
Abstract
Introduction:
The present review explores the existing documentation in the literature related to the fixation of mandibular fractures undertaken in maxillofacial surgery.
Methods:
English language articles were searched in various databases such as Pubmed, Scopus, Science Direct and Google Scholar. The keyword used for searching are “Mandible Fracture,” “Maxillomandibular fixation,” “Fixation” and “Recent Advancements.”
Results about the history of fixation:
Extended history into the pre-Christian era, early medieval, through the 17th, 18th and 19th, 20th, 21st centuries have been dealt in the narrative review. Emphasis on the present plating system with focus on present and future prospects like AI, virtual reality as well as Magnesium based plating systems have also been dealt here.
Conclusions:
The present review spotlights on understanding present, past, and future aspects of fixation of mandibular fractures. Currently, titanium plates are being used and the most popular materials though future holds good prospects for polymer based and magnesium based materials.
Introduction
History plays a crucial role in understanding the past and predicting the future, providing a foundation for the development of new approaches and improving our understanding of current procedures. This narrative review article explores the history of fracture treatment in maxillofacial surgery, highlighting key advancements and notable contributions from ancient civilizations to the modern era. Various databases like Pubmed, Scopus, Science Direct and Google Scholar were utilized for searching English language articles. Keywords used for searching were “Mandible Fracture,” “Maxillomandibular fixation,”“Fixation.” By tracing the evolution of fracture management techniques, we can gain valuable insights into the development of current practices and appreciate the progress made in craniofacial fracture treatment.
Past
The Pre-Christian Era
Hammurabi’s ancient law system, documented on clay tablets, includes an early reference to fracture care in 5000 B.C. The Edwin Smith papyrus, translated by Prof. Breasted, 1 was discovered in Egypt around 1600 B.C. and seems to be a military surgeon’s work. It provides instructions for reducing a dislocated mandible by placing the thumbs on the ends of the mandible and using fingers under the chin to guide it back into place. Simple jaw fractures were treated with bandages soaked in honey and egg whites, while fresh meat was applied to wounds on the first day. In ancient India, pedicle flaps sourced from either the forehead or cheek were used to repair defects concerning the nose or lips, as a means of punishment. Asklepios, renowned for his war wound care during the Trojan Wars, became a symbol for the medical profession, represented by the Caduceus. Hippocrates, born in 460 B.C., introduced the concept of connecting loose teeth with a gold or linen thread until the bone healed. Bandaging with Carthaginian leather strips provided support for jaw fractures. Hippocrates cautioned that incorrect bandaging could cause harm despite its limited benefits for jaw fractures.
The Early Medieval Period
During the Roman Empire, there were no significant advancements in the treatment of maxillofacial injuries, and physicians continued to rely on Hippocratic methods. In 1275, the first European Medical School was founded in Salerno, Italy. Guglielmo Salicetti published detailed instructions on treating mandible fractures in his book Praxeos Totius Medicinae. These instructions closely resembled those of Hippocrates. Interestingly, Salicetti’s 2 later work in 1492 introduced the concept of using the stable upper jaw’s teeth to immobilize the lower jaw, a concept that was later forgotten until its reintroduction by Gilmer in 1886. Gunshot wounds during that time were believed to contain poisonous substances, so they were treated with boiling oil and cautery, often resulting in deformities. In 1572, Ambroise Paré, a surgeon from medieval Europe, endeavored to treat wounds using soothing slaves. 3 He suggested using pieces of cloth placed on either side of the wound and stitching them together, allowing the flesh to adhere and heal.
The 17th and 18th Centuries
We can find references to maxillofacial injuries during the English Civil War and also by the early part of the 18th century, a lot of progress was made in anatomical and physiological knowledge. Pierre Fauchard’s book titled Traite de Chirurgie Dentaire 4 in 1728 paved the way for the development of dental prostheses and techniques for controlling fracture fragments using teeth ligation and bandages. In their work “Traite des Maladies Chirurgicales” published in Paris in 1779, Chopart and Desault introduced a splint made of iron, resembling a shallow trough, which was inverted and positioned over the occlusal surfaces of the lower teeth flanking the fracture line. This device was secured firmly by screws that manipulated rods connected to a submental plate crafted from sheet iron, forming an intra-oral apparatus. 5 Consequently, the compression between the occlusal teeth surfaces and the lower mandibular border effectively hindered any motion of the fragments. Variations of this principle were used in Germany, England, and Holland.
The 19th Century
The 19th century witnessed significant advancements in fracture treatment techniques. Von Graefe’scranio-maxillary suspension apparatus (Figure 1), introduced in 1823, revolutionized external suspension methods. 6 In 1824, Ringelmann mentioned that Laudet(1812) had utilized a wire passed through the alveolar bone to assist in securing an upper denture. 7 This technique is similar to the current per-alveolar wiring method used for an edentulous upper jaw. In 1840, Baudens presented a method for managing oblique jaw fractures by running a wire around the bone and wrapping it over a molar tooth. 8 This technique evolved into the modern circumferential wiring used to keep a splint in place in an edentulous mandible. Transosseous wiring using iron or silver wire was performed by Buck, Kinloch, Annandale, and Cotton in the mid-1800s.9-11 Hamilton in 1857 noticed that the traditional 4-tailed bandage could displace the fractured jaw fragment posteriorly increasing the risk of respiratory obstruction. 12 In 1866, Guerin made a discovery that trauma occurring beneath the orbits not only leads to fractures in the maxillary bones but the pyramidal portion of the palatine bone and the pterygoid processes of the sphenoid bone are also impacted. The presence of echymosis around the greater palatine foramen can help in diagnosing low-level upper jaw fractures. 13 Before plastic surgery, facial and jaw injuries were often treated by skilled metal craftsmen who created intra-oral and extra-oral prostheses. Thomas Brian Gunning developed a splint of vulcanized rubber in the 1800s. 14 He used a monobloc splint for significant vertical displacement, held in place by screws in both jaws. 15 Gilmer rediscovered the technique of ligating individual teeth with annealed soft copper wire to immobilize the mandible. In 1907, Gilmer described the arch-bar method of fixing, using a German silver wire that connected upper and lower teeth. 16 Angle introduced modified orthodontic bands and threaded arch bars for controlling jaw fractures in 1890. 17 Rene le Fort’s studies in 1901 provided a comprehensive understanding of bone displacements and fracture patterns in the facial skeleton. 18 Fractures of the orbital floor and zygomatic bone received attention from Lang, Matas, Lothrop, and Keen in the late 1800s and early 1900s.
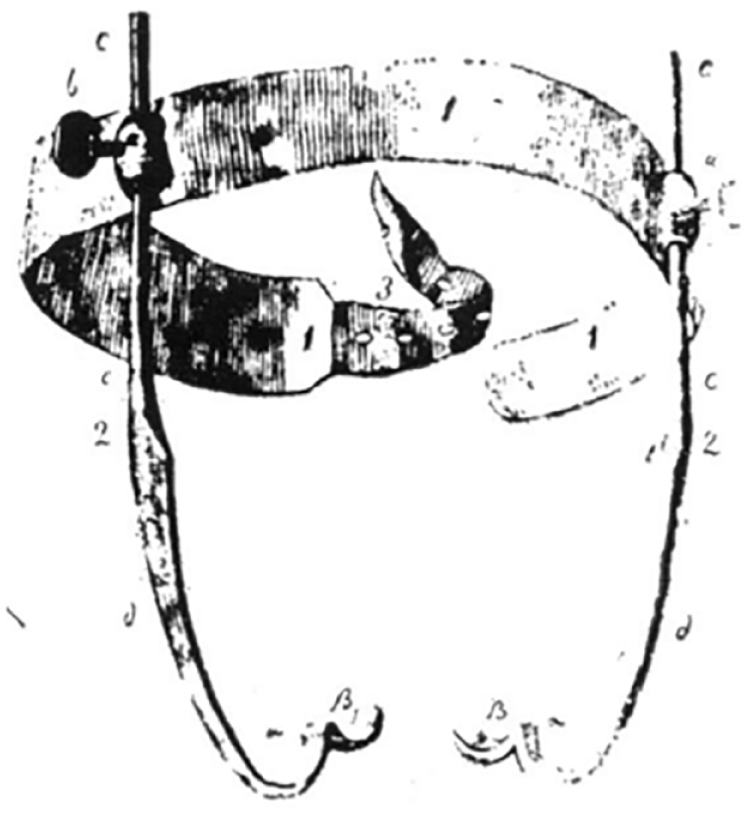
Von Graefe’scranio-maxillary suspension apparatus. GRAEFE, C. F. (1823) J. der Chir. u. Augenheilk. IV, 583-593.
First and Second World War
The First Word War (1914-1918)
Amid the First World War, the stationary trench combat and high-speed projectiles resulted in a notable number of injuries to the maxillofacial region. Major Gillies established a special center for these injuries, promoting cooperation between plastic surgeons, anesthetists, and dental surgeons. This period saw advancements in dental treatment by Captain Kelsey Fry and the invention of endotracheal anesthesia by Major Magill. X-rays were discovered by Roentgen which assisted the surgeons in aligning bone fragments. The introduction of skin grafting intraorally and the identification of the tube pedicle by Gillies 19 in 1917 marked the initiation of facial reconstruction. Despite this, during that period, jaw splints were fashioned as single units, and the fragments were adjusted within the splint during the reduction process. 20
The intervening years
During the interwar period between the 2 World Wars, notable progress was scarce. Notable exceptions included the introduction of the temporal approach for treating depressed zygomatic bones and the innovation of interdental eyelet wiring.
The Second World War (1939-1945)
The Second World War marked a turning point for maxillofacial surgery, with the establishment of maxillofacial units at home and in the military and the specialties of plastic surgery, anesthesia, and dental surgery would have to co-operate with the neurosurgeon and the ophthalmic surgeon. Significant progress occurred in both intra-oral and extra-oral fixation methods, bolstered by advancements in dental laboratory technology. The introduction of the locking plate technique by Kelsey Fry, Shepherd, McLeod, and Parfitt enabled personalized fitting and precise alignment of jaw fragments, ensuring the seamless continuity of the jaw structure. Other techniques, such as extra-oral pin fixation and the Brenthurst clamp, were also developed. In 1942, Adams 21 brought forth the idea of internal skeletal fixation by employing subcutaneous suspension wires threaded through perforations drilled in either the zygomatic process of the frontal bone, the inferior orbital rim, or the zygomatic bone. This method was aimed at providing support to either the maxilla or the mandible.
Development of fixation
The AO-ASIF guidelines underscore the fundamental principles of rigid fixation, encompassing actions such as reducing bony segments, stable fixation, immobilization, safeguarding blood supply, and encouraging early functionality. 22 Titanium hardware remains the prevailing choice, featuring a variety of plate and screw sizes and shapes that cater to surgeons’ requirements. In scenarios where surgical exposure might jeopardize blood supply or in cases of contaminated wounds, temporary use of skeletal pin external fixation might be employed. 23 Before the advent of contemporary internal fixation techniques, maxillomandibular fixation (MMF) or interdental fixation was extensively employed. MMF compresses fractures at the alveolus, yet there might still be a gap along the inferior border of the mandible. MMF contributes to achieving anatomically favorable configurations. Diverse hardware designs and techniques are accessible for MMF, including arch bars, ivy loops, and MMF screws. Utilizing arch bars for MMF provides the added advantage of creating a tension band at the alveolar component of maxillomandibular fractures, aiding in withstanding tensile forces near the teeth.
Rigid versus functionally stable fixation
The concept of rigid versus functionally stable fixation was explored, with rigid fixation aiming to prevent interfragmentary movement between fracture segments. Non-rigid fixation techniques, such as the one given by Champy for mandibular angle fractures, allow for controlled interfragmentary motion during healing.
At a histologic level, when rigid internal fixation is employed with a minimum gap between bone segments, it offers the advantage of facilitating primary bone healing through haversian remodeling. In this process, osteoclasts cross the fracture gap, followed by angiogenesis and the deposition of osteoid by nearby osteoblasts. Over time, the bone undergoes remodeling, resulting in the development of mature haversian bone. The situation is different for fractures that have a significant gap or interfragmentary movement between the fragments, as they heal through secondary intention with the formation of an intermediate hematoma and bone callus.
In 1978, Champy explained the application of a single miniplate adapted to the superior border of fractures occurring at the angle of the mandible. This approach has been referred to as “functionally stable” since it permits mandibular movement during the healing process, even when there is movement between the fractured segments. 24
Compression plate osteosynthesis
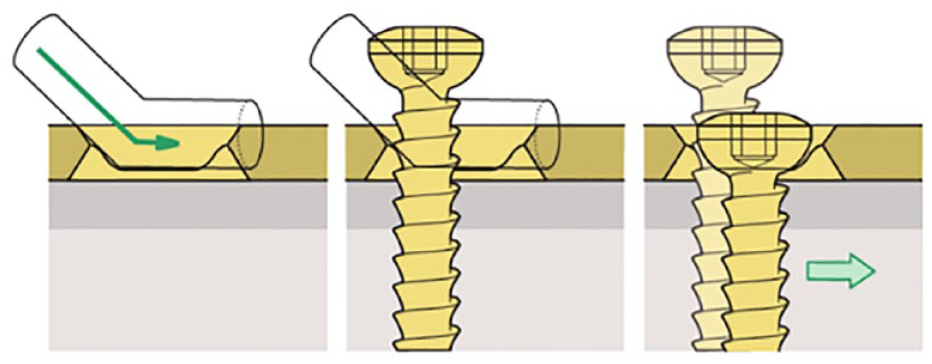
Compression plating techniques have found extensive application in maxillofacial surgery for managing fractures of the mandible. The primary objective of compression osteosynthesis, as outlined by AO, is to attain complete stability along the fracture site, thereby minimizing motion. This fosters an optimal setting for direct bone healing by generating friction among compressed bone segments and decreasing the gap between them. 25 Dynamic compression plates (DCPs) are specifically designed with eccentric holes and inclined planes, generating interfragmental pressure through the “spherical gliding principle.” (Figure 2) The horizontal movement of screws in the plate holes approximates the fracture surfaces and creates interfragmental pressure, promoting compression. However, compressive plating techniques, including DCPs, require precise technique and are prone to operator error.
Spherical gliding principle (AO). Principles of Internal Fixation of the Craniomaxillofacial Skeleton Trauma and Orthognathic Surgery (Michael Ehrenfeld | Paul N Manson | Joachim Prein).
Noncompressionosteosynthesis
Noncompressionosteosynthesis techniques, such as non-compression bone plates and reconstruction plates with locking mechanisms, offer wider uses and little room for error compared to compression osteosynthesis.
Miniplates
Mini plates are commonly used in mandible fracture fixation, with the Champy method being the most important application. Monocortical fixation is preferred, but bicortical fixation also has its applications. These miniature plates are compatible with the identical screws used in conventional mandibular fracture plates and frequently belong to the category of locking plates. However, they are thinner and more malleable compared to traditional plates. The Champy method involves placing a mini plate at the zone of tension, specifically the superior border, after reducing the fracture. Care must be taken to avoid damaging dental structures. There may be events of screws becoming loose and infectious complications concerning these miniplates due to their reduced stability and strength in comparison with the thicker hardware.
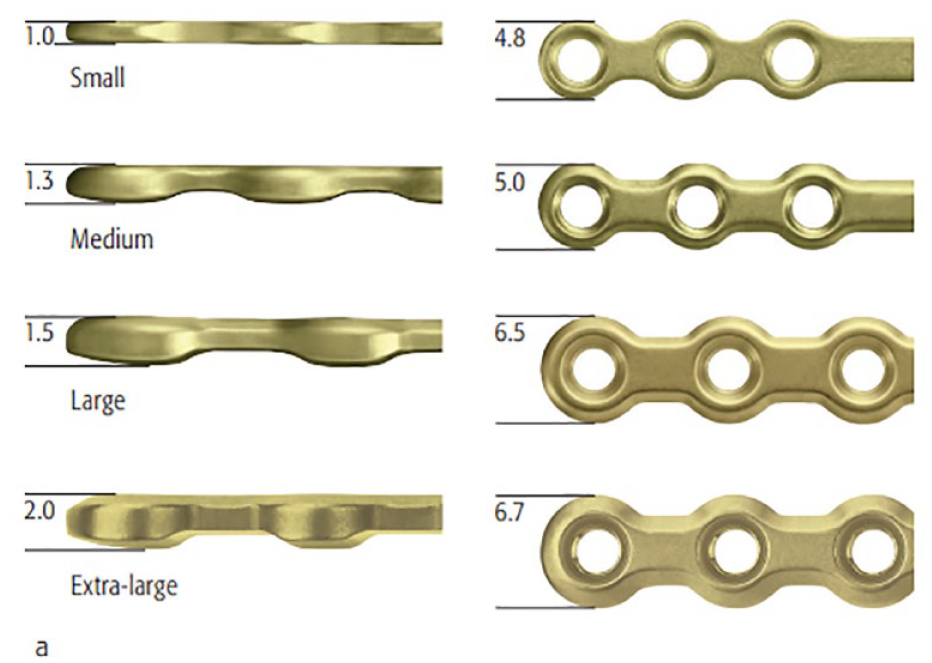
There are different types of mini plates available for mandibular and midfacial fixation. 2 mm system mandibular mini plates are utilized in the mandible (Figure 3), and their appropriate use is crucial for adequate stability. Midfacial mini plates are available in various shapes and sizes with different screw options. Microplates are even smaller in size to minimize visibility and palpability but still offer strength. The selection of screws depends on their size, head design, and self-tapping characteristics.
Mandibular plates. a. 2.0 Compact Lock Plates (AO). Principles of Internal Fixation of the Craniomaxillofacial Skeleton Trauma and Orthognathic Surgery (Michael Ehrenfeld | Paul N Manson | Joachim Prein).
Mandibular reconstruction plates are longer and stronger plates used for bridging defective areas of the mandible. These load-bearing plates require at least 3 or 4 screws on each side of the area of defect. Reconstruction plates for mandible are available in different shapes and sizes, with most using 2.7 mm screws. Some plates allow for compression or neutral screw placement.
Bioabsorbable plate fixation
The use of titanium implants in surgery poses challenges such as biocompatibility and susceptibility to infection. Metal implants do not undergo remodeling like surrounding bone and can lead to the formation of a fibrous envelope that hampers immune cell migration and clearance of bacterial contamination. Bioabsorbable fixation devices have emerged as a solution, eliminating the need for the hardware to be removed and decreasing the complications of prolonged retention. These implants have been extensively studied in pediatric craniofacial surgery and show advantages in preventing plate migration and restricting bone growth. The most common bioabsorbable materials are variations of polylactic acid and polyglycolic acid polymers, with variations in resorption rates and handling characteristics. While bioabsorbable hardware is not as strong as titanium, 25 it has demonstrated comparable outcomes in terms of rates of infection, bone union, and other complications. Proper case selection is crucial for successful outcomes. Resorbable materials have lower tensile strength compared to metallic systems, which affects their handling during implantation. The manufacturing and sterilization processes can also affect stability.
Lag Screws (Brons and Boering in 1970)
Lag screw osteosynthesis is an effective technique for fracture compression, allowing for stable fixation without the need for plate bending or multiple screws. This technique is commonly used for mandibular fractures and provides excellent stability and minimal complications 26 when performed correctly. In contrast to plate osteosynthesis, lag screw osteosynthesis involves directly passing through the fracture line, evenly distributing compressive forces, and minimizing lingual displacement.
Recent advancements in maxillofacial fixation
Recent advancements in maxillofacial fixation have improved techniques for managing complex fractures resulting from high-velocity trauma. These advancements include enhancements in fracture fixation and reduction techniques, as well as the application of other surgical developments to trauma management. Instances of these advancements encompass enhanced diagnostic imaging, minimally invasive surgical approaches, endoscopic procedures, progress in biomaterials, real-time imaging during surgery, rapid prototyping techniques, computer-guided surgery, and customized implants.
Intermaxillary fixation screws
An enhancement involves the utilization of intermaxillary fixation screws that incorporate a gap beneath the screw head for wire passage. These screws are positioned above the root tips in both the maxilla and mandible, and wires are threaded through these openings to bring the mouth into occlusion. 27 These screws serve as temporary fixation tools that can be taken out either during the operation or at a subsequent time. They offer swift placement, promote improved oral hygiene, and present a reduced risk of injury compared to the use of arch bars and wires for fixation (Figure 4)

Intermaxillary fixation with the help of screws. Textbook of Oral and Maxillofacial Surgery Fourth edition (Neelima Anil Malik).
Rapid intermaxillary fixation
Rapid IMF 28 is a flexible plastic band with adjustable properties that encircles a tooth, establishing a point of anchorage for temporary maxillomandibular fixation and immobilization. This technique reduces the possibility of needle-stick injuries and can uphold intermaxillary fixation for 3 weeks.
SonicWeld treatment
The SonicWeld Rx system is an advancement that utilizes ultrasound vibration to insert a completely resorbable SonicPin into a predrilled hole. 29 The SonicPin welds to the resorbable plate, creating a three-dimensional stable construct. This system offers quick implant insertion with minimal risk of stripping or shearing compared to screw fixation. The SonicPin is made of the same material as PDLLA implants and safely degrades through hydrolysis and the metabolic process.
Self-drilling, self-tapping screws
Self-drilling, self-tapping screws provide an advantage by eliminating the need to drill a hole, thus reducing the osteosynthesis process and involving the use of fewer instruments. These screws exhibit similar pull-out strength to conventional self-tapping screws in the bone which is thin and has superior retentiveness in cancellous bone due to their compressive action. Its use may be limited in dense bone like mandible. 30
Locking plates and screw system
Locking plates and screws offer a mini internal fixator by locking the screw to the bone as well as to the bone plate. This provides additional stability and avoids cortical necrosis that can occur with compressive plates.
3D plates
3D plates provide tridimensional stability and can be inserted through intraoral techniques. They have shown low complication rates and offer an alternative to traditional plates that depend on plate thickness for stability.
Trapezoidal condylar plates
Trapezoidal condylar plates fulfill biomechanical requirements for stable osteosynthesis in the condylar region. These plates provide superior stability compared to single-plating techniques and rectangular plates in the sagittal plane.
Delta plate fixation for condylar fractures
The fixation system known as the delta plate is specifically tailored for condylar fractures. Its distinctive delta configuration is capable of accommodating varying loads and can be conveniently positioned within the limited area of the condylar neck. Utilizing an endoscopic-assisted transoral approach, fracture realignment, and stabilization can be achieved with the delta-shaped miniplate, circumventing noticeable scars on the face and neck. These plates are made from pure titanium, measuring 1.3 mm in thickness, and are secured using 2.0 mm TriLock titanium screws 31 (see Figure 5).
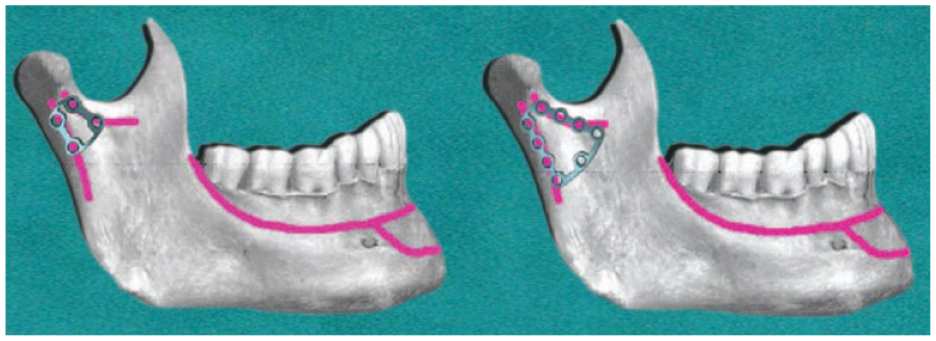
Delta plate for fixation of condylar fracture. Textbook of Oral and Maxillofacial Surgery Fourth edition (Neelima Anil Malik).
Porous polyethylene implants
Porous polyethylene implants, such as MEDPOR, have become popular for facial augmentation, contour deformities correction, orbital floor repair, and enophthalmos correction. 32 These implants allow for fibrovascular ingrowth, reducing the chances of extrusion and rejection.
The evolution of fixation systems has seen advancements in dynamic compression plates, lag screws, bio-absorbable plates, mini plates, and locking plates. Each type offers specific advantages and disadvantages in terms of compression, cost, strength, and incidence of inflammatory complications.
Biomechanical principles of fixation
Biomechanical principles play a crucial role in the development of fixation systems. Understanding masticatory stress distribution in the mandible is essential for designing and positioning osteosynthesis plates effectively. Considerations include re-establishment of occlusion, anatomical reduction, stable fixation, and maintenance of blood supply.
Future of fixation in maxillofacial surgery
The twentieth century witnessed rapid discoveries and global dissemination of knowledge. In the field of maxillofacial surgery, advancements in histology/anatomy and biology/physiology have laid the foundation for significant changes. Technological progress, such as computer-based surgical navigation 33 and 3D printing, has revolutionized surgical practices and paved the way for robotic surgery. Engineering-assisted tissue repair has also made great strides, enabling the development of biomaterials and dental implants. Non-IMF reduction procedures and endoscopic techniques offer alternative approaches to mandibular fracture therapy and facial fracture treatment, respectively, with potential benefits such as faster healing and reduced scarring. Biodegradable metals, particularly Mg-, Zn-, and Fe-based materials, have diverse applications in oral and maxillofacial regions, promoting tissue regeneration. 34 Future research goals include exploring the mechanical properties of biodegradable plates and screws, investigating degradation mechanisms, developing new materials like bone glues and staplers, and evaluating rapid fixation procedures, require minimal equipment, and have low morbidity and cost-effectiveness.
Future
Virtual reality (VR) and augmented reality (AR) technologies are promising tools in maxillofacial surgery, offering enhanced precision and safety. Mixed reality (MR) allows for the replacement of physical cutting guides with projected guidance lines directly onto the patient’s anatomy, aiding surgeons in real-time visualization of patient-specific cutting lines and interactive feedback. Recent studies demonstrate MR’s potential in various craniomaxillofacial surgeries. In contrast, AR overlays MRI or CT data onto the patient’s body during surgery, providing detailed insights into internal structures, which can help with precise incisions and visualizing critical anatomical features. 35 Ackermann et al introduced an AR application utilizing Microsoft HoloLens to aid pelvic osteotomy and fragment reorientation, enhancing visualization of the osteotomy cutting planes with marker-equipped mounts. 36 While AR and MR offer substantial benefits, they also face limitations, including tracking issues and hardware challenges. Further research is required to refine these technologies and overcome their associated limitations.
Artificial intelligence (AI) is the ability of intelligent machines to predict unknown variables by using algorithms and internal statistical patterns and information structures.
The working areas of AI in maxillofacial and plastic surgery are wide and in the fields of rhinoplasty, orthognathic surgery, cleft lip and palate, augmentation in implants, and diagnosis and determination of survival rate in cancer patients.
Data-driven algorithms can be built by machines, and thus, they can solve prediction problems without human intervention. Several AI applications in maxillofacial surgery utilize digital imaging, 3D photography, intraoral scans, and 3D photographs to predict results and plan surgeries, for example, after skeletal trauma.37-39
Future Materials That Can be Used for Maxillofacial Surgery
Magnesium-based materials are gaining attention in maxillofacial surgery as a promising alternative to traditional titanium plates and screws due to their comparable physical properties. These materials address the limitations of synthetic polymeric plates, offering resorbable options and enhanced biocompatibility. Research, including animal studies, has been actively conducted to assess magnesium’s suitability in osteofixation for facial fractures. Studies explore corrosion resistance and potential surface modifications to improve biocompatibility. Notable experiments with hydroxyapatite-coated magnesium plates and promising results in beagle dog cases highlight the potential benefits of magnesium-based solutions. While magnesium-based headless screws applied to the fractures of the condylar head in human cases exhibit excellent biocompatibility and comparable results to titanium, 40 further clinical studies are needed to assess their viability for broader use in maxillofacial surgery.
Conclusion
In conclusion, this narrative review provides a comprehensive overview of the historical development of fracture treatment in maxillofacial surgery. From ancient civilizations to the modern era, various techniques and approaches have been utilized to improve patient outcomes and restore normal function. The understanding of bone healing, advancements in reduction and internal fixation techniques, and interdisciplinary collaboration have significantly contributed to the progress in craniofacial fracture treatment. Overall, the article provides an overview of the historical advancements in maxillofacial fixation systems and highlights the current approaches used in the 21st century. By reflecting on the past, we can better appreciate the advancements made and pave the way for future innovations in fracture care. The further advancement of polymer-based materials should prioritize enhancements in their mechanical strength, minimization of foreign-body responses, the ability to regulate the rate at which they are absorbed by the body, and improved ease of use in procedures like plate bending and self-tapping.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
Institutional Review Board approval was not required.