
Abstract
Aim:
To examine an association between virtual care and mental health care use and whether there is any different pattern in the association across key demographic characteristics, specifically age, race/ethnicity, and educational attainment.
Methods:
A cross-sectional, observation study was conducted among the general population in the United States. This population-based study used data from the 2022 National Health Interview Survey. Main effect and interaction models using binary logistic regression were performed.
Results:
Of a total of 708 males and 1,238 females with symptoms of major depressive disorder (MDD), virtual care was associated with an increase in mental counseling or therapy use (males: adjusted odds ratio [aOR]: 2.75, 95% CI: 1.82–4.16, p ≤ 0.001; females: aOR: 3.38, 95% CI: 2.42–4.73, p ≤ 0.001). Females from a Hispanic background (aOR: 7.17, 95% CI: 2.97–17.33, p ≤ 0.001), aged 18–29 (aOR: 7.18, 95% CI: 3.51–14.70, p ≤ 0.001), and with less than high school graduation (aOR: 5.55, 95% CI: 1.97–15.62, p = 0.001) or college degrees (aOR: 5.52, 95% CI: 2.91–10.47, p ≤ 0.001) had notable increases in mental counseling or therapy use with virtual care.
Conclusions:
Virtual care is associated with a significant increase in accessing mental health care. Individuals who historically experience challenges related to in-person settings, including those with low educational attainment and Hispanics, may significantly benefit from virtual options.
Keywords
Introduction
In 2021, about 58 million adults in the United States had mental health conditions, and half of Americans were diagnosed with mental disorders at some point in their lifetime, suggesting that mental health is a major public health concern in the country. 1 Moreover, recent data showed continued worsening in mental health with major depressive disorders (MDDs) rising from 6.6% in 2005 to 9.2% in 2020.2,3 Mental health conditions are associated with other public health issues such as substance use disorder, including drinking alcohol and smoking behaviors.4,5 For instance, people with mental conditions have higher smoking rates. 4 Furthermore, previous work has pointed to the association between mental illness and substance use behaviors, including cigarette smoking and cessation across age groups and genders. 6
To address these public health issues, the U.S. Healthy People 2030 has set goals that include timely prevention or interventions. 7
Early, adequate interventions are critical, not only for improving mental health but also for additional benefits, such as enhancing social activities, including family relationships, daily routines, and work performances. 8 Medications, such as antidepressants, are widely employed to prevent the onset of psychological symptoms or the advancement of existing conditions. 9 Psychotherapy, another common form of mental health treatment, includes a range of measures, such as counseling and cognitive behavioral therapy. 10 This approach, also known as talk therapy, has gained attention because clinical measures based on effective patient-provider communications and interactions facilitate evidence-based interventions that serve individuals’ care needs and increase clinical effectiveness. 11 Despite these interventions, a national statistics report showed that only one in five U.S. adults receives mental health services in response to their health concerns. 12
Considering the importance of mental health care, the existing evidence about gaps and variations in accessing mental health care across demographic characteristics is concerning. 13 For example, less than half of Black individuals with moderate to severe symptoms of anxiety or depression (47%) reported receiving care, 0.73 times lower than their White counterparts (64%). 14 Age-group differences have also been reported with younger adults receiving a higher rate of mental health care. 12
Individuals who delay or miss necessary care complain about frequent barriers or challenges, such as time constraints, lack of mental health facilities, or difficulties making appointments with providers.15,16 With technological advancements, mental health services through virtual modalities have rapidly evolved. Compared with less than 1% of outpatient mental health care delivered in virtual settings in 2019, it became widely popular, rising to 35–40% between 2020 and 2021. 17 Amid the health care disruptions during the COVID-19 pandemic, virtual care demonstrated a pivotal role in serving populations who may otherwise have delayed or foregone needed mental health services. Clinic-based studies also showed that virtual mental health care was not different in clinical outcomes and was associated with increased perceived quality of care compared with in-person care.18,19 Although most people report a preference for in-person care, they are open to virtual options. 20 With unique features that either reduce or pose barriers, including availability and knowledge of technology and individuals’ attitudes, virtual care can have important implications for mental health care across populations.20–22
Despite prior studies documenting evolving virtual care across health care disciplines as alternatives to traditional face-to-face care, it is unclear how virtual options play a role in access to mental health care across varying population characteristics.17–19 Therefore, the current study aimed to 1) examine whether a significant association exists between an individual’s virtual care use status and mental health care use and 2) whether there is any different pattern in the association across key demographic characteristics, specifically age, race/ethnicity, and educational attainment. This study hypothesizes that virtual care use status is associated with increases in mental health care use, and there is heterogeneity in the association across population subgroups.
Methods
Data
This population-based, cross-sectional study used 2022 data from the National Health Interview Survey (NHIS), an annual household interview survey conducted by the U.S. Census Bureau. 23 This population survey targets non-institutionalized adult individuals 18 years or older residing in 50 U.S. states and the District of Columbia. NHIS employs geographically clustered sampling techniques to select the sample and uses a face-to-face interview format to collect respondents’ self-reported health-related information. These data are widely used to monitor a broad range of national-level population health issues. Samples included in this study represent males and females who reported their symptoms of depression through the Patient Health Questionnaire (PHQ) 8 (Table 1) and reported whether they used mental health counseling or therapy. Of a total of 27,648 individuals, 1,948 participants who had PHQ 8 scores ≥ 10 (5% of males and 9.1% of females), considered as having symptoms of MDD, were included. 24 Additional inclusion criteria selected participants who reported counseling or therapy experiences, resulting in 1,946 individuals for analysis (708 males and 1,238 females). As this study analyzed deidentified, publicly available secondary data, consent for the data was not necessary.
Patient Health Questionnaire (PHQ)−8

Measures
Key outcome
The study outcome was a binary measure (Yes/No) of receiving mental health counseling or therapy using responses to the following question, “During the past 12 months, did you receive counseling or therapy from a mental health professional such as a psychiatrist, psychologist, psychiatric nurse, or clinical social worker?”
Covariates
The primary independent variable was an indicator of virtual care of any kind that participants reported through the following question, “During the past 12 months, have you had an appointment with a doctor, nurse, or other health professional by video or by phone?”
Key demographic characteristics of interest were age, race/ethnicity, and education, each categorized as 18–29, 30–39, and 40–49; non-Hispanic White, non-Hispanic Black, non-Hispanic others, and Hispanics; and less than high school graduation, high school graduation, some college education, and a bachelor’s degree or above, respectively. Additional covariates were included to account for potential confounding effects in the association, such as health insurance coverage, marital status, smoking status, general health, diabetes, and disability.22,25,26 Marital status was a dichotomous variable to indicate whether participants were married or not. Smoking status had three categories, such as never, formerly, and currently smoking. Health-related variables were dichotomized for good health or not good health and whether respondents had health conditions, including diabetes and disability.
Statistical analysis
We calculated the percentage of mental health counseling or therapy use across participants’ demographic characteristics and then broke down this percentage by virtual care use. Binary logistic regression analysis was performed to examine an association between mental health counseling or therapy and virtual care use status without and with accounting for study covariates, such as age, race/ethnicity, education, marital status, health insurance, smoking, general health, diabetes, and disability. Since the interaction effect of virtual care on mental health care use is of primary interest, we calculated the percentage of people receiving counseling or therapy across age, race/ethnicity, and education by virtual care to assess whether there are differences in mental health care use associated with virtual care. Next, an interaction model using logistic regression was performed by interacting age, race/ethnicity, and education with virtual care (virtual care use × age, virtual care use × education, and virtual care use × race/ethnicity) to evaluate any difference in mental health care use based on the individuals’ virtual care use.
In addition, sensitivity analysis was performed with the sample restricted to those with symptoms of severe MDDs (PHQ-8 scores ≥ 20) to examine if the associations are consistent with those of primary analyses. Complex survey weights and design variables were adjusted in all analyses. The statistical significance level was p < 0.05 and STATA version SE 18.0 was used. This study was reviewed by the University of OO Institutional Review Board and additional ethical approval was not necessary because the data are part of publicly available secondary datasets.
Results
Of a total of 708 males with symptoms of MDD, about 41.1% received mental health counseling or therapy (Table 2). This rate decreased with age increase, going from 49.8% (ages 18–29) to 31.7% (ages 65+). Those with some college education or above had a higher rate of receiving mental health care compared with those with less than high school graduation (39.1∼47.9% vs. 28.8%). Among females with symptoms of MDD, about 42.4% reported that they received mental health care with adults aged 18–39 and those with some college education or above revealed a disproportionately higher rate. In both males (55.9% vs. 28.3%) and females (55% vs. 26.3%), mental health counseling or therapy was more prevalent for those who use virtual care compared with those who do not.
Mental Health Counseling or Therapy Use (%) by Sample Characteristics in Males and Females with Symptoms of Major Depressive Disorders

Simple logistic regression confirmed that those who use virtual care had greater odds of receiving counseling or therapy compared with those who do not use virtual care in males (odds ratio [OR]: 3.21, 95% CI: 2.19–4.72, p ≤ 0.001) and females (OR: 3.42, 95% CI: 2.53–4.62, p ≤ 0.001) (Table 3). The adjusted regression analysis showed consistent results.
Association Between Population Characteristics and Mental Health Counseling or Therapy Utilization in Males and Females with Symptoms of Major Depressive Disorders

aOR represents adjusted odds ratio, accounting for population characteristics.
p < 0.001.
p < 0.05.
p < 0.1.
Variations were observed in the rate of mental health counseling or therapy by virtual care use status across age, race/ethnicity, and educational attainment (Table 4). Among male participants, individuals in the age groups of 50–64 (46.6%) and 65 or above (37.3%) showed receiving mental health care less frequently with virtual care than younger people (64.6 − 70.4%). A lower rate of mental health care use was also shown among those with less than a high school graduation. Among females, people aged 18–24 and 30–39 revealed a higher rate of mental health care use associated with virtual care than those of other age groups (65.5 − 75.2% vs. 24.5–50.1%). A notable difference was found in receiving mental health care for non-Hispanic black people (45.4%%) compared with non-Hispanic White counterparts (56.8%).
Mental Health Counseling or Therapy Utilization by Population Characteristics by Virtual Care Use Status Among Individuals with Symptoms of Major Depressive Disorders
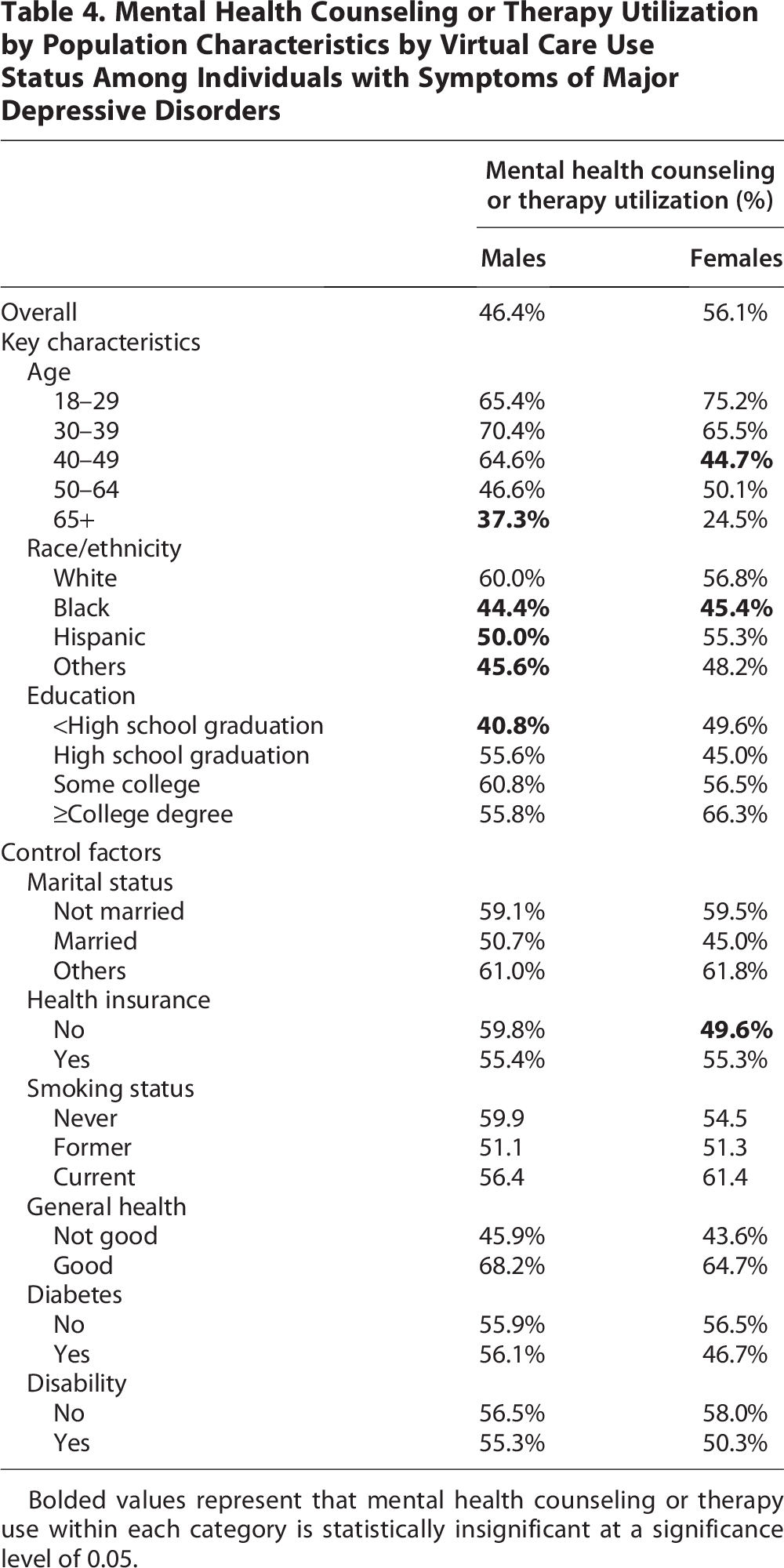
Bolded values represent that mental health counseling or therapy use within each category is statistically insignificant at a significance level of 0.05.
Interaction models in Table 5 showed that among White males and females, virtual care use status was significantly associated with an increase in counseling or therapy use (males: adjusted odds ratio [aOR]: 2.75, 95% CI: 1.82–4.16, p ≤ 0.001; females: aOR: 3.38, 95% CI: 2.42–4.73, p ≤ 0.001). Markedly, Hispanic female participants experienced 7.17 times greater odds of counseling or therapy use for those who use virtual care compared with those who do not (95% CI: 2.97–17.33; p ≤ 0.001). In terms of age, younger females aged 18–29 showed a substantial association (aOR: 7.18, 95% CI: 3.51–14.70, p ≤ 0.001). Females with less than high school graduation (aOR: 5.55, 95% CI: 1.97–15.62, p = 0.001) or a college degree (aOR: 5.52, 95% CI: 2.91–10.47, p ≤ 0.001) had notable increases in mental health care use with virtual care. Among males, people aged 30–39 (aOR: 4.95, 95% CI: 1.89–12.96, p = 0.001) and 40–49 (aOR: 4.64, 95% CI: 1.58–13.59, p = 0.005) had increased mental health care associated with virtual care. While results from sensitivity analysis with individuals with symptoms of severe MDD were largely consistent, females aged 18–29, of Hispanic ethnicity, and having a college degree showed even a larger increase in mental health care use associated with virtual care use (Tables 6 and 7).
Interaction Effect of Virtual Care Use Status on the Association Between Population Characteristics and Mental Health Counseling or Therapy Receipt Among Males with Symptoms of Major Depressive Disorders—Interaction Model

aOR denotes adjusted odds ratio, accounting for population characteristics, and aOR of the interaction effect is the odds of receiving mental health counseling or therapy among those who reported virtual care use compared with odds of receiving mental health counseling or therapy among those with reported no virtual care use within each category of the population characteristic.
p < 0.001.
p < 0.05.
p < 0.1.
Virtual Care Use by Population Characteristics in Males and Females with Severe Major Depressive Disorders (PHQ-8 Scores ≥20)

Association Between Population Characteristics and Receipts of Mental Health Counseling or Therapy in Males and Females with Symptoms of Severe Major Depressive Disorders (PHQ-8 Scores ≥20)

aOR represents adjusted odds ratio, accounting for population characteristics.
p < 0.05.
p < 0.001.
p < 0.1.
Discussion
This study examined the relationship between virtual care and receiving mental health counseling or therapy, focusing on key demographic characteristics, such as age, race/ethnicity, and education. Between 41% and 43% of the study participants received mental health care and approximately half reported virtual care use. Virtual care use status was associated with the increased use of mental health counseling or therapy among both males and females, suggesting that virtual care may play an important role in improving access to mental health services and treatments.19,27 However, there were heterogeneous patterns in this association across assessed key population characteristics.
Specifically, males aged between 30 and 59 years old or with at least high school graduation had more frequent mental health care use associated with virtual care use status. Moreover, non-Hispanic White male participants showed increased mental health care use among those who use virtual care compared with those who do not, while non-White minorities did not show a significant association. These findings align with previous work and may suggest that since virtual care requires certain tools, including technologies and spaces, these subsets of the population may have better access to these resources, allowing them to address mental health care needs through virtual options.28,29 The findings may also reflect what has previously been reported in terms of knowledge or skills necessary for virtual care affirming that White, younger, highly educated individuals experience fewer issues than their racial minority counterparts, including competency in digital environments.28,30,31 Furthermore, perceptions about the wide-ranging advantages of virtual modalities, including less concerns about time and geographical limitations, are possibly contributing to this association.
Conversely, males with less than high school graduation, those aged 65 years or older, and racial and ethnic minorities did not show increases in receiving mental health care with virtual care. Previous research has shown that people with low educational attainment and older adults often complain about technology barriers and low levels of digital capability, undermining their ability to use technology-assisted care and the satisfaction associated with it.21,32 With such lacking skills and up-to-date technology support, it is possible that these individuals experience limited benefits out of virtual modalities or even disruptions of care, leading them to seek in-person visits or forgo care if in-person care is not accessible. While the evidence suggests that virtual care can positively influence health care access, the population variations raise substantial concerns about the possibility that certain groups of people continue to encounter barriers that prevent them from utilizing timely care assisted by virtual modalities as needed or wanted to fill health care gaps they experience.18,19
Overall, females who use virtual care showed greater use of mental health counseling or therapy. Specifically, younger people aged between 18 and 39 had a noted increase in mental health care use with virtual care. According to the national study, young females are the most vulnerable to psychological disorders. 33 Their disproportionate exposure to many stressors related to household work and childcare responsibilities is among the probable factors causing poor mental health. 34 Females in this age range are also characterized as individuals of reproductive age, suggesting that they face pregnancy-related stressors over their perinatal periods. Notably, depression is one of the most common maternal morbidities during prenatal and postpartum. 35 However, despite the anticipated high mental care needs, burdens of family responsibilities and pregnancy circumstances may impose substantial restrictions on individuals’ time, travel, and physiological state in pursuing physical encounters with providers. These unique experiences may drive young females to look for mental health care remotely to substitute for in-person visits.36,37
In addition, females with a college degree revealed a marked increase in mental health care use given virtual care use, which is aligned with earlier findings that higher educational attainment is associated with higher levels of positive attitudes toward virtual options and is linked to fewer barriers.38,39 However, Hispanics and those having less than a high school graduation also showed improved access to mental health care when they were using virtual care. Earlier findings from a national study on women aged 18–44 suggest that those with lower educational attainment and from a Hispanic ethnic group tended to use virtual care more frequently than those with higher education levels and other racial/ethnic groups. 22 Research has shown that these disadvantaged populations experience poor health care and challenges in clinical settings, which has been a major obstacle, triggering individuals to delay or forgo necessary care.40,41 Multi-faceted factors, such as language barriers, discrimination, and insurance denials concerning in-person visits, are potential determinants for these historically disadvantaged people to choose virtual options.22,42–44 These heterogeneous associations across populations are significant findings, advancing the knowledge base on mental health care in the rapidly changing health care landscape. Future studies are warranted to further the understanding of what specific circumstances lead to these observations.
Policy implications
Virtual care may provide additional options for accessing quality mental health care. Health care professionals consider integrating in-person and virtual care as a promising opportunity to improve access to care across health care disciplines. 45 Although the current analysis indicates that the general population can benefit from using virtual care, some may not do so due to barriers they face at both individual and community levels. Markedly, females having low educational attainment and Hispanic females had increases in mental health care use with virtual care, which further suggests that those who experience challenges related to in-person settings may benefit from virtual options. The dynamic associations found in this study require continued in-depth investigations into what influences people’s decisions regarding mental health care using information and communication technology. These findings provide important implications to inform health care and public health policy in efforts to improve Americans’ mental health. For instance, clinical and public health efforts to decrease substance use among individuals who suffer from mental conditions might benefit from incorporating virtual care as an option to address disparities in access to care. 5 Indeed, the increased use of virtual services in the current health care delivery, some due to the COVID-19 pandemic, has shown the effectiveness of virtual treatments for substance use.46,47 In addition, virtual services are considered an alternative to in-person treatments for individuals with limited access to mental health and substance use health care, such as those living in rural communities.5,48
Limitations
This study has many strengths, including analysis of population-representative data. However, this study has some limitations. First, while our findings showed increased mental health counseling or therapy for those who use virtual care, our key independent variable is not exclusive to mental health care. Future studies are warranted to improve or strengthen the current findings by analyzing more targeted measures. Second, this study relies on participants’ self-reports and inherently has limitations, such as social desirability and recall bias. Third, our study includes single cross-sectional data due to the availability of PHQ-8 questionnaires. An extended data period with continued collection of mental health screening would strengthen the current findings.
Conclusions
Virtual care use is associated with an increase in accessing mental health counseling or therapy, revealing its potential to supplement traditional in-person care to tackle rising mental health problems. The current findings suggest the role of virtual care in improving access to mental health across population groups. It is critical to further the understanding of unique health care behaviors around mental health care and care modalities to better address health care access inequities.
Footnotes
Author Disclosure Statement
No potential conflicts of interest relevant to this article were reported.
Funding Information
No financial disclosures were reported by the authors of this article.
Author’s Contributions
C.V.O. and J.L. conceived the study, analyzed data, and drafted and revised the article. C.V.O. supervised the project.
Ethical Approval and Informed Consent Statements
This study was reviewed by the University of Texas at San Antonio Institutional Review Board and additional ethical approval was not necessary because the data are part of publicly available secondary datasets.