
Abstract
Objective:
This study presents a novel approach that utilizes recombinant human bone morphogenic protein 2 (rhBMP-2) and cellular bone matrix (CBM) for revision alveolar bone graft (ABG) in unilateral cleft lip and palate (UCLP) and bilateral cleft lip and palate (BCLP) patients following failed autologous ABG.
Methods:
A case series of 14 UCLP and 4 BCLP patients who had failed autologous ABG with revision ABG with rhBMP-2 and CBM. Review of demographics, operative data, Bergland score, and alveolar cleft gap volume was performed.
Results:
Revision ABG had short operative times and low blood loss in both UCLP and BCLP. No postoperative complications were found in either revision group. Repeat ABG surgery was required in one patient. Bergland score improved from 3.86 ± 0.53to 1.21 ± 0.80 in the UCLP group and from 3.75 ± 0.50to 1.00 ± 0.00 in the BCLP group. The cleft volume decreased by 83.62 ± 9.78% in UCLP and by 86.73 ± 13.65% in the BCLP group.
Conclusions:
Revision ABG with rhBMP-2 and CBM is a successful and reliable approach. This method has decreased operative time and no postoperative complications. Most patients achieved clinically successful grafting with canine eruption. Both UCLP and BCLP groups saw a significant decrease in alveolar cleft gap volume.
Introduction
Alveolar bone grafting (ABG) is a reconstructive procedure for the alveolar ridge, commonly performed in children with cleft lip and palate to stabilize the maxillary arch, facilitate dental eruption, and oronasal fistula clsoure.1-4 Various techniques are used for alveolar bone grafting, with autologous bone grafts involving the transfer of the patient’s bone, usually from the hip, and grafting it into the alveolar ridge.
Failure of ABG can result in persistent alveolar fistula and insufficient bone stock to support the maxillary arch, complicating tooth eruption. The incidence of ABG failure has been reported to be as high as 18% in unilateral cleft lip and palate (UCLP) and 32% in bilateral cleft lip and palate (BCLP). 5 Parents often desire an alternative to ABG with an autologous iliac crest graft, and cleft surgeons are utilizing an increased number of non-autologous materials. 6
Allografts, which utilize bone graft substitutes, offer an alternative to alveolar ridge reconstruction. These allograft materials are readily available, user-friendly, reduce operative times, and eliminate donor site pain.7-9 Cellular bone matrix (CBM) is a unique allograft composed of an extracellular bone matrix that retains mesenchymal stem cells, providing osteoconduction, osteoinduction, and osteogenic potential.10-12 The osteogenic potential of CBM has led to increased use in spinal fusion surgery, but its application in alveolar ridge reconstruction has not been reported.12-14
Recombinant human bone morphogenic protein-2 (rhBMP-2), an osteoinductive growth factor, has been shown to have outcomes similar to autologous ABG reconstruction when combined with allograft materials.2-4,15,16 Among North American cleft surgeons, 23% report using allograft bone products, and 31% employed rhBMP-2. 6
This study presents a novel approach for alveolar reconstruction by combining CBM with rhBMP-2 for revision ABG in UCLP and BCLP following failed autologous ABG. Outcomes were evaluated using operative and orthodontic data and volumetric analysis with cone beam computed tomography (CBCT).
Methods
A retrospective review of patients with UCLP and BCLP who experienced failed autologous ABG followed by revision ABG using rhBMP-2 and CBM was performed following institutional review board approval (STU 2023-0692) by the University of Texas Southwestern Medical Center. Medical records were reviewed to collect demographic, operative, and post-operative information. Senior author YJP reviewed dental radiographs and CBCT for an orthodontic evaluation. Cleft alveolus volume was evaluated using CBCT performed pre-operatively and 6 months post-operatively. Manual CBCT segmentation of the empty alveolar gap was performed using Mimics 25.0 (Materialise, Belgium), and volume calculations were performed using 3-Matic 17.0 (Materialise, Belgium). Segmentation borders encompassed the pyriform aperture superiorly, the alveolar margin inferiorly, and the adjacent teeth alveolus is shown in Figure 1. Additional evaluation of the failed autologous ABG with iliac crest bone graft was performed for baseline characterization.
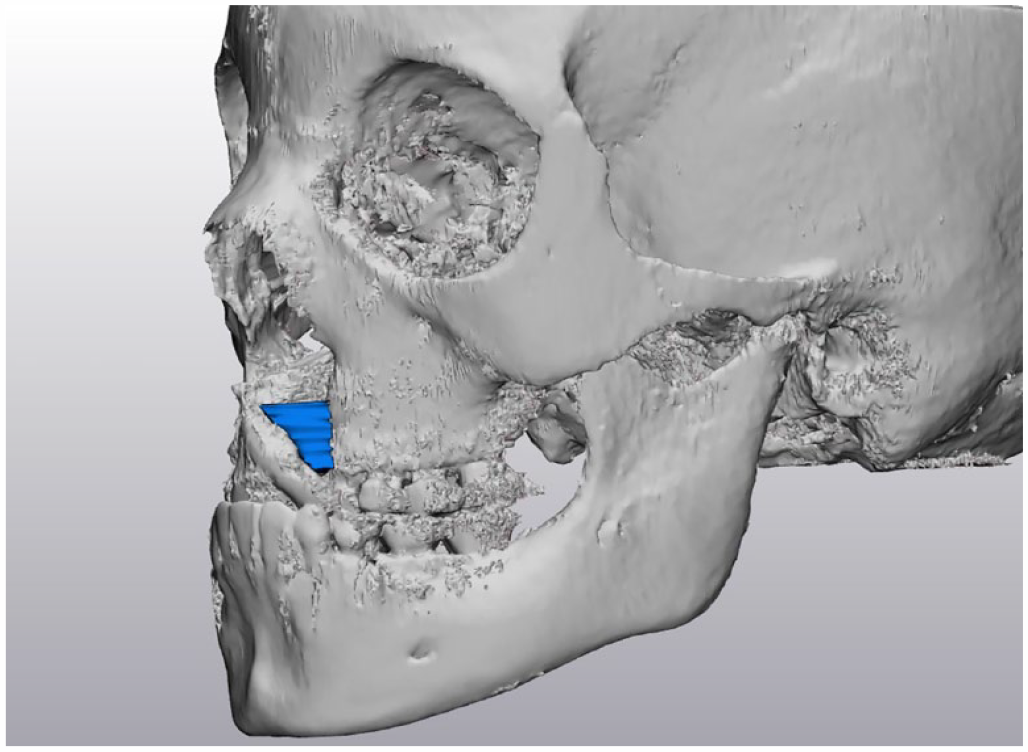
Alveolar cleft gap volume segmentation boards with pyriform aperture superiorly, alveolar margin inferiorly, and adjacent teeth alveolus.
Operative Technique
Mucoperiosteal flaps were elevated with superiorly based gingival flaps, and flaps were raised with the edges of the alveolus isolated. The pyriform floor and premaxilla were separated from the overlying mucosa. A watertight pocket is created centrally to place rhBMP-2 (Infuse Bone Graft, Medtronic) and CBM (Trinity Elite, MTF Biologics) and closed with an interrupted suture.
Results
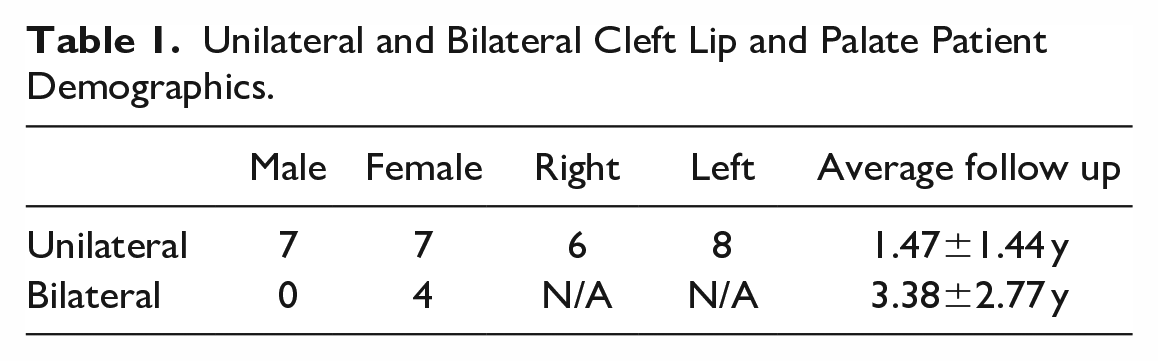
A total of 14 patients with UCLP and 4 with BCLP had experienced failed autologous ABG and underwent revision ABG using rhBMP-2 and CBM, as shown in Table 1. Autologous ABG failed due to bone deficiency in 66.6% of cases and exposure in 33.3%. The average post-operative follow-up time was 1.47 years in UCLP and 3.38 years in BCLP. All patients had previously undergone orthodontic treatment with a rapid palatal expander to address the maxillary transverse discrepancy and improve surgical access to the cleft.
Unilateral and Bilateral Cleft Lip and Palate Patient Demographics.
UCLP autologous ABG and revision ABG with rhBMP-2 and CBM operative data are shown in Table 2. The average age of operation was 11.45 years at revision ABG. The operative time was, on average, 1.5 hours. Blood loss was, on average, 21 mL. The hospital length of stay was just over 1 day following ABG. The canine eruption occurred in 100.0% following revision ABG. The canine eruption was not interfered with, and orthodontic tooth movement through graft was successful. Two patients needed surgical exposure of cleft side canine due to their poor location, and both canines were brought to the correct position. Bergland scores increased from an average of 3.86 to 1.21. No significant complications were found. One patient required re-operation following revision ABG. The cleft alveolus gap, on average, decreased by 83.62% from an average volume of 364.41 to 59.75 mm3. At the time of CBCT, the canine adjacent to the cleft erupted in 42.9% of revision ABG.
Unilateral Cleft Lip and Palate Primary and Revision Alveolar Bone Graft Operative Data.
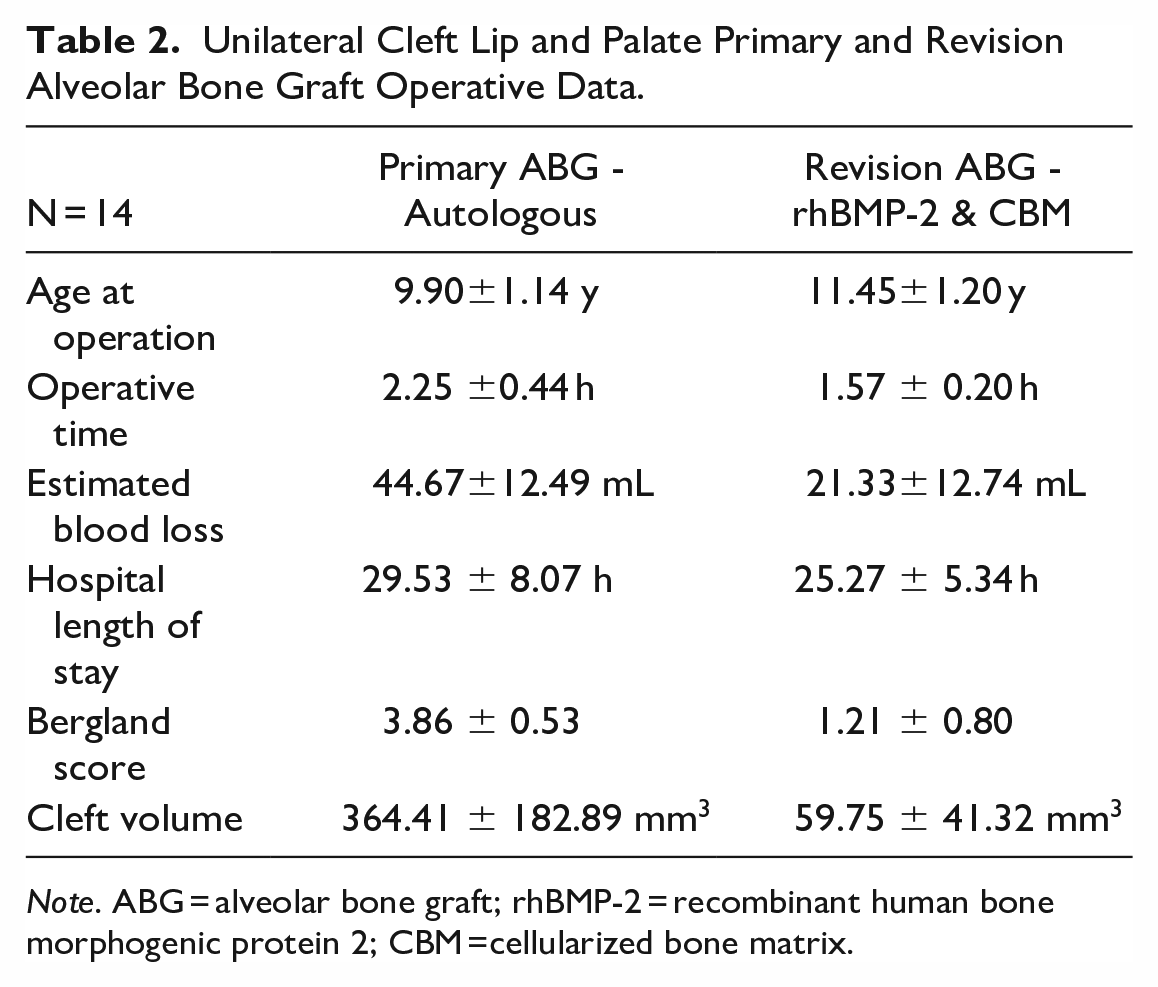
Note. ABG = alveolar bone graft; rhBMP-2 = recombinant human bone morphogenic protein 2; CBM =cellularized bone matrix.
BCLP autologous ABG and revision ABG with rhBMP-2 and CBM operative data are shown in Table 3. The age of operation was, on average, 11.30 years in revision ABG. Operative time was, on average, 3 hours in revision ABG. The estimated blood loss was 27 mL. The hospital length of stay was just over 1 day on average. The canine eruption was not interfered with, and orthodontic tooth movement was successful through graft. One patient needed surgical exposure of bilateral impacted canines due to the location, and one remained impacted due to a dilacerated root. Bergland’s scores improved from an average of 3.75 to 1.00. No significant complications were found. No patients needed re-operation following revision ABG. The cleft alveolus gap decreased by 86.73% from an average volume of 336.40 to 53.46 mm3. At the time of CBCT, the canine adjacent to the cleft had erupted in 75.0% of revision ABG.
Bilateral Cleft Lip and Palate Primary and Revision Alveolar Bone Graft Operative Data.
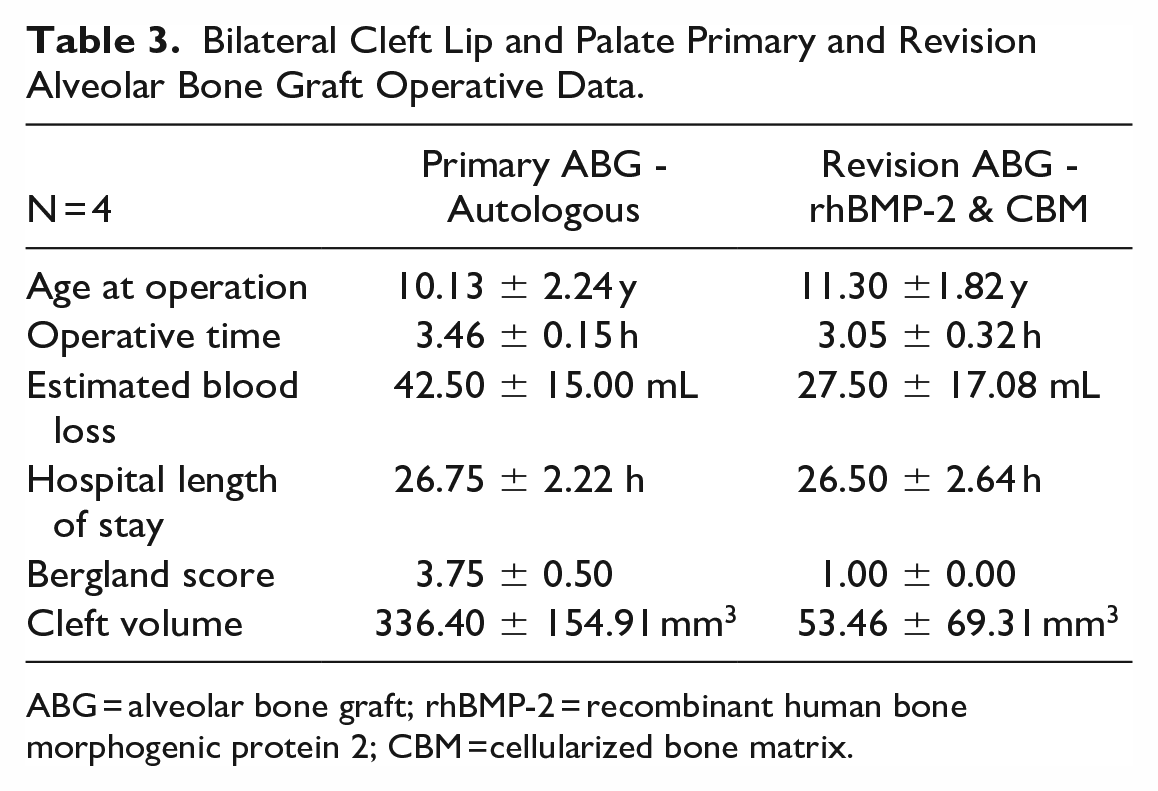
ABG = alveolar bone graft; rhBMP-2 = recombinant human bone morphogenic protein 2; CBM =cellularized bone matrix.
Discussion
ABG failure occurs when grafting does not yield sufficient bone formation to support the maxillary arch to facilitate dental eruption and provide closure of the oronasal fistula. Several factors can contribute to failed ABG, including inadequate bone grafting material, infection, or poor blood supply to the grafted area.1,17 In our study, the primary cause of failure was a bone deficiency, while graft exposure accounted for a smaller proportion of cases. ABG failure rates have been reported as high as 18% in UCLP and 32% in BCLP. 5
There is currently a scarcity of literature about revision ABG following failed ABG. Sivak et al utilized allograft bone mixed with demineralized bone matrix (DBM) for revision ABG in 11 patients with previously failed ABG. 17 They found shorter operative times, improved Enemark score, and decreased extrusion than secondary autologous ABG. However, they found decreased graft volume and complete eruption of the canine. Hammoudeh et al, in a review of autologous ABG, found that of the cleft patients who had ABG failure, on average, 2 subsequent operations were needed to close the alveolar cleft. 4 While in the rhBMP-2 and CBM technique, an average of only one revision procedure was required.
Bone morphogenic proteins (BMPs) are a group of growth factors that promote bone growth and repair. rhBMP-2, when used in alveolar bone grafting, is typically delivered in a carrier substance such as a collagen sponge used in this study. While a relatively new treatment, current literature indicates a potential benefit to the alveolar bone formation with the use of rhBMP-2. 15 Francis et al reviewed 36 patients treated with rhBMP-2 encased in DBM and found a 97.2% success rate, superior in both Bergland and Chelsea scales, and decreased infection rates compared to autologous reconstruction. 3 In a more extensive review of 258 patients who underwent ABG with rhBMP-2 and DBM by Hammoudeh et al, the results were similar to autologous reconstruction without an increase in serious complications. 4 BMPs have shown great promise in promoting bone regeneration, but more research is needed to understand their long-term effectiveness and potential risks fully.
CBM is an allograft composed of an extracellular bone matrix containing proteins and minerals essential for osteoconduction, osteoinduction, and mesenchymal stem cells (MSC) with osteogenic potential. These living MSC can differentiate into various cell types, including osteogenic lineage. 12 Currently, there are no reports of CBM being used in ABG, and it is primarily used in spinal fusion, and the limited available studies report success rates ranging from 90.2% to 92.3%. 14 In our current study, we combined rhBMP-2 in an absorbable collagen sponge with CBM. rhBMP-2 provides osteoinductive influence, but the absorbable collagen sponge provides suboptimal osteoconduction.3,18 The extracellular bone matrix in CBM has additional osteoinductive potential but also provides an osteoconductive scaffold. 12 The CBM creates increased volume to prevent the collapse of the alveolar pocket by resisting compressive forces. 3 The unique aspect of CBM, compared to DBM, is the addition of MSC, which allows for osteogenic differentiation for ideal de novo bone formation. 12
A consideration for this procedure is the cost of the rhBMP-2 and CBM. However, while the exact cost of these materials differs by institution, the cost is offset due to the reduction in anesthesia, pharmacy, and operating room costs. Previous studies have analyzed the cost involving rhBMP-2 and DBM in ABG and were found to be cost-effective due to the decreased operative time.2,3,19
The orthodontic evaluation showed successful canine eruption and orthodontic tooth movement through the graft in most patients following revision ABG. Three out of 18 patients required surgical exposure of impacted canines. This was due to the poor location and eruption path, which remained unchanged after the revision of ABG with rhBMP-2 and CBM. The Bergland score, a radiographic criterion for measuring bone graft success, showed that most patients achieved a score of 1 following revision ABG, indicating full graft uptake. However, one patient in the UCLP had complete bone graft failure resulting in a score of 4 and will need a future re-operation. No identifiable factors could indicate the cause of failure in this individual.
In our imaging analysis, volumetric segmentation of the alveolar cleft gap showed an 83.6% improvement in UCLP and an 86.7% improvement in BLCP. Previously Liang et al evaluated volumetric bone fill using CBCT in patients undergoing secondary ABG and found only 31.6% bone fill in the rhBMP-2 and DBM group and 32.5% in the autologous group. 16 A systematic review of volume improvement following ABG in UCLP showed an average of 62.0% improvement with autologous reconstruction and 68.7% improvement when using other allograft materials. 20
Our study has several limitations, primarily stemming from the small sample size. The inclusion criteria required patients to have experienced failed autologous ABG followed by revision, resulting in a limited sample of 14 UCLP and 4 BCLP patients, which restricted the statistical analysis. Another limitation is that long-term follow-up data are not available for those patients. Our average follow-up in UCLP was 1.47 years, and in the BCLP was 3.38 years. Further studies should provide larger cohorts and long-term follow-up to evaluate the effect at skeletal maturity.
Conclusion
In this study, using rhBMP-2 and CBM for ABG provides a successful approach for revision ABG in patients with UCLP and BCLP who had previously experienced failed autologous ABG. Using rhBMP-2 and CBM provided short operative time and low blood loss without complications in both groups. Most patients achieved clinical and orthodontic success following revision ABG, with all patients experiencing canine eruption. Volumetric analysis of the alveolar cleft gap showed considerable improvements, with an 83.6% increase in UCLP and an 86.7% increase in BCLP.
Footnotes
Acknowledgements
None
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
This study was approved and followed the guidelines set by the University of Texas Southwestern Institutional Review Board (STU2023-0692).
Presented at (if applicable)
None