
Abstract
Isolated frontosphenoidal synostosis (FSS) is an extremely rare pathology in which premature fusion of the frontal and sphenoid bones produces asymmetry of the forehead in a newborn or young child. If left untreated, these children may suffer significant esthetic and neurologic symptoms. Therefore, surgery is time-sensitive and necessary for correction. This report details the case of a male infant who presented to clinic at 3 months of age with unilateral, isolated FSS. Clinical features of this patient included an asymmetric forehead with flattening of the right frontal temporal area, indentation of the right temporal sphenoid area, and inferiorly displaced right orbit. Previous reports have been in older patients who were treated with open fronto-orbital advancement. With the patient’s early presentation, the primary surgical approach deployed here included anterior cranial vault remodeling with right distractor placement and fronto-orbital osteotomy. Four months following the procedure, the patient returned with increased right-sided hypoglobus and enophthalmos. CT imaging revealed a pseudomeningocele, secondary to a dural tear. Consequently, the 7-month-old underwent a second surgery, which included fronto-orbital advancement reconstruction. The child remains stable with improved forehead symmetry at 11 months of age. Due to the rare nature of FSS, treatment options are limited and traditional in their approach. This report aims to contribute additional clinical insights and treatment guidance to the growing body of literature surrounding FSS.
Keywords
Introduction
Normal neurological development is contingent on harmonious growth and expansion of the calvarium. Cranial sutures are positioned throughout the newborn skull in order to accommodate the rapidly increasing volume demand of the growing infant brain. At birth, these sutures should be patent, and continued fusion takes place throughout childhood and early adolescence. 1 However, if one or more of the sutures is prematurely fused, a sequela of cosmetic and neurological symptoms may ensue. 2
Typically discovered within the first year of life, craniosynostosis is a rare pathology involving premature fusion of one or more sutures of the cranium. The etiology may be attributable to various gene mutations with the most common being fibroblast growth factor, fibroblast growth factor receptor, and TGF-ß. 3 Although an abnormal head shape is the most salient feature of craniosynostosis, the ramifications of this condition extend beyond esthetics. The fused suture restricts bone growth in the corresponding plane of the skull. As the brain expands throughout normal childhood development, there is limited intracranial volume leading to a potential increase in intracranial pressure. Renier et al demonstrated that increased intracranial pressure is found in approximately 30% of synostotic patients, which can produce dire health outcomes if left untreated. 4 Manifestations may include sleep disturbances, headaches, nausea, vomiting, visual disturbances, and impaired cognitive development. 5
When a child is noted to have frontal bone deformity, the most likely clinical suspicions include deformational plagiocephaly and frontoparietal synostosis (FPS). Asymmetry of a child’s skull is more commonly the result of deformational plagiocephaly with an estimated incidence ranging from 5% to 46% in healthy infants.6,7 Deformational plagiocephaly often results from external, mechanical pressure on the cranium—whether through intrauterine forces, prolonged positioning after birth, or torticollis.6,8 Deformational plagiocephaly can be treated with physical or helmet therapy. 8 In contrast, frontoparietal synostosis (FPS) arises from early fusion of the frontal and parietal bones, and it is the most likely synostotic cause of frontal bone asymmetry. 2 The most common synostotic etiology for this appearance is unilateral coronal craniosynostosis. To determine whether the cause of cranial abnormality is of deformational or synostotic origin, additional clinical and radiological information are required.
A much less common cause of frontal bone malformation is isolated frontosphenoidal synostosis (FSS). Due to its extremely rare incidence, unilateral FSS is often overlooked in the differential diagnosis of an infant presenting with frontal plagiocephaly. In some cases, FPS also involves the fusion of the frontal and sphenoid bones. However, isolated fusion of the frontal and sphenoid bones is an extremely rare pathology with 53 total reported cases to date. 2
This report aims to detail the clinical features and radiologic findings of a 3-month-old infant presenting with isolated unilateral FSS, as well as describing a novel methodology for its treatment. The patient was initially treated with fronto-orbital osteotomy and distraction osteogenesis (DO). Complications arising from this primary surgical method are presented to inform future surgeons of the potential risks associated with this treatment modality with the underlying goal of expanding the current scientific literature on FSS management options.
Case Description
A male infant, born at 40 weeks’ gestation via vaginal delivery with forceps, was noted to have right frontal bone deformity. There was no family history of cranial deformities or craniosynostosis. Initial evaluations described concavity of his right frontotemporal region. CT imaging obtained in Egypt at 4 weeks of age demonstrated all sutures to be patent.
The patient presented to clinic at 3 months of age due to progressive skull bone deformity, which had worsened since birth. His mother reported he was meeting developmental milestones. Physical examination demonstrated concavity and asymmetric forehead flattening of the right fronto-temporal region, indentation at the right temporal sphenoid area, and an inferiorly placed right orbit as compared to the left (Figure 1). The patient’s anterior fontanelle was patent and non-bulging. His oculomotor movements were grossly intact. Initially, the patient did not demonstrate any chin or nasal deviation. No Harlequin sign was observed. Ophthalmologic examination did not reveal any papilledema. Informed consent was obtained for usage of all patient photos.

The patient presenting with right sided concavity in the frontotemporal region.
A repeat CT taken at 11 weeks of age revealed fusion of the right frontosphenoidal suture, with patency of the bilateral coronal sutures and left frontosphenoidal suture (Figure 2). Based on the imaging findings, a diagnosis of isolated unilateral FSS was determined.
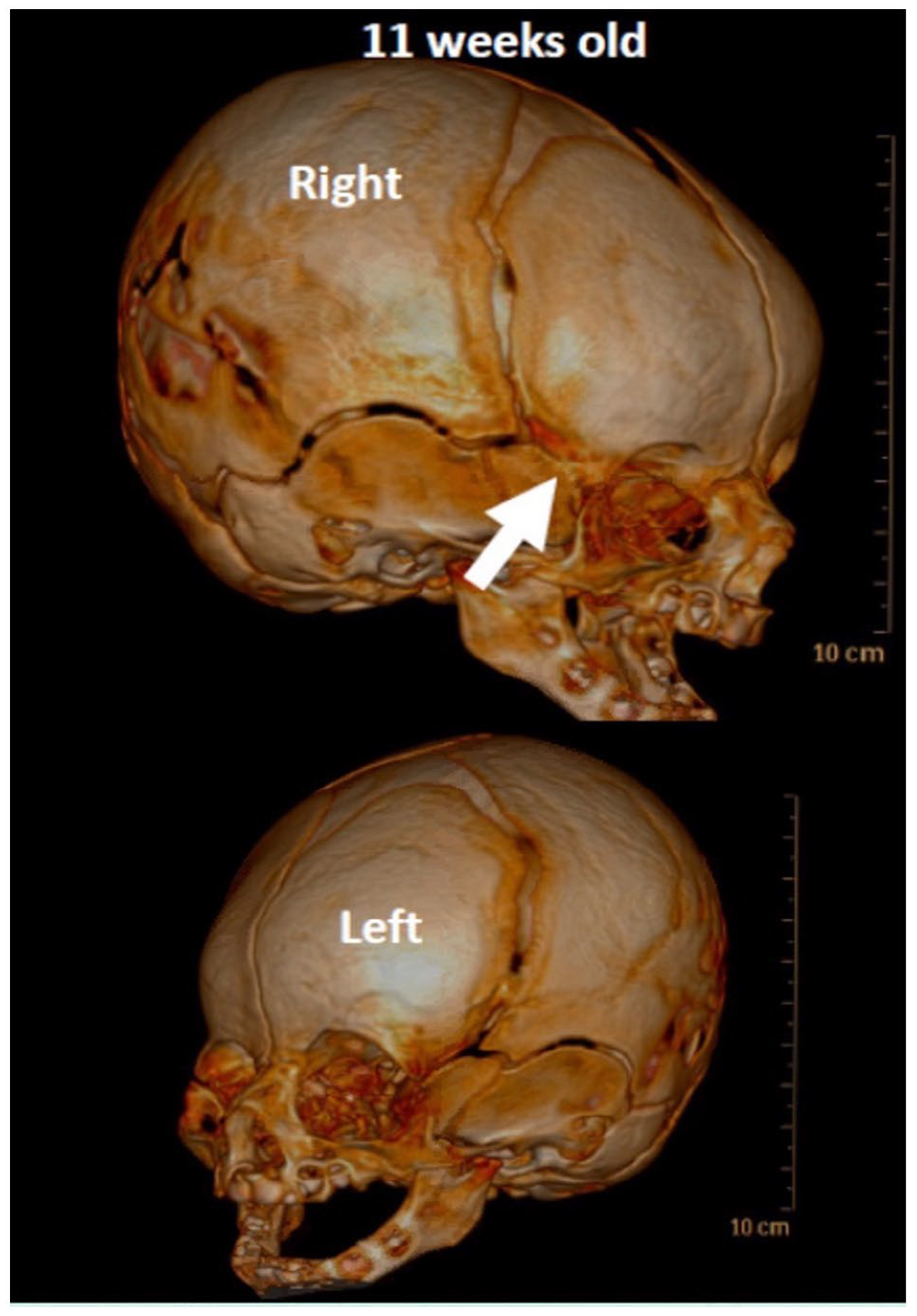
CT taken at 11 weeks of age demonstrating fusion of the right frontal and sphenoid bones. All other sutures remain patent.
Given the patient’s young age, a thorough discussion was had with the patient’s mother regarding traditional fronto-orbital advancement after 6 months old, versus a less invasive approach at this time. After carefully weighing her options, a fronto-orbital osteotomy and unilateral distraction osteogenesis was decided upon. Virtual surgical planning was used to generate 3D computerized models, and surgery took place at 4 months of age.
Osteotomies were created similar to a unicoronal distraction procedure, as previously reported. 9 However, given the differences in orbital shape and nasal deviation, a different vector was chosen, with the pivot point at the superior frontal bone at the contralateral parasagittal osteotomy. The fused fronto-sphenoidal suture was excised. A 30-mm KLS distractor device was placed to the right of the spheno-temporal area near the level of the fronto-zygomatic suture with a superomedial vector (Figure 3A and B). Horizontal barrel stave osteotomies were made on the lateral aspect of the contralateral frontal bone to decrease bony step-offs. A closing wedge osteotomy was made at the superior orbital rim to decrease the horizontal width of the orbit. There were no observable intracranial injuries, dural tears, or CSF leakage at this time. The child underwent 48 hours of latency prior to distraction activation and subsequently distracted at a rate of 1 mm/day, and rhythm of 2 turns daily. After 11 weeks of distraction and consolidation, he underwent surgery for distractor removal at 6 months of age. Upon surgical inspection, it was noted that the patient distracted approximately 25 mm with the distractor device remaining intact (Figure 4).
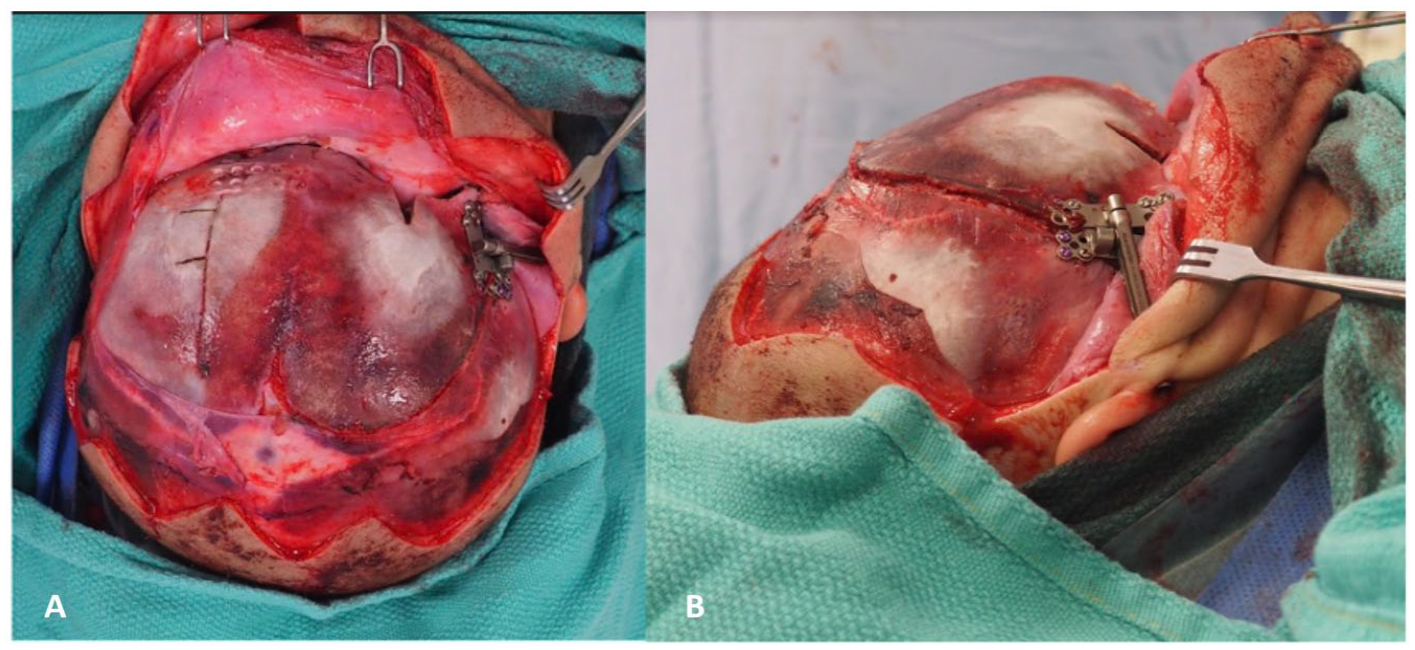
(A) Resorbable plate fixed with screws in the horizontal position on the frontal bone. (B) Distractor placed to the spheno-temporal area with a superomedial vector.
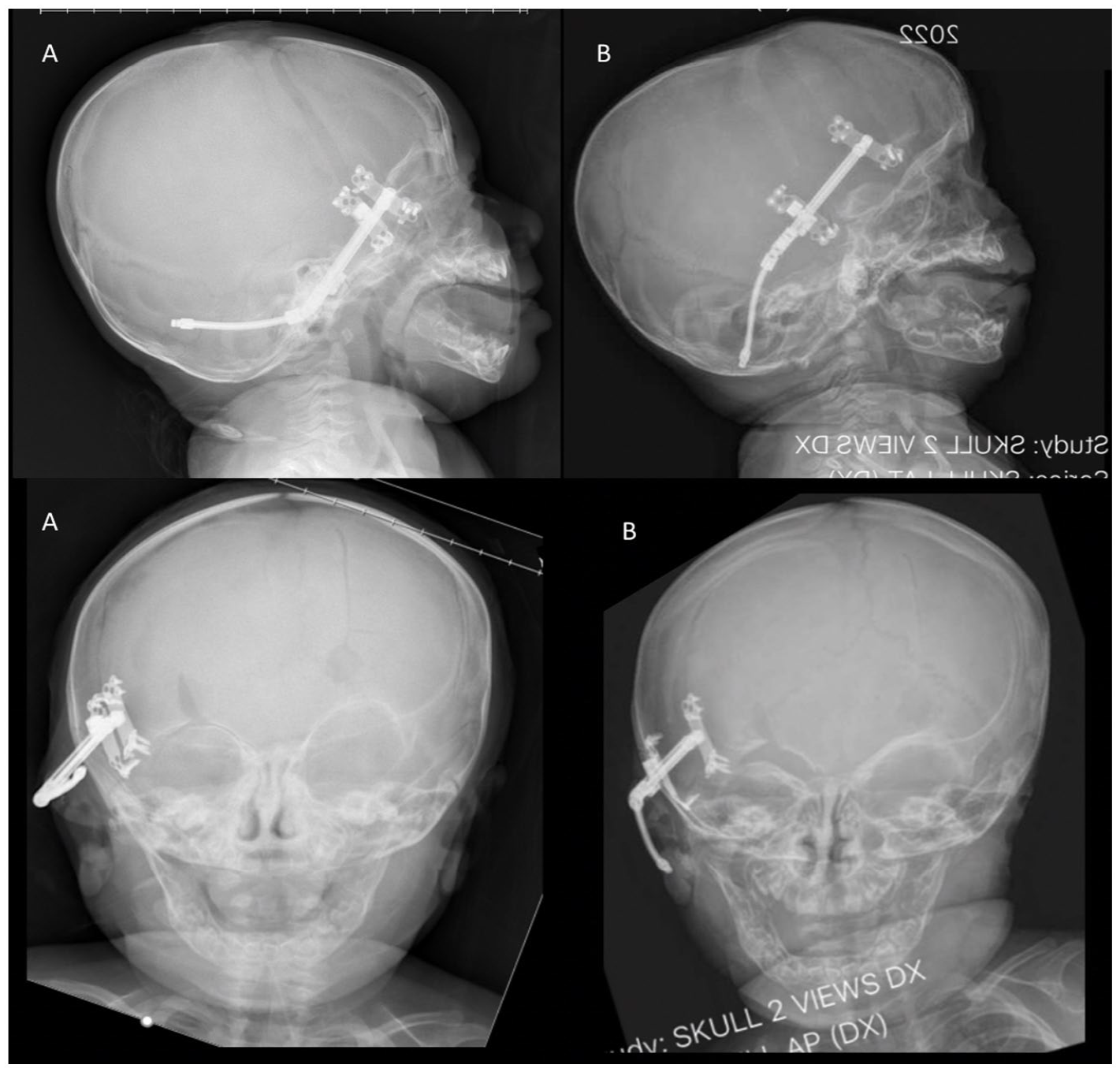
Lateral and AP radiographs of the patient at the time of latency (A) and after 25 mm of distraction (B). Note the change in orbital height and frontal bone advancement.
Four weeks after the primary operation, the mother reported continued inferior displacement of the right globe relative to the left. CT imaging revealed the patient’s right-sided hypoglobus and enophthalmos were due to a pseudomeningocele, likely the result of a dural tear during surgery (Figure 5). To relieve this complication, an open frontal orbital advancement and duraplasty was performed at 7 months of age. During the procedure, it was noted that the patient had a very thin bone at the right superior orbit combined with a bluish hue in the area, consistent with a pseudomeningocele. The dural tear measured 4 × 2 cm at the level of the frontal lobe just above the right superior orbit. The tear was repaired with a free pericranial graft and the pseudomeningocele was aspirated. The supraorbital bandeau and frontal bones were removed and reshaped ex vivo. These were then replaced into their corrected position and fixated using resorbable plates. Post-operatively, patching of the left eye was done for 30 minutes per day to prevent amblyopia and left eye preference (Figure 6).
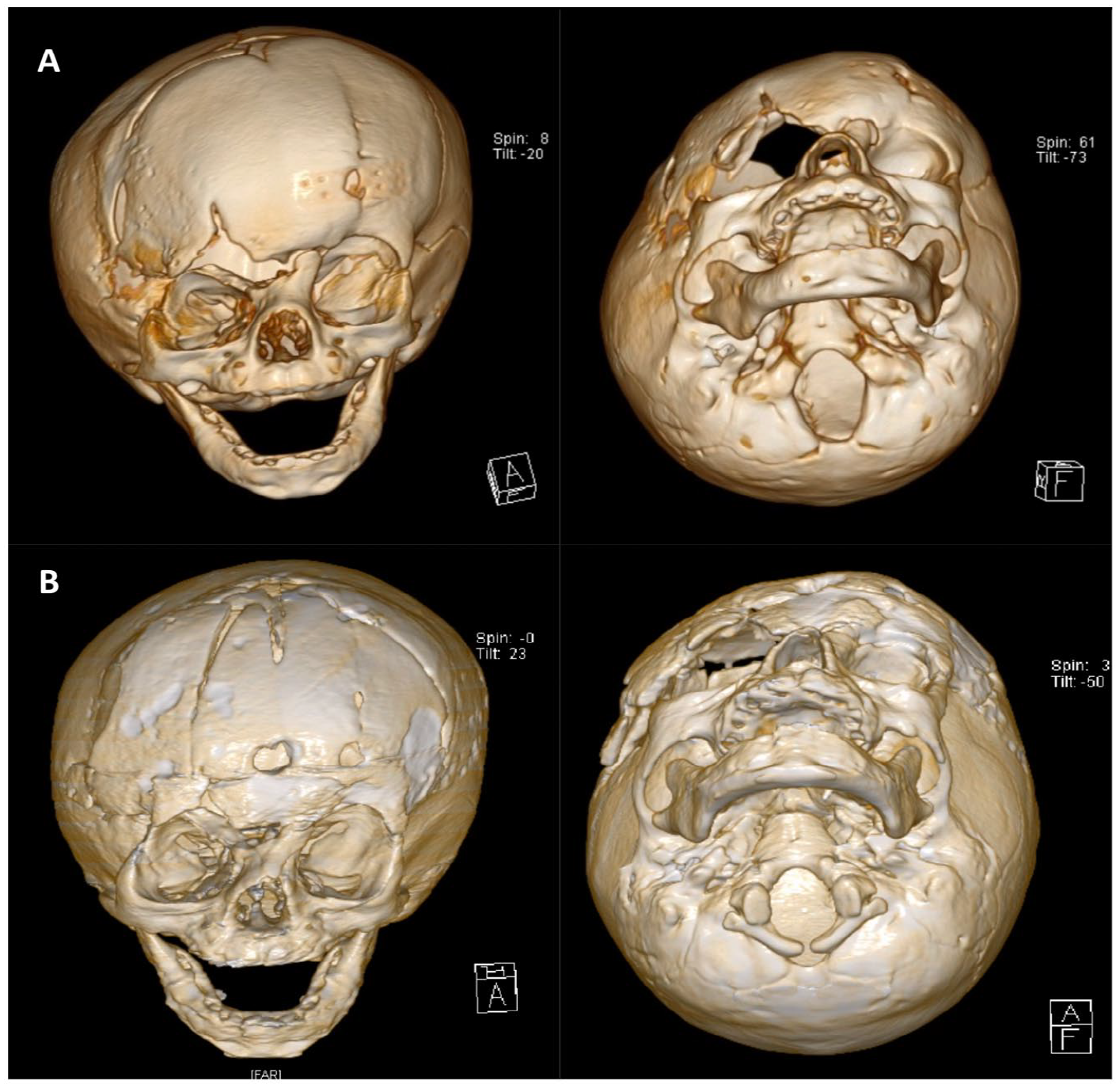
AP and worm’s eye view of patient after unilateral distraction and immediately after device removal (A) and after subsequent repair of pseudomeningocele and frontal orbital advancement (B).

Frontal view of patient following 25 mm distraction (A) and after frontal orbital advancement (B).
Three weeks following the dural repair, the patient’s mother noticed new acute inferior displacement of the globe. Physical examination revealed right hypoglobus and vertical orbital dystopia. MRI showed a recurrent meningocele displacing the right globe. Given the recurrence, the patient was brought back to the OR for exploration. Through a limited hemi-bandeau osteotomy, the orbital roof was accessed. Though a meningocele was aspirated, no clear area of CSF leak or tear was identified. A pedicled pericranial flap was inset, and a resorbable plate was placed to reconstruct the orbital roof and anterior cranial base. In addition, a lumbar drain was placed to offload CSF flow and removed at POD 5. No CSF recurrence was identified at 2-month follow-up.
Discussion
The frontosphenoidal suture lies at the lateral aspect of the skull, serving as a border between the frontal and sphenoid bones. It stretches from the anterior end of the frontoparietal suture, anteriorly and inferiorly, where it eventually meets the lateral aspect of the orbit, bilaterally. This junction remains patent from birth until about 7 years of age. 10 The frontosphenoidal suture, in conjunction with the frontoparietal, frontoethmoidal, sphenoethmoidal, and sphenotemporal sutures, make up the coronal ring. 11
FSS is known to produce a characteristic asymmetric frontal bone flattening. This phenomenon results from continued growth at the contralateral frontosphenoidal junction coupled with arrested expansion of these bones on the ipsilateral side, altogether producing obvious asymmetry. Based on the study from Hennedige et al this rare pathology consequently presents with ipsilateral frontal bone flattening, contralateral frontal bone bossing, and ipsilateral orbit downward positioning. 2 Mixed findings pertaining to the deviation of the nasal root have been reported with the majority of literature describing contralateral nasal root deviation.2,12-14
While CT is recommended to confirm the definitive diagnosis of FSS, observable clinical trends have been extrapolated from previous cases in efforts to narrow the differential diagnosis through physical exam findings alone. Similar to FPS, FSS is known to produce ipsilateral frontal bone flattening with contralateral frontal bone bossing. 15 Likewise, both synostoses have been shown to produce nasal root deviation, though the direction of this deviation is mixed in FSS patients. FPS tends to skew the nasal root ipsilaterally to the site of suture fusion.2,13 However, an important difference from FPS is an absence of the Harlequin orbit deformity. 16 Instead, FSS demonstrates inferolateral elongation of the ipsilateral orbit, as evidenced in our patient. This patient’s physical exam findings were consistent with the aforementioned frontal bone asymmetry, Though he did not initially present with nasal deviation, contralateral deviation of the nasal-frontal root became more apparent as he aged.
The suggested timeline to undergo FSS surgery varies among the literature with reports ranging from 6 to 18 months.17,18 Ruiz et al affirms that among synostotic patients, elevated intracranial pressure does not typically manifest during the first year of life, thus reducing the urgency of surgical intervention within this time frame. 5 Hence, surgical timing is determined based on the goal of improving esthetic outcome at a time that assures patient health and stability. 2 Among the current literature to date, fronto-orbital advancement reconstruction (FOAR) has been the chosen intervention for FSS treatment.
Cranial vault remodeling with FOAR usually takes place between 6 and 12 months of age. 19 This delay in intervention allows the skull bones to harden so that they may retain their shape and accommodate the internal fixation intrinsic to this approach. Furthermore, the child is larger, making them better able to physiologically withstand blood loss and stress from surgery. Drawbacks to FOAR include risk of relapse as well as longer time spent recovering in the hospital. Also, depending on the amount of advancement, scalp closure may be tight and contribute to relapse. Additionally, this approach is linked to significantly higher rates of strabismus compared to the distraction osteogenesis approach.20,21
Distraction osteogenesis (DO) typically takes place within 3 to 6 months of age. The desired time course varies among patients and is dependent upon adequate expansion of the cranial bones. In a 2009 study by Choi et al DO provided greater correction to the skull axis angulation as compared to traditional bone grafting methods. 22 Disadvantages of DO include distractor infection, multiple surgeries, or device displacement. 23 Together, the surgical team and the patient’s caregiver agreed on this surgical approach for several reasons. In comparison to FOAR, it requires less operative time, a shorter hospital post-operative stay, avoids removal and devascularization of the frontal bone, and decreases the chance of relapse.21,23 Though distraction has been described for a multitude of craniosynostosis indications, it has not been reported for FSS. As such, a full informed consent process was performed with detailed discussion of risks and benefits of this strategy with the patient’s family.
One disadvantage of DO is that it is a unilateral vector. Additionally, without frontal bone elevation, DO provides minimal visibility in the pterion area, making dissection challenging. 24 The dural tear in our patient may have had several causes including partial thickness thermal injury from the ultrasonic scalpel during the superior orbital osteotomies or distraction hardware. As there was no CSF leak identified at the initial surgery, a dynamic process may have occurred postoperatively with brain pulsation converting a partial thickness to full thickness injury or catching of the dura by the distraction screws and slow displacement. Esparza and Hinojosa demonstrate the increased risks of dural tears and CSF leaks in the distraction osteogenesis surgical technique as compared to FOAR. 24 Furthermore, issues of device malfunction and lack of visibility are eliminated in FOAR. One advantage of this patient’s course was that the distraction process acted as a tissue expander of the forehead skin, thereby eliminating tension of scalp closure during the FOAR, and potentially limiting bony relapse.
Conclusion
With its own distinct sequelae of radiologic and clinical manifestations, FSS remains a rare form of craniosynostosis. As seen in this case, distraction osteogenesis can be a useful technique, however it does have the added risk of limited visibility of osteotomies which may contribute to dural tears. FOAR may still be the primary modality of choice due to its comprehensive reshaping capability, however, this would be indicated only in children older than 6 months old. While an individualized surgical approach should be prioritized based on the patient’s anatomical morphology, this report demonstrates the feasibility of early surgery (<6 months old) using distraction osteogenesis in this patient cohort.
Footnotes
Ethical Approval
Institutional Review Board approval was not required.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.