
Abstract
Introduction:
We seek to evaluate the financial impact of the COVID-19 pandemic on pediatric craniomaxillofacial surgeries for cleft lip and/or palate. These surgeries are carefully timed for optimal outcomes, but the pandemic necessitated postponement or cancellation of elective procedures. Our study quantifies the decline in cases and associated charges at a single academic medical center before and after the pandemic.
Methods:
After receiving Institutional Review Board approval, we analyzed the financial billing data of 83 patients who underwent cleft lip and/or palate repair at an academic medical center. The caseload and charges incurred in the year before the COVID-19 pandemic (March 2019 to February 2020) were compared to the 2 years following the pandemic’s onset (March 2020 to February 2022). Statistical analysis was conducted using paired t-tests and the Wilcoxon signed-rank.
Results:
In the year following the onset of the pandemic, we observed a significant decrease in the number of cleft lip and/or palate repairs performed per month (from 2.75 to 1.42 per month, P-value .021) and a decrease in per-month charges for these procedures ($13 334.75 to $7237.17 per month, P-value .036). However, when examining data over the 2 years post-COVID, these differences no longer remain statistically significant (P-value .25 for cases and P-value .32 for charges), indicating a return to pre-COVID baseline.
Conclusion:
There was a statistically significant decrease in cleft lip/palate repair surgeries in the 12 months following the start of the COVID-19 pandemic. Both the caseload and total charges decreased after March 2020, with a subsequent return to baseline after 2 years. These findings emphasize that the pandemic had a transient impact on pediatric craniomaxillofacial surgical volume at our institution. While acknowledging our study’s external validity, we advocate for a nuanced approach, with flexible staffing crucial in facilitating a swift return to normal elective volumes.
Introduction
Experts theorize that the SARS-CoV2 virus entered the U.S. as early as December 2019, subsequently drastically impacting the entire world economy, particularly the healthcare sector. 1 The U.S. government recommended to defer nonessential surgical care, leading to institutions cancelling or deferring elective surgical procedures. 2 These deferrals and cancellations caused large backlogs in procedural care, causing progression of patient disease and stress on hospital systems across the country. One study that analyzed surgical volume at a 1017-bed quaternary care center revealed a 44.6% decline in weekly surgical volume during the peak of the COVID-19 pandemic, with surgical volume increasing to approximately 86% of pre-pandemic levels post-pandemic. 3 While this number accounts for all different types of surgical procedures, the American Hospital Association shows that the reduction of elective procedures, which account for a disproportionately large amount of hospital revenue and margins, caused $200 billion in financial losses between March and June 2020, prior to accounting for relief funds. 4 When analyzing which specialties were affected the most, McKinsey & Company showed that orthopedic surgery, otolaryngology, and plastic surgery represented the largest relative decline in surgical volume amongst all specialties. 5 There are a variety of mechanisms describing how these delays in care lead to increased patient morbidity, with one being the decreased financial and organizational capacity of hospitals provide care for months and years to come, leading to progression of disease states and suboptimal outcomes.
With the threat of future pandemics and new virus variants, it has become increasingly important to understand the financial implications of reduced operating room (OR) capacity, as this has direct effects on hospital system sustainability and patient outcomes. Currently, there is minimal literature on how cancellation and deferral of specific types of procedures impacted hospitals’ financial health. Stratifying this analysis by procedure type is particularly important as different surgical procedures generate varying amounts of revenue and gross margin for hospitals. Since cosmetic and reconstructive surgeries specifically provide cushion for hospital margins, analyzing how cancellation of specific cosmetic/reconstructive procedures impact hospital liquidity and cash flow will allow us to better understand how the financial health of hospital systems can be negatively impacted by OR delays and cancellations. This will allow administrators and clinicians to strategize how to mitigate losses associated with reduced OR capacity and maintain financial solvency.
For cleft lip and palate cases in particular there is a need to identify the effects of rapid changes in resource allocation to accommodate the expected increase in volume of COVID-19 cases while concurrently decreasing potential exposure for young children requiring head and neck surgeries. Additionally, while cleft lip and/or palate has previously been categorized with a non-emergent surgical status, the need to determine the delay in care relies on the practice of coordinating the sequence of cleft lip and palate repair in time with the development of the child. This tightly controlled coordination increases the odds of a more favorable outcome. With the emergence of the COVID-19 pandemic, potential delay in operative cases may likely affect overall outcomes for the cleft lip and palate repair cases.
In this study, we hope to characterize the financial losses experienced by a single, tertiary hospital system in the southeastern United States due to pandemic-associated reduced OR capacity by analyzing the financial implications associated with cleft lip and cleft-palate repair procedures. As these procedures are typically done by either plastic surgeons or ENTs specialized in facial plastics, this procedure will help illustrate financial losses associated with the most at-risk specialties, as these were 2 of the 3 specialties reported with the largest decrease in surgical volume. 5
Methods
This study is a retrospective review of financial data obtained from the Department of Plastic and Reconstructive Surgery at an academic medical center. It obtained an exemption from the Institutional Review Board. The specific focus of the study was on the repair of cleft lip/nasal deformity, using the CPT codes 40700 and 40701, as well as palatoplasty for cleft palate, using the CPT codes 42200 and 42210. The study period spanned from March 2019 to February 2022, encompassing 2 distinct time periods: before (March 2019 to February 2020) and during/after (March 2020 to February 2021) the onset of the COVID-19 pandemic.
The study analyzed and compared the average monthly number of cases, the average amount billed to insurance providers, and the average revenue received from insurance providers. To perform the analysis, monthly averages were calculated for each parameter and compared between the 2 groups: the 12 months preceding the COVID-19 pandemic and the 12 months during/after the pandemic. Microsoft Excel (Microsoft Corporation, Redmond, Washington, USA) was used for statistical analysis. The paired t-test and the Wilcoxon signed-rank test were employed to compare the average monthly caseload, charges, and reimbursement between the 2 groups. The paired t-test, a parametric test, offers greater statistical power; however, due to the limited sample size of this study, the non-parametric Wilcoxon signed-rank test was used as an additional measure of significance. A significance level of P < .05 was set to determine statistical significance.
Results
In the 12 months prior to the onset of the COVID-19 pandemic, there were a total of 33 cleft lip/palate repairs performed at this academic medical center, working out to an average of 2.75 cases per month (Figure 1). A total of $160 017.00 was charged to insurers, and a total of $30 828.01 was paid by insurers for the same time period, with monthly averages of $13 334.75 and $2569.00, respectively (Figure 2). In the 12 months following the onset of COVID-19, there were a total of 17 cleft lip/palate repairs, with an average of 1.42 cases per month (Figure 1). A total of $86 846.00 was charged to insurers, and a total of $17 356.81 was paid by insurers for the 12 month period following the onset of COVID-19, with monthly averages of $7237.17 and $1446.40, respectively (Figure 2).
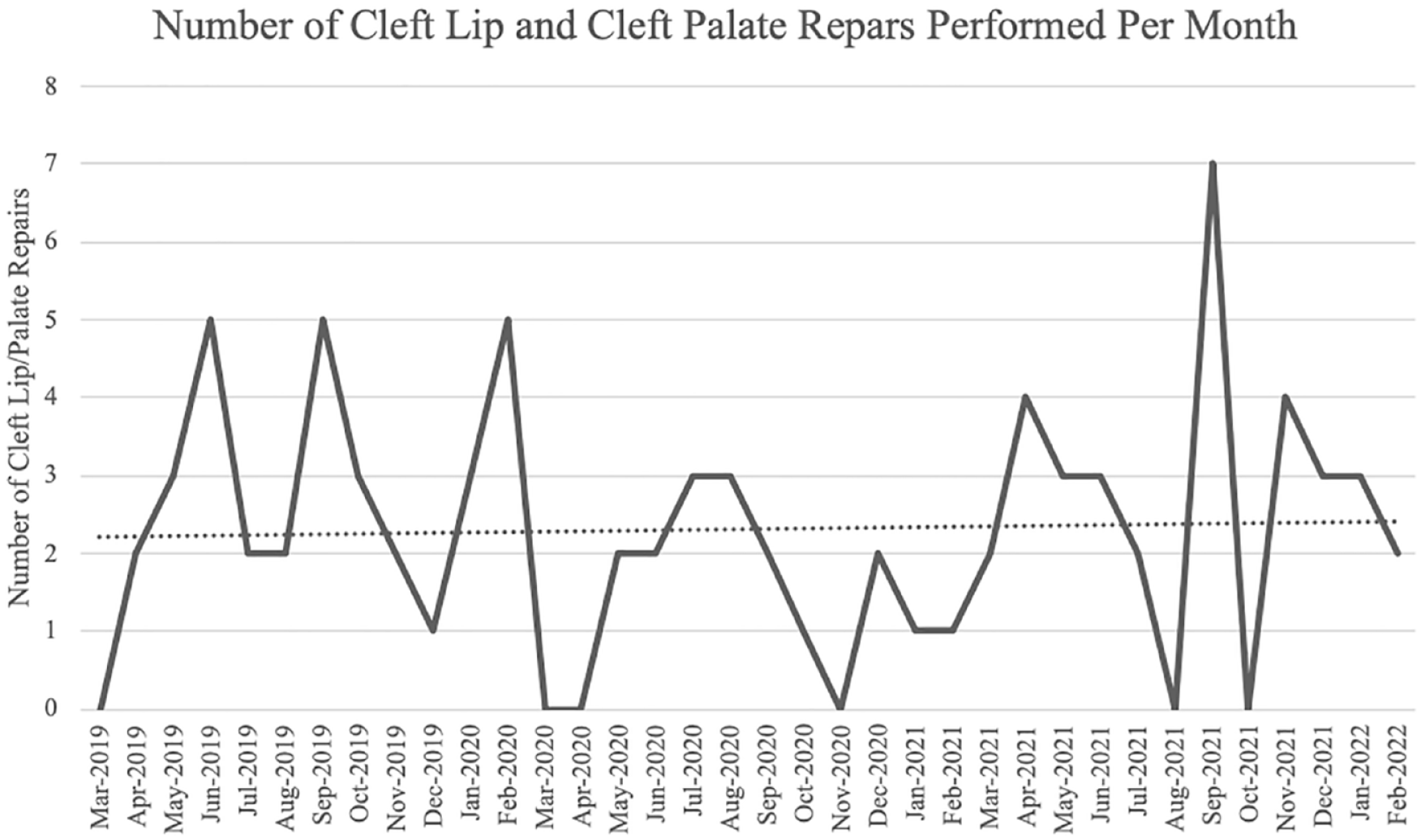
Number of cleft lip and palate repairs performed per month from March 2019 to February 2022.
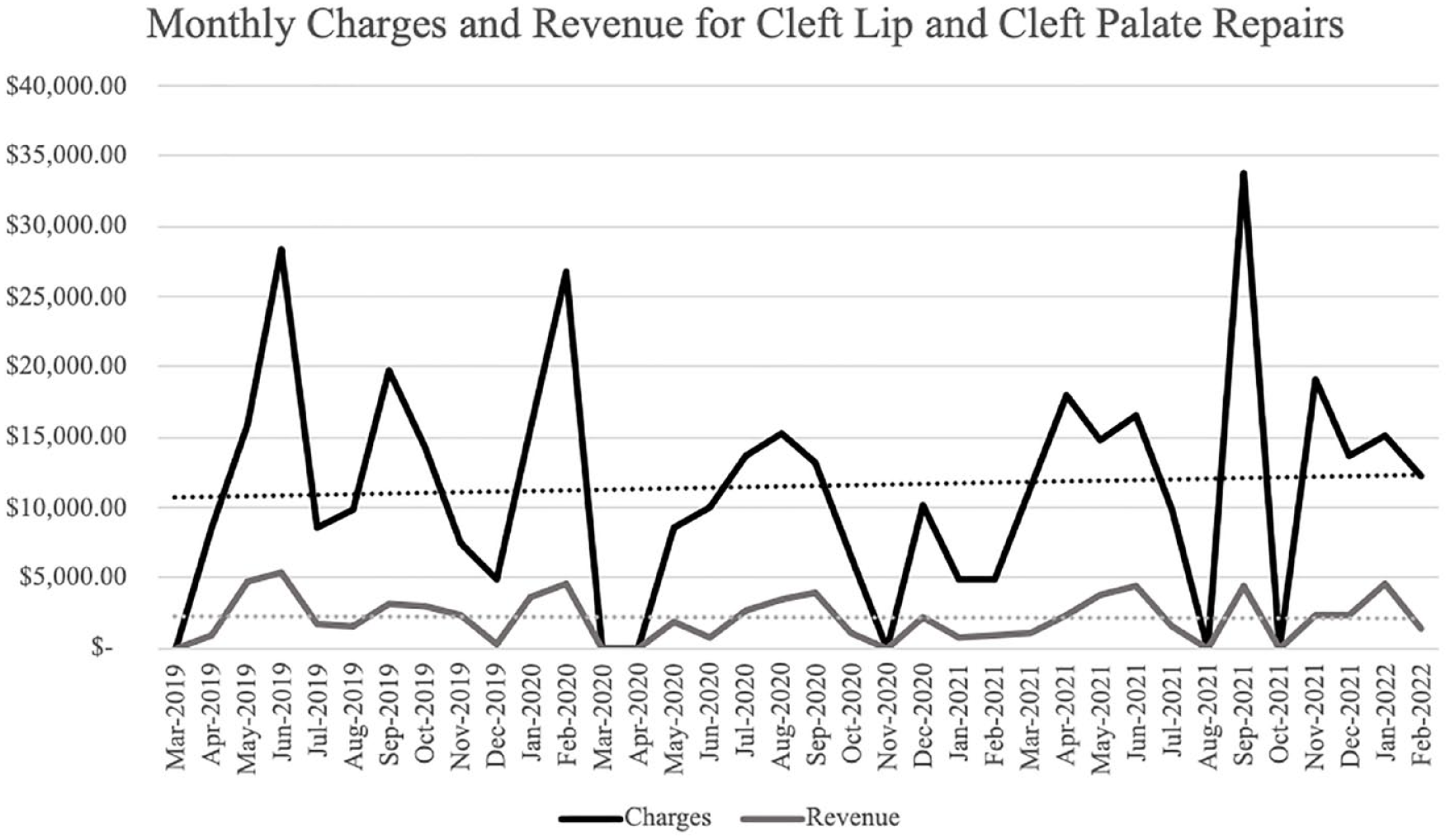
Monthly charges and revenue received for cleft lip and cleft palate repairs from March 2019 to February 2022.
Comparing the monthly average cases of cleft lip/palate repairs performed in the 12 months prior to the onset of the COVID-19 pandemic in March of 2020 to the 12 months post-onset, the average decreased by 1.33 (Figure 1). This decrease reached statistical significance, shown by a paired t-test with a P value of .021. The test statistic from the Wilcoxon signed-rank test was 7, which is smaller than the critical value of 13. Thus, this test also demonstrated a statistically significant decrease in the number of cleft lip/palate repairs in the year following the onset of the COVID-19 pandemic.
When analysis of the number of cleft lip/palate repairs is expanded to include the first 24 months following the onset of the COVID-19 pandemic, the average monthly number of cases decreased from 2.75 to 2.09 (Figure 1). However, this decrease fails to reach statistical significance (P value = .25).
Comparing the monthly amount charged to insurers in the 12 months prior to the onset of the COVID-19 pandemic to the 12 months post-onset, there was an average monthly decrease of $6097.58. This decrease reached statistical significance, shown by a paired t-test with a P value of .036. The test statistic from the Wilcoxon signed-rank test was 10, which is smaller than the critical value of 13, showing a statistically significant decrease in the amount charged to insurers per month for cleft lip/palate repairs in the year following the onset of the COVID-19 pandemic.
When analysis is expanded to include the first 24 months following the onset of the COVID-19 pandemic, the average monthly amount charged to insurers decreased from $13 334.75 to $10 464.21 (Figure 2). However, this decrease fails to reach statistical significance (P value = .32).
Finally, the amount of revenue received by insurers for cleft lip/palate repairs per month did decrease by $1122.60 after the onset of the COVID-19 pandemic. However, this decrease failed to reach statistical significance (P value = .11), and this statistical insignificance is further established by the Wilcoxon signed-rank test, with a test statistic 19 being greater than the critical value of 13. Additionally, when analysis is expanded to include the first 24 months following the onset of the COVID-19 pandemic, the decrease in the average amount of revenue received from insurers per month shrinks to only $677.52. This decrease is also statistically insignificant (P value = .24).
Discussion
The impact of the COVID-19 pandemic on surgical volume is an on-going investigation as institutions continue to gather objective data. One study has reported a decrease of 48.0% in surgical cases. 6 Strategically designed healthcare policies aimed at limiting the spread of viral infections resulted in restrictions on non-emergent or elective surgeries. While these necessary measures sought to protect public health, they consequently impacted surgical volumes, leading to profound financial repercussion. 7 Of the specialties affected, plastic surgery was expected to endure a dramatic impact due to the predominantly elective nature of its surgical procedures. 8 However, given the lasting impairment linked to the delay of treatment of cleft lip and cleft palate, it may be regarded as essential by definition. 9 While surgical repair of cleft lip or cleft palate is not regarded as fully elective, healthcare policy changes amidst the pandemic may have led to a delay in care for these conditions. ACPA modified guidelines, instructing providers to delay treatment to ensure patient safety during. 10 Thus, the primary objective of this study was to examine the repercussions of the COVID-19 pandemic on the volume of cleft lip and/or cleft palate repair cases, as well as the associated charges and total payments, within a single institution. With this data, hospital systems will be able to more accurately project financial losses in order to more effectively manage their revenue cycle and OR capacity, and consequently improve patient outcomes by providing effective care.
Our analysis demonstrated that 12 months after the onset of the pandemic, the average number of cleft lip and cleft palate repair cases as well as the per-month charges decreased. These results align with the ACPA’s guidelines to defer cleft lip repair during the COVID-19 pandemic. 10 Additionally, our findings are consistent with the results reported in other studies, which highlight the significant impact of the COVID-19 pandemic on cleft lip/palate surgeries and other surgical procedures.9,11 However, our study failed a find a statistical difference in the monthly revenue received from insurers in the 12 months following the pandemic onset. This is likely due to the small sample size, and thus relatively small decrease in monthly revenue ($1122.60), contained within this study. Further analysis that pulls from multiple institutions could provide a more robust set of data that answers this question on revenue; however, given that both caseload and charges to insurers were significantly lower in the 12 months post-pandemic, the logical outcome would be that revenue from these insurers would decrease as well.
In the 2 years following the pandemic, results do not indicate a significant difference in case volumes, per-month charges, and revenue incurred compared to the pre-pandemic period. These findings strongly suggest a return to pre-pandemic surgical rates, which may be influenced by multifactorial dynamics. A major contributing factor to this notable rebound can be attributed to the backlog of surgical procedures that accumulated during the pandemic.7,11,12 The resumption of cleft lip and palate surgeries, which are critical for achieving optimal surgical and speech outcomes, may reflect the families’ desire to schedule these procedures, in addition to addressing the backlog of new cases awaiting repair. Additionally, studies have observed that physicians and health systems rapidly adapted to the new changes and created local guidelines to prioritize and continue surgical procedures.6,13 It is reasonable to presume that 2 years after the onset of the COVID-19 pandemic, hospitals had established robust and effective testing and vaccination guidelines to control viral spread and ensure the uninterrupted continuation of operations. Altogether, this suggests that the pandemic had a temporally significant effect on cleft lip and palate repairs, but the effect wears off by at least the 2-year mark. This inference demonstrates that during the early stages of the pandemic, healthcare protocols demanded and underwent a rapid evolution to address emerging challenges. However, as hospitals implement resilient counter-measures to better navigate the ongoing effects of the pandemics, surgical volumes returned to baseline. Importantly, based on what we have observed, such wide system shut down is very costly, disruptive, and at the core, not really beneficial nor necessary. With this knowledge, we can gain a better appreciation of the long-term clinical impacts the COVID-19 pandemic will have on those whose care was delayed.
We hope that the data from this study will allow hospital administrators and clinicians to use advanced analytics and forecast demand and manage capacity in real time, allowing health care systems to optimize delivery of care and patient outcomes while simultaneously respecting and abiding by sanitation protocol and federal guidelines if faced with another mass closure of operating rooms. This study provides hospital administrators with the ability to forecast demand more accurately. This insight facilitates the forecasting in changes to surgical volumes amidst a pandemic by providing historical data and practice proactive flexible resource allocation, ensuring that staffing levels, equipment availability, and other supply chains align with anticipated surgical volumes. The integration of such analytics into real-time decision-making processes can empower hospitals to adapt swiftly to unexpected events, such as mass closures of operating rooms, while adhering to sanitation protocols and federal guidelines. Furthermore, the study’s data can be leveraged to enhance operational efficiency by identifying optimal scheduling practices and contributing to cost management. By correlating surgical outcomes with variable factors, hospitals can improve patient outcomes without compromising on efficiency or financial sustainability. While a better understanding of the institutional impact of cleft lip and palate surgeries amidst the pandemic is now available, the long-term clinical impact of the delay in care remains unknown. Healthcare systems shifted their focus on prioritizing patient and provider safety and allocating resources effectively. However, the potential implications of postponed cleft lip and palate repairs warrant continued research to enhance evidence-based guidelines and preparedness for future pandemics. Furthermore, the emergence of new variants and viruses continue to pose a significant risk to hospital system liquidity. An adequate characterization of the losses and change in cash flow will help hospitals maintain financial sustainability during unforeseen challenges.
As our study is a retrospective investigation of case volume and reimbursement data at a single institution, which may introduce certain limitation, impacting the findings reported. The study relies on accurate documentation and is susceptible to charting and coding errors. Additionally, because we analyzed a single institution, the findings may not be fully representative of other institutions with differing state insurance policies, hospital reimbursement procedures, and state-specific guidelines during the COVID-19 pandemic.
Conclusion
The COVID-19 pandemic led to a massive nationwide delay in surgical care, and as surgical procedures tend to provide substantial financial cushion to hospitals, these delays have potential to negatively impact hospital finances and their capacity to provide effective care. With threats of future respiratory virus variants, understanding the downstream effects of surgical delays is of crucial importance. Given the study’s design nature, external validity is limited. Nonetheless, the findings yield crucial insights. At our institution, the impact of the recent COVID-19 pandemic on orofacial cleft surgical volume is transient. These findings strongly advocate against the layoff of operating room staff, as such a practice would impede the anticipated post-pandemic ramp-up. Instead, a more viable solution is the implementation of flexible staffing, distributing the reduced workload evenly among nursing staff during the pandemic’s peak, recognizing the temporary nature of this perturbation. Most significantly, our observations suggest that a stringent shutdown is not beneficial. Avoiding such indiscriminate measures could potentially ease the post-pandemic recovery process. These findings collectively offer valuable guidance for navigating the challenges posed by the pandemic and optimizing healthcare operations for the future.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
IRB No. 1939136-2