
Abstract
Background:
Patients with cleft lip often have a secondary cleft-lip deformity (SCLD), resulting from the initial repair procedure for their congenital cleft. Patients with SCLD often undergo multiple surgeries to achieve symmetry of the lip and nose. However, little is known about how patients perceive their deformity, and if those deformities are noticeable to their peers. The purpose of this study is to use eye-tracking to evaluate how patients with cleft lip repair look at themselves and evaluate how this perception changes when the same photo is perceived by 2 different cohorts: patients who have undergone cleft-lip surgeries and control subjects who have no craniofacial pathology.
Methods:
Participants were divided into 4 cohorts: adolescents with SCLD viewing images of themselves (Cohort 1), adolescents with SCLD viewing images of peers with SCLD (Cohort 2), adolescents without SCLD viewing images of peers with SCLD (Cohort 3), and healthy adolescents without SCLD viewing images of themselves (Cohort 4). Surveys were conducted after the eye-tracking portion to determine correlations between objective gaze data and subjective opinions.
Results:
Total fixation duration was highest in the eye region for all 3 cohorts, followed by the upper lip region. Cohort 2 fixated the longest on all areas of pathology, while Cohort 1 fixated the least on all areas of pathology. Cohort 4 spent significantly more time looking at the nose bridge compared to Cohort 1.
Conclusions:
The results provide insight into how adolescents with SCLD are perceived by themselves and others and can help to better understand the complexities of the roles different areas of pathology play in self-perception.
Keywords
Introduction
Cleft lip can result in a range of physical deformities, including muscular defects in the lips, asymmetry in areas of pathology including the lips, nose, and nostrils, and visible scarring, known as secondary cleft lip deformities (SCLD). 1 Surgeons often aim to improve the appearance of SCLD through multiple surgical procedures. However, little is known about how patients perceive their deformities post-surgery, or if these deformities are noticeable to others.
Literature has described a myriad of psychosocial impairments in affected children that accompany the residual scar and facial asymmetry. Previous works have shown greater degrees of social isolation, low self-esteem, teasing, and bullying in affected children that lead to higher rates of anxiety and depression.2-5 While these factors can be attributed to the inherent facial deformity, the nuances between self-perception and peer-perception are not well studied. Previous studies have investigated behaviors toward media showing faces of the “self” and “others,” finding that participants typically explore their own faces differently than they explore unfamiliar faces. 6 Additionally, literature has provided evidence that self-esteem may play a role in patterns of self-perception, as patients with lower levels of self-confidence tended to avoid their own faces.7,8
Eye-tracking can be a useful tool for evaluating how individuals perceive post-operative surgical outcomes.9-11 Eye fixations have been shown to be an effective proxy for gaging interest and attention on facial areas, and tracking fixations has allowed for better understanding of how individuals react to and perceive facial anatomy. 12 To date, the most common application for eye-tracking in plastic surgery has been to assess observer gaze in subjects with cleft lip and SCLD.1,3,13,14 However, these studies do not consider how cleft lip pathology affects facial viewing patterns in different groups of individuals.
The purpose of this study was to use eye-tracking to examine the self-perception and peer-perception in adolescents with SCLD. The study aims to provide insight into how these individuals perceive their own deformities compared to how they are perceived by other individuals with SCLD and by peers without SCLD. By understanding the ways in which adolescents with SCLD analyze facial features, this research can help to shed light on the complex relationships between different areas of deformity and self-perception.
Materials and Methods
This prospective study included 4 cohorts of subjects recruited from the Fogelson Plastic Surgery and Craniofacial Center at Children’s Health Specialty Center in Dallas, Texas.
Case Selection
Four cohorts were included in this study as follows: Cohort 1 included 20 subjects between the ages of 10 and 18 who had a surgically repaired non-syndromic cleft lip (unilateral left, unilateral right, or bilateral) and did not have any preexisting ocular impairments. Cohort 2 included 20 subjects who met the same criterion as Cohort 1 and, additionally, did not participate in the Cohort 1 recruitment. Cohort 3 included 20 subjects between the ages of 10 and 18 who did not have any craniofacial pathologies and did not have any preexisting ocular impairments. Cohort 4 included 20 subjects who met the same criterion as Cohort 3 and, additionally, did not participate in the Cohort 3 recruitment. Individuals who were incapable of normal eye movements or who had confirmed affective psychiatric disorders were excluded from the study. Case selection was conducted consecutively, based on appointment schedules within the Plastic Surgery clinics. Potential research candidates were identified using the specified inclusion and exclusion criteria. Cohorts 1 and 2 consisted of subjects aged 10 to 18 with surgically repaired non-syndromic cleft lips, while Cohorts 3 and 4 comprised subjects aged 10 to 18 without craniofacial pathologies. Individuals who were incapable of normal eye movements or who had confirmed affective psychiatric disorders were excluded from the study. After their clinic visits, these candidates were approached and informed consent was obtained from all participants. IRB approval (STU-2018-025) was obtained prior to initiating any study procedures.
Procedure
Eye-tracking data acquisition and analysis were performed on a Tobii Pro system. Twenty frontal facial photographs of subjects from Cohort 1 were obtained in a studio at our clinic using a Sony Cybershot DSC-HX100 camera. Photographs were limited to the face region and uploaded to the Tobii Pro Spectrum Lab Software where it was added to a standardized presentation scheme and then displayed on the Tobii Pro Spectrum eye-tracking device screen. Each participant in Cohort 1 was instructed to view their own photographs, which were kept on the Tobii Pro Spectrum screen for 8 seconds while their eye movements were recorded via the system’s 2 built-in eye-tracking cameras. After the eye-tracking procedure was complete, the participants were asked to fill out a brief survey discussing their personal satisfaction with different areas of their face and their perception of the impacts that their residual cleft lip deformity has on their day-to-day tasks and peer interaction.
An additional 40 subjects in Cohort 2 (n = 20) and Cohort 3 (n = 20) were recruited and were instructed to view a presentation of the 20 previously compiled study images taken of Cohort 1 patients on the Tobii Pro Spectrum Eye-Tracking screen. Photographs were organized into 5 separate schemes—each a unique order of photos to prevent positional bias due to eye-fatigue. Participants were randomly shown one of the 5 schemes and between each picture, an empty black screen was displayed to allow the subject to reset their gaze. Each photo was displayed for 8 seconds with a 1-second display of a black screen in between. At the end of the presentation, the subjects were shown each picture again, one at a time, and asked a series of questions regarding their perception of each face. Survey questions included ranking the 3 most noticeable facial features and if they liked the appearance of the person’s nose and lips.
To act as a control group for Cohort 1, 20 subjects with no craniofacial pathologies were recruited (Cohort 4) and asked to look at their own images. The 20 frontal facial photographs of subjects from Cohort 4 were obtained in a studio at our clinic using the same procedure described above for Cohort 1. Similarly, eye-tracking data and surveys were collected from each participant.
Gaze Assessment and Analysis
The primary metric analyzed was total fixation duration including zero (TFD) within the Tobii Pro Lab software. The Tobii I-VT (fixation) filter was used on all exported data and areas of interest (AOIs) were manually defined within the Tobii Pro Lab software, which can be seen in Figure 1. The defined AOIs included eyes, cheeks, chin, forehead, lower lips, nares, nose bridge, nose tip, and upper lip. Of the 9 AOIs, the upper lip, nares, nose tip, nose bridge, and conglomerate nose were defined as “pathologic” areas of interest in reference to the characteristic facial areas affected in cleft lip. 1 Secondary analysis was based on the same 9 AOIs which were further subdivided bilaterally into left and right sides.

Example of separated Areas of Interests (AOI) created in the Tobii Pro Lab software. Selected AOIs include forehead, eyes, cheeks, chin, nose bridge, nose tip, nares, upper lip, and lower lip. Each AOI was broken up bilaterally into left and right sides for secondary analysis.
Survey
Upon completion of viewing the presentation, each subject was asked to fill out a survey. Correlations between survey responses and eye-tracking data were obtained.
Subjects in Cohorts 1 and 4 were asked 5-point rating scale questions assessing how they feel about their own looks (1 = not happy at all, 3 = neutral, and 5 = very happy) and how much or little they feel their facial differences affect them socially and physically (1 = not at all, 3 = neutral, 5 = very much). They were also asked to rank the top 3 facial features they were most unsatisfied with when considering their cheeks, eyes, forehead, jaw, lips, and nose. Cohorts 2 and 3 were asked to rank the top 3 most noticeable features between the cheeks, eyes, forehead, jaw, lips, and nose as well as questions using a 5-point rating scale to assess if they thought the face looked normal, if they liked the face, and if they liked the appearance of the person’s nose and lips (1 = not at all, 3 = neutral, 5 = very much).
Statistical Analysis
The metric this study utilized for analysis was total fixation duration including zero (TFD). The data from this metric was separated by individual AOIs for each cohort. The AOIs included eyes, cheeks, chin, forehead, lower lip, nares, nose bridge, nose tip, and upper lip (Figure 1). The values from the nares, nose bridge, and nose tip were combined within the Tobii Pro Lab software to be analyzed as one single AOI we notated as “nose.” Areas of pathology were defined as nose tip, nares, and upper lip.
Cohort comparisons for each area of interest were done using an analysis of variance (ANOVA) test; pairwise multiple comparisons were made with Tukey-Kramer at the 0.05 significance level. Data analysis was performed in Excel.
Secondary analysis was done to understand how the laterality of a patient’s cleft lip affects perception. Only photographs of patients with RUCLP and LUCLP were used. A label of “affected” indicates the side that is affected by the cleft lip repair. Analysis of laterality was done using Student’s t-test for paired comparisons (intra-cohort analyses), ANOVA (affected cleft side vs non-affected cleft side) followed by post hoc Tukey-Kramer tests, and repeated measures test (rANOVA) (affected cleft side vs non-affected side for each pathologic area of interest (nose tip, nares, and upper lip) both within (α < .05) and between (α < .05) cohorts. The secondary analysis did not include data from any bilateral subjects.
Results
Cohort 1 was comprised of 9 female participants and 11 male participants. Eight patients were classified as having left unilateral cleft lip and palate (LUCLP), 5 patients having right unilateral cleft lip and palate (RUCLP), and 7 having bilateral cleft lip and palate (BCLP). The mean (±standard deviation) age of the females in this cohort was 14.8 (±2.3) years and the mean age of males was 13.7 (±3.0) years. Cohort 2 was comprised of 12 female participants, with a mean age of 14.7 (±2.1) years, and 8 male participants, with an average age of 14.9 (±1.9) years. Cohort 3 was comprised of 10 female participants, with a mean age of 14.8 (±1.9) years, and 10 male participants, with a mean age of 15.1 (±2.4) years. Cohort 4 was composed of 13 female participants with a mean age of 13.7 (±2.5) years, and 7 male participants with a mean age of 13.4 (±2.9) years.
Eye-tracking data (Figure 2) showed that all cohorts fixated on the eyes, upper lip, and nose for the longest amount of time. Cohort 2 spent significantly more time (P < .01) looking at the nose (1.86 seconds) compared to Cohort 1 (0.99 second) and Cohort 3 (1.20 second) (Figure 3). Cohort 2 also spent significantly more time (P < .01) looking at the upper lip (1.55 seconds) compared to Cohort 1 (1.02 second). Cohort 3 spent significantly more time (P < .01) looking at the lower lip (0.50 second) compared to Cohort 1 (0.13 second) and Cohort 2 (0.19 second). Cohort 4 spent significantly more time (P < .01) looking at the nose bridge (0.48 second) compared to Cohort 1 (0.29 second) (Figure 4). No significant difference was observed in the eye region between the first 3 cohorts nor between Cohort 1 and 4. Similarly, no significant difference was observed in the regions of the chin and forehead. Figure 3 shows composite heat maps representing the total fixation duration on the image of the subject with RUCLP. Warmer colors indicate longer fixation times for participants in each cohort.
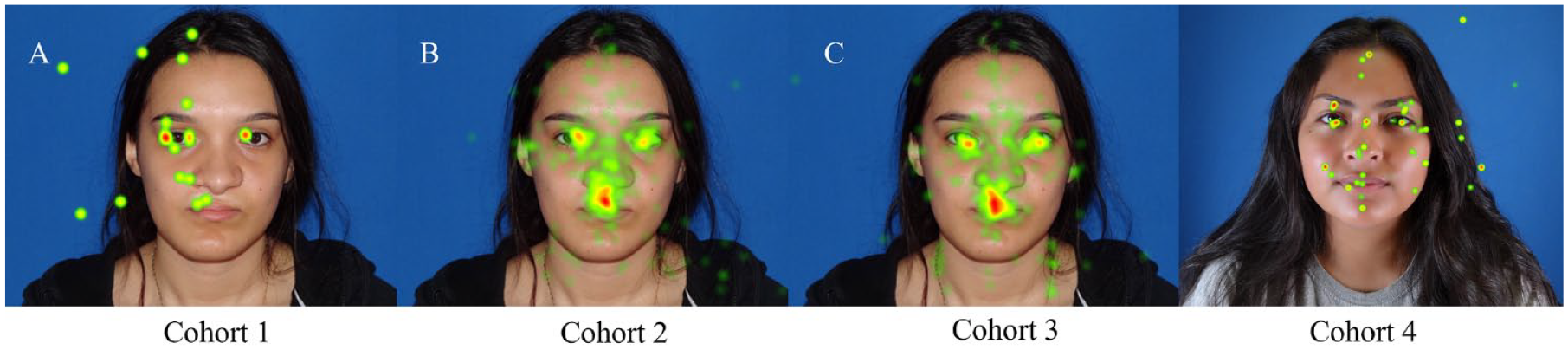
Composite heat maps representing total fixation duration on image of subject with right unilateral cleft lip and/or palate (RUCLP). Cohort 1 (A) total fixation duration of subject looking at their own image (n = 1), Cohort 2 (B) composite total fixation duration viewing Cohort 1 subject (n = 20), Cohort 3 (C) composite total fixation duration viewing Cohort 1 subject (n = 20), and Cohort 4 (D) total fixation duration of subject looking at their own image (n = 1).

Box-plot summary of primary analysis. Total fixation duration distribution of all cohorts separated by AOI. Lower and upper box boundaries represent the 25th and 75th percentiles, respectively, lines inside boxes represent means, lower and upper error lines represent 10th and 90th percentiles, respectively, and crosses represent data which fell outside the 10th and 90th percentiles.
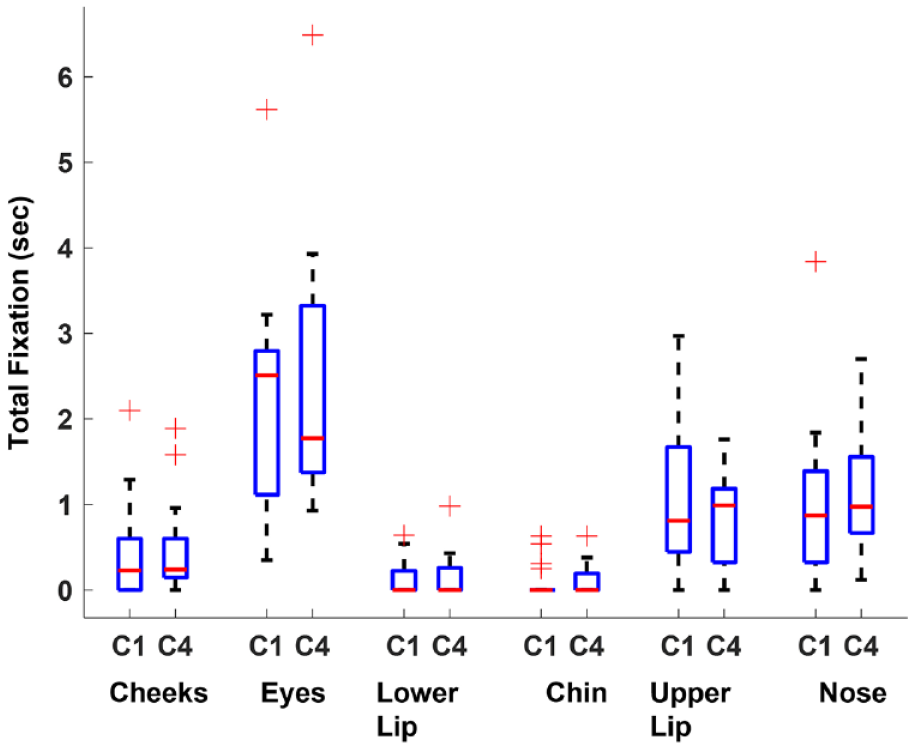
Box-plot summary of primary analysis. Total fixation duration distribution of cohorts C1 and C4 separated by AOI. Lower and upper box boundaries represent the 25th and 75th percentiles, respectively, lines inside boxes represent means, lower and upper error lines represent 10th and 90th percentiles, respectively, and crosses represent data which fell outside the 10th and 90th percentiles.
Analysis of laterality shows that Cohort 2 spent significantly more time looking at the affected upper lip (1.036 second) compared to Cohort 1 (0.307 second and 0.487 second, respectively). Although Cohort 3 (0.164 second) fixated on the normal nares for a longer duration than Cohort 1 (0.090 second), this difference was not significant upon post hoc Tukey-Kramer analysis. Analysis of laterality for regions of pathology can be seen in Figure 5.
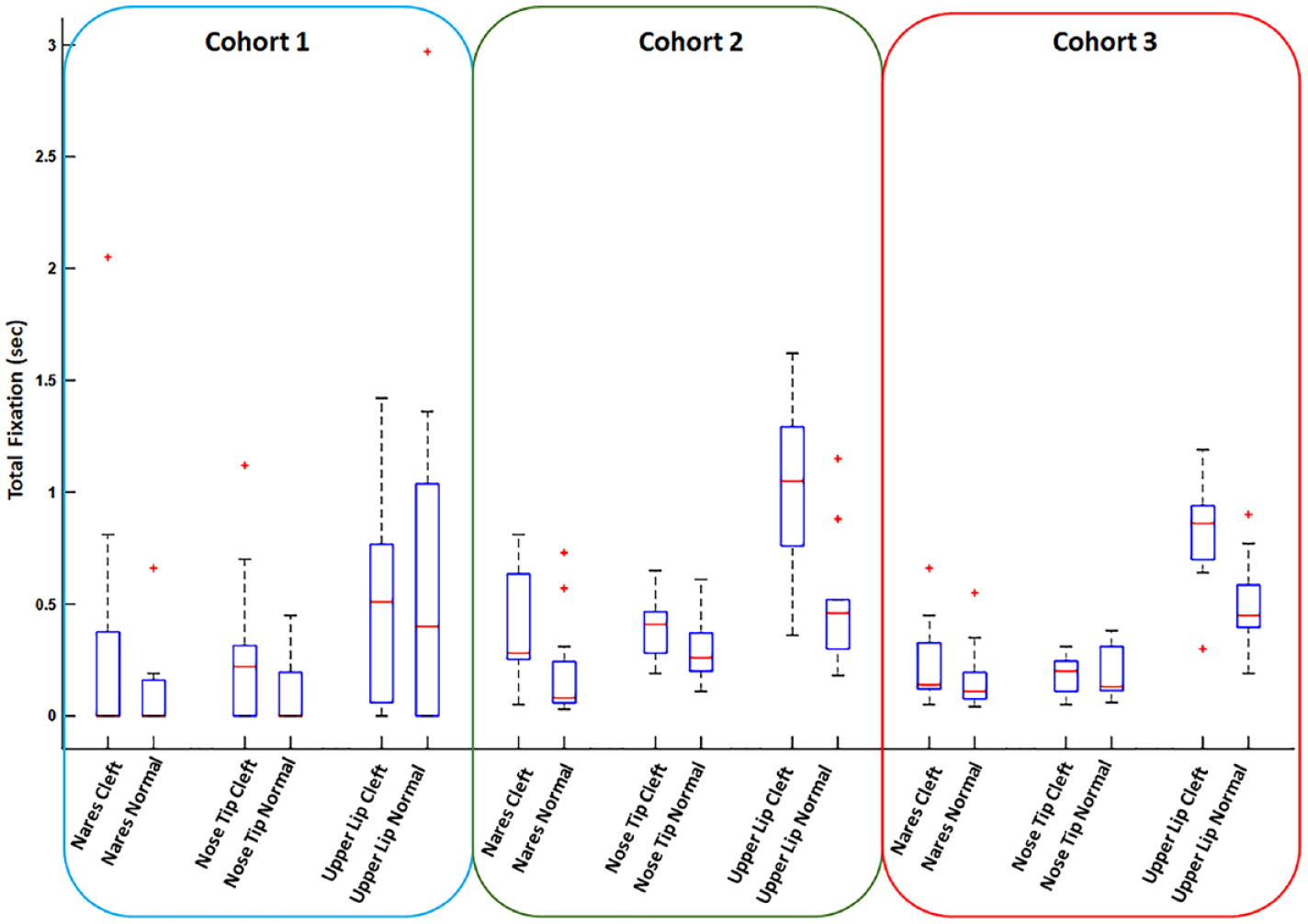
Boxplot summary of secondary analysis. Total fixation duration distribution between cohorts across laterally divided AOIs which have been defined as “pathologic.” Comparing TFD in affected versus unaffected areas. Lower and upper box boundaries represent the 25th and 75th percentiles, respectively, lines inside boxes represent means, lower and upper error lines represent 10th and 90th percentiles, respectively, and crosses represent data which fell outside the 10th and 90th percentiles.
Survey responses followed trends in fixation duration seen in the eye-tracking data. Cohort 1 and Cohort 4 both ranked the nose as the feature they were least satisfied with (40% and 40%, respectively), followed closely by the lips in Cohort 1 (35%) and the forehead in Cohort 4 (25%). Cohort 1 also indicated that socializing with their peers is “not at all” or “not very much” impacted by their facial differences (mean 1.76; based on a 5-point Likert scale). Cohort 4 answered “not very much” or “neutral” when asked if they felt their least liked features impacted how well they socialized with their peers (mean 2.42; based on a 5-point Likert scale). Cohorts 2 and 3 followed a similar pattern in ranking AOIs in terms of noticeability, ranking the nose as most noticeable (34% and 38%, respectively) and the lips as second most noticeable (29% and 35%, respectively). Survey data is summarized in Figure 6.
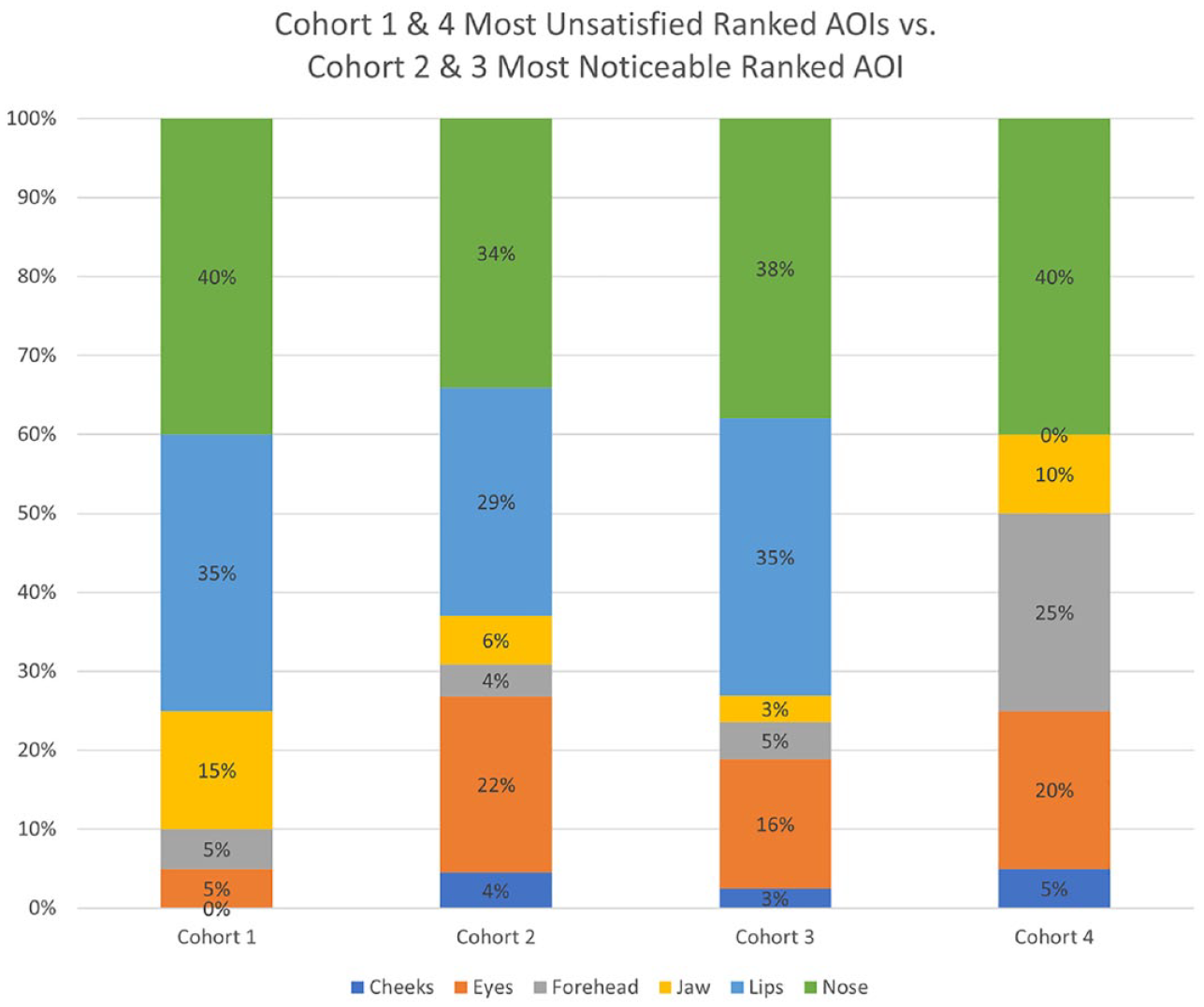
Histogram representing the percentage of times each AOI was ranked first in Cohort 1 and 4 survey question, “Please rank the top 3 facial features you are most unsatisfied with, with 1 being your least liked feature” and Cohorts 2 and 3 survey question, “Please rank the top 3 facial features that stood out to you the most, with 1 being the most noticeable.”
Discussion
In this study, we used eye-tracking as a measure of attention to investigate self-perception and peer-perception in a group of patients with SCLD. Our results showed differences in gaze patterns between the cohorts of participants. Specifically, participants in Cohort 1 tended to spend less time looking at pathological regions in their own images, while Cohorts 2 and 3 spent significantly more time looking at the upper lip and nose, respectively. This discrepancy may be due to various factors, such as avoidance or the development of coping strategies over time.15,16
Meyer-Marcotty et al noted that emotional displeasure elicited from reflecting on participants’ own CL-relevant facial features may result in aversion to their images, yielding higher fixation times in non-pathological areas such as the eyes. 17 Other literature has provided some evidence that older individuals may cope better with disfigurement than younger persons due to the sheer passage of time or from the development of coping strategies.2,18 These coping adaptations have been termed “self-presentation strategies,” which allow patients living with craniofacial differences to maintain a sense of self-acceptance against societal reactions. 2
When considering non-pathological areas, Cohort 3 spent significantly more time viewing the lower lip (0.50 second) than the other 2 cohorts. This may be due to the prior intimate knowledge of SCLD that Cohorts 1 and 2 have compared to that of Cohort 3. In previous studies, Boonipat et al found that individuals who reported a personal or family history of facial deformity fixated more on the perioral region than did laypeople, whereas Meyer-Marcotty et al reported patients with UCLP spent more time viewing the nose instead of the eyes. 17 Orthodontists have also been found to fixate more on the upper lip area when viewing images of cleft lip and palate than individuals with cleft lip and palate and laypeople. 19 These findings suggest that different groups may have different patterns of attention and focus when viewing facial deformities.
Surveys from both Cohorts 1 and 4 indicated that their least-liked features do not affect their ability to socialize with their peers. These results show a similarity in self-perception between adolescents with SCLD and those without SCLD. Previous studies showed that peer problems for females with cleft lip were within the normal range at both ages 10 and 16.20-22 Additionally, close friendships were perceived more positively by 16-year-old males with visible clefts compared to a reference group or peers with non-visible clefts. 22
We found a high degree of similarity between the areas that Cohort 1 was least satisfied with on their own faces and the areas Cohort 2 and Cohort 3 found to be most noticeable in the images. This indicates that the subjective opinions of the participants may be supported by the objective data collected through the eye-tracking protocol. Several studies have investigated the relationship between eye-tracking data and subjective rating scales, including measures of attractiveness, severity, and personality attributes. In some cases, a correlation was found between the 2,23-25 but in other studies no association was observed. 26 The inconsistencies in the findings may be due to limitations in the assessment measures used or the limitations of eye-tracking in detecting certain aspects of the evaluation.
A large variance can be seen in Cohort 1 data compared to Cohorts 2 and 3, which can be seen in Figures 1 and 2. This may be because each participant in Cohort 1 only viewed one image of themselves, while the data from Cohorts 2 and 3 included the eye-tracking data from 20 subjects for each of the 20 images. Another limitation of our study is the lack of “normal” photographs (ie, patients without any SCLD) in the presentations shown to the study participants, which may be addressed in the future by including randomly dispersed control photographs within the procedural format.
Further investigation is necessary to better understand the relationship between self-perception and peer-perception in adolescents with SCLD. This could include the examination of long-term treatment effects on these perceptions and the potential impact of coping strategies. This information could aid in the design of effective interventions for adolescents with SCLD.
Conclusions
The results showed that all cohorts fixated on the eyes, upper lip, and nose for the longest amount of time, although each cohort’s time varied. Additionally, survey responses indicated that both adolescents with SCLD and aged-matched control subjects were least satisfied with their noses, which was also ranked as the most noticeable in adolescents with SCLD by their peers. Overall, the study suggests that there are variations in how different groups of people view and perceive facial differences associated with cleft lip and palate.
Footnotes
Author’s Note
Presented at the 79th American Cleft Palate-Craniofacial Association (ACPA)
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
This study was approved and followed the guidelines set by University of Texas Southwestern Institutional Review Board (STU-2018-0250).