
Abstract
Introduction
Platelet-rich plasma (PRP) is an autologous solution comprised of fractionated plasma and platelet concentrate. 1 Currently, PRP can be applied to injured tissue to promote healing and enhance repair with reported applications in orthopedic, cardiovascular, and maxillofacial surgery.2,3 When used in conjunction with autologous bone grafts, PRP has been shown to accelerate bone regeneration, increase the volume of new bone formed, and reduce negative post-operative outcomes like pain and edema.4-6 The exact mechanisms by which PRP performs these beneficial functions are not entirely understood. However, in addition to their well-established role in stimulating the clotting cascade following injury, 7 platelets are increasingly recognized to release growth factors that chemotactically attract and promote proliferation of mesenchymal cells responsible for collagen production and angiogenesis, thereby supporting tissue repair.8,9 The growth factor likely most relevant to orthopedic applications of PRP is plasma derived growth factor (PDGF), a glycoprotein derived from and concentrated in PRP that has been shown to attract and induce proliferation of osteoblasts that regenerate bone.10,11
Traditional approaches used to repair mandibular bone defects involve using either vascularized bone autografts for the primary reconstruction of larger defects, or non-vascularized bone autografts for the secondary reconstruction of smaller defects typically under 6 centimetres in length.12,13 While considered standard, bone grafting necessitates donor site morbidity and may increase the post-operative recovery period. One important advantage of using a bone substitute plus PRP composite matrix is the optimization of healing by PRP and reduction in both operative and recovery time permitted by not having to excise, prepare, and insert an autograft.
To our knowledge, this report describes the first patient described in medical literature to undergo a mandibular reconstruction procedure using only a composite matrix of PRP and cadaver-derived cortical bone chips to repair facial bone gaps larger than 1 centimetre following trauma. The reported patient is also a notable example of how mental health issues can complicate the surgical management of facial trauma, and how PRP can provide flexibility when devising various treatment plans.
Case Presentation
A 33-year-old male with schizophrenia presented to the Emergency Department of a tertiary care hospital in Toronto, Canada in June, 2017 with bilateral mandibular fractures secondary to physical assault earlier that same day. Computed tomography (CT) imaging identified a right-sided fracture involving the body of the mandible just posterior to the second molar and a left-sided fracture involving the angle of the mandible also just posterior to the second molar. The patient was to be treated with maxillary mandibular fixation (MMF) using arch bars for 6 weeks.
Due to premorbid mental health issues, including psychosis and anxiety, the patient removed the arch bars himself 1 day after discharge and did not seek medical attention until presenting to the Emergency Department approximately 6 weeks post-fracture. The patient presented at this time with malocclusion showing an anterior open bite, worsening pain, hypersalivation, oral incompetence, and a 15 pound weight loss (Figure 1). CT imaging was repeated, confirming non-union of both mandibular fractures and early signs of osteomyelitis (Figure 2). He was referred to the primary author for surgical management. The procedure was further delayed by 7 weeks due to difficulties obtaining consent and maintaining contact with the patient. Psychiatry was consulted and surgical management of his mandibular defects was deemed medically necessary to prevent life-threatening complications, including failure to thrive, aspiration pneumonia, and severe bilateral osteomyelitis of the jaw. The reconstruction procedure was performed approximately 13 weeks post-fracture.

Pre-operative occlusion 13 wk post-injury: severe malocclusion, anterior open bite, and no dental contact.
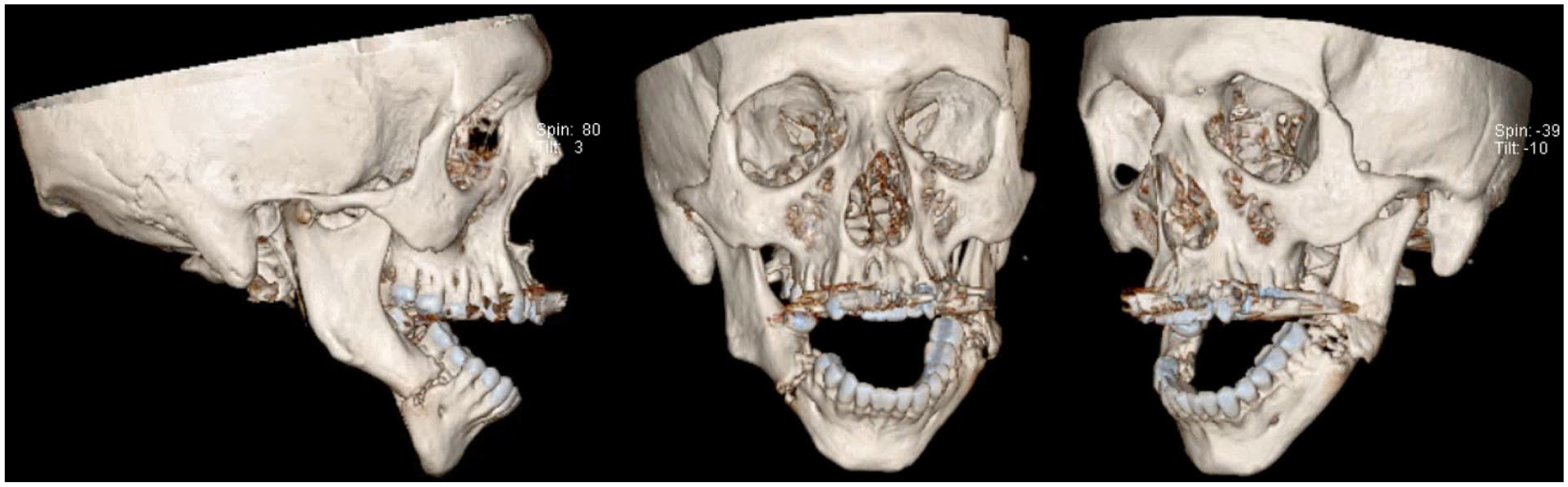
Preoperative CT showing non-union of bilateral mandibular fractures and radiological signs of osteomyelitis.
The right mandibular body and left mandibular angle were exposed using bilateral submandibular incisions. Upper and lower Rapid Hybrid MMF (Stryker) devices were applied to maintain occlusion. Significant malunion and purulence of the bone were observed at both fracture sites. The right body and left angle were then burred down to healthy bleeding bone, resulting in a 1 cm bone gap on the right and a 1.5 cm gap on the left. Once a mobile central fragment was established, MMF was achieved using a 24-gauge wire. The right mandibular body and left mandibular angle were then plated using a High Profile 2.8 reconstruction plates (Stryker) (Figure 3). Bone cultures were sent for culture and sensitivity analyses, resulting in laboratory confirmation of Coagulase negative Staphylococcus, Corynebacterium, and mixed aerobic organisms.
During the consent process, the patient refused to undergo any procedure involving a cancellous bone graft from the iliac crest or any other potential site, thereby necessitating the pursuit of alternative approaches for this unique situation. We therefore created a bone substitute solution consisting of cadaver bone chips and PRP. The PRP was retrieved using an Arthrex system, whereby 25 mL of venous blood was drawn from the patient and centrifuged. 10 mL of PRP was then withdrawn from the resultant plasma layer, resulting in PRP 2.5 times the concentration found in whole blood, as per evidence that osteoblast and fibroblast proliferation in vitro, as well as osseous regeneration in vivo, are optimized at this concentration.14,15 Approximately 5 mL of cortical bone chips was then mixed with the PRP to create a composite bone matrix for healing that was then applied to both fracture sites in equal parts. Both surgical sites were closed in a water tight fashion, and the patient was admitted to the Intensive Care Psychiatric ward for 2 weeks while in MMF (Figure 4).
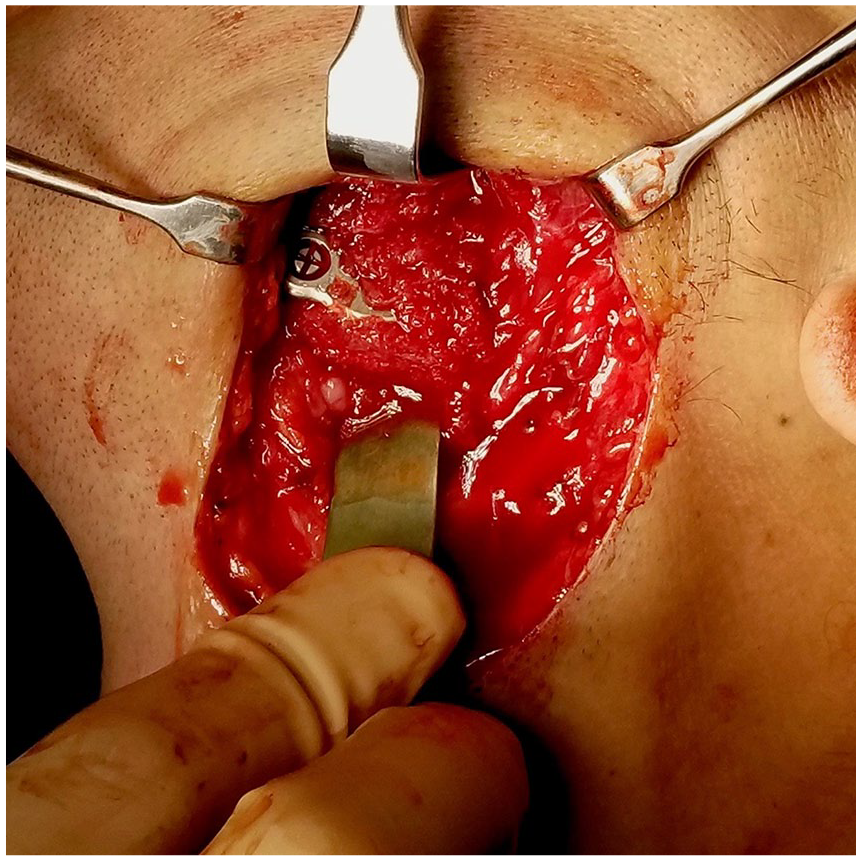
Bilateral debridement of mandibular angle. Application of reconstruction plate and grafting with PRP plus cortical bone chip solution.

Intraoperative photo after reconstruction. Normal pre-traumatic occlusion achieved.
Intravenous cefazolin and metronidazole were administered during this time. The MMF bars were removed 2 weeks following their placement, and the patient was discharged home with adequate occlusive alignment. He was given oral cefalexin and metronidazole for 4 more weeks, with weekly follow-up appointments. At 8 weeks the patient was pain free and in native occlusion. Approximately 36 months post-operatively (October, 2020), there is complete union bilaterally confirmed by CT imaging (Figure 5). The patient reports no complications and is satisfied with his repair. On clinical examination there is satisfactory occlusive alignment back to the premorbid state and structural integrity present on both sides of the mandible (Figure 6).
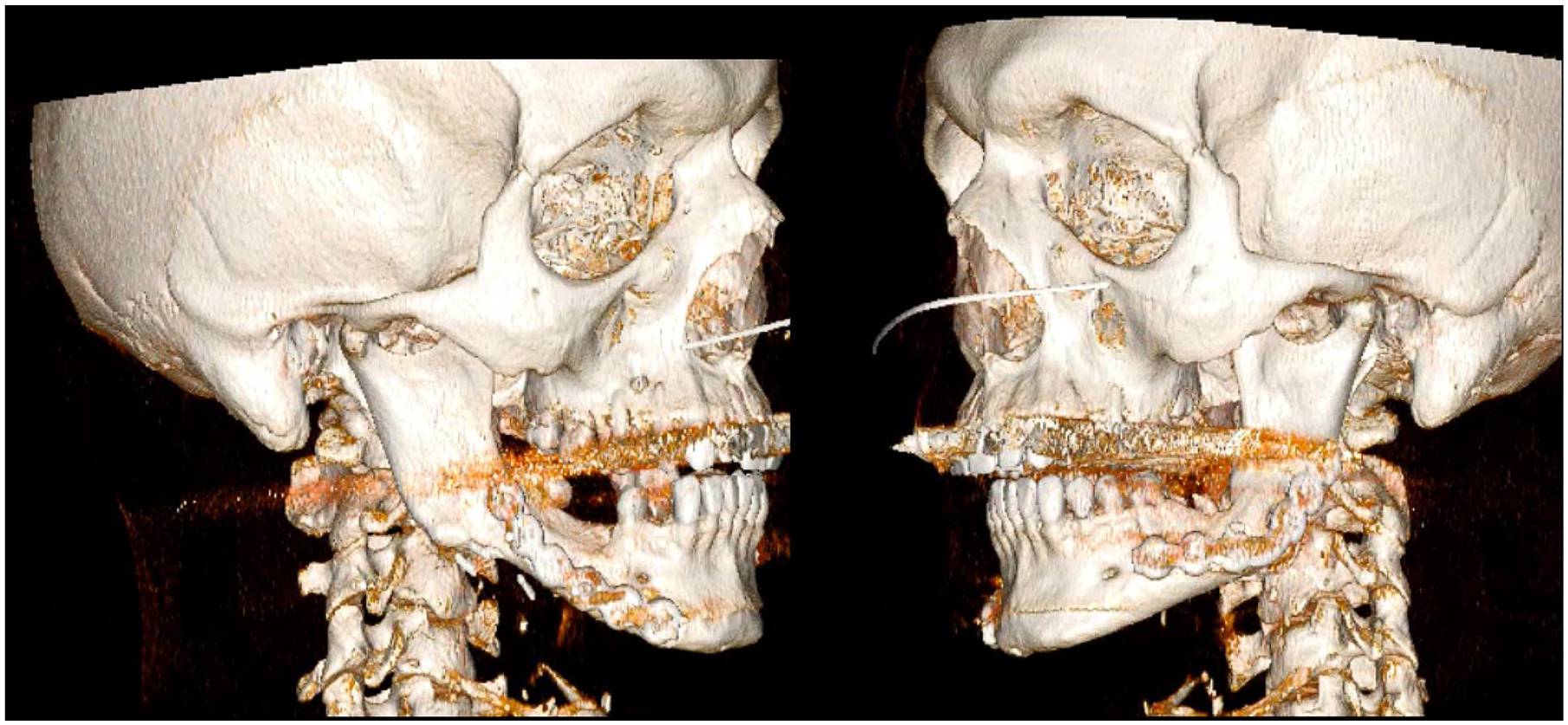
Postoperative CT showing complete union bilaterally 36 mo following procedure.

Post-operative occlusion 36 mo following procedure. Adequate occlusion maintained.
Conclusion
The use of a composite matrix comprised of cadaver-derived bone chips and PRP to span significant mandibular defects and regenerate bone tissue was successful in treating the presented case, thereby demonstrating the utility of this novel approach in repairing a trauma-induced mandibular bone defect in an individual with a complicated trajectory of treatment and recovery.
The reported and foreseeable advantages of using PRP in surgery are manifold. For one, the creation and application of this solution is straightforward and uncomplicated for the operative team to perform. Using PRP plus bone substitute also obviates the creation of additional surgical sites to retrieve donor bone grafts, thereby reducing donor site morbidity and time spent operating. Importantly, it has been shown that the benefits of PRP do not likely come at the expense of efficacy. In an unsponsored randomized clinical trial involving 20 patients with large vertical defects of the maxilla, it was demonstrated that using a composite matrix consisting of PRP and manufactured bone substitute was not only just as effective at regenerating maxilla as size-matched autografts, but that it did so with less morbidity and equal cost-effectiveness. 16
Facial trauma patients, especially those like the reported case who present with complex premorbid conditions, are likely to derive significant benefit from treatment involving a substance like PRP with demonstrated pro-healing properties. Traditional surgical management of the mandible often requires patients to spend multiple weeks with their bite maintained in occlusion—an experience that causes great discomfort for many patients, and potentially unbearable anxiety for some, including those who suffer from addiction and/or mental health conditions. This latter population is of particular interest when considering options to repair maxillofacial trauma because mental health conditions and substance use disorders are demonstrated risk factors for trauma to the viscerocranium.17,18
Anti-microbial and immune-boosting effects are also benefits of PRP reported in the literature. In vitro, certain autologous formulations of PRP have been shown to inhibit the growth of Staphylococcus aureus and Psuedomonas aeruginosa, among other bacterial strains. 19 Additionally, PRP applied in vitro to peripheral blood monocytes has been demonstrated to encourage the differentiation of these precursor immune cells into anti-inflammatory cell types thought to optimize wound healing. 20 In rabbit models of tibial osteomyelitis, locally injected PRP plus intravenous antibiotics were shown to be more effective than antibiotics alone at reducing bone destruction and increasing bone formation. 21 For sternotomy wound infections in humans, prophylactically applied PRP was shown to be associated with a significant decrease in the incidence of deep and superficial sternal wound infections. 22 Overall, given that PRP has been shown to stimulate angiogenesis and increase pro-inflammatory cytokines via PRP-derived proteins, it is theorized that PRP may promote healing in the context of osteomyelitis by attracting immune cells and facilitating access to infected, necrotic tissue. 23
The findings of this case report must be interpreted in the context of its limitations. The presented case report does not allow for generalizations or conclusions about the efficacy of this approach over standard approaches to be made. However, this case report remains valuable because the described approach was successful in achieving functionally and clinically satisfactory outcomes in a patient for whom traditional bone gap spanning approaches were unfeasible. It is also the first reported case of multiple trauma-induced mandibular bone defects repaired using a matrix made only of bone substitute and PRP, making for a notable example of how PRP may provide flexibility when devising various treatment plans for surgical management dilemmas.
Future directions regarding the efficacy and success of PRP in maxillo-facial surgery should be pursued in the form of non-case report research formats. The details of which patient profiles and centers would benefit from the implementation of this technique is currently unknown. Additionally, the size of mandibular gap repairable using this technique is unclear. Case series, chart reviews, prospective cohort studies, or a randomized control trial comparing recovery time, complication rates, and the cost of PRP plus bone substitute versus other treatment modalities, all make for logical next steps.
Footnotes
Patient Consent
The authors have received informed written consent from the patient to reproduce the presented case report and associated images.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.