
Abstract
Introduction:
Comprehensive management of cleft lip with or without cleft palate (CL/P) often begins prenatally, continues into adulthood, and involves multidisciplinary collaboration. This study aims to review the current literature and summarize sociodemographic disparities that impact access to care, management, and postoperative outcomes in patients with CL/P.
Methods:
A systematic review was conducted using Pubmed, Embase, and Medline databases. Studies discussing sociodemographic disparities regarding access to care, management, and treatment outcomes for patients with CL/P were included. Studies performed outside the US and published before the year 2000 were excluded.
Results:
Of 3782 studies initially identified, 26 met the inclusion criteria. Disparities discussed included access to care (n = 11), missed appointments (n = 2), use of nasoalveolar molding [NAM] (n = 3), surgical timing (n = 8), and surgical outcomes (n = 8). Minority race or ethnicity, particularly black, Hispanic, Asian, and Native-American, as well as public insurance were associated with impaired access to care. Other factors causing impaired access to care were non-English primary language and high cost. Predictors for missed appointments were black race and Medicaid insurance. Decreased use of or success with NAM was associated with Asian race, public insurance, and long travel distance to a cleft care center. Factors associated with delayed CL surgery were Asian or black race, Hispanic ethnicity, public insurance, and non-English primary language. Surgical outcomes were assessed using various esthetic, speech, and quality of life measures; factors linked to worse outcomes included black or latin race and public insurance.
Conclusion:
Patients with CL/P from minority racial or ethnic groups, particularly black, Asian, and Hispanic, as well as those with public insurance are disproportionately impacted by health disparities. Disparities related to age, geographic location, and primary language have also been reported, among others. Statewide or institutional social programs may help address these disparities.
Keywords
Introduction
Cleft lip (CL) is one of the most common congenital anomalies in the world. In the United States, isolated CL (iCL) affects 1 out of every 2800 births while combined cleft lip and palate (CL+P) occurs in 1 out of 1600 live births. 1 Cleft lip with or without cleft palate (CL/P) can be diagnosed as early as 20 weeks gestational age during routine prenatal ultrasound screening.2,3
Comprehensive management of CL/P is multidisciplinary and involves collaboration between craniofacial surgeons, dentists, otolaryngologists, speech and language pathologists (SLP), and geneticists. Management can begin with family and genetic counseling in the prenatal period and often continues into early adulthood. Primary CL repair is routinely performed between 3 and 6 months of life.4,5 Early primary CL repair is crucial to promote feeding and growth, permit eventual speech production, and improve cosmetic appearance in this population.6,7 Other important aspects of effective CL management include pre- and/or postoperative nasoalveolar molding (NAM), cleft rhinoplasty, revision surgeries if needed, myringotomy, speech therapy, oral hygiene, and dental care. Children with unilateral iCL have been reported to have an average total number of 5.3 surgeries during their childhood and early adulthood, while those with CL+P require an average of over 9 surgeries before their mid-20s. 8
Given the prolonged, multidisciplinary treatment course needed for patients with CL/P as well as the benefits of early surgical repair, effective comprehensive management may be limited by sociodemographic barriers to care. While previous studies have reported different types of health disparities in the management of CL, there have been no systematic reviews summarizing these disparities. Therefore, the aim of this study is to perform a systematic review of the current literature to identify and describe sociodemographic disparities affecting access to, management of, and postoperative outcomes in patients with CL/P.
Methods
This study was conducted according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines. 9
Search Strategy
Literature searches were performed on October 25, 2022 using the Pubmed, Ovid Medline, and Embase databases. The search strategies for each database are provided in the Supplement and included all relevant keywords for “cleft lip” and “health disparities” (Supplemental File 1). Results included studies published online ahead of print publication. Prior to study screening and selection, the search strategy results were restricted to English language only.
Study Selection
Studies were screened by title and abstract using predefined inclusion and exclusion criteria. Screening was performed by 2 independent reviewers (CO, NM), and any differences were resolved by consensus. Duplicate studies were removed. Full text articles were then reviewed by the 3 independent reviewers (CO, AB, JB) for final inclusion. The following inclusion criteria were utilized: studies discussing any sociodemographic disparities regarding access to care, overall management, or treatment outcomes in patients with CL/P, published in and discussing disparities specifically within the US, and with a full text available in English. Review or summary articles, case reports, epidemiologic studies, opinion pieces, studies published before the year 2000, and those with no available full text article were excluded. The PRISMA guidelines were utilized for the entire study selection process (Figure 1).
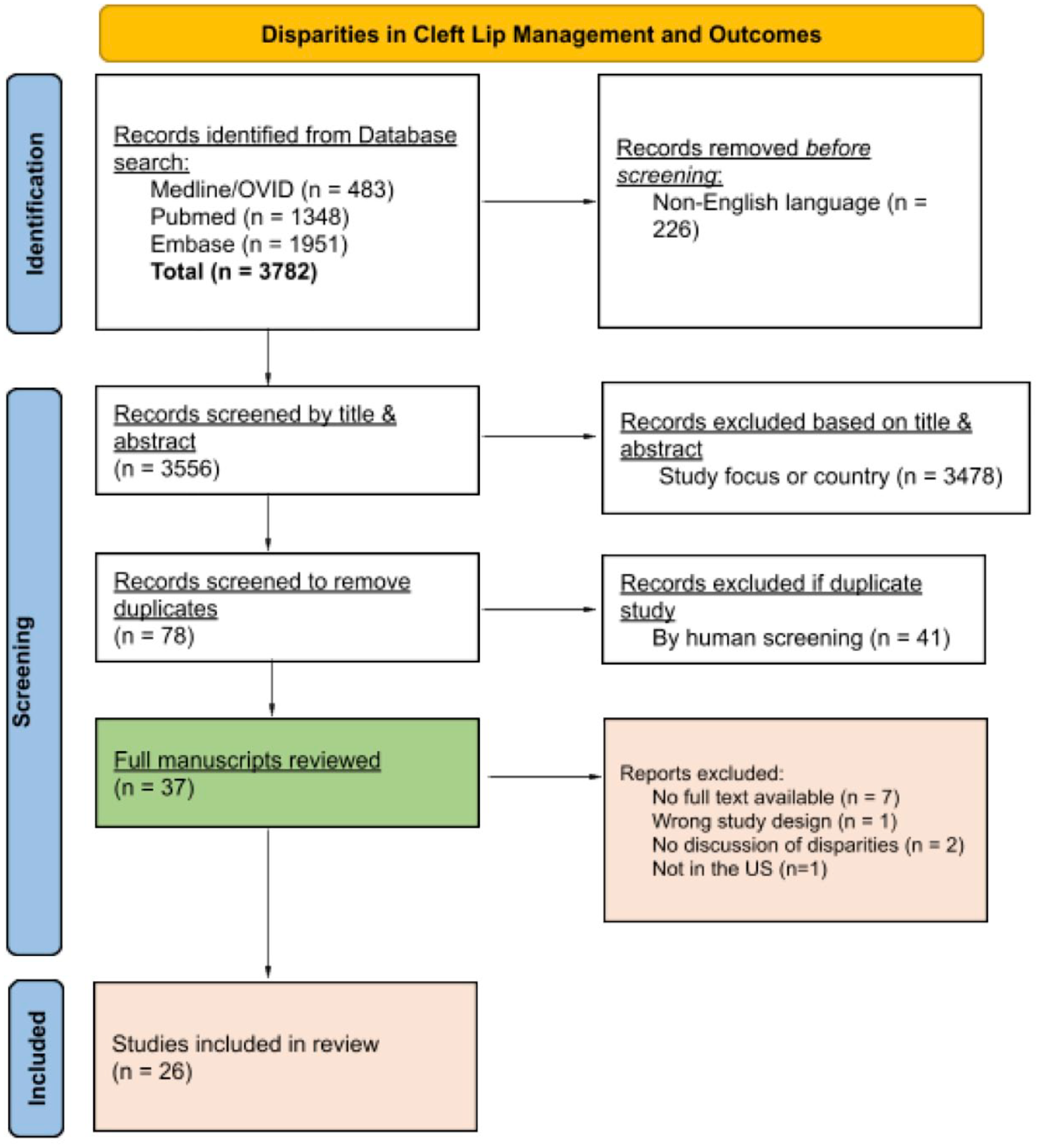
Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) study flow diagram.
Data Extraction
Data extraction was performed by 3 independent reviewers (CO, AB, JB) using standardized, predefined templates. Extracted data included the following: author information, publication year, study type, number of patients specifically with CL as well as demographic information such as sex, race, and/or ethnicity, and insurance status. For any studies discussing isolated CP (iCP) in addition to CL/P, only demographic information specific to patients with CL/P was documented. In addition, the patient age was uniquely defined in each study reviewed, with some using age categories and others reporting the mean or median age. Due to this inconsistency, patient age reported in each study was not documented for our review.
Data Organization
Studies were stratified into 5 predefined categories according to the type of health disparity discussed: (1) “Access to care,” (2) “Missed appointments,” (3) “Use of NAM,” (4) “Surgical timing,” and (5) “Surgical outcomes.” Studies were categorized as “Access to care” if they examined any barriers to CL/P care, including access to healthcare personnel or comprehensive cleft care centers, surgical evaluation or management, clinic visits, or speech therapy. “Missed appointments” studies focused on patients with appointments that were scheduled but not attended as well as patients who were lost to follow-up after initial evaluation. Any study primarily discussing utilization and outcomes after preoperative NAM were characterized as “Use of NAM.” “Surgical timing” studies focused on timely CL repair, which was defined uniquely by each study. Finally, studies discussing any type of postoperative outcome, including esthetic, speech, or oral health outcomes as well as postoperative complications and quality of life (QOL) were categorized as “Surgical outcomes.” Data was organized and stored on a secure, cloud-based spreadsheet (Google LLC; Mountain View, California).
Analysis
Due to considerable study heterogeneity, no quantitative meta-analysis was performed.
Results
Initial literature search yielded 3782 articles, 226 of which were screened out as non-English. After screening by title and abstract, 3478 articles were excluded. Forty-one articles were then identified as duplicates and removed. Thirty-seven articles were included for full text review. Of these 37 articles, 7 studies were excluded due to lack of an available full text, 2 studies were excluded because health disparities were not discussed, 1 article referred to a non-US based patient population, and 1 article utilized an irrelevant study design (evaluation of crowdfunding campaigns). Ultimately, 26 articles were reviewed in full.
Of all articles meeting final inclusion criteria, 13 (50%) were retrospective cohort studies, and 21 (80.8%) were published after 2010 (Table 1). Eleven (42.3%) articles discussed access to care, 2 (7.7%) discussed missed appointments, 3 (11.5%) discussed use of NAM, and 8 (30.8%) articles each discussed surgical timing or surgical outcomes. Of note, many studies failed to report demographic data for patients with CL/P separately from patients with iCP. For instance, only 9 studies specifically reported the number of black patients with CL/P. In contrast, most other studies reported the number of black patients with either iCP or CL/P, while some studies combined black patients with other racial minorities.
Study Characteristics and Demographic Information.
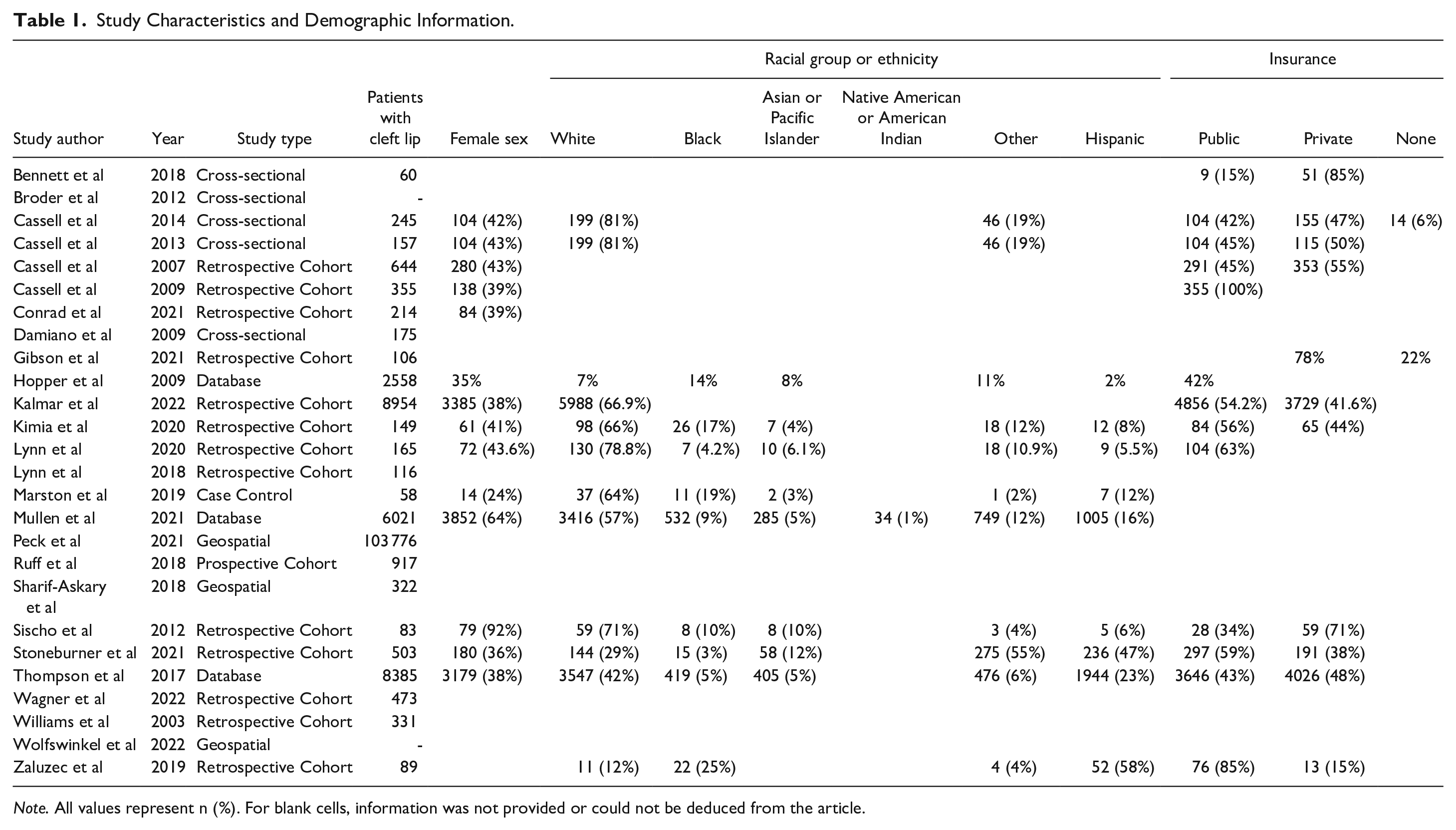
Note. All values represent n (%). For blank cells, information was not provided or could not be deduced from the article.
Access to Care
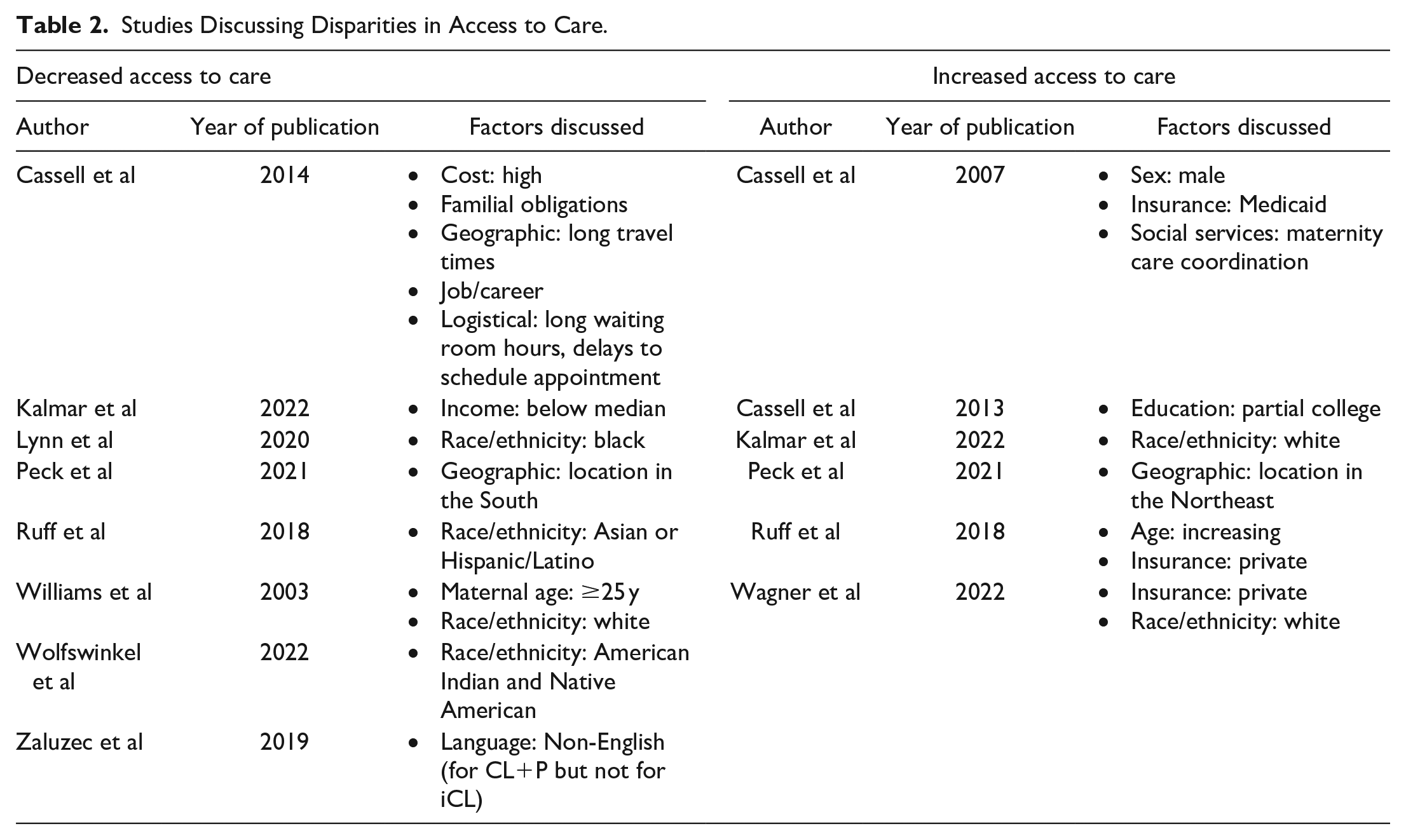
The most common factors associated with increased or decreased access to care were race/ethnicity and insurance status (Table 2).
Studies Discussing Disparities in Access to Care.
Race and Ethnicity
Several studies demonstrated that patients from minority racial groups have decreased access to care. In their 2020 retrospective, single-institution cohort study consisting of 165 patients with CL/P undergoing surgical repair, Lynn et al performed a multivariate analysis and found that black patients were first evaluated by a SLP 55 weeks later than non-black patients (P = .03). 10 In 2018, Ruff et al performed a prospective cohort study which included 917 patients with CL, and they found that Asian or Hispanic patients had significantly fewer surgeries than their white counterparts. 11 Furthermore, a recent geospatial study demonstrated that 47.1% of American Cleft Palate Craniofacial Association (ACPA) accredited centers situated in areas highly populated by American-Indian or Native American people were not staffed by craniofacial surgeons, compared to just 21.1% of ACPA centers nationwide. 12
Two other studies demonstrated that white patients had better access to care compared to other races. In their retrospective, single-center study including 473 patients with CL/P, Wagner et al examined health disparities before and after implementation of a cleft nurse navigator (CNN). 13 They noted that white patients had significantly more communication with nursing staff and had earlier cleft care than non-white patients before CNN implementation. After implementation, however, these racial disparities were no longer observed. In 2022, Kalmar et al found that white patients were more likely than non-white patients to be treated by a high-volume surgeon, defined by surgeon case volume greater than the 80th percentile (adjusted odds ratio [OR] = 2.5, 95% confidence interval [CI] 1.6-3.9). 14
While most studies demonstrated an association between minority race and decreased access to care, one study appears to challenge this finding. In a 2003 retrospective cohort study including 331 patients with CL/P from the Florida Birth Defects Registry, white patients were found to have lower rates of contact with state-run cleft management centers than black or Hispanic patients. 15
Insurance Status
Two studies evaluated the impact of private insurance on access to care. Wagner et al demonstrated that patients with private insurance had their first outpatient cleft care appointment 12 days earlier than those with public insurance before implementation of a CNN (P < .001). 13 This disparity was reduced but still remained after CNN implementation. In addition, Ruff et al showed that patients with private insurance had higher rates of esthetic procedures than those with non-private insurance. 11
In contrast, one study noted increased access to care for Medicaid-insured patients. In a 2007 study which included 644 patients with CL/P, Cassell et al reported that patients insured by Medicaid were more likely than non-Medicaid patients to be referred to the North Carolina Child Service Coordination Program, a state-run specialized service for children with birth defects. 16
Other Risk Factors for Decreased Access to Care
Non-English primary language has been linked to older age at the first clinic visit for patients with CL+P but not for those with iCL. 17 In a 2014 survey-based study, Cassell et al identified multiple barriers to care as reported by caregivers of children with CL/P, including high cost, familial or job obligations, and long travel distances. 18 Remaining risk factors for decreased access to care reported by other studies were low income level, maternal age over 25 years, maternal education lower than college level, and geographic location in the Southern US.14,15,19,20
Missed Appointments
Only 2 studies assessed health disparities related to missed appointments (Table 3). Lynn et al’s 2018 article defined missed appointment rate as the number of missed appointments divided by the number of scheduled appointments. 21 They found that black patients had significantly higher rates of missed appointments compared to white patients (P = .00). In addition, this study demonstrated that patients insured by Medicaid, from unstable households, or those with multiple siblings had increased rates of missed appointments compared to their counterparts in a multivariate analysis.
Studies Discussing Disparities in Missed Appointments and Use of Nasoalveolar Molding.
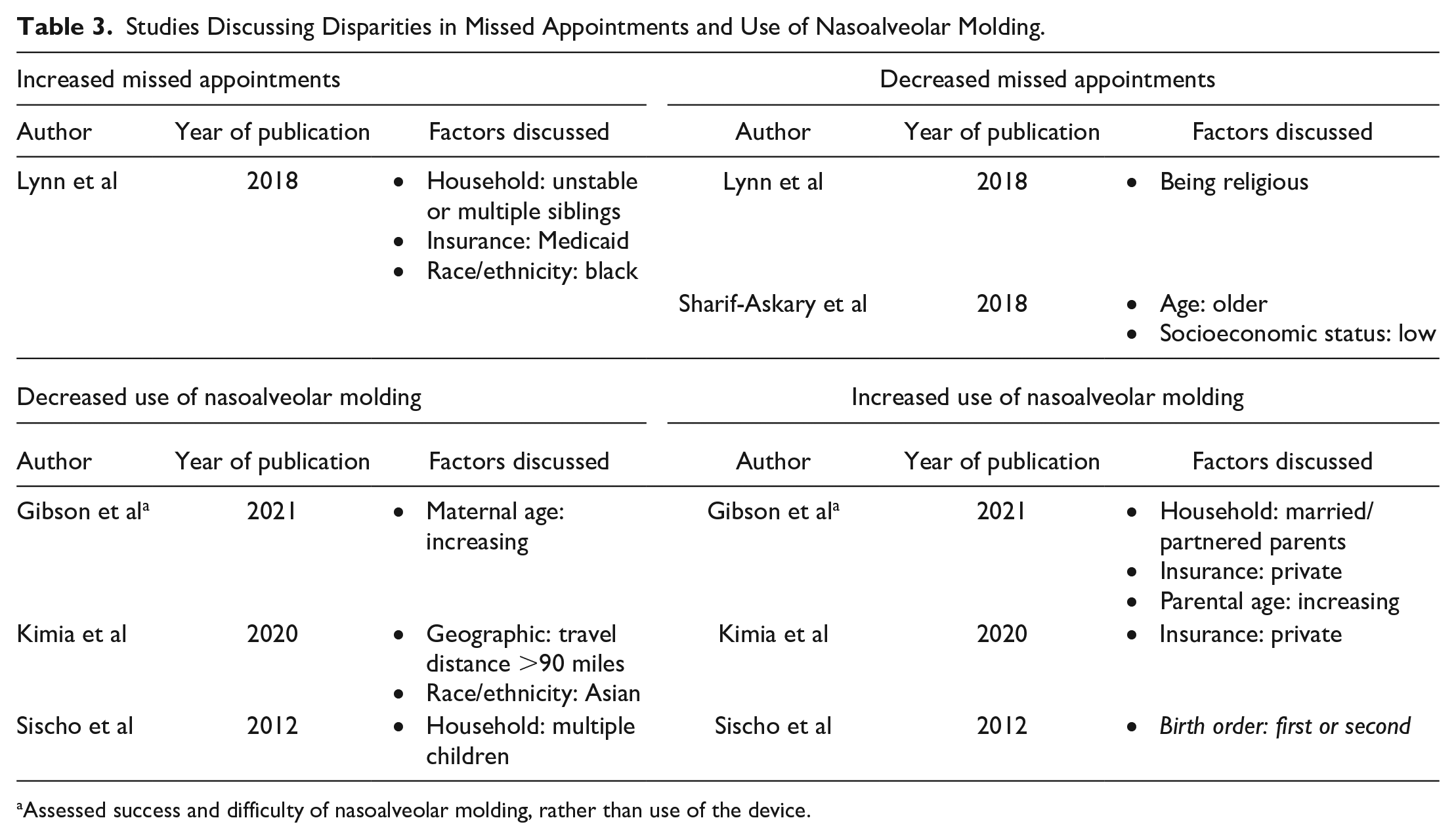
Assessed success and difficulty of nasoalveolar molding, rather than use of the device.
In a 2018 study, Sharif-Askary et al examined risk factors for “loss to follow-up” (LTFU), defined as missing 3 consecutive appointments despite attempts to resume follow-up or over 2.5 years with no attempted follow-up. 22 They performed 2 multivariate analyses–with and without consideration of geospatial dependency. Results demonstrated that patients who were older at the time of last follow-up had a lower odds of LTFU, regardless of geospatial dependency (OR 0.81, 95% CI 0.75-0.88 without geospatial dependency; OR 0.81, 95% CI 0.77-0.85 with geospatial dependency). In addition, lower socioeconomic status (SES), which was determined based on each patient’s address, was associated with a slightly lower rate of LTFU when considering geospatial dependency (OR 0.98, 95% CI 0.97-0.99), but there was no significant difference in LTFU based on SES when excluding geospatial dependency from analysis.
Use of Nasoalveolar Molding
Three studies assessed the use of preoperative NAM in patients with CL/P, with all reporting factors associated with increased and decreased use (Table 3).
Risk Factors for Decreased Use or Success
Kimia et al defined use of NAM based on attendance to clinic appointments and adherence to treatment. 23 They demonstrated that Asian patients were significantly less likely than white patients to use NAM (OR 0.09, 95% CI 0.01-0.97). In addition, patients with a travel distance of greater than 90 miles to the cleft care center were less likely to utilize NAM than those with a shorter travel distance (OR 0.27, 95% CI 0.09-0.80). In their 2012 retrospective cohort study, Sischo et al noted that patients with multiple siblings were significantly less likely to receive NAM than those with no siblings (P < .05). 24 Gibson et al focused on the success and difficulty associated with NAM use. 25 This study found that increasing maternal age was associated with decreased success in cleft gap closure (P = .041).
Factors Associated With Increased Use or Success
Kimia et al reported that patients with private insurance were more likely than those with public insurance to use NAM. 23 Similarly, Gibson et al showed that private insurance was associated with fewer appliance wear issues compared to non-private insurance, indicating lower difficulty of use (P = .019). 25 Married or partnered parents also had fewer appliance issues than single or divorced parents (P = .018). Gibson et al further found higher rates of cleft gap closure, indicating greater treatment success, in patients with married or partnered parents compared to single or divorced parents (P = .018) as well as in those with older paternal age (P = .007). Lastly, Sischo et al demonstrated that patients who were their parents’ first or second born were more likely to receive NAM than those who were third born or higher. 24
Surgical Timing
Most of the studies that discussed surgical timing focused on risk factors for delayed surgery, with race and insurance status being the most commonly cited risk factors (Table 4).
Studies discussing disparities in surgical timing.
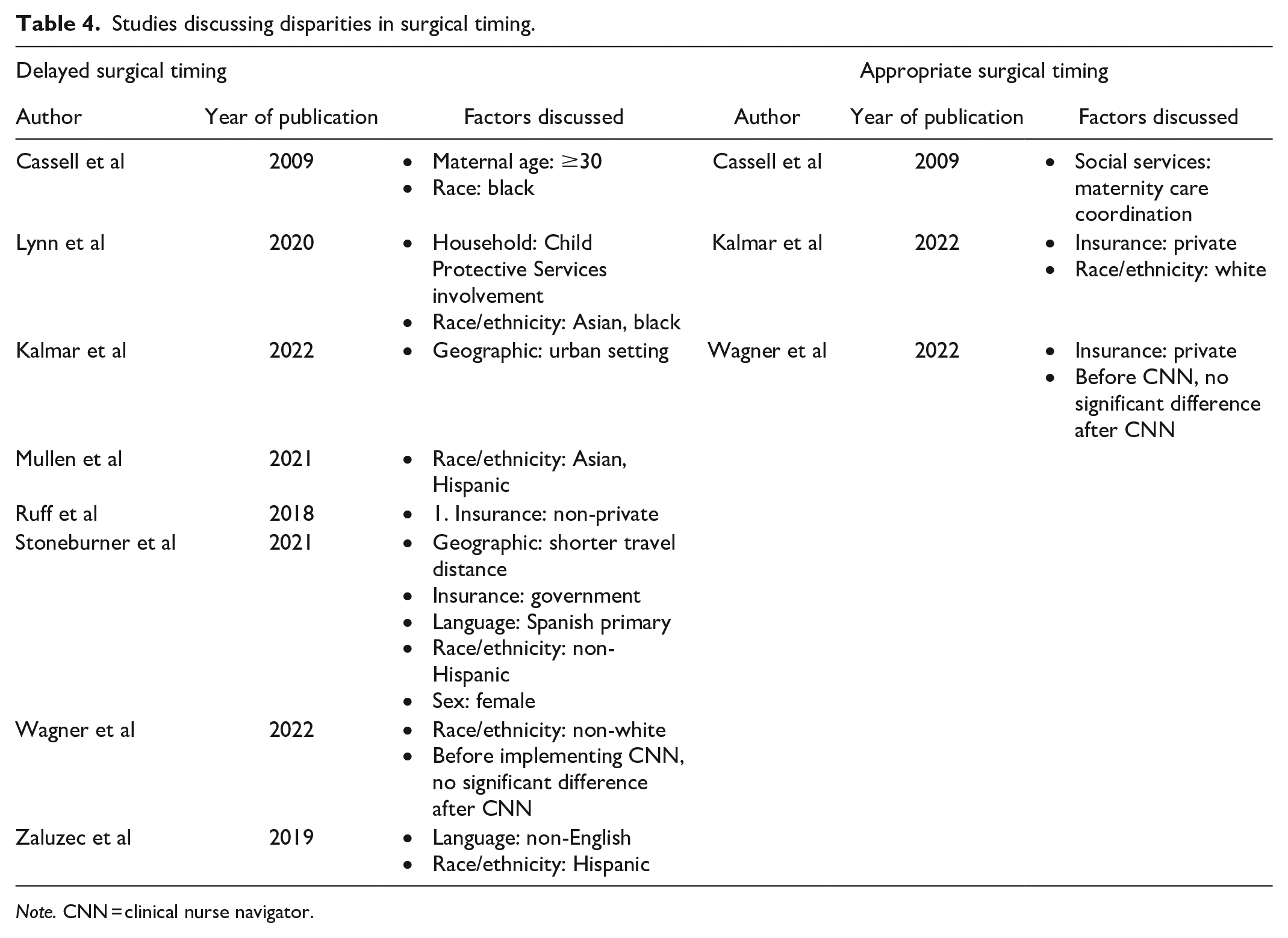
Note. CNN = clinical nurse navigator.
Race and Ethnicity
Multiple studies in this review have suggested that non-white or minority race was often associated with delayed operative intervention. In the 2009 study by Cassell et al, which included 355 patients with CL, timely cleft surgery was defined as occurring within 18 months of life in children with CL/P. 26 They conducted a multivariate logistic regression, which demonstrated that non-Hispanic black patients had a significantly lower odds of timely surgery than non-Hispanic white patients (adjusted OR 0.30, 95% CI 0.14-0.67).
In their 2020 study, Lynn et al noted that Asian and black race were both significantly associated with older age at the time of surgical repair compared with white race. 10 In a retrospective database review that included 6021 patients with CL, of which 285 patients (4.7%) were Asian, Mullen et al similarly demonstrated a higher likelihood of delayed CL repair in Asian compared to white patients. 27 Furthermore, Wagner et al showed that non-white patients received CL repair 16 days later than white patients before implementation of a CNN (P = .011), but this disparity decreased to 8 days after CNN implementation (P = .095). 13 Kalmar et al also noted that white race was associated with significantly earlier CL repair than non-white race (P < .001), which remained true for patients with unilateral or bilateral CL. 14
Several studies have examined the impact of Hispanic ethnicity on timeliness of surgery. Mullen et al reported an increased likelihood of delayed CL repair in Hispanic patients compared to Caucasians. 27 Likewise, Zaluzec et al found that Hispanic children had a significantly longer lag time, defined as time from first clinic visit to CL repair, than white children (3.8 vs 2.6 months, P = .05). In contrast to these findings, Stoneburner et al noted that non-Hispanic patients were significantly more likely to have delayed CL repair, defined as surgery after 6 months of life, compared to Hispanic patients. 28
Insurance Status
Two studies have cited non-private or public insurance as a risk factor for delayed CL repair. Stoneburner et al found that patients with government insurance were more likely to have delayed CL repair than those with private insurance. 28 In addition, Ruff et al noted that patients with non-private insurance were more likely to postpone recommended surgeries than those with private insurance. 11 Other studies have identified private insurance as a predictor of timely surgery. Both Kalmar et al and Wagner et al reported that patients with commercial or private insurance had significantly earlier CL repair than their publicly insured counterparts. However, Wagner et al further showed that this disparity was present before but was no longer observed after implementation of a CNN.
Other Risk Factors for Delayed Surgical Timing
Primary language spoken in the child’s household appeared to impact the timeliness of CL repair. Children were more likely to have delayed surgery if they were from non-English-speaking or primarily Spanish-speaking households.17,28 Other risk factors for delayed surgical timing were maternal age over 30, involvement of Child Protective Services in the household, and living in an urban location.10,14,26
Surgical Outcomes
Race and insurance status were repeatedly found to impact treatment outcomes (Table 5).
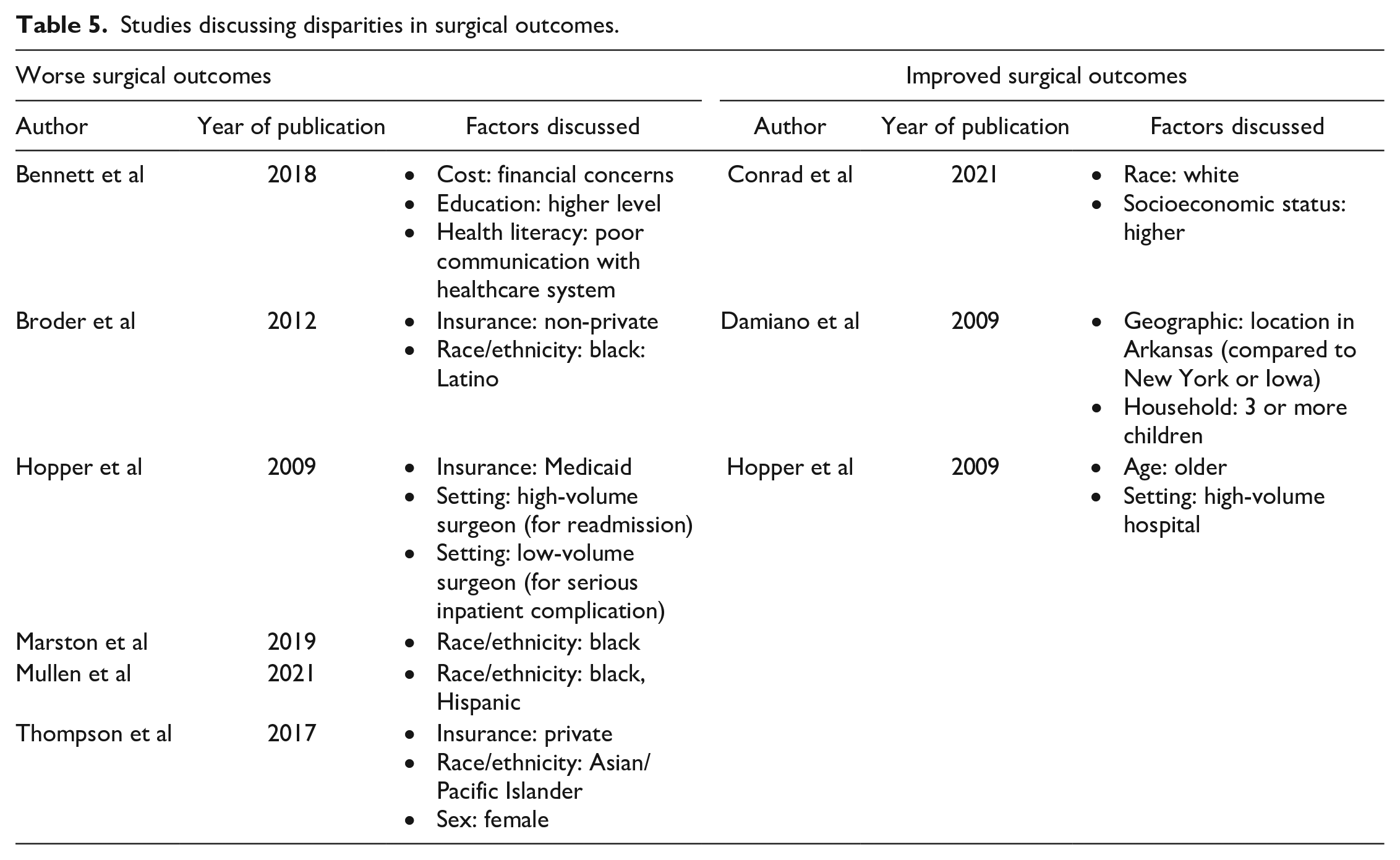
Studies discussing disparities in surgical outcomes.
Race and Ethnicity
Three studies showed that minority race, often black, was associated with worse surgical outcomes.27,29,30 Marston et al demonstrated worse scar outcomes in black patients compared to white patients, and Mullen et al showed higher readmission rates in black and Hispanic patients compared to Asian and white patients.27,30 In 2012, Broder et al utilized a survey instrument to assess various QOL measures. 29 Compared to Asian and white patients, black and Latino patients in this study had lower scores for emotional well-being (P < .001) and for school (P < .05), which was defined as their ability to engage in school-related tasks. Similarly, Conrad et al’s questionnaire-based study found that white race was predictive of better parent-reported functioning, despite controlling for the amount of surgeries undergone. 31
Insurance Status
Two studies reported public insurance as a risk factor for worse surgical outcomes. In Broder et al’s study, non-private insurance was associated with lower functional and emotional well-being scores. 29 Hopper et al performed a retrospective database study consisting of 2558 patients who underwent primary CL repair. In this study, patients with Medicaid demonstrated a higher odds of readmission compared to those with non-Medicaid insurance. 32 Thompson et al reported that private insurance was linked to a higher odds of CL revision. 33
Other Risk Factors for Worse Surgical Outcomes
Hopper et al showed that children undergoing primary CL repair at an older age were more likely to be discharged on the same day. 32 In addition, Bennett et al demonstrated worse caregiver-reported speech and esthetic outcomes from caregivers who expressed concerns about healthcare costs as well as those who endorsed low health literacy. 34 Thompson et al reported that female patients were more likely to undergo revision CL repair than their male counterparts. 33 Other factors impacting surgical outcomes were household size and practice setting.32,35
Discussion
Multiple health disparities affecting the overall management of CL/P as well as postoperative outcomes after CL repair have been reported. Most of the articles reviewed in this study were published in the last decade, suggesting a growing interest and awareness of this issue. A variety of sociodemographic factors were noted to impact the care of patients with CL/P, including race and ethnicity, insurance status, sex, primary language, and geographic location, among others. Disparities related to patient race and insurance status were most frequently reported. These represent possible targets for future advocacy efforts.
Patients from minority racial and/or ethnic groups, particularly black, Asian, and Hispanic, were disproportionately affected by disparities in all categories of CL/P management and outcomes defined by this study. One study demonstrated disparities in access to care specifically for Native-American or American-Indian patients. 12 However, it is important to note that this racial group was rarely included independently and was often combined with other racial groups due to a small sample size. As a result, it is possible that disparities for this racial group may be more prominent than reported in the literature. Nevertheless, exact reasons for the racial disparities observed in this study have not been well defined. Some studies speculate that differences in access to resources or cultural preferences may have a role.11,26 Though not commonly reported specifically in patients with CL/P, potential explanations for racial disparities have been explored across other medical specialties. These potential explanations include racial differences in socioeconomic status, access to resources, health literacy, or cultural practices as well as implicit bias among providers.36-38 Historical or ongoing systematic and discriminatory practices, such as residential segregation, that disproportionately impact racial minority groups may also play a role in the disparities observed in our review. 39 More than likely, the reasons for the racial disparities affecting patients with CL/P are multifactorial, involving a complex combination of the aforementioned factors.
Insurance status was another frequently reported disparity also affecting all categories defined in this study. Compared to those with private or commercial insurance, patients with public insurance more frequently encountered barriers to equitable care. These results suggest that publicly-insured children may be receiving a lower quality of cleft care than their privately insured counterparts.
Fortunately, some studies in this review have reported that disparities in CL/P management and outcomes may be mitigated by institutional or statewide social programs. Wagner et al’s study demonstrated improved racial and insurance disparities for both access to care and surgical timing after implementation of an institutional CNN. 13 In their 2009 study, Cassell et al evaluated the impact of maternity care coordination services, a program offering medical, psychosocial, and financial support during and after pregnancy for women eligible for Medicaid in North Carolina. They found that children of caregivers who received these services had a higher odds of timely cleft surgery within 18 months of life. 26 Though these studies report favorable results, larger, multi-institutional studies are necessary to reinforce the efficacy of similar or innovative social programs for reducing disparities in CL/P care.
This study has several limitations. In particular, all studies included in this review were retrospective or cross-sectional, which brings into questions the generalizability of these results. In addition, many of the studies were limited to a single institution. Furthermore, some studies combined results for patients with iCP and those with CL/P rather than reporting disparities for patients with CL/P separately, which increases the risk of confounding bias for our review. Lastly, while we were able to characterize all studies based on predefined categories, each study had unique methods for defining the outcomes assessed. For example, appropriate surgical timing was defined differently in each study that evaluated this outcome. Variations in the definitions employed across different studies may have introduced bias into our results.
Conclusions
Patients with CL/P from minority racial or ethnic groups, particularly black, Asian, and Hispanic, as well as those with non-private insurance are disproportionately affected by health disparities and may be at risk of receiving inferior care. Disparities related to sex, geographic location, and primary language have also been reported. Statewide or institutional social programs can help address these disparities. Future research should focus on developing new strategies to promote equity in the management of patients with CL/P.
Supplemental Material
sj-docx-1-fac-10.1177_27325016241227614 – Supplemental material for Revealing a Cleft in the Community: A Systematic Review of Sociodemographic Disparities Affecting the Care of Patients With Cleft Lip
Supplemental material, sj-docx-1-fac-10.1177_27325016241227614 for Revealing a Cleft in the Community: A Systematic Review of Sociodemographic Disparities Affecting the Care of Patients With Cleft Lip by Chioma G. Obinero, Alexandra Boyd, Jose Barrera, Alyssa Valenti, Naikhoba Munabi, Thomas Imahiyerobo and Matthew R. Greives in FACE
Supplemental Material
sj-docx-2-fac-10.1177_27325016241227614 – Supplemental material for Revealing a Cleft in the Community: A Systematic Review of Sociodemographic Disparities Affecting the Care of Patients With Cleft Lip
Supplemental material, sj-docx-2-fac-10.1177_27325016241227614 for Revealing a Cleft in the Community: A Systematic Review of Sociodemographic Disparities Affecting the Care of Patients With Cleft Lip by Chioma G. Obinero, Alexandra Boyd, Jose Barrera, Alyssa Valenti, Naikhoba Munabi, Thomas Imahiyerobo and Matthew R. Greives in FACE
Footnotes
Cleft Abbreviations
CL = Cleft lip
CL/P = Cleft lip with or without cleft palate
CL+P = Combined cleft lip and palate
CP = Cleft palate
iCL = Isolated cleft lip
iCP = Isolated cleft palate
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
Institutional Review Board approval was not required.
Informed Consent
Informed Consent was not required for this article
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.