
Abstract
Background:
The method of epidermal closure during cleft lip repair is important to consider, as it may affect complication rates, cosmetic outcomes, and patient comfort levels. Historically, this has most commonly been performed with permanent suture that requires subsequent removal, which is not well tolerated in infants. The purpose of this study is to compare the outcomes between 2-octyl cyanoacrylate liquid with a self-adhesive polyester mesh tape (2-OPMT) and typical suture closure techniques, which to our knowledge has never previously been investigated.
Methods:
In nine consecutive cleft lip repairs, the epidermal closure was performed with permanent suture, and in the subsequent nine consecutive cleft lip repairs, the epidermal closure was performed with 2-OPMT. Complication rates were compared between the groups. Esthetic scar outcomes were investigated via post-operative photograph analysis utilizing the Manchester Scar Scale. Statistical significance was determined with Fischer Exact Tests and Wilcoxon Rank-Sum tests. Subsequently, scar scores for 30 cleft lip repairs performed with 2-OPMT in our practice were compared to previously reported scores in the literature for 30 cleft lip repairs performed with typical suture technique.
Results:
Three patients in the permanent suture group had documented scar-related complications and one patient in the 2-OPMT group had documented scar-related complications. No statistically significant difference was found in complication rates between the two groups. No statistically significant difference was found in esthetic scar scores between the two different closure techniques either within our practice or in comparison to reports in the literature.
Conclusions:
Overall, the use of 2-OPMT offers comparable esthetic outcomes and complication rates to the use of permanent suture in epidermal closure of cleft lip repairs.
Introduction
The skin closure technique used during primary cleft lip repair plays a crucial role in achieving a satisfactory cosmetic outcome and preventing postoperative complications, such as surgical site infection, wound dehiscence, and scar hypertrophy. In particular, the method of epidermal closure is important to consider, as it may affect surgical outcomes, cost, and patient comfort.
Historically, permanent sutures have been employed for epidermal closure in cleft lip repairs. These sutures, usually made of non-absorbable synthetic materials, provide mechanical strength to the wound edges during the initial healing phase. They are typically removed 5 to 7 days later, reducing the chance that chronic inflammation at the suture site will affect the scar. Their utilization in the infant population presents unique challenges, primarily related to the need for subsequent suture removal. This can be both distressing for the infant and their caregivers as well as costly, as it usually requires sedation. 1
In recent years, efforts have been made to explore alternative methods for epidermal closure in cleft lip repairs, aiming to overcome the drawbacks associated with permanent sutures. One such alternative is the use of dermal glue, a liquid adhesive composed of 2-octyl cyanoacrylate. Dermal glue forms a flexible, waterproof, and biocompatible film that adheres to the skin surface, protecting the wound edges and holding them together. It is designed to undergo gradual biodegradation, eliminating the need for subsequent removal.
Several studies have previously investigated the efficacy, safety, and cosmetic outcomes associated with the use of dermal glue compared to permanent sutures in cleft lip repairs.2-4 These studies have examined various factors, including wound healing, infection rates, scar appearance, and patient satisfaction. Comparable results have been found between the two closure techniques, with the added benefits of a protective barrier, simplified wound care, and no need for suture removal. 3
This study investigates the use of an alternative product, a 2-octyl cyanoacrylate liquid with a polyester mesh tape (2-OPMT), for epidermal closure of primary cleft lip repair. This glue/mesh combination offers several distinct benefits compared to traditional dermal glue for skin closure. Firstly, utilizing 2-OPMT combines the adhesive properties of 2-octyl cyanoacrylate with a self-adherent, non-absorbable mesh backing. This mesh backing provides added mechanical support to the wound edges, promoting enhanced wound stability and reducing tension on the closure site. 5 Additionally, 2-OPMT demonstrates a longer-lasting effect compared to dermal glue alone due to its enhanced structural integrity and durability, simplifying postoperative wound care.
To our knowledge, no previous study has investigated the outcomes of 2-OPMT for cleft lip repair closure. The purpose of this study is to compare the safety as well as the esthetic results between 2-OPMT and typical permanent suture techniques for epidermal closure in primary cleft lip repair. By doing so, this research aims to contribute to the ongoing discussion surrounding optimal epidermal closure methods in cleft lip repair and ultimately improve outcomes for infants undergoing this surgical intervention.
Methods
This was a two-part retrospective study that reviewed the surgical outcomes of patients in the senior author’s practice who underwent primary cleft lip repair using either the permanent suture technique or the 2-OPMT technique. Patient records were retrospectively reviewed to collect relevant information for analysis. Demographic characteristics, such as age and gender, were recorded for each patient. Surgical variables, including the cleft type and surgical technique were also documented. In addition, data regarding postoperative complications and scar appearance were collected from follow-up records.
The first part of the study reviewed the medical records of 18 consecutive patients who underwent primary cleft lip repair during the timeframe in our practice when the epidermal closure technique was changed to eliminate the need for subsequent suture removal under sedation. In the first 9 consecutive patients the epidermal closure was performed with permanent suture, and in the subsequent 9 consecutive patients the epidermal closure was performed with 2-OPMT. These patients represent the last 9 patients in the senior author’s practice to undergo closure with permanent suture and the first 9 patients in the senior author’s practice to undergo closure with 2-OPMT. In the group of patients who received permanent sutures, 6-0 Prolene was used for the epidermal closure after wound edge approximation was achieved with deep dermal sutures in a Millard technique cleft lip repair. In the group of patients who received 2-OPMT, the adhesive mesh was applied after wound edge approximation was achieved with deep dermal sutures in a Millard technique cleft lip repair. The application technique was standardized across all patients in this group (Figure 1).
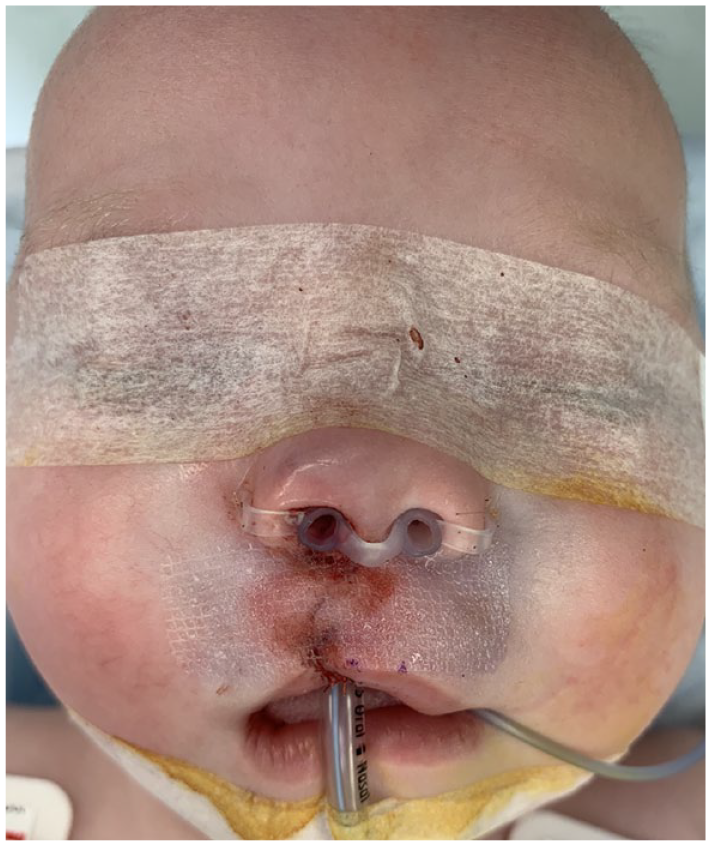
Intraoperative cleft lip closure with 2-OPMT.
Complication rates were compared between the groups, including surgical site infection, partial incisional dehiscence, scar hypertrophy, and scar widening. Partial incisional dehiscence was defined as any perceivable opening or gapping along the suture line. Scar hypertrophy was defined as thickened scars raised more than 1 mm above the level of the surrounding skin. Scar widening was defined as widening of a flat scar >1 mm. Statistical significance for rates of complication was determined with Fischer Exact Tests.
Esthetic scar outcomes were investigated via post-operative photograph analysis. A panel of four board-certified plastic surgeons was assembled from the faculty at Virginia Tech Carilion Section of Plastic Surgery. These surgeons were not involved in any parts of the patients’ care. The surgeon panel was invited to objectively and independently review photographs of the patients and grade the appearance of the cleft lip scars utilizing the Manchester Scar Scale (MSS), a validated scoring system that quantitatively assesses scar characteristics including color, contour, and finish (Figure 2). For the purpose of this study, the MSS was modified to exclude the category of scar texture, as texture is difficult to accurately evaluate in photographs. This modification is supported in the existing cleft literature. 6
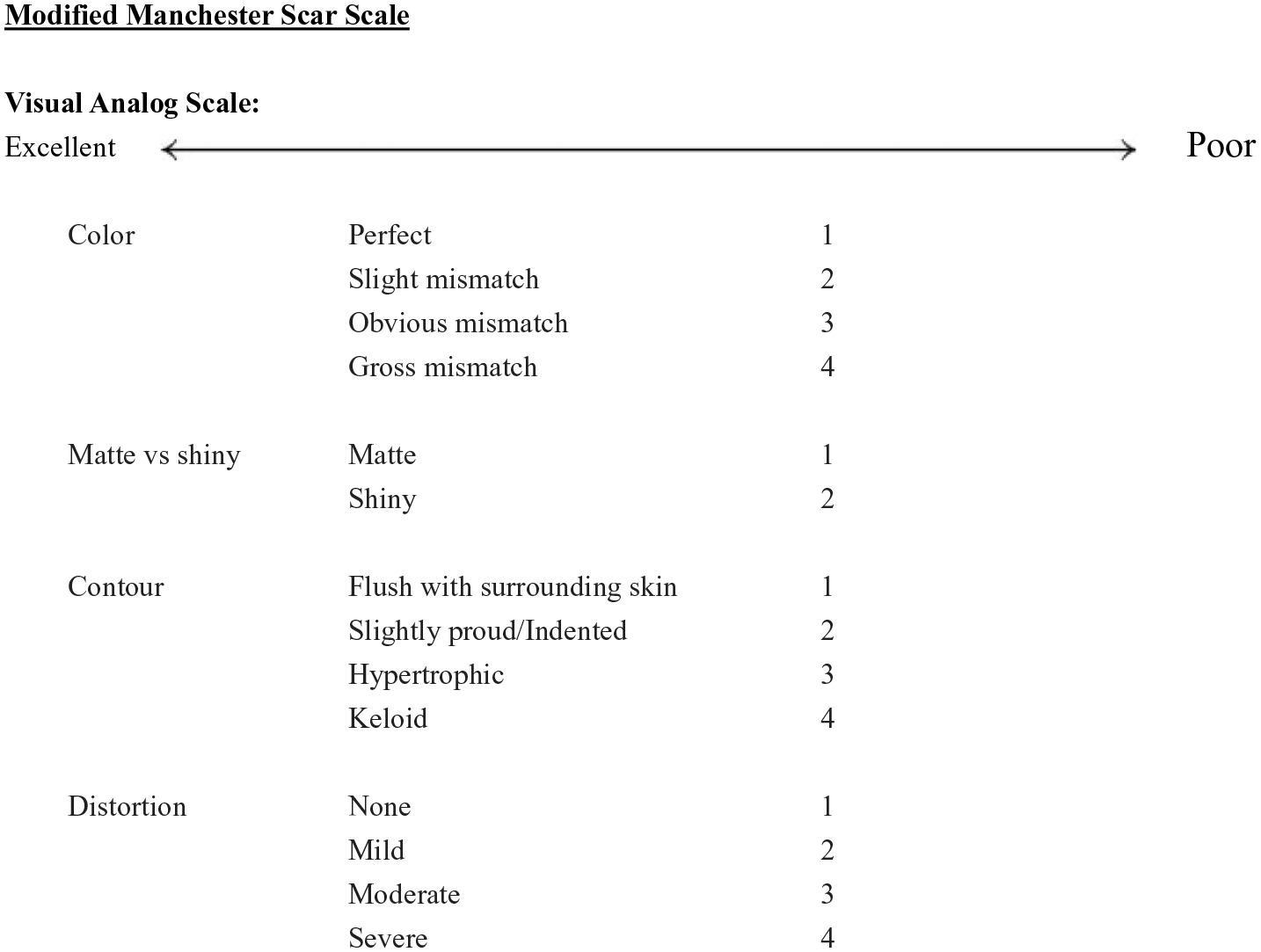
Modified Manchester Scar Scale.
All photographs were taken as part of the patients’ standard postoperative care. The photographs from the patients’ last postoperative visit were selected, which on average took place approximately three years following cleft lip repair. All photographs selected for surgeon panel review were masked to conceal patient identity. Statistical significance was determined with Wilcoxon Rank-Sum tests (Figure 3).
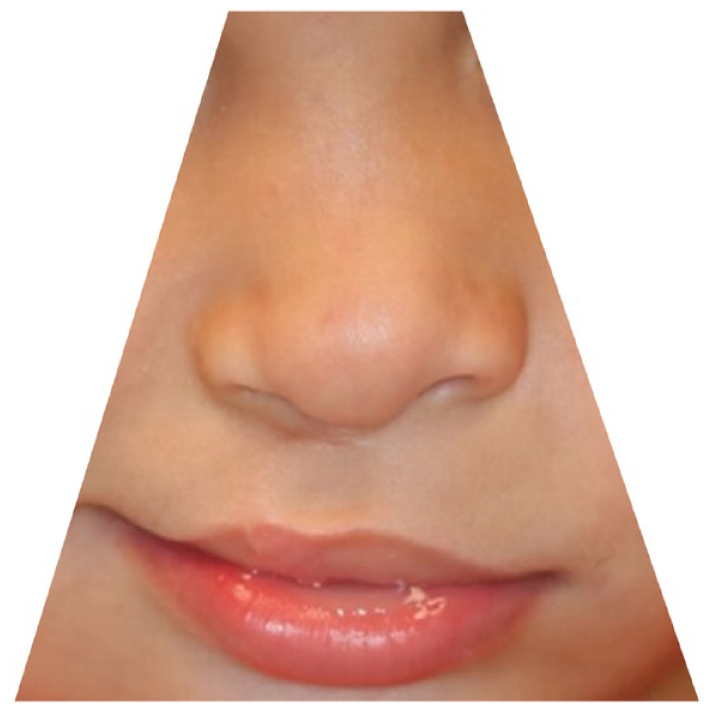
Example of masked post-operative photographs graded by the panel of plastic surgeons.
The second part of the study reviewed the records of 30 consecutive patients who underwent primary cleft lip repair epidermal closure with 2-OPMT. These patients represent the first 30 patients to undergo this treatment method in the senior author’s practice. The esthetic scar outcomes were evaluated by the same panel of board-certified plastic surgeons assembled for the first part of the study. The panel similarly reviewed post-operative photographs and graded the appearance of the cleft lip scars utilizing the modified Manchester Scar Scale. These scores were then compared to previously reported scores in the literature. A study by Ramly et al. was selected for comparison. 6 This study utilized an identical modified Manchester Scar Scale to evaluate the esthetic outcomes of 30 cleft lip repairs performed utilizing a Millard technique with permanent sutures for the epidermal closure. The average total scar score and standard deviation from this study were compared to the average total scar score and standard deviation from our patient series. Statistical significance was determined with two-sample t-tests.
Results
Part 1
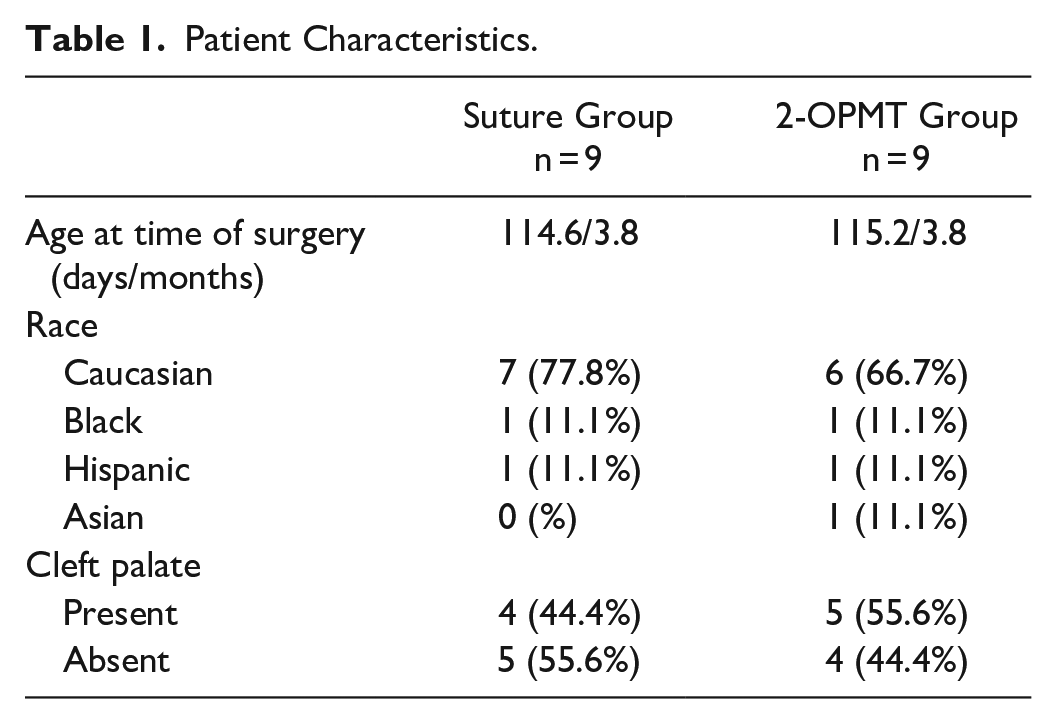
Medical records were reviewed for 9 consecutive patients who underwent cleft lip epidermal closure with permanent suture and 9 consecutive patients who underwent cleft lip epidermal closure with 2-OPMT (Table 1).
Patient Characteristics.
Three patients in the permanent suture group had documented scar-related complications, including one instance of partial incisional dehiscence, two instances of scar hypertrophy, and one instance of scar widening. One patient in the 2-OPMT group had documented scar-related complications, including both partial incisional dehiscence and scar hypertrophy. There were no reports of surgical site infection in either group. No statistically significant difference was found in complication rates between the two groups (Table 2).
Complication Rates of the Permanent Suture Group Compared to the 2-OPMT Group.

Post-operative photographs that underwent review were taken an average of 3.1 years after the cleft lip repair. One patient in the permanent suture group was lost to follow up and subsequently did not have post-operative photographs available for review. The average modified MSS for patients in the permanent suture group was 10.6 and the average modified MSS for patients in the 2-OPMT group was 8.5 (with lower scores demonstrating a better cosmetic result). No statistically significant difference was found in esthetic scar scores between the two groups (Table 3).
Manchester Scar Score Results for Part 1 of the Study, A Comparison of the Senior Author’s Permanent Suture Group Compared to the Senior Author’s 2-OPMT Group.

Part 2
Medical records were reviewed for 30 consecutive patients who underwent cleft lip epidermal closure with 2-OPMT. Post-operative photographs that underwent review were taken an average of 2.3 years after cleft lip repair. The average modified MSS as determined by the surgeon panel was 6.48 + 1.63 SD. This was compared to previously reported data from Ramly et al., in which the average modified MSS for patients who underwent a Millard technique cleft lip repair with permanent suture epidermal closures was 6.77 + 1.18 SD. 6 No statistically significant difference was found in esthetic scar scores between the 2-OPMT epidermal closures in our practice and the permanent suture epidermal closures reported in the Ramly et al. study (Table 4).
Manchester Scar Score Results for Part 2 of the study, A Comparison of the Ramly et al. Permanent Suture Group Compared to the Senior Author’s 2-OPMT Group.
Cost analysis was also performed to evaluate the difference between the 2-OPMT group and the permanent suture group with a second sedation procedure. The charge for the 2-OPMT product used at our hospital is $485, compared to the average charge of returning to the OR for a 15-minute suture removal procedure of $15 374.
Conclusion
This study demonstrated no statistically significant difference observed in the complication rates or esthetic outcomes between epidermal closure using permanent sutures and epidermal closure using 2-OPMT in primary cleft lip repair. These results suggest that both techniques can be considered safe and effective methods for achieving satisfactory wound closure in cleft lip repairs. The choice between permanent sutures and 2-OPMT may be influenced by factors such as surgeon preference, patient characteristics, and resource availability. Further prospective studies with larger sample sizes are warranted to validate these findings.
Discussion
The method of epidermal closure in the repair of the cleft lip usually involves either a permanent suture which must be subsequently removed, or some version of dermal glue and/or resorbable sutures to avoid the removal procedure. Due to the delicate nature of the lip skin as well as its functional and esthetic importance, surgeons desire to produce the most pleasing scar possible. In this study we sought to determine in an objective fashion whether the change to epidermal closure with a dermal mesh/glue combination affected subsequent scar formation.
We chose to use the Manchester Scar Scale as it is a well-established and validated scoring system used to evaluate scar characteristics, including color, contour, texture, and overall appearance. The MSS was first described by Beausang et al. in 1998 for assessment of surgical scars. 7 The scale consists of 5 items, each scored on a scale of either 1 to 2 or 1 to 4, with higher scores indicating worse scar characteristics, as well as a visual analog scale (VAS) that is scored from 0 to 10. The scores from each category and the VAS score are then added together to give a final scar score, with a minimum (best) possible score of 5 and a maximum (worst) possible score of 24. Its utilization provides a standardized and objective method for quantifying scar quality. Previous studies have demonstrated satisfactory interrater reliability for the Manchester Scar Scale, indicating that it can be reliably used across different raters, enhancing the credibility and validity of scar assessment in both research and clinical settings. For the purpose of our study, we utilized a modified MSS that excluded assessment of scar texture, given the difficulty to accurately evaluate texture in a photograph. This was established as a precedent for accurate assessment of cleft lip scars in the Ramly et al. study that was used as a control group for the second part of this study. 6 The modified MSS utilized in both studies have a minimum (best) possible score of 4 and a maximum (worst) possible score of 20. This method of scar assessment specifically evaluates the scar itself (which was the goal) and not the overall esthetics of the cleft lip repair.
This study is not without limitations. Notably, this was a single surgeon retrospective investigation with relatively small sample numbers. There were only 9 patients who underwent the permanent suture technique before the change was made in our practice to the 2-OPMT technique. To overcome this limitation, we added the second portion of the study, which took advantage of a previously published series of 30 patients who had undergone a rotation/advancement cleft lip repair using permanent suture and were evaluated using the modified MSS. This allowed us to compare our first 30 patients closed with the 2-OPMT technique to previously published data. The study design was inherently susceptible to selection bias due to the nature of retrospective chart review. This study also only focused on short-term outcomes and did not explore long-term scar quality or patient-reported satisfaction. Additionally, while the Manchester Scar Scale provides a standardized tool to evaluate scores, it is important to acknowledge that scar assessment is a subjective process and may be influenced by individual interpretation and bias. This is particularly important when considering that the results of our surgeon panel were compared to the results of a different group of surgeons in the Ramly et al. study. Likewise, it is important to consider that the nuances of cleft lip repair can vary among surgeons, even when utilizing similar rotation-advancement flap techniques, which is another limiting factor of this study.
Overall, we conclude that the 2-OPMT method of epidermal closure yields similar results in subsequent scar healing compared to permanent sutures. The product used in this study anecdotally seemed to allow for better precise approximation of the epidermal edges than tissue glue alone and allowed for significant cost savings by avoiding the need for a sedated suture removal procedure.
Footnotes
Author’s Note
Presented at:
Southeastern Society of Plastic and Reconstructive Surgeons 66th Annual Scientific Meeting Mini-Symposium on Craniofacial and Cleft Surgery
June 19, 2023
Nassau, Bahamas
Southeastern Society of Plastic and Reconstructive Surgeons 66th Annual Scientific Meeting Resident Quickshot Podium Presentation
June 18, 2023
Nassau, Bahamas
Plastic Surgery the Meeting 2023
October 28, 2023
Austin, Texas
Short Running Head:
“Esthetic Outcomes of Cleft lip repair with 2-OCPM”
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
This study was approved by our Institutional Review Board (# IRB-21-1322) on May 09, 2022. This was a retrospective study. All patient information was deidentified, and the study was exempted by the IRB from obtaining informed consent.