
Abstract
Background:
Despite improvements in microsurgical techniques and broad application of free tissue transfer for reconstruction in the adult population, there is currently a paucity of literature regarding microsurgical reconstruction in the pediatric population, notably a limited number of case series evaluating outcomes following head and neck reconstruction.
Methods:
A retrospective analysis of National Surgical Quality Improvement Program Pediatric (NSQIP-P) database from 2015 to 2020 was performed. Pediatric patients undergoing head and neck reconstruction with microvascular muscle and fasciocutaneous flaps were identified using Current Procedural terminology codes (CPT). Multivariate logistic regressions were conducted to assess postoperative outcomes of interest.
Results:
A total of 120 head and neck free flap reconstructions were performed in the pediatric population. Most free flaps were microvascular muscle (n = 82, 68%) followed by fasciocutaneous (n = 38, 32%) flaps. The surgical complication rate was 8% (n = 9) and was primarily due to wound infection 6% (n = 7), whereas medical related complication rate was 14% (n = 17) with majority of patients requiring blood transfusion 12% (n = 14). The median length of stay was 4 days, and ventilator dependence was found to be significantly different among microvascular free flap types. Patients with underweight BMI and ASA Class >2 had higher odds (OR 59.7 and 17.0, P < .05 respectively) of developing any complication for microvascular muscle flaps.
Conclusion:
Analysis of a national cohort of pediatric patients revealed a low flap-related complication rate. Although free flap reconstruction in the pediatric population is technically demanding, microsurgical free tissue transfer in this population is safe and should be considered if indicated.
Background
Microvascular free flap reconstruction techniques are continuously evolving and have been utilized to address various anatomic defects in the adult population.1-3 Although free flap reconstruction is an established and reliable method for adults, the use of microsurgical tissue transfer is less common in the pediatric population. The indication for head and neck reconstruction differs by age. In adults, head and neck tumors are commonly squamous cell carcinomas, whereas in children they are most commonly sarcomas.4,5 Removal of such tumors in pediatric patients might necessitate an aggressive approach with extensive resection leaving substantial tissue deficit for reconstruction. Furthermore, the technical challenges in smaller patients are greater due to anatomic differences, such as smaller vessel size, smaller donor size, and increased risk of vasospasm.6-9 Another concern is donor-site morbidity and the potential for asymmetry and functional deficit at the donor site, especially in patients undergoing osteocutaneous or muscle free flap reconstruction. Still another concern is whether the transferred tissue grows commensurate with the surrounding native tissue without causing contracture, atrophy, or bone graft growth restriction over time.
Despite the improvement of microsurgical techniques and broad application of free flap reconstruction in adult populations, there is a paucity of literature pertaining to the pediatric population. Current reports are limited to a few large case series evaluating outcomes following reconstruction in children for all over the body.7,8,10 Several studies have examined the subset of lower limb reconstruction with free flap in the pediatric population.6,11,12 However, similar outcomes following head and neck reconstruction in this group have seldom been reported.13-19 In the present study, the authors sought to evaluate outcomes and risk factors for 30-day postoperative complications in pediatric patients undergoing head and neck microvascular free flap reconstruction utilizing a nationwide sample.
Methods
Following review by the Institutional Review Board of the Icahn School of Medicine review, the study was given exempt status (No. 22-01071). A retrospective review was performed using the American College Surgery National Surgical Quality Improvement Program Pediatric (NSQIP-P) database from 2015 to 2020. NSQIP-P is a deidentified surgical database from over 140 sites nationally with variables covering patient demographics, comorbidities, preoperative, intraoperative, and postoperative outcomes.
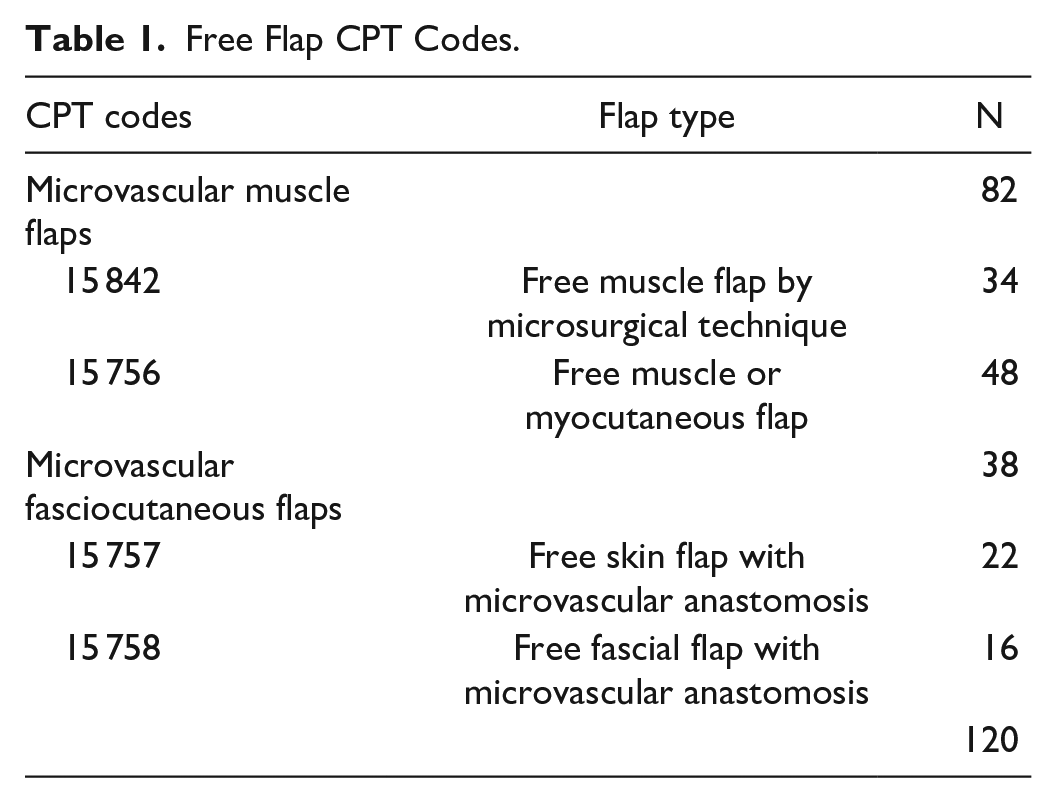
Current Procedural Terminology (CPT) codes were used to identify pediatric patients who underwent free flap reconstruction (Table 1). Following retrieval of all free flaps (n = 400), 2 independent authors manually screened and identified cases with diagnosis related to head and neck using Classification of Diseases ICD-9 and ICD-10 diagnosis (Supplemental Table 1). Only patients undergoing a single free flap reconstruction were included in the study and cases were screened for duplication. Patients who underwent head and neck reconstruction with free flaps were further categorized into microvascular muscle flaps and microvascular fasciocutaneous flaps cohorts (Table 1).
Free Flap CPT Codes.
Study Variables
Patient demographics (age, sex, race, ethnicity), pulmonary comorbidities (bronchopulmonary dysplasia/chronic lung disease, structural pulmonary/airway abnormalities, history of asthma), cardiac comorbidities (cardiac risk factors, previous cardiac surgery), neurological comorbidities (seizure disorder, cerebral palsy, developmental delay/impaired cognitive status, neuromuscular disorder, structural CNS abnormality), blood transfusions within 48 hours prior to surgery, congenital malformation, esophageal/gastric/intestinal disease, hematologic disorder, history of malignancy, nutritional support, open wound (with or without infection), oxygen support, premature birth, SIRS/sepsis/septic shock within 48 hours prior to surgery, steroid use (within 30 days), tracheostomy, ventilator dependence, and surgical characteristics (American Society of Anesthesiologists [ASA] Classification, total operation time, and wound classification) were extracted. BMI was calculated from height and weight. Patients lacking either information or below the age of 2 years old were excluded in BMI analysis. BMI-for-age percentiles were calculated based on Center for Disease Control and Prevention (CDC) growth charts. 20 Patients with a BMI less than the fifth percentile for their age and sex were assigned underweight, between 5th and 85th percentile normal weight, 85th-95th percentile overweight, and >95th percentile obese.
Postoperative surgical complications include those at the surgical site (superficial, deep, or organ-space surgical site infection [SSI]; deep wound disruption/dehiscence). Medical complications included acute renal failure, bleeding requiring blood transfusion, pneumonia, postoperative Clostridium difficile complication, progressive renal insufficiency, seizure disorder, sepsis, septic shock, unplanned intubation, urinary tract infection, and venous thrombosis. Other postoperative complications include unplanned reoperation, unplanned readmission, death within 30 days of the original procedure, and length of hospital stay (LOS) >4 days.
Statistical Analysis
Descriptive statistics of categorical variables were reported as frequencies and proportions (N, %) and P-values were calculated using Pearson’s Chi-Square test. Continuous variables were reported with median and interquartile ranges (median, IQR), and P-values were calculated using Kruskal–Wallis Test. Multivariate logistic regressions were conducted to calculate the odds ratios and 95% Confidence (OR, 95% CI) when controlling for confounding variables. Risk factors demonstrating an association with any postoperative complication at P < .2 in univariate analysis were entered into backward stepwise regression with exit criteria of P < .05. The resulting variables were included in the logistic regression models. Total operation time and total relative value units were included in regressions to control for effects of operative time and concurrent surgical procedures. This was conducted for all microvascular free flap types to compare complications rates (complications, surgical complications, medical complications, bleeding requiring blood transfusion, LOS > 4 days, unplanned reoperation and readmission,) between microvascular free flap types. Hosmer-Lemeshow and C-statistic values were calculated to assess the calibration and discrimination of the overall goodness of model fit. All statistical tests were performed in IBM SPSS v28.0 (IBM, Armonk, NY) using a 2-tailed alpha of 0.05 to denote significance, and missing values were excluded in analysis.
Results
A total of 120 head and neck free flap reconstructions were performed in pediatric patients, with majority being microvascular muscle flaps (n = 82, 68%) followed by fasciocutaneous flaps (n = 38, 32%) (Table 1). There were 2 different post-operative ICD-9 codes and 49 ICD-10 Codes (Supplemental Table 1). The median age was 9 years (6.99-12.8) and majority of patients (n = 76, 70%) had a normal BMI (Table 2). Most patients were male (n = 69, 58%), White (n = 79, 66%), and non-Hispanic (n = 67, 60%), followed by unknown/not reported (n = 22, 18%), Asian (n = 7, 6%), and Black or African American (n = 12, 10%) (Table 2). The highest comorbidities consisted of congenital neurological comorbidities (n = 49, 41%), congenital malformation (n = 38, 32%), history of malignancy (n = 28, 23%), and pulmonary comorbidities (n = 17, 14%) (Table 3). Most patients were ASA Class 2 (n = 70, 59%) and wound classification of clean or clean/contaminated (n = 71, 59% and n = 49, 41%). Median operating time was 429 minutes (233-546). Ventilator dependence was found to be significantly different (P < .05) among microvascular free flap types (Table 3).
Demographics.
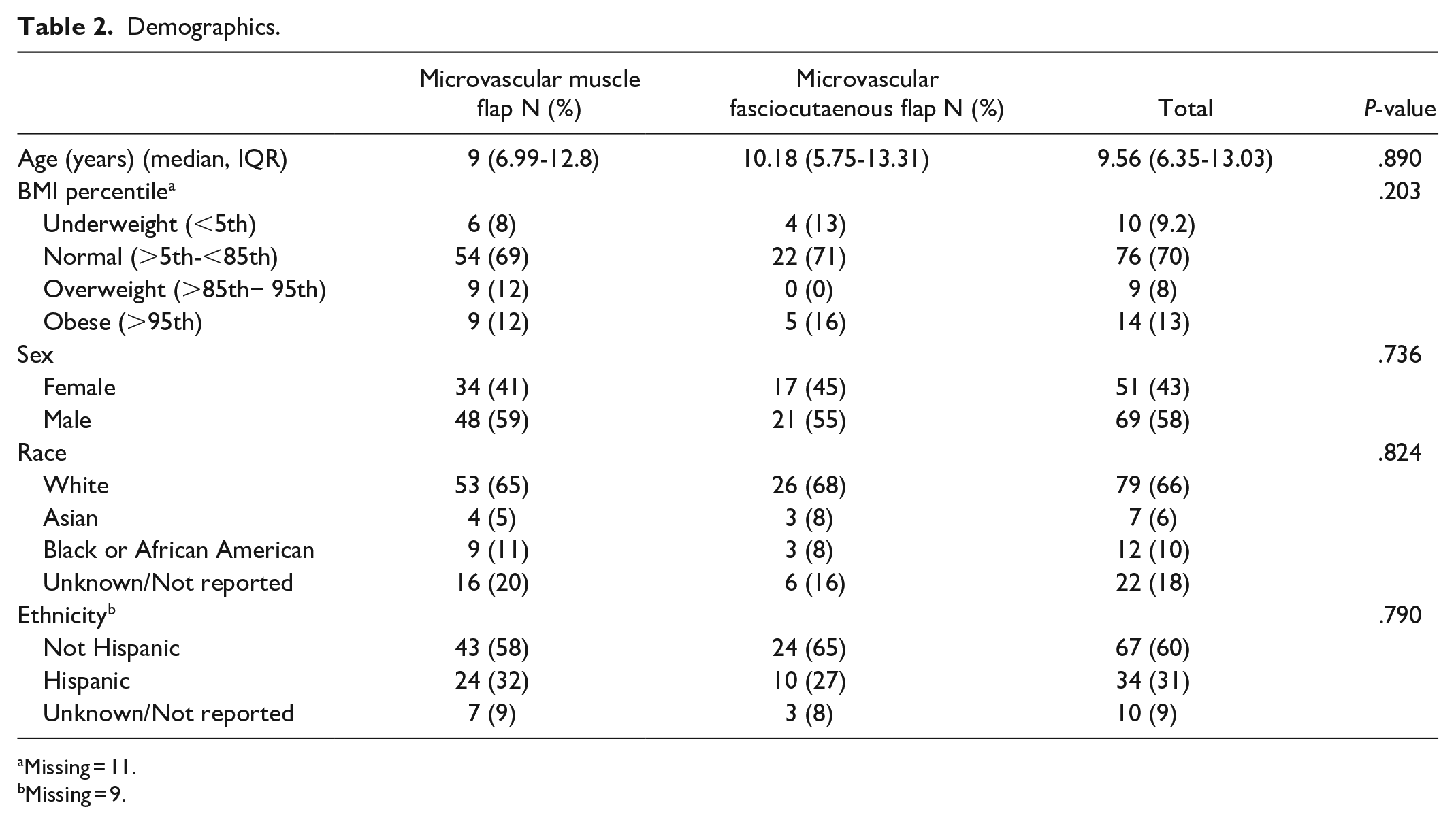
Missing = 11.
Missing = 9.
Comorbidities and Surgical Characteristics.
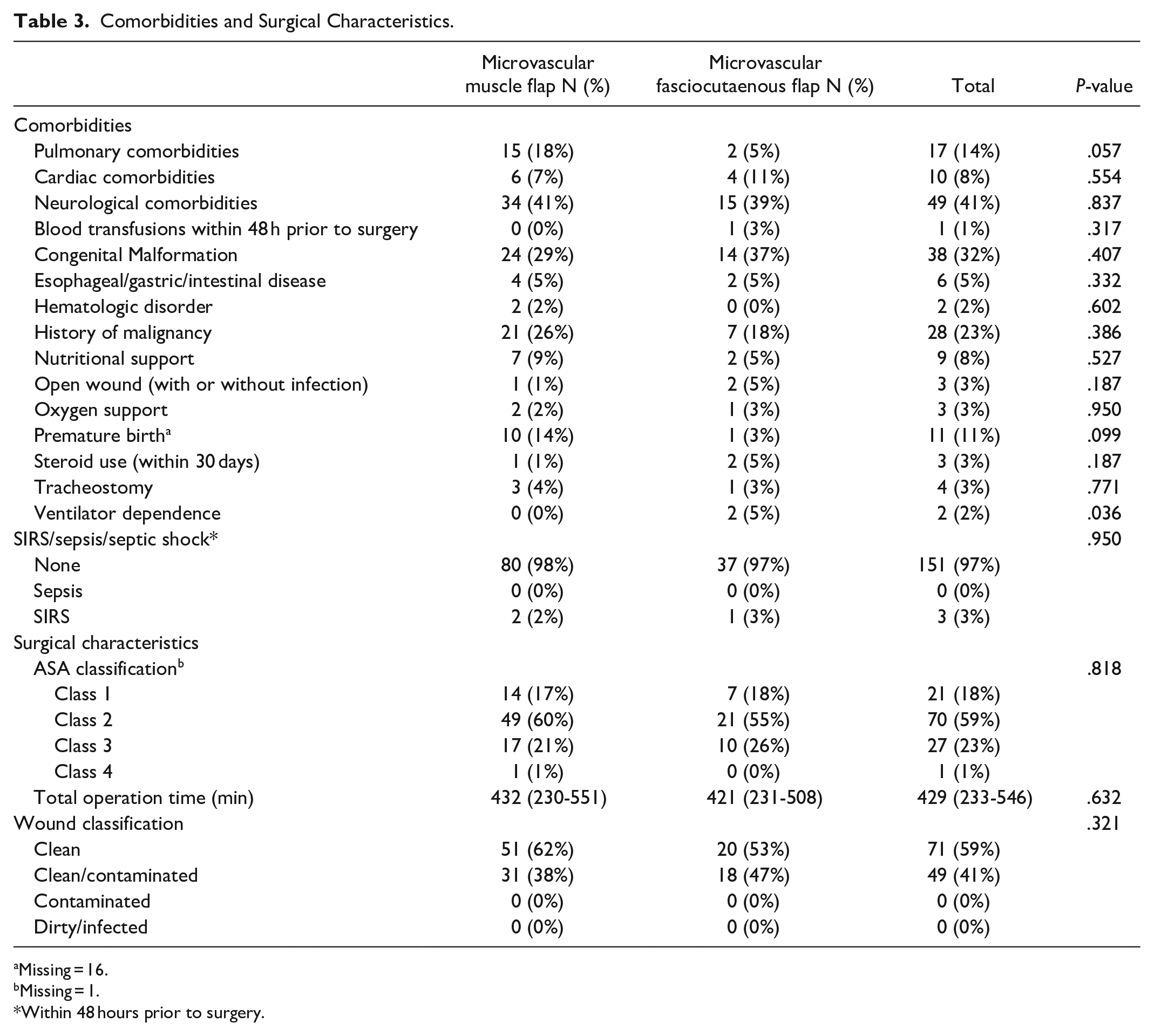
Missing = 16.
Missing = 1.
Within 48 hours prior to surgery.
Table 4 summarizes data regarding postoperative complications. Twenty-six percent of patients (n = 30) had any complication. Nine patients (8%) had surgical complications and 17 (14%) patients related to non-flap complications.
Complications.
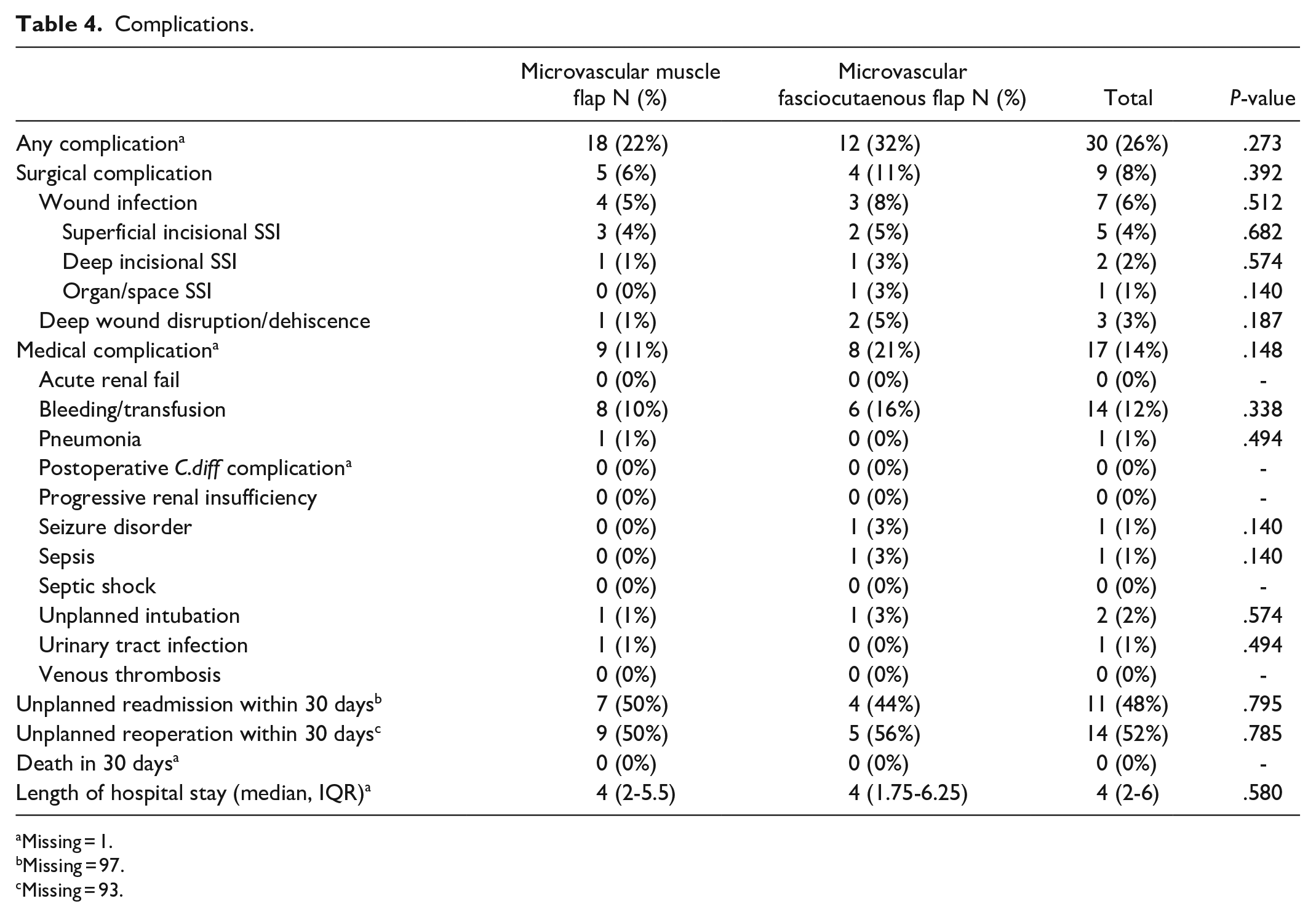
Missing = 1.
Missing = 97.
Missing = 93.
Surgical and medical complications were primarily from wound infection 6% (n = 7) and bleeding requiring blood transfusion 12% (n = 14), respectively. The data available for readmission and unplanned reoperation within 30 days was limited to n = 23 and n = 27 patients respectively. Of the available data, number of patients readmitted was n = 11 and reoperated n = 14. The median LOS was 4 days (2-6).
Patients with underweight BMI and ASA Class > 2 had higher odds (OR 59.7 and 17.0, P < .05 respectively) of developing any complication for microvascular muscle flaps. For microvascular fasciocutaneous flaps, male gender and total operation time (OR 146.9 and 1.01, P < .05) had higher odds for any complication (Table 5).
Associated Risk Factors Stratified by Microvascular Free Flap.
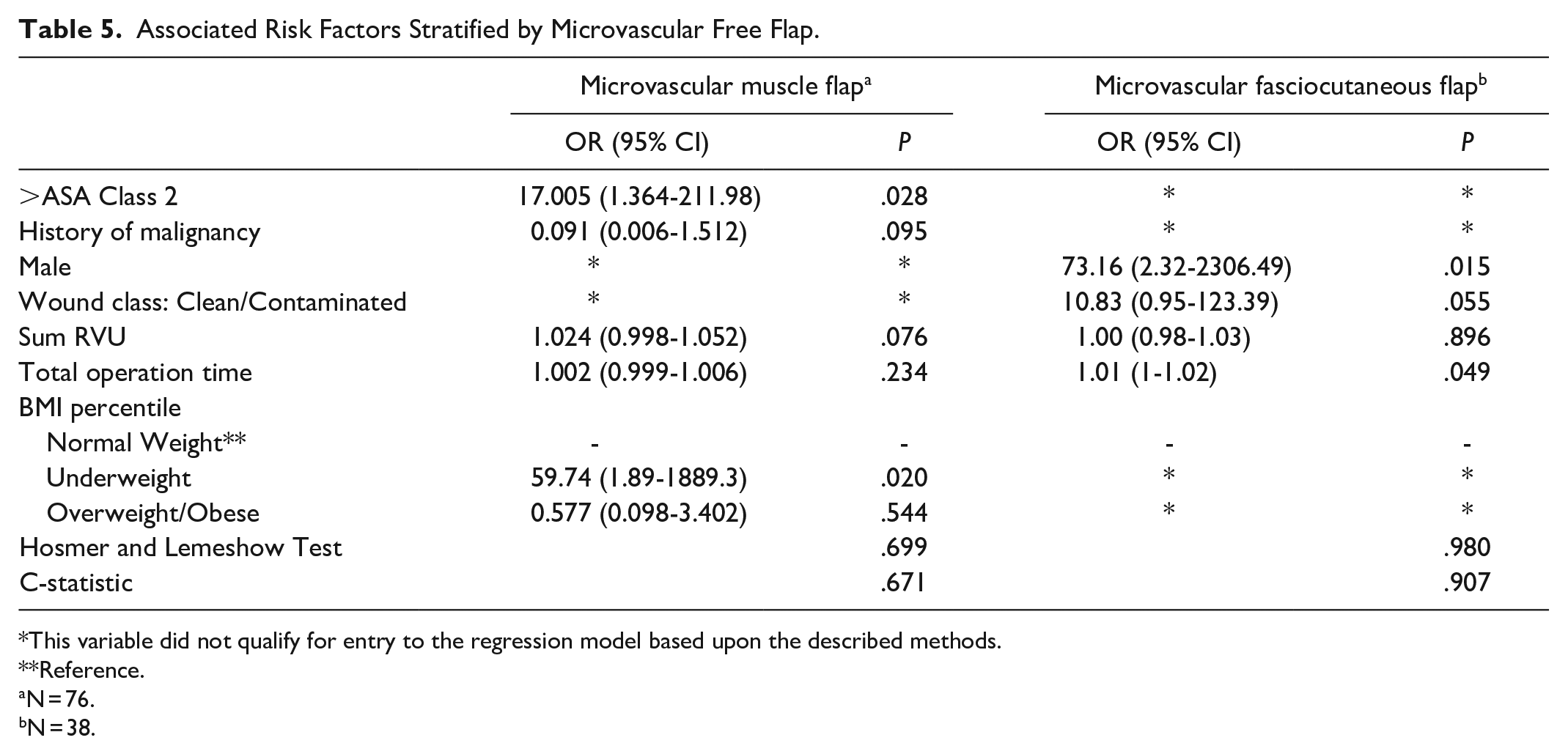
This variable did not qualify for entry to the regression model based upon the described methods.
Reference.
N = 76.
N = 38.
Table 6 demonstrates multivariate logistic regressions conducted for postoperative outcomes of interest. Increased total operation time was associated with higher odds of developing bleeding requiring blood transfusion (OR 1.01, P = .008), unplanned reoperation (OR 1.03, P = .037), unplanned readmission (OR 1.01, P = .038) and LOS > 4 days (OR 1.01, P = .005), although the odds ratios were all close to 1. Wound classification clean/contaminated (OR 324.9, P = .05) and >ASA Class 2 (OR 38.6, P = .027) were associated with higher odds of medical complications. Furthermore, overweight/obese (OR 9.6, P = .002) and age (OR 1.3, P = .019) were associated with higher odds of LOS > 4 days.
Associated Risk Factors for Surgical and Medical Complications, Bleeding, LOS > 4, Unplanned Reoperation, and Readmission.
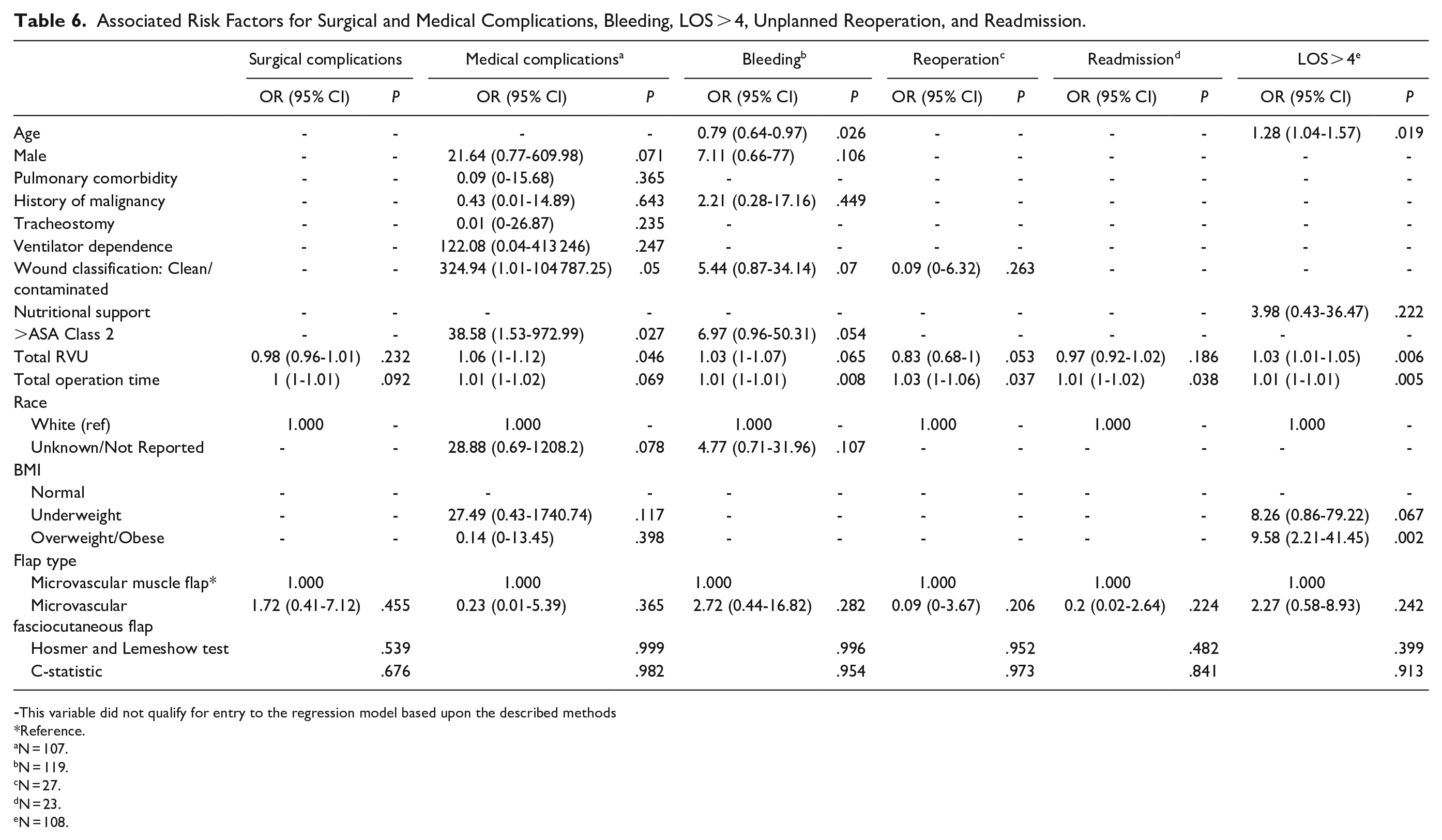
-This variable did not qualify for entry to the regression model based upon the described methods
Reference.
N = 107.
N = 119.
N = 27.
N = 23.
N = 108.
Discussion
Since Harii and Ohmori described first cases of microvascular reconstruction in children under 5 years with free groin flaps to the lower extremities, 21 studies have focused on reporting larger cohort outcomes.6-8,11 Despite concerns regarding the feasibility and technical difficulties associated with free flap transfer in pediatric patients, recent studies have reported high success rates even with microvascular anastomoses as small as 0.3 mm in diamter.6-8,11,22
Similar to our study, previous studies focused on pediatric lower limb reconstruction have also indicated a higher prevalence of free muscle flaps compared to fasciocutaneous flaps.6,23 However, recent studies have observed an emerging trend toward the utilization of fasciocutaneous flaps.6,24,25 This shift is primarily driven by the lower functional morbidity experienced at the donor site, the increased ease of performing secondary procedures like secondary bone grafting, and their effectiveness in preventing the development of functional contractures. A similar trend is seen in the adult population which leans toward utilizing fasciocutaneous flaps over free muscle flaps for both head and neck and lower limb reconstruction.26-28 This preference arises from the broader range of applications fasciocutaneous flaps offer, including their suitability for mucosal lining and pharyngeal defects, their less bulky nature, resistance to fluctuations in weight, and their ability to yield enhanced esthetic outcomes at the donor site.29-31
In our study, the surgical complication rate was 8% and was primarily due to wound infection (6%). These findings were consisted with previously published papers where infection rate ranged from 5.9% to 6.7%.14,18 Medical complication rate was 14% with majority of patients requiring blood transfusion (12%). When comparing to adults undergoing head and neck reconstruction with free flaps, rates for bleeding requiring transfusion are much higher in adults ranging from 24.6% to 32.9% than in pediatric patients.32,33
The total operation time for microvascular soft tissue reconstruction was 7.2 hours and was consistent with other studies.6,10 Furthermore, increased total operation time had higher odds to develop any complication for microvascular fasciocutaneous flaps. Although causal relationship between these factors could not be determined, several studies have analyzed relationship between operative time and surgical outcomes.34,35 Hardy et al reported that each hour increase in surgery duration is associated with 21% higher odds of morbidity. 34
Reconstruction with free muscle flaps were noted to have higher odds of developing any complication for patients who were underweight BMI and had > ASA Class 2. In a previous study, Makiguchi et al investigated the relationship between skeletal muscle mass loss and outcomes in patients undergoing free flap reconstruction for patients with oral cancer. They found that underweight was significantly related to SSI in recipient site. 36
A previously reported overall survival rate of free flaps reconstruction in children was noted to be 96.4%. 17 The high flap survival rate in pediatric patients and lower complication rate versus adults could be explained by the fact that comorbidities influencing microsurgical patency such as atherosclerosis, diabetes mellitus, hypertension, or smoking are absent in pediatric patients and surgeons rarely have to deal with significant co-morbidities such as myocardial infarction, stroke or pulmonary disease.
One concern with free tissue transfer in children is whether transferred tissue grows over time. However, Upton and Guo evaluated 433 free flap reconstruction in the pediatric population and concluded that myocutaneous as well as fasciocutaneous flaps grow commensurate with skeletal support and do not contract over time. He also reported that innervated muscles will grow and increase in bulk, whereas denervated muscle will atrophy but only expand with underlying skeletal growth. 8 Although free flap reconstruction in pediatric population is technically demanding, high success survival rate can be achieved with meticulous preoperative planning and involvement of surgeons with advanced surgical techniques.
Limitations
Several limitations of the ACS NSQIP database have been reported in the literature.37,38 Main limitations include the lack of detailed information regarding demographics, surgical characteristic, and patient outcomes, such as outcomes after 30 days, long-term flap, and donor-site complications. Other well-known limitations are accuracy of data entry and precision of the coding used. Furthermore, the database does not include specialty-specific outcomes, such as in this case free flap reconstruction. Additionally, in the present study, a number of unplanned readmission and reoperation data for head and neck reconstruction was missing, limiting analysis and impact of these factors on outcomes.
Conclusion
Analysis of the national cohort of pediatric patients undergoing free flap head and neck reconstruction revealed low flap related complication rate. Microsurgical free tissue transfer in pediatric patients should be pursued, as pediatric patients present with minimal comorbidities, previously unaltered anatomy, and predictable normal wound healing.
Supplemental Material
sj-docx-1-fac-10.1177_27325016231212094 – Supplemental material for Microvascular Soft Tissue Reconstruction Outcomes and Risk Factors in Pediatric Patients Undergoing Head and Neck Reconstruction
Supplemental material, sj-docx-1-fac-10.1177_27325016231212094 for Microvascular Soft Tissue Reconstruction Outcomes and Risk Factors in Pediatric Patients Undergoing Head and Neck Reconstruction by Justin James, Nargiz Seyidova, Evans Takyi, Olachi Oleru and Peter J. Taub in FACE
Footnotes
Acknowledgements
The American College of Surgeons National Surgical Quality Improvement Program Pediatric (ACS-NSQIP-P) and the hospitals participating in the ACS NSQIP P are the source of the data used herein; they have not verified and are not responsible for the statistical validity of the data analysis or the conclusions derived by the authors.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics Approval
Following review by the Institutional Review Board of the Icahn School of Medicine review, the study was given exempt status (No. 22-01071).
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.