
Abstract
It is unclear which psychosocial factors explain individual differences in seeking primary, secondary, and tertiary care, and under which conditions. The current work integrates the study of personality and health care into existing theoretical models to determine extent to which traits can be used to understand who seeks health services. Using data from the Health and Retirement Study (N = 14,358, with 141,401 distinct measurements), multilevel logistic models were used to estimate the likelihood of using health services from known correlates of healthcare utilization (age, self-rated health, and diagnosis of chronic conditions), personality traits, and the interaction of these domains. Independent of health status, traits were associated with the use of health services. Little evidence of moderation was found, although chronic conditions strengthened the association between conscientiousness and seeking health care. These results suggest that personality traits may influence health beyond simply affecting the need for health services.
Keywords
Introduction
In the United States, lack of health insurance used to be the primary determinant of health care utilization. Less than a decade ago, having health insurance increased the likelihood of seeking health care by a magnitude of seven, even among those with chronic conditions (CDC, 2010; Smulowitz et al., 2014; Taubman et al., 2014). However, since the implementation of the Affordable Care Act, health insurance plays a smaller role in the decision to seek health care. Since the passage of the ACA, the percentage of uninsured adults in the United States has dropped from 17% to 12.5% (Collins et al., 2019), although that number rose to 13.5% by 2021 (Cohen et al., 2022). Given that having insurance is a smaller determinant in the decisions to seek health services, other contributing factors, including psychosocial factors, become more consequential. Of particular interest for the current study are individual differences in temperament and behavior: personality.
When focusing on the role of psychosocial individual differences in the pursuit of care, it is necessary to acknowledge that the reasons for seeking care likely differ across the many types of healthcare services one might seek. For example, individuals will seek hospital services, regardless of resources, if they are experiencing an emergency (Gelberg et al., 2000). On the other hand, patients make regular doctor’s appointments only if they are able to afford them (Kenney et al., 2012). By assessing multiple services, it is possible to examine how personality traits impact primary care (i.e., stopping illnesses before they can begin), secondary care (i.e., bringing a sick patient back to health), and tertiary care services (i.e., managing long-term illness) in different ways (Andersen & Newman, 2005). In the current study, we made use of data that tracks the pursuit of multiple healthcare service types by a large number of individuals over many years, allowing us to model within-person variability of health care utilization and health needs. Before detailing the aims of this research, we first summarize prior research in this area, including both empirical findings and theory.
Why do People Seek Health Care?
There are many factors that lead individuals to seek healthcare. Commonly, these factors are organized into three categories: personal characteristics, enabling resources, and need (Andersen, 1968, 1995, 2008). Personal characteristics represent predisposing characteristics that are not specific reasons for individuals to seek health care but instead lead to changes in resources and needs. These factors include psychosocial factors such as social support (Hastings et al., 2008; Knowlton et al., 2005), demographic factors like age, sex, and education (Lodi-Smith et al., 2010), as well as health beliefs (Pachter, 1994), and social structures (Evans & Kantrowitz, 2002). Enabling resources are those factors that influence access to healthcare, such as health insurance. Need factors encompass both a physical need for services (one’s objective or subjective health) and a perceived need. Importantly, need greatly outweighs resources when it comes to HCU. Homeless individuals will seek out health care when they experience severe illness, despite being unable to pay for those services (Gelberg et al., 2000). Since the passage of the ACA, United States citizens have received more resources in the form of better access to health insurance. There is evidence that the expansion of health care coverage will additionally reduce the relative impact of other resources, such as wealth. For example, in Ontario, where healthcare is universal, evidence suggests that HCU is relatively unrelated to income (Finkelstein, 2001).
As noted by Andersen (1995), perceived need is informed by social context. One’s perceived need for health care may be informed by one’s values, fear for one’s safety, the priority of health among other life domains, and family history. Perceived physical need may not correspond with physical need. For example, someone experiencing a panic attack may believe they need care in an emergency room, but they do not; conversely, some deny needing care even when exhibiting signs of an infection. The latter example is less common, as patients with inaccurate health perceptions use more healthcare resources than patients with better perceptions (Connelly et al., 1989).
Relationships Between Personality and Health
Personality traits should be considered primary predictors of healthcare utilization (HCU) because of their consistent association with health, health perception, and other important life outcomes (Bleidorn et al., 2019; Roberts et al., 2007). Traits are broadly defined to include a wide variety of relatively stable (at least in the short- and medium-term) individual differences in thoughts, feelings, and behaviors. While dozens of personality traits have been identified, most personality and health psychologists commonly describe personality broadly using the Big Five taxonomy of traits (Goldberg, 1992). They are defined by neuroticism (characterized by strong negative reactions to stressors, as well as anxiety and depressive tendencies), agreeableness (e.g., compassion, warmth, and friendliness), openness (e.g., openness to new experiences, intellect, creativity), conscientiousness (e.g., self-discipline, industriousness, responsibility), and extraversion (e.g., sociability, positivity, activity). The use of the Big Five framework allows for a broad measurement of personality that is predictive of significant life outcomes (Ozer & Benet-Martínez, 2006).
Traits have been linked to health outcomes such as overall physical health describing dynamics of personality states (H. S. Friedman et al., 2010; Kern et al., 2014; Turiano et al., 2012bTuriano, Pitzer, et al., 2012), health behaviors (Bogg & Roberts, 2004; Turiano et al., 2012aTuriano, Hill, et al., 2012), specific disease onset (Goodwin & Friedman, 2006; Weston et al., 2015), and mortality (Graham et al., 2017; Jokela et al., 2013). Traits are also linked to the perception of health (Costa & McCrae, 1987; Watson & Pennebaker, 1989). In other words, traits predict who becomes ill, what they become ill with, and how they perceive that illness. The links between personality and health outcomes have generated interest in utilizing personality as a sort of psychological vital sign (Condon et al., 2017; Israel & Moffitt, 2014).
Given this, personality traits should also predict HCU; that is, if traits predict who becomes ill or who perceives themselves as ill, it seems tautological that personality is linked to healthcare utilization. Only a few recent studies have examined this relationship empirically, however. Findings by Chapman et al. (2009), for example, suggest that insured, older adults higher in extraversion and lower in agreeableness are much more likely to use emergency services. In this study, traits predicted healthcare utilization over and above income and education (i.e., over and above the resources available to them). Similarly, a Swedish-based study found that among older adults, individuals with higher neuroticism and lower activity were more likely to have been hospitalized in the last 12 months (Hallgren et al., 2016), and that evidence was not found for these effects among middle-aged adults. This suggests that the effects of personality on healthcare utilization may differ over the life course, at least in magnitude. It may be that personality traits play a larger role as people age, perhaps driven by a greater need for health care in older adulthood. Finally, a recent coordinated analysis found associations between health care utilization and traits of conscientiousness and neuroticism, although the direction of these effects was mixed across services (Willroth et al., 2023). In terms of more specific health care, personality traits have been studied among those discharged from the emergency department: few associations between broad traits were found, although participants who report being high on the item “responsible” were more likely to follow up with a physician, refill a prescription, and not return unexpectedly to the emergency room (Atherton et al., 2021). Cancer screeners are positively linked to traits conscientiousness, extraversion, and neuroticism (Aschwanden et al., 2019).
While these studies have begun to broadly sketch out the relationship between traits and HCU, important details have yet to be filled in. First, it is unknown which health services are predicted by personality traits. Healthcare utilization extends far beyond emergency rooms and hospitals, encompassing a large number of services, including routine checkups, dental care, and elective procedures. In the same vein, not all health care is responsive. Some forms of HCU are preventive in nature. These are arguably more important to examine, as they are to a larger extent elective and more likely to be predicted by psychosocial factors. Second, it is crucial to identify the mechanisms that link personality to healthcare utilization. Possibly, the effect of personality is entirely due to differences in health behaviors. That is, traits may lead some individuals to become more ill than others due to avoidance of healthy behaviors or the pursuit of unhealthy ones. It is possible that this is the only pathway through which personality is associated with health. On the other hand, it may be that personality influences HCU above and beyond differences in health behaviors, implying that personality is associated with HCU through other (additional) pathways. Research on this second concern is especially relevant to the potential development of targeted interventions that encourage the efficient use of health care services (Hagger-Johnson & Pollard Whiteman, 2008; Mroczek et al., 2020).
Pathways From Traits to HCU
We propose that personality traits may impact HCU through three pathways: (1) directly, or independently of health factors, (2) through physical need, and (3) through perceived need. First, personality traits may have a direct association with HCU independent of health states or perceived need. This is to be expected, given the role of other personal characteristics on HCU, including demographic factors and other psychosocial traits. For example, parent traits predict seeking pediatric care (Weston et al., 2021), an association which cannot occur because of the health needs of the person making decisions.
Second, personality traits may influence HCU by directly influencing physical health or health states. Traits (particularly, conscientiousness, openness, and neuroticism) are associated with both objective health (Goodwin & Friedman, 2006; Weston et al., 2015) and subjective health (particularly neuroticism) (Costa & McCrae, 1987; Löckenhoff et al., 2008; Watson & Pennebaker, 1989). Thus, there is reason to believe that the associations between personality traits and HCU can be at least partially explained through health.
Third, personality traits may influence HCU through perceived need, or via the threshold at which someone seeks care. Recent attempts to predict health outcomes from personality traits have suggested that personality traits manifest in response to events or situations (Fleeson, 2004; Weston & Jackson, 2016). In other words, the strength of the relationship between utilization and need factors will vary as a function of personality. Some individuals will seek out medical services, for example, when they low levels of need (mild, intermittent stomach pain); others will resist seeking health care even when facing a debilitating chronic disease, like cancer. The threshold of health severity at which an individual seeks out medical services may be moderated by their personality. For example, those high in neuroticism may be more likely to interpret a somatic symptom as being worse than it is (e.g., Larsen, 1992), while those low in neuroticism may not take conditions like high blood pressure seriously enough. To be clear: this moderation would represent the influence of personality on HCU through perceived need. That is, the slope of HCU on health represents perceived need (the threshold of ill-health at which one seeks care) and this would be associated with personality. Thus, we propose that personality traits may influence HCU by changing the relationships between health and health care services.
Older Adulthood
An important context to consider the role of personality traits is that of older adulthood. In general, older adults use more health care services than younger adults (Nie et al., 2008), although there is evidence that the oldest adults decline in HCU (Vegda et al., 2009). Given that this population poses the greatest stress on the health care system – and is growing in the United States (Centers for Disease Control and Prevention (CDC), 2003) – it is especially important. In addition, pathways from traits to outcomes, particularly health, change across the lifespan (Shanahan et al., 2014). For example, trait conscientiousness may have stronger effects in younger and middle adulthood, when this trait predicts avoidance of risky behavior and life choices (career, spouse) that directly impact the ability to receive healthcare. Conversely, in older adulthood, conscientiousness may have a smaller impact on health due to processes like biological senescence and general population maturation.
The Current Study
The current study aims to incorporate personality traits and health status into a single model predicting HCU. We build on previous models that independently demonstrate that need (Andersen, 1995) and personality (Chapman et al., 2009; B. Friedman et al., 2013) predict healthcare utilization among older adults. In doing so, we hope to clarify how personality and health are interrelated in the prediction of HCU. Specifically, we seek to answer two questions.
First, are personality and health status independent predictors of HCU? If so, we would conclude that personality traits predict HCU at least partially through non-need mechanisms. We predict that they are independent and, more specifically, that conscientiousness is associated with the utilization of preventive health services (i.e., doctor and dentist visits). For example, a healthy person high in conscientiousness has no immediate need to see a doctor but may schedule a check-up as part of routine health maintenance. In this study, we measure physical need using two markers of health: chronic conditions and self-rated health. Both captures chronic experiences of health, although from different perspectives.
Second, do personality traits predict perceived health need? To test this question, we examine the degree to which personality traits moderate the within-person relationship between health need and HCU. That is, we operationalize perceived need as the relationship between health and HCU. This allows us to determine whether someone’s perceived need for health care is (or is not) associated with their experience of their health, either measured through chronic conditions or through self-rated health. Some people schedule a doctor’s appointment at the first sign of a cold. Others refuse treatment, even when managing serious and chronic health conditions, like emphysema. We predict that more conscientious individuals will show a weaker relation between health needs and HCU; that is, we expect less conscientious individuals will require worse health or more need (in terms of chronic conditions and/or self-rated health) in order to seek health services. While neuroticism is commonly associated with both health and psychosomatic experiences, these findings are mixed enough to allow for compelling arguments in either direction. For that reason, we make no specific predictions about neuroticism here.
We note here some limited overlap with a recently published coordinated data analysis examining the associations between personality traits and use of dental care, general medical practitioners, and hospitals, which included the HRS among its samples (Willroth et al., 2023). Our study expands on these analyses in the following ways: First, we test additional health care services, including prescription medications and special facilities. Second, we examine effects longitudinally, whereas previous work was cross-sectional. Third, we test personality as a potential moderator of the within-person health-HCU relationship.
Methods
Participants
Data were taken from the Health and Retirement Study (HRS; Servais, 2010), a national longitudinal study of aging adults. Data were collected in two-year waves, starting in 1992 and most recently in 2018 (at the time of analysis). Participants entered the survey at various times between 1992 and 2010. See the HRS website (https://hrs.isr.umich.edu/) for more information about participant entry. At entry in the study, participant ages ranged from 24 to 89 (M = 56.37, SD = 7.72). Participants were excluded from these analyses if they provided fewer than 5 waves of data or if they did not complete any of the 2010, 2012, 2014, 2016, or 2018 psychosocial questionnaires, which included the measures of personality. Participants were ensured at 92% of all occasions, likely because most were eligible for Medicare. Such high insurance rates limited our ability to test for the influence of insurance status on health or personality. As a result, specific measurement occasions were excluded if the participant did not report having health insurance on that occasion.
The final data set thus consisted of 14,358 participants (59% female) who provided between 5 and 13 waves of data, for a total of 141,401 distinct measurements. These participants were mostly white (79%). Participants received an average of 12.91 years of education (SD = 3.02). At the time they completed the personality assessment, participants were on average 69.01 years old (SD = 10.83) and 64% reported having a spouse or partner. Partnership status was measured at each wave, and was included as a covariate along with age, race, gender, and education.
We note that the authors of this manuscript do not have permissions to broadly share these data. However, these data are publicly available upon registration with the Health and Retirement Study, and so readers can reproduce these findings. All code used to analyze the data are presented in the supplemental file.
Measures
Outcome: Health Care Utilization (HCU)
The outcome of interest was the use of various health care services among adults in the HRS. At each wave of data collection (i.e., every two years), participants were provided a list of health care services and asked whether they had used each service at least once since the last wave. These services included: (1) seeing a dentist for dental care, including dentures; (2) seeing or talking to a medical doctor (excluding emergency room or clinic visits); (3) being a patient in a hospital overnight; (4) regularly taking prescription medications; (5) having outpatient surgery; or (6) using a special facility or service including adult care centers, appointments with social workers, outpatient rehabilitation, or transportation or meals for the elderly or disabled. In an average year, 68% of participants had seen a dentist, 93% had seen a medical doctor, 21% had stayed overnight in a hospital, 77% were taking prescription medications, 20% had one or more outpatient surgeries and 9% had used a special facility or service. Supplemental Figure 1 displays the usage rates for each service across the study.
Predictors: Health
Two measures of health were used as year-level predictors: the number of chronic conditions a participant had been diagnosed with at the time of the interview and the participant’s self-rated health. Chronic conditions were assessed with a series of questions, all starting with the frame, “Has a doctor ever told you that you have….” The conditions assessed were high blood pressure or hypertension; diabetes or high blood sugar; cancer or a malignant tumor; a chronic lung disease, such as chronic bronchitis or emphysema; a heart attack, coronary heart disease, angina, congestive heart failure, or other heart problems; a stroke; and arthritis. Of all participants, 14,288 (92.7%) had at least one chronic condition during the study. On average, participants had 1.85 chronic conditions (SD = 1.44).
Self-rated health was assessed using a single item: “Would you say your health is excellent (5), very good, good, fair, or poor (1)?” At the time of personality assessment, participants rated themselves an average of 2.81 (SD = 1.06).
Predictors: Personality Traits
Personality assessments were included in a psychosocial leave-behind questionnaire, a packet of questions left with participants to be returned by mail. This questionnaire was administered to one cohort (N = 7424) of participants in 2010, 2014, and 2018; it was administered to a second cohort (N = 6446) in 2012 and 2016. The remaining participants received the questionnaire in 2014 (N = 872), 2016 (N = 560) and 2018 (N = 118). (We note that the personality measure was also administered in 2006 and 2008; however, this version of the measure included fewer items and worse reliability. We opted to use only the personality assessments that included the more reliable measure for this study.)
While personality was assessed at multiple waves, using personality traits as a Level 1 variable would necessarily limit our data to only those waves during which personality traits were observed (between one and three observations per participant). However, if we choose to treat personality as a Level 2 variable, we are able to incorporate all observations of health and HCU for each participant (up to 13 observations per participant). Treating personality as a Level 2 variable assumes personality is stable across the four to eight years between assessments. Given prior work on personality change over the lifespan (e.g., Graham et al., 2020a; Roberts & Mroczek, 2008), we feel confident that personality traits change is relatively small during this developmental stage and, even in the case of larger changes, the benefit of examining changes in health across two decades outweighs the limitations of assuming personality stability. We chose to use each participant’s first assessment of personality as their Level 2 personality score.
The personality assessment administered was the MIDI, a 26-item adjective scale, in which participants are asked to report how well each adjective describes them on a scale from 1 (Not at all) to 4 (A lot). Extraversion was the average response to the items “outgoing,” “friendly,” “lively,” “active,” and “talkative” (M = 3.17, SD = 0.57, α = .75). Agreeableness was the average response to the items “helpful,” “warm,” “caring,” “softhearted,” and “sympathetic” (M = 3.50, SD = 0.50, α = .78). Conscientiousness was the average response to the items “organized,” “responsible,” “hard-working,” “careless” (reverse scored), and “thorough,” (M = 3.56, SD = 0.42, α = .72). Neuroticism was the average response to the items “moody,” “worrying,” “nervous,” and “calm” (M = 2.01, SD = 0.62, α = .71). Openness was the average response to the items “creative,” “imaginative,” “intelligent,” “curious,” “broadminded,” “sophisticated” and “adventurous” (M = 2.91, SD = 0.58, α = .80).
Data Analysis
Multilevel modeling was used to estimate the relationships between health, personality, and health care utilization. Measurements (Level 1) were nested within person (Level 2). Before incorporating personality traits into the models, we first created a set of baseline models in which we regressed health care use onto health (number of chronic conditions, average self-rated health, and within-person centered self-rated health) and demographics (age at the time of personality assessment, race, gender, and education). We allowed for varying intercepts -- allowing individuals to vary in how much they seek health care in general -- and varying slopes for both chronic conditions and self-rated health (within-person centered) -- allowing individuals to vary in how much they modulate health care as a function of changes in their health. Thus, the baseline models have the formula:

To address whether traits were associated with health care above and beyond health, we added personality traits as Level 2 predictors to the above model. Given the substantive correlations between the Big Five traits, incorporating all as predictors in a single model increases the likelihood of multicollinearity among predictors and potentially washes out valuable effects. As a result, we estimated one model for each combination of health care service and personality trait. However, we also present the correlations between traits and note potential overlapping effects in the discussion section.
Finally, to address whether personality traits are associated with the relationship between health and health care, we added one term to each of the personality models estimating an interaction between the person-level trait and the varying slopes (relationship of health care to both chronic conditions and within-person self-rated health). We used R (Version 4.2.1) (R Core Team, 2021) and the R-package lme4 (Version 1.1.30) (Bates et al., 2014) for these analyses. For all analyses, we use p < .01 as the threshold of significance.
Results
Correlations Between Study Variables.

Note. Correlations greater than .01 in absolute value are significant at the .05 level. Correlations greater than .02 in absolute value are significant at the .01 level.
The bottom section of Table 1 shows the within-person correlations, using the within-person centered variables. These results mirror the between-person correlations: in years when participants use more of one service, they are more likely to use other services. When participants are less healthy than average (more chronic conditions, worse self-rated health), they are more likely to seek health care. Again, dental services display the opposite pattern to other services.
Are Personality Traits Associated with Health Care Utilization Above and Beyond Health Factors?
Relationship of Personality Traits to HCU Above and Beyond Demographic Variables and Health.
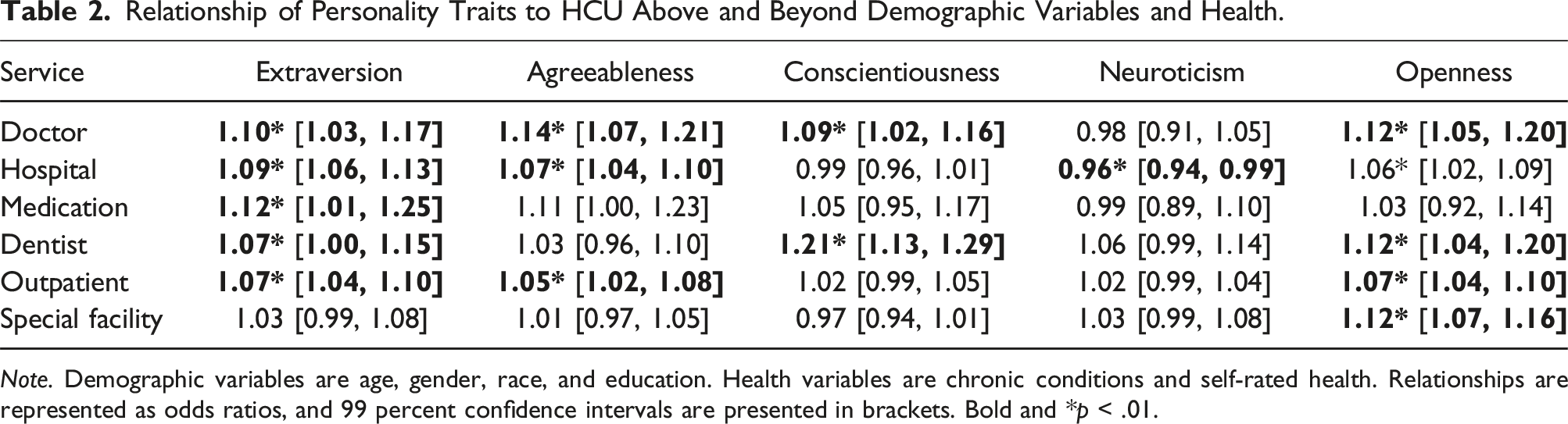
Note. Demographic variables are age, gender, race, and education. Health variables are chronic conditions and self-rated health. Relationships are represented as odds ratios, and 99 percent confidence intervals are presented in brackets. Bold and *p < .01.
Extraversion and openness had the greatest number of associations with HCU. Extraversion was associated with a greater likelihood of using all services except for special facilities, and openness was associated with a greater likelihood of using all services except medication. Effect sizes were modest, with odds ratios between OR = 1.07 (dental and outpatient procedures) and 1.12 (prescription medication). Similarly, openness was associated with greater odds of OR = 1.06 (hospital) and 1.12 (dentist) of using services. Agreeableness was also consistently associated with HCU. Individuals high in agreeableness were more likely to use outpatient (OR = 1.05), hospital (OR = 1.07), and general practitioner services (OR = 1.14).
Surprisingly, conscientiousness was only associated with greater use of general practitioner (OR = 1.09) and dental (OR = 1.21) services. Neuroticism was only associated with lower odds of seeking hospital services (OR = 0.96).
Do Personality Traits Moderate the Relationship Between Health Factors and Health Care Utilization?
Tests of Moderating Effects of Objective and Perceived on the Relationship Between Traits and HCU.

Note. Objective health is measured by number of chronic conditions, and perceived health is measured with self-rated health, within-person centered. Each coefficient is the odds ratio effect size of the interaction term and indexes the degree to which the personality-HCU relationship changes as a function of increases in the moderator. Brackets contain 99% confidence intervals and bold/* indicate p < .01.
Conscientiousness and neuroticism moderated the relationship of chronic conditions to health care utilization. More conscientious individuals were expected to have stronger relationships between chronic conditions and outpatient and special facility services. Conversely, individuals higher in neuroticism had weaker relationships between chronic conditions and hospital services, medication, and the use of special facilities. These relationships are plotted in Supplemental Figure 3.
While extraversion, openness, and agreeableness were consistent predictors of health care utilization in the prior models, they were unassociated with the relationships between health and HCU. No traits moderated the relationship between perceived health (within-person self-rated health) and HCU after controlling for chronic conditions.
Exploratory Analyses: Does Personality Relate to HCU More (or Less) in Older Adulthood?
During peer review, it was suggested that the relationship of traits to HCU may be impacted by age, especially noting that adults aged 65 and older are eligible for additional social services in the United States. We refit the models testing the independent association of personality to HCU by adding age, dichotomized at age 65, as a moderator of personality. These results are presented in Supplemental Table 11. Age did significantly moderate several associations (7 of 30 tested). A consistent pattern was that personality predicted greater medication use in younger adults but less medication use (or no association with medication use) in older adults for all traits except neuroticism). A second consistent pattern was that neuroticism had a stronger association with (lower) HCU among older adults than younger.
Exploratory Analyses: Does Controlling for Wealth Change the Associations Between Personality and HCU?
During peer review, it was suggested that these analyses control for wealth, in addition to the covariates already used in the present study. We ran additional exploratory analyses in which we include household wealth – the total net value of the household primary and secondary residences; real estate; vehicles; businesses; IRA accounts; stocks, mutual funds, and investment trusts; checking, savings, and money market accounts; CD, government savings bonds and T-bills; bonds and bond funds; and all other savings minus the sum of the household mortgages, home loans, and other debts – converted into 2022 dollars. These analyses are presented in Supplemental Table 12. General patterns of significance remain the same – extraversion, conscientiousness, and openness consistently predict health care use. Surprisingly, however, the direction of these effects is reversed, such that higher levels of traits predict lower HCU. This may suggest that a primary pathway from traits to health care is through wealth.
We note here two concerns about these models. First, education has been shown to correlate very highly with wealth. For example, in the present data, these values correlate at r = .24, but in other datasets, they are associated as high as r = .72 (Hughes et al., 2022). This makes the inclusion of both education and wealth redundant in most cases and potentially over-fitting remaining covariates, like personality. Second, prior work on personality and health has largely accounted for education but not wealth; in order to best situate our findings within the current literature, we believe it is important to use the same covariates as other studies, for optimal comparisons of effects sizes.
Discussion
The current study examined the relationship between personality and health care utilization through two pathways. First, the current study found that personality traits were directly associated with the use of health care services above and beyond the effect of self-rated health and chronic condition diagnoses. Second, we found that neuroticism and conscientiousness moderated the relationship of health (specifically, chronic condition diagnoses) and health care utilization such that the relationship between health and seeking services was stronger for those higher in conscientiousness and lower in neuroticism. We note mixed support for our specific hypotheses – conscientiousness was positively associated with seeking primary care services, but the relationship between health and health care was stronger, not weaker, at high levels of conscientiousness. In addition, we tested for moderating effects of personality traits on the relationship between health need and HCU; we found relatively few results and inconsistent patterns. This suggests to us that significant associations are likely spurious, so we will not discuss the significant interactions in this discussion. We note that these may be targets of future confirmatory research.
Do Traits Predict the Type of Health Care Service Used?
One of the main motivations of this study was understanding whether traits were associated with different kinds of health care: preventive, secondary, and tertiary. We found evidence that traits were associated with primary care: both general physician use and dental services were predicted by all traits except neuroticism. We also found evidence for the association between traits and secondary care, as overnight stays in the hospital and outpatient surgeries were associated with several traits. There is less evidence that traits are associated with tertiary care; only openness predicted use of special facilities. We suspect that tertiary care decisions may involve or even sometimes rely on family members of a patient, thus reducing any potential link between the patient’s traits and this type of care.
Do Traits Predict Health Care Use Directly or Only Through Health Need?
Prior work has long established the effect of personality traits on health, so a major question in connecting traits to health care use is whether this is fully explained by health status. Even when controlling for both self-rated health and chronic condition status, nearly all traits were associated with the use of multiple health care services. This supports the theory that traits predict HCU directly and not only through health status. This seems to be the case of traits extraversion, openness, and agreeableness, perhaps because these traits are less frequently associated with health and health behaviors than the others (conscientiousness and neuroticism). In other words, it may be that conscientiousness and neuroticism lead to specific health states, which lead to health care seeking, while the other traits predict HCU through non-health pathways. Future work may seek to determine these pathways, which may include general compliance health care norms and recommendations or even seeking additional social interaction. Unfortunately, these findings do not clarify an already mixed literature: prior work has found both positive and negative associations between extraversion or agreeableness and health care (Chapman et al., 2009; Hallgren et al., 2016; Willroth et al., 2023). Interestingly, we are unaware of other work that shows consistent associations between openness and health care.
As hypothesized, conscientiousness was positively associated with utilizing primary care services, specifically general practitioners (doctors) and dentists; moreover, the relationship between health and health services (outpatient and special facility) was stronger for individuals with higher levels of conscientiousness. Together, these results are suggestive of the effects of the rule-following facet of conscientiousness. That is, we expect the mechanism linking conscientiousness to health care is rule-following, including taking the advice of physicians about treatments for health problems and adhering to more general advice (e.g., see a dentist twice yearly). Future research might examine facets of conscientiousness or more narrow traits to determine whether rule-following is the only or primary mechanism linking conscientiousness to health care (e.g., Jackson et al., 2010).
Finally, neuroticism was associated with less use of hospital services and a weaker relationship between health and health care (hospital, medication, and special facilities). This supports the theory that individuals high in neuroticism avoid negative health news (Weston & Jackson, 2016) while contradicting the idea that neuroticism may lead to greater vigilance and thus care for health symptoms (H. S. Friedman, 2000; Graham et al., 2020b; Weston & Jackson, 2018). Overall, avoidance of health care is a potential mechanism explaining the negative association between neuroticism and health (Jokela et al., 2013; Roberts et al., 2007).
Do Traits Predict Health Care Through Perceived Need?
Our final set of models tested whether traits predict the relationship between health and health care – in other words, do traits change the threshold of poor health at which someone seeks care? In this case, we found that conscientiousness and neuroticism were both predictors of the health-HCU relationship. In general, high levels of conscientiousness predicted a stronger link, while high levels of neuroticism predicted a weaker one. We believe these findings support the theories proposed above: specifically, individuals high in conscientiousness are more rule-following and thus more likely to comply with recommendations by health care providers and public health officials (Hill & Roberts, 2011). That is, conscientiousness is linked to responding to health changes by changing one’s health care. Meanwhile, those high in neuroticism seek care in accordance with non-health factors. This may be due to misaligned perceptions of health – e.g., perceiving symptoms as worse than they are and seeking care unnecessarily or downplaying and avoiding serious health issues. Prior work suggests that neuroticism is associated with close attendance to one’s body (Weston & Jackson, 2018), but this does not imply that neuroticism is associated with more accurate somatic perceptions (Larsen, 1992). Indeed, such attention may fool those high in neuroticism to believe they know best.
Limitations
The current study benefits from incorporating data collected over two decades and examining a variety of health services; together, these allow for a more precise estimation of the relationship between changes in health and use of health services, as well as how these relate to personality. Future research can improve on the current study in the following ways. First, future research should incorporate a non-self-report assessment of health status and should seek to measure health more frequently than every two years. The use of electronic health records can be used to identify diagnosis dates, subtle or gradual changes in health status, and more fine-grained and detailed use of health services (Condon et al., 2017).
The broad nature of the health services measurement used here certainly obscured important individual differences in the use of services, including possible curvilinear relationships. For example, both participants who never see their PCP and participants who see their PCP multiple times a year may experience worse health – the former if they are negligent about attending to health needs and the latter if multiple visits are necessitated by a major health problem. However, even this may be an oversimplification of the relationship between HCU and health – there are many reasons, but for treatment and prevention, to see physicians and also many reasons for people to not see physicians. Even so, wellness visits have become an essential cornerstone of health care and are especially important for aging populations. For that reason, we are confident in the assertion that, in general, infrequent use or avoidance of PCPs is unlikely to result in positive outcomes.
Second, the current line of research, and the fields of personality and personalized health as a whole, can benefit from more narrow, unidimensional measures of personality. The current measure, the MIDI, is popular due to its relatively short nature. However, this strength also dramatically limits its predictive ability (Mõttus, 2016; Mõttus et al., 2020), and the same concern holds for most other personality measurement frameworks. Future research should move beyond the Big Five and incorporate measures of narrower traits to better understand mechanisms linking personality to health and to improve prediction.
Third, generalizability is constrained because the HRS recruits as its primary respondents U.S. residents who are 55 or older. This limitation is offset somewhat by the inclusion of younger spouses among the many secondary respondents, but it is still largely a study of older adults who are in generally good enough health to continue as participants in a long-term longitudinal panel survey. The HRS does try to achieve some representativeness, yet it remains the case that people who are from the unhealthiest segments of the U.S. population are either not part of the HRS (poor health is a major reason for survey non-response) or have died prior to the eligibility age of 55.
Moreover, the use of U.S. residents only is notable – we believe it would be inappropriate to have combined samples from many countries, as national health service policies can differ dramatically and create different health care environments for participants. An important avenue of cross-cultural research would be to examine countries with universal healthcare (e.g., Canada, the U.K., Sweden) and countries with no national health care. Some countries (e.g., Egypt) are currently preparing to adopt national health care systems and would make for excellent quasi-experimental designs to study the effects of national health care on personality and health.
Conclusion
The current study found that personality traits are associated with the use of health services above and beyond health needs (chronic condition diagnosis) and perceptions of health. These findings highlight the importance of studying the role of personality in health care, especially as previously common barriers to health care (e.g., lack of health insurance) have been reduced.
• Personality related to seeking health care independent from health status. • Extraversion was the most consistently linked to health care. • Conscientiousness and neuroticism moderated the health-seeking care relationship. Traits contribute to seeking care beyond simply through influencing health need. We conceptualize the relationship between health status and seeking care as itself an individual difference and show that traits explain variance in this relationship.Key insights
Relevance statement
Supplemental Material
Supplemental Material - The Role of Personality Traits in Health Care Utilization
Supplemental Material for The Role of Personality Traits in Health Care Utilization by Sara Weston, David Condon, Eileen Graham, and Daniel Mroczek in Personality Science
Footnotes
Author note
Marco Perugini was the handling editor.
Acknowledgements
Not applicable.
Author contributions
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
ORCID iD
Not applicable.
Data accessibility statement
The materials required for reproducing the study results can be found in the supplemental material. Data are freely available through the Health and Retirement Study website, and data files can be accessed following registration. See hrs.isr.umich.edu for details.
Supplemental material
Supplemental material for this article is available online. Depending on the article type, these usually include a Transparency Checklist, a Transparent Peer Review File, and optional materials from the authors.
Notes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.