Orbital analysis comparing volume, height, and width of affected versus non-affected sides preop and postop. Paired t-test performed with Excel.
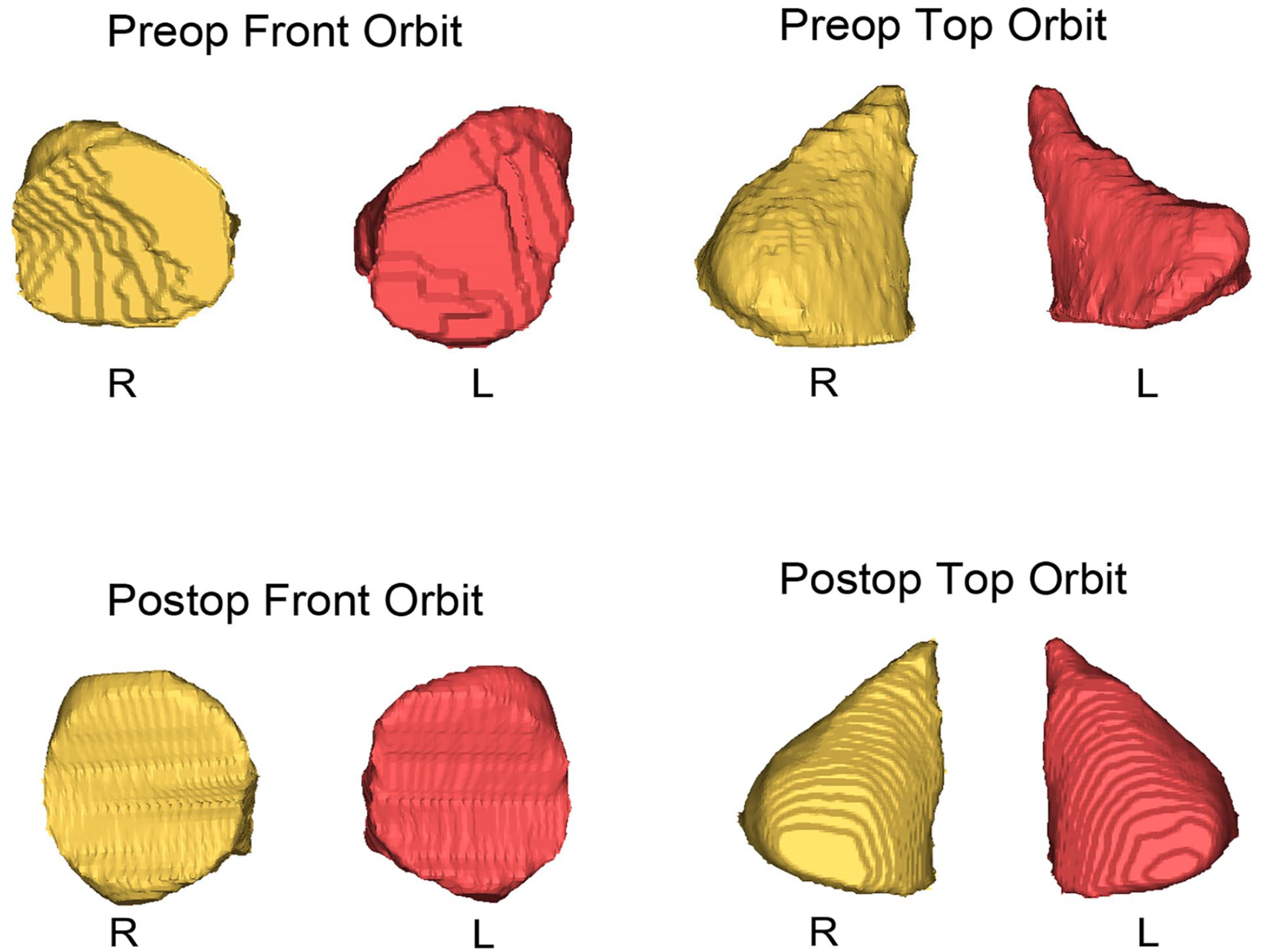
Orbital shape changes for patient 10 preop at 100 days old and postop at 22 months and 12 days old (Right orbit in yellow unaffected and left orbit in red is the affected side).
Discussion
The primary goals of surgery for craniosynostosis should strive for an improvement in form and function for the patient. Whereas surgery to optimize brain growth and development is paramount, the correction of the craniofacial dysmorphology is also important due to it’s psychosocial implications. 6 UCS is particularly challenging to correct due to orbital asymmetries, and skull base scoliosis imparting facial asymmetry. 22 UCS has higher rates of postoperative deformity which may require additional procedures despite overcorrection.1,5,15 Currently, surgical correction through FOAR is the most common choice of treatment. However, successful results have been reported with endoscopic surgery and postop cranial orthotics,4,17 and distraction osteogenesis.21-23
Although treatment of craniosynostosis with spring cranioplasty and successful long-term results have been reported by many centers, there is a paucity of information on their use for UCS. The majority of reports focus on spring cranioplasty for sagittal synostosis and it has become widely accepted as a treatment option with comparable long-term results to traditional cranial vault reconstruction. Lauritzen et al 28 reported in 2008 the safety and efficacy of springs in 100 craniofacial cases. In 2020, Runyan et al published their long-term outcomes for sagittal synostosis treated with spring cranioplasty compared with cranial vault remodeling (CVR). They reported significantly less surgical time, blood loss, and hospital stay even when combining spring placement and removal data compared to CVR. Additionally, the spring surgery cohort had better Whitaker scores and improved Cephalic Index. 29 Only recently has there been a published report on 2 UCS patients treated with spring cranioplasty; both exhibited good correction of facial and skull base scoliosis even over 3 years postop. 27
Here we present our experience with spring cranioplasty for UCS. Admittedly we had 2 transfusions that were related to our institution’s anesthesia protocols pertaining to CVR procedures and a reluctance to change protocols until the newer spring cranioplasty procedures consistently yielded a lower EBL. Hospital LOS was also longer than would be expected. We anticipate a reduction as the institution gains greater experience with this procedure. We had no dural injuries, infection, spring exposure, or bleeding complications. Compared to previous reports28,29 we had no spring malposition, which may be related to our technique to create notching in the osteotomies for the spring footplates (Figure 1). Two patients were found on clinical exam to have 1.5 cm bone gaps during their 2 year follow up. However, one of these patients had no detectable bone defect on the 4 year postop visit and the second patient was only 2 years old at the time of analysis.
One of the earlier patients in our series required a secondary FOAR (Supplemental Material 3A-N). The primary surgery only employed 2 springs whereas all other cases employed 3 or 4 springs. The secondary FOAR was noted to be much easier as the surgeon had less deformity to correct in the orbit and forehead; requiring more of a simple advancement as opposed to a reshaping and advancement. Although antecdotal, this may suggest that our protocol of using multiple and stronger springs for UCS could lead to improved outcomes. Of note is the fact that spring removal often occurs at 8 to 10 months of age, which is a common timing for FOAR. This has an advantage of giving the surgeon a well timed back up procedure in case there is insufficient correction using springs.
Intracranial volume increased an average of 64% postoperatively. However, it is difficult to tell how much is from the spring cranioplasty versus regular growth. We do not have a set of age- and sex-matched controls to reference for ICV changes and we are unaware of an available reference. Our ICV average (995 cm3) compared to the normal 9 month old value quoted in Jimenez and Barone 4 (925 cm3), suggests spring cranioplasty might be a successful method for ICV expansion for UCS. This is supported by previous reports of spring cranioplasty being an effective method to expand the intracranial space. 30
Most striking during our analysis was the consistent improvement in MFT and SBT. On clinical exam there was qualitative improvement of nasal positioning, and forehead and brow position (Figures 2A -F and 3A -F). MFT and SBT was significantly improved postoperatively. This correlates with the recent UCS spring cranioplasty case report and UCS distraction osteogenesis findings. This suggests that dynamic methodologies might modify the cranial base angulation to a greater degree than FOAR; although the exact mechanism is not defined, it is hypothesized that there is a translation of force from the site of distraction to the cranial base. FOAR does not directly address the cranial base angulation and thus may have more of a passive effect on the cranial base resulting in less degree of correction.21,22,27
Another striking finding in our patients was the improvement in orbital symmetry. In UCS there is bilateral orbital dysmorphology despite only 1 coronal suture being fused. 31 This contributes to the challenge of achieving superior esthetic and ophthalmic functional outcomes treating UCS. It has been well reported that UCS patients have significant ophthalmic manifestations such as strabismus, astigmatism, and amblyopia.10,32-35 Our patient population is still too young to report long-term ophthalmic results. However, the initial orbital analysis appears promising. Preoperative orbital volume, height, and width was significantly different between affected and non-affected orbits which correlates with previous reports.26,36,37 Preoperative orbital volume was significantly smaller on the affected side, additionally, orbital height was taller and orbital width was narrower compared to the non-affected orbit. Postoperatively, there was a qualitative change in orbital shape bilaterally toward a more symmetric appearance (Figure 4) and no significant difference between the affected and non-affected orbit for volume and height; suggesting a trend toward orbital symmetry. Orbital width on the affected side postoperatively remained significantly narrower than the non-affected side which correlates with reported findings for DO 26 and FOAR. 5
In our more than 2 decades experience of treating UCS, parents have consistently valued 3 outcomes adjacent to the normalization of cranial morphology: (1) Prevention of pressure on the brain to allow the brain to be the best brain that it can be; (2) Make their child look normal; and (3) Heal the skull such that it is completely protective allowing the child to fully engage in activities without elevated risks of brain injury. In our experience, current techniques are excellent at achieving 2 of the 3 goals but less consistent in delivering on all 3 goals. The disappointing long-term results with FOAR led us to seek an alternative treatment. Spring cranioplasty is appealing because surgery can be performed earlier (<6 months old), which takes advantage of the phase of rapid brain growth, gets ahead of the coronal ring fusion cascade, and may lead to improved neuropsychological outcomes.9,11,12,23 Additionally there is decreased surgical time, blood loss, and blood transfusions. Endoscopic surgery with cranial orthosis offers similiar benefits, however we preferred springs because cranial orthosis requires frequent visits, compliant parents, and competent technicians to fabricate the helmets, as well as can be associated with significant postoperative costs and a long duration of treatment.4,19,20 Although distraction osteogenesis offers promising long-term results and a predictable distraction distance, this method was less appealing due to pin-site infection risk, scarring/alopecia, and limitations on the number of vectors of distraction.22,23,38
Common criticisms of spring cranioplasty are the need for 2 surgeries (placement and removal), and the unpredictability of the springs.6,27,28 We have compared our operative time for UCS patients undergoing FOAR versus the combined operative times for spring placement and removal (not published), and found spring cranioplasty has significantly shorter operative times. This correlates with the findings of Runyun et al for sagittal synostosis patients. There is a valid concern of the effect of anesthesia on the developing brain however it is unknown whether total length of anesthesia time versus number of anesthesia exposures is significant. 29 Lauritzen et al 28 pointed out that the lack of control of spring action should not be a point of objection because there is a large body of clinical experience using springs. Advocates of DO over springs feel that the distraction distance is less reliable with springs. We have found the amount of advancement we see has been consistent when 3 or more springs are employed. This may be explained by the observed consistency in outcomes with more springs because a larger force can be applied that is distributed more evenly along the osteotomies. 39
There are a few limitations of our study. Presently we have no followup greater than 5 years postop as our patients are still too young; therefore we can not fully assess if there is a relapse toward the preoperative craniofacial dysmorphology. Second, we do not have a database readily available to compare our patients against matched normals. We have not compared our FOAR versus spring cranioplasty results, but are in the process of collecting and analyzing this data. The qualitative and quantitative analysis of CT and clinical photos suggest a significant improvement in craniofacial form however measurements are performed in 2D. Future analysis would benefit from the use of geometric morphometrics, which would facilitate 3D assessment.
Conclusions
Here we report our experience and early outcomes with spring cranioplasty for UCS. We have found that when used in younger patients (<5 months) cranial springs can be a safe and effective strategy to minimize skull base scoliosis, facial scoliosis, and orbital asymmetry, as well as increase intracranial volume. Although long-term data needs to be assessed, we are optimistic that early correction of cranial base scoliosis will translate to stable results as patients reach dentoskeletal maturity.
Supplemental Material
sj-docx-1-fac-10.1177_27325016241287911 – Supplemental material for Spring-Assisted Cranioplasty in Unicoronal Synostosis: Analysis of Outcomes
Supplemental material, sj-docx-1-fac-10.1177_27325016241287911 for Spring-Assisted Cranioplasty in Unicoronal Synostosis: Analysis of Outcomes by Sarah Anne Frommer, Patrick Duffy Combs, Elizabeth Christine Tyler-Kabara and Patrick Kevin Kelley in FACE
Supplemental Material
sj-jpg-2-fac-10.1177_27325016241287911 – Supplemental material for Spring-Assisted Cranioplasty in Unicoronal Synostosis: Analysis of Outcomes
Supplemental material, sj-jpg-2-fac-10.1177_27325016241287911 for Spring-Assisted Cranioplasty in Unicoronal Synostosis: Analysis of Outcomes by Sarah Anne Frommer, Patrick Duffy Combs, Elizabeth Christine Tyler-Kabara and Patrick Kevin Kelley in FACE
Supplemental Material
sj-jpg-3-fac-10.1177_27325016241287911 – Supplemental material for Spring-Assisted Cranioplasty in Unicoronal Synostosis: Analysis of Outcomes
Supplemental material, sj-jpg-3-fac-10.1177_27325016241287911 for Spring-Assisted Cranioplasty in Unicoronal Synostosis: Analysis of Outcomes by Sarah Anne Frommer, Patrick Duffy Combs, Elizabeth Christine Tyler-Kabara and Patrick Kevin Kelley in FACE
Supplemental Material
sj-jpg-4-fac-10.1177_27325016241287911 – Supplemental material for Spring-Assisted Cranioplasty in Unicoronal Synostosis: Analysis of Outcomes
Supplemental material, sj-jpg-4-fac-10.1177_27325016241287911 for Spring-Assisted Cranioplasty in Unicoronal Synostosis: Analysis of Outcomes by Sarah Anne Frommer, Patrick Duffy Combs, Elizabeth Christine Tyler-Kabara and Patrick Kevin Kelley in FACE
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics Approval
University of Texas at Austin Institutional Review Board approval was obtained for this study under IRB # STUDY00002700.
Informed Consent
Written informed consent for publication of patient images and information was obtained from the patients’ legal guardians.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.