
Abstract
Purpose:
Patients with cleft lip and/or palate (CLP) often present with Class III malocclusions resulting from maxillary deficiency. Although orthognathic surgery can correct this, it is not performed until skeletal maturity. Bone-anchored maxillary protraction (BAMP) can be used during adolescence to stimulate maxillary growth. We report the outcomes of BAMP therapy in 10 patients with CLP.
Methods:
Beginning in 2019, patients born with CLP with mild, moderate, or severe Class III malocclusion started BAMP therapy. Four Bollard miniplates were surgically placed in each patient following a standard protocol under general anesthesia. Miniplates were secured using self-tapping titanium screws. Orthodontic elastics were initiated 2 weeks after surgery with an initial loading force of 100 g bilaterally and later increased to 200 g at 12 weeks postoperatively. Before (T1) and after (T2), Cone Beam CT (CBCT) radiographs were taken and reviewed by a single examiner.
Results:
Ten patients met the inclusion criteria. Their mean age at the time of Bollard miniplate placement was 12.2 (range, 9-14) years. Before treatment, the average cephalometric measurements for the SNA, SNB, and ANB were 73.3°, 78.0°, and −4.7°, respectively. After treatment, the average cephalometric measurements for SNA, SNB, and ANB were 74.4°, 77.7°, and −3.3°, respectively.
Conclusion:
We have demonstrated positive results with BAMP therapy. BAMP therapy led to corrective orthopedic maxillary protraction and induced favorable dental and skeletal outcomes, improving overall facial balance. Cleft surgeons should consider this modality after alveolar bone grafting when treating pediatric patients with Class III malocclusions.
Keywords
Introduction
Cleft lip and/or palate (CLP) is a common congenital craniofacial deformity that often necessitates multiple corrective surgical interventions throughout an individual’s lifetime. The resultant scarring from these surgeries can adversely affect maxillary growth, resulting in a Class III malocclusion.1,2 It is estimated that 25% to 60% of patients with unilateral cleft lip and palate (UCLP) will ultimately require surgical maxillary advancement to correct malocclusion and improve facial esthetics. 3
Historically, facemask therapy (FM) has been used to stimulate forward growth of the maxilla in children with maxillary deficiencies. Although FM therapy can be initiated earlier in a patient’s life, the discontinuation of maxillary protraction before skeletal maturity places the patient at particular risk for relapse of occlusal relationships.4-6 Furthermore, FM therapy utilizes bulky intra and extraoral devices that demand frequent clinical adjustment. The inherent discomfort, costs, and social stigma associated with wearing such an appliance can hinder patient compliance. 7 Adverse effects such as maxillary incisor proclination and clockwise rotation of the mandible have also been observed.8-11
To address these issues, De Clerk et al. described Bone-anchored maxillary protraction (BAMP) therapy in the early 2000s as a novel method of stimulating maxillary protraction.12,13 The technique promotes maxillary growth through skeletally anchored miniplates connected by class III intraoral elastics. Compared to FM therapy, BAMP therapy allows for a more constant and precise application of skeletal forces to avoid undesireable dentoalveolar effects.14-16 Despite these apparent benefits, the published literature describing experiences with BAMP therapy in patients with CLP is limited to a few integral studies. 17 In this case series, we present our experience with 10 patients with CLP who underwent Bollard miniplate treatment for at least 12 months at our institution.
Materials and Methods
Patient Population
Our team began selecting patient candidates for BAMP therapy in 2019. Patients with mild, moderate, and severe Class III malocclusions were counseled on BAMP therapy in the orthodontics clinic. Between September 2019 and September 2022, 25 patients underwent BAMP therapy; Before and after radiographs were not taken for all patients.
A retrospective chart and radiographic reviews were conducted after obtaining Institutional Review Board (IRB) approval. Patients who had at least 12 months of treatment, reported more than 12 hours/day of elastic wear on average and had before and after CBCT radiographs were included in the study. Patients who did not receive BAMP therapy for at least 12 months or were not compliant with elastics were excluded. Recorded data included sex, age, treatment duration, and cephalometric angular values.
BAMP Protocol
A total of 4 Bollard Miniplates (KLS Martin, Umkirch, Germany) were surgically placed on each patient following a standard protocol under general anesthesia. Two Bollard miniplates were placed bilaterally on the maxilla at the infrazygomatic crest, above the permanent maxillary first molars. Two more Bollard Plates were placed bilaterally on the mandible between the roots of the permanent lateral incisors and canines. The Bollard miniplates used are shown in Figure 1 and are depicted on a maxilla and mandible model in Figure 2. The miniplates were fixated to the bone using monocortical (5-7 mm length; 2 mm diameter) self-tapping titanium screws (KLS Martin, Umbirch, Germany); 3 screws were placed per plate in the maxilla, and 2 screws per plate in the mandible. A single dose of IV amoxicillin and clavulanic acid was administered during surgery.

Bollard Miniplates.
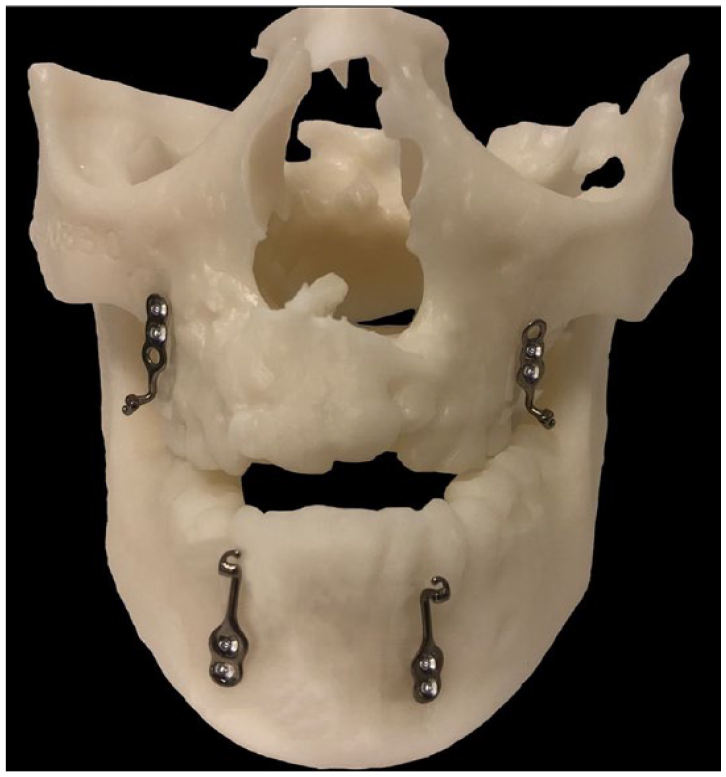
3D model demonstrating the position of the Bollard Miniplates on the mandible and maxilla.
Two weeks after the placement of the miniplates, orthodontic elastics were connected between the maxillary and mandibular miniplates. The initial loading forces were measured to 100 g per side. Approximately 12 weeks later, the force was increased to 200 g per side and maintained throughout BAMP therapy. The patients were instructed to wear the elastics full-time (day and night) and change them whenever they brushed their teeth or ate.
Radiological Follow-Up
Cone-beam computed tomography (CBCT) scans were taken before therapy (T1) and after therapy (T2). T1 CBCTs were taken as part of the surgical planning for miniplates placement, whereas T2 CBCTs were taken to evaluate the postoperative outcomes and maxillomandibular relationship changes. Cephalometric radiographs were extrapolated from each CBCT, and the same examiner (RC) traced each radiograph in Dolphin Imaging Software (Patterson Dental Supply, Inc., Chatsworth, California) using the standard American Board of Orthodontics (ABO) anatomical identification points. SNA, SNB, and ANB measurements were taken from each tracing and analyzed.
Statistical Analysis
Basic descriptive statistics, including initial and final measurements of SNA, SNB, and ANB, treatment duration, age, and gender were recorded for each patient. To assess the changes in SNA, SNB, and ANB measurements over the treatment period, paired t-tests were conducted; Cohen’s d was computed to provide insight into the magnitude of observed differences. The strength and directionality of the relationship between ANB and treatment duration was calculated using Pearson’s Correlation. A simple linear regression model was fitted to further understand the relationship between the change in ANB and changes in treatment duration. A multiple linear regression model was used to evaluate the combined effect of treatment duration, age, and gender on the change in ANB. All statistical analyses were conducted using R software (version 4.2.3) utilizing the “base,” “effsize,” and “ggplot2” packages [R Core Team, 2023; Torchiano, 2020; Wickham, 2016].18,19,20
Results
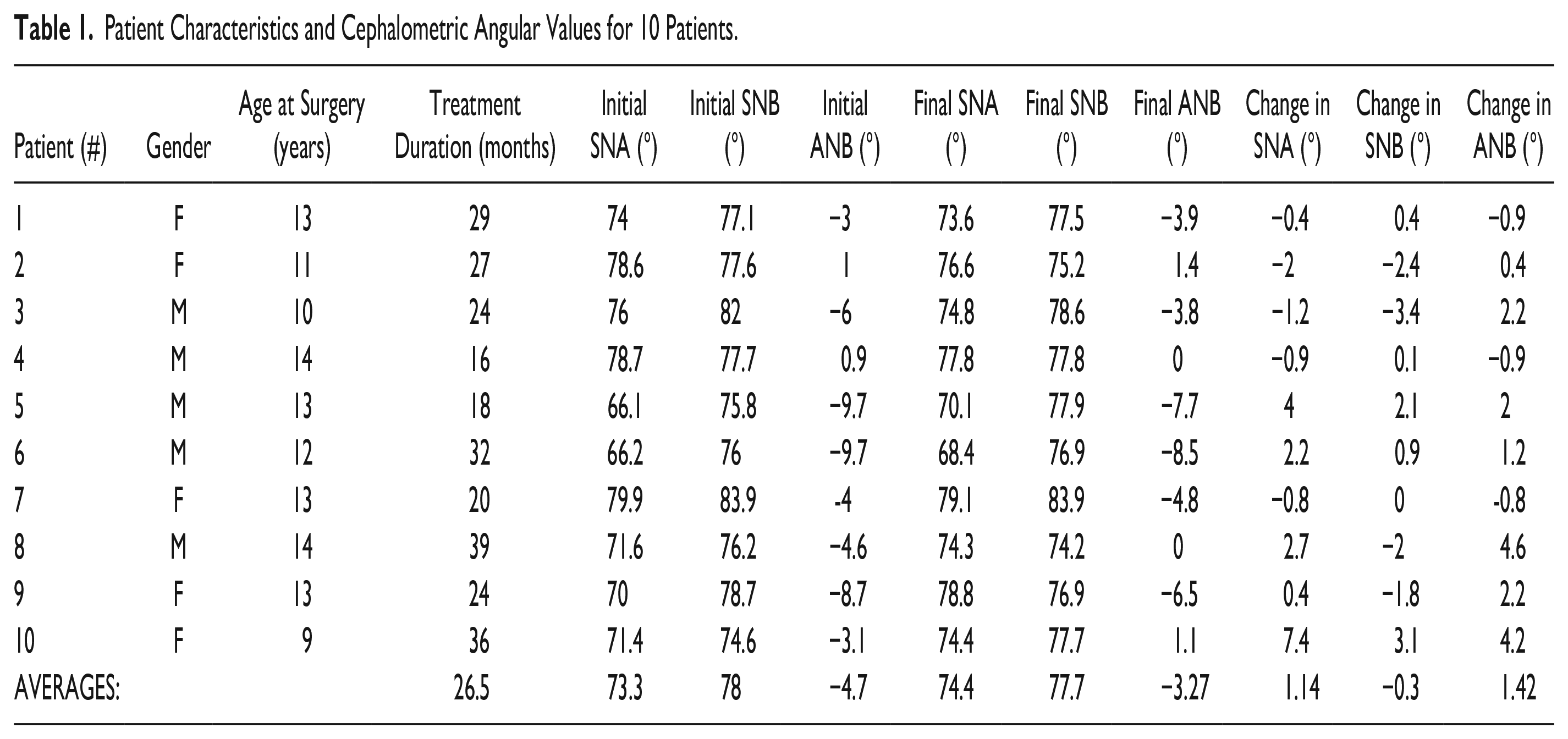
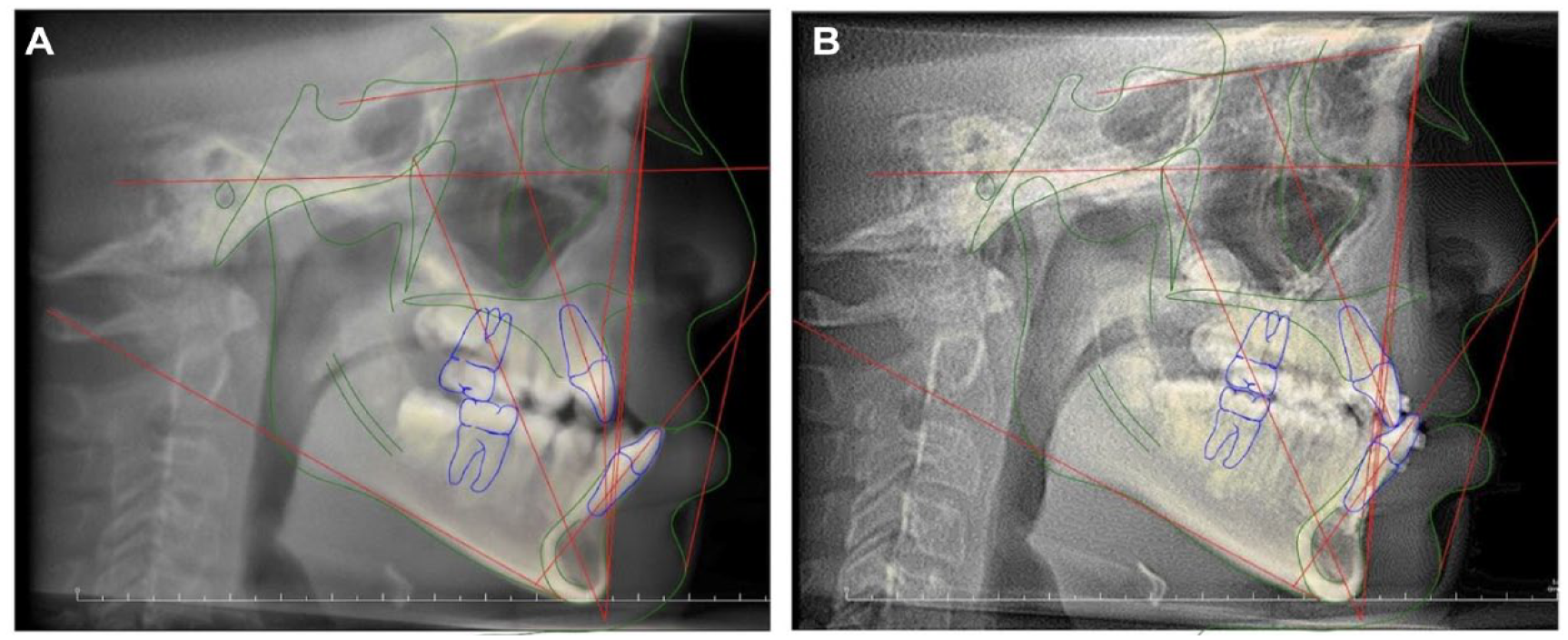
Ten patients met our inclusion criteria. Of these, 6 had unilateral CLP, 2 had bilateral CLP, and 2 had CLP with unspecified laterality. The average age at the time of miniplate placement was 12.2 years, with an average treatment duration of 25 months. The cohort was evenly split between males and females. The average change in ANB was +1.42°, ranging from −0.9° to 4.2° (Table 1). T1 and T2 cephalometric radiographs for 3 patients are illustrated in Figures 3 to 5. Notably, the patient with the most substantial ANB improvement transitioned from −3.1° before BMP therapy to 1.1° post-therapy, marking an enhancement of +4.2° (Figure 5). The superimposition for this patient is presented in Figure 6. Of note, one patient required surgical replacement of the right maxillary miniplate due to plate instability and gingival impingement. Another patient experienced mucosal irritation around the miniplates that persisted for one-month post-operatively but did not lead to ulceration. No other complications were reported.
Patient Characteristics and Cephalometric Angular Values for 10 Patients.
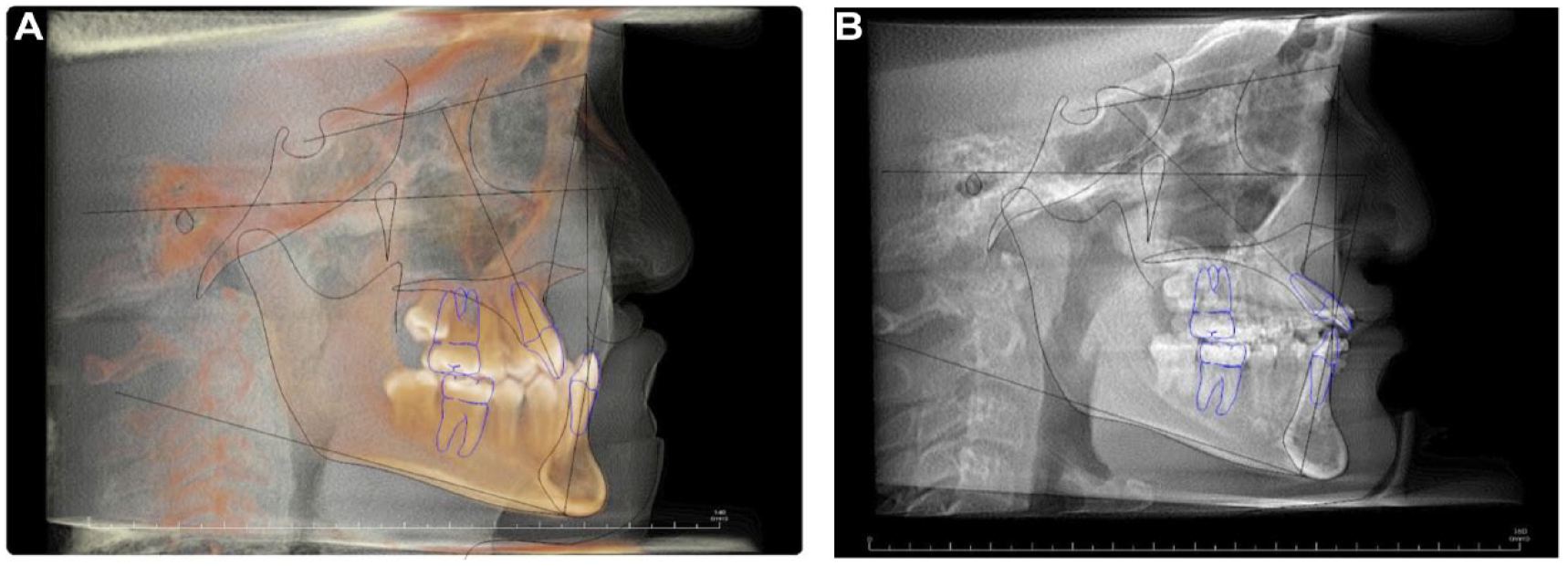
Patient JS. (a) T1 and (b) T2.
Patient RG. (a) T1 and (b) T2.
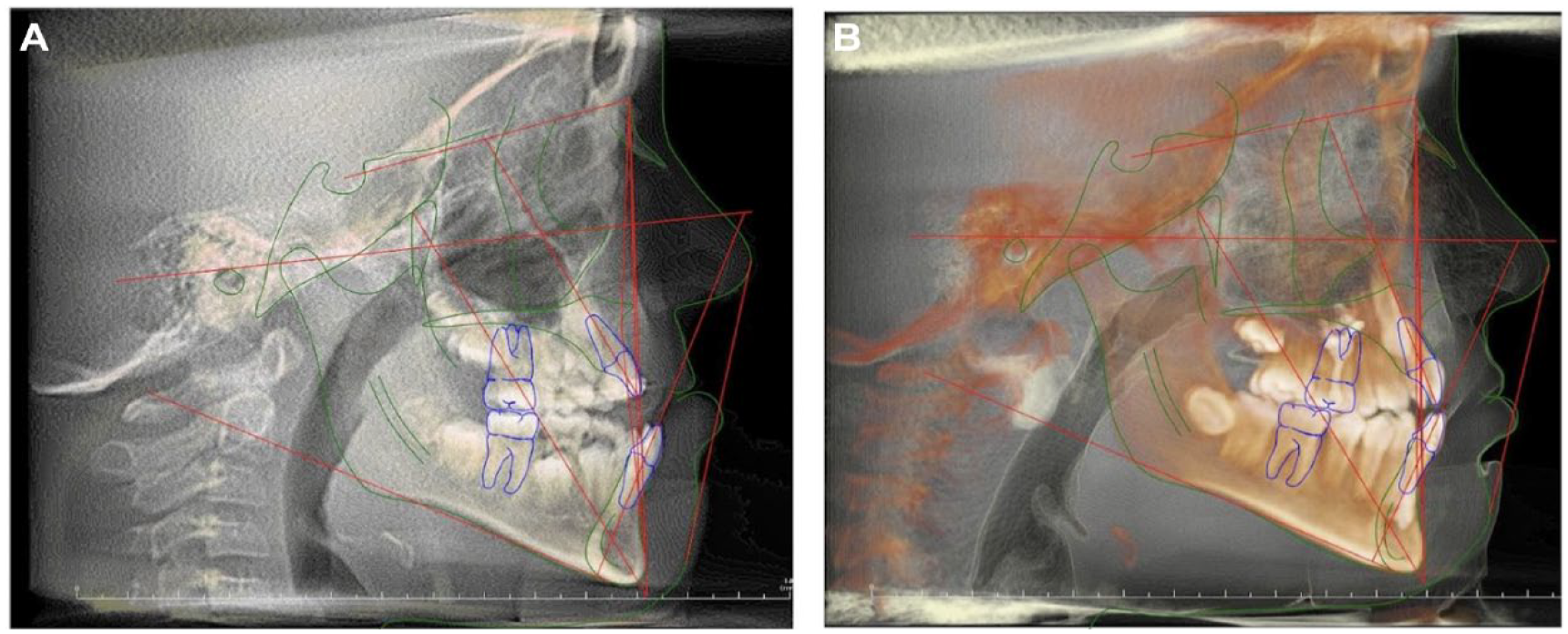
Patient ZS. (a) T1 and (b) T2.
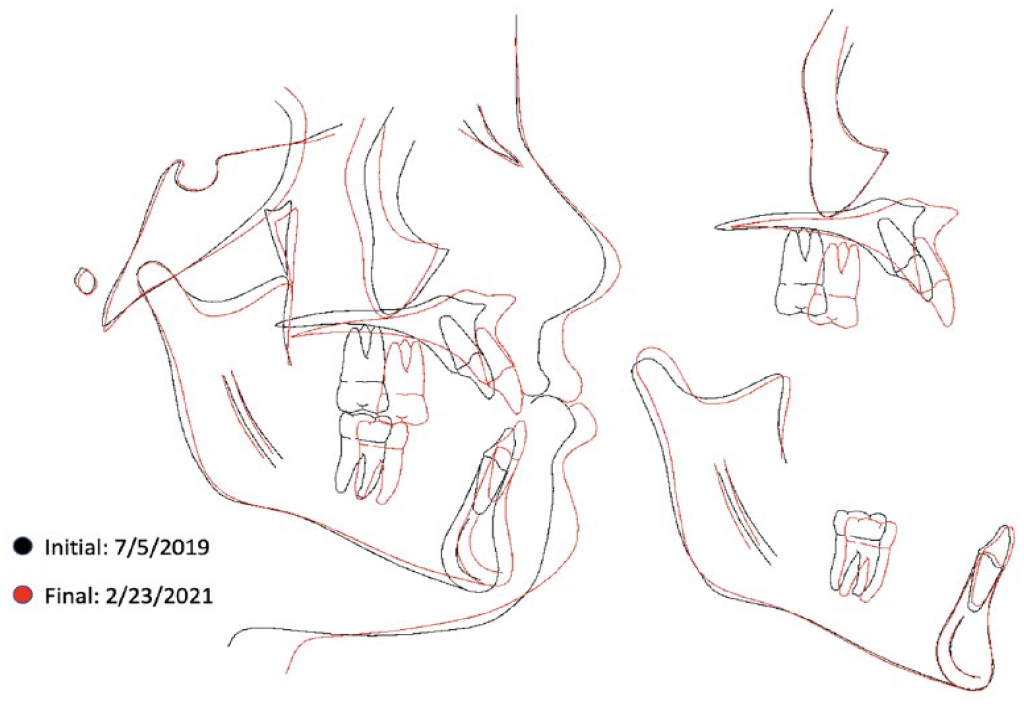
Superimposition for patient ZS.
There were no significant differences between initial and final measurements for both SNA (P = .1739) and SNB (P = .6580). The change in ANB measurements was borderline (P = .0519) but did not reach statistical significance. Analysis of effect size demonstrated a moderate change in SNA values (Cohen’s d = 0.4669) and a small change in SNB values (Cohen’s d = −0.1447). Notably, there was a moderate to large change (Cohen’s d = 0.7083) in ANB values. Correlation analyses between the change in ANB and treatment duration demonstrated a Pearson’s Correlation of .6457. Simple linear regression demonstrated an R2 of 0.417, with every additional month of treatment corresponding to an increase of 0.1702° in ANB change (P = .0440). Expanding the model to also include age and gender diminished statistical significance but yielded an R2 of 0.541. In this model, treatment duration resulted in 0.1596° increase in ANB change per month (P = .082), each added year of age predicted a decrease of 0.2834° in ANB change (P = 0.455), and female gender was associated with a decrease of 1.250° in ANB change (P = .294).
Discussion
BAMP therapy utilizes bone-anchored titanium miniplates connected by class III elastics to facilitate bone-borne orthopedic forces.16,17 Early publications by De Clerck et al. underscored the benefits of BAMP therapy in patients without CLP.12,13,15 Their experiences highlighted the advantages of self-tapping screws, pre-surgical counseling, minimally invasive techniques, and regular orthodontic follow-up.15,21 Adhering to this protocol, we achieved a miniplate anchorage success rate of 97.5% with minimal complications.
Patients with CLP are particularly susceptible to maxillary retrusion secondary to the scarring from previous surgeries. A study by Semb et al demonstrated that as patients with CLP progress through craniofacial development, the anteroposterior position of the maxilla decreases by an average of 5.4°.2,22 Thus, interventions that stabilize or enhance occlusal relationships are invaluable, especially if they result in less invasive and smaller orthognathic surgical movements later in life. In specific instances, BAMP therapy may negate the need for orthognathic surgery entirely. 1
While it is still unclear what percentage of patients undergoing BAMP therapy will require orthognathic surgery, Faco et al. demonstrated the efficacy of BAMP therapy in patients with UCLP in a comparative study of cephalometric outcomes. 23 Those undergoing BAMP therapy exhibited significant maxillary protraction and Class III skeletal pattern improvements compared to a control group. Specifically, the treatment group showed an ANB improvement of +1.69°, in contrast to the control group’s ANB decrease of −0.26°. The cephalometric outcomes of our patients in the retrospective review aligned with these findings, demonstrating varied ANB changes, with an average improvement of +1.4o. Although this improvement did not achieve statistical significance (P = .0519), the effect size, represented by a Cohen’s d of 0.7083, suggests a moderate to large practical difference between initial and final ANB measurements. Combined with evidence from previous research, our findings support the clinical significance of BAMP therapy as an effective modality for maxillary protraction patients with CLP.
To ensure adequate duration BAMP therapy, our institutional approach initiates BAMP therapy post-alveolar bone grafting after the eruption of the mandibular permanent canines. Therapy continues until the patient is ready to begin orthodontic preparation for orthognathic surgery or until it is determined that a possible overjet and an acceptable occlusion can be achieved with braces alone. Bollard plate removal typically occurs around the age of 15 for females and 16 for males, and can coincide with the removal of wisdom teeth if necessary. Although correlation analysis indicated a strong positive linear relationship between treatment duration and change in ANB (Pearson’s = 0.6547), there was notable variability in ANB change between patients. At the time this study was conducted only 2 patients, those with the longest duration of treatment, had achieved class I occlusion (patients 8 and 10 in Table 1).
Regression analyses provided further insight into the relationship between treatment duration and the factors influencing the variability of ANB change at our institution. A simple linear regression model between ANB change and treatment duration explained 41.7% of the variability in our study, with each month of treatment associated with a significant 0.1702° change in ANB (P = .0440). Multiple linear regression including age and gender explained 54.1% of the variability but lost statistical significance for treatment duration (P = .082) and did not reach statistical significance for age and gender, likely due to our limited sample size. However, the decreases in ANB change associated with increasing age (−0.2834° change per year) and gender (−1.250° change for female gender) correspond with our current biophysical understanding of skeletal maturation in patients with CLP. As we expand our sample size in future studies, the effects of these factors may become more apparent to guide the temporal optimization of BAMP therapy initiation at our institution.
The biomechanics of BAMP therapy also require consideration throughout pediatric development. During therapy, the elastics exert a posterior force vector on the mandible, promoting maxillary advancement as the child grows. As many of our patients had received BAMP therapy for over 2 years, the prolonged distalization of force on the mandibular condyle raises concern for the burden placed on the temporomandibular joint (TMJ). However, we did not observe any TMJ pain or change in our patient cohort. We believe that the lack of TMJ-related complications is due, in part, to active remodeling of the TMJ during adolescence. However, we recommend monitoring for complications related to this biomechanical burden in all patients undergoing BAMP therapy.
Our case series reinforces the conclusions drawn from the literature and underscores the value of BAMP therapy in orthognathic treatment for patients with CLP. Ongoing observation is essential to assess final orthognathic surgery needs, surgical outcomes, and cephalometric measurements.
Conclusion
Between 2019 and 2022, our institution observed maxillary growth improvements in adolescent patients using BAMP therapy. Rather than waiting until skeletal maturity for definitive correction with orthognathic surgery, this proactive approach was well-received by our patients and their families. Cleft surgeons should consider this modality after alveolar bone grafting in patients with Class III malocclusions. Through continued research and analysis of our BAMP therapy in our patient population, we aim to optimize treatment for malocclusions in our patients with CLP and provide a more predictable option for maxillary advancement during adolescence.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
The study was conducted in accordance with the Declaration of Helsinki and was approved by Institutional Review Board (no. H-52428) on 5/5/2023, with an exemption from informed consent.