
Abstract
Background:
Telemedicine has become an important mechanism for delivering health care in the wake of the COVID-19 pandemic. While some medical subspecialties were able to rapidly integrate telecare into their workflow, ophthalmology is one field in which telemedicine has not been as widely adopted. In this systematic review, we analyze published studies assessing patient and provider viewpoints on telemedicine for eye care. Our aim is to understand how adoption of teleophthalmology is being studied and whether definitive conclusions regarding patient and provider perspectives on telecare can be drawn from published literature.
Methods:
We performed a systematic PubMed search for studies utilizing surveys to assess patient and provider perspectives regarding remote eye care. Articles were excluded if they were irrelevant to teleophthalmology, did not assess patient or eye care provider perspectives regarding teleophthalmology, assessed specific platforms or aspects of eye care, were reviews without primary data, or if the survey used was not available. The questionnaires from the included articles were analyzed for validation status, subspecialty, question wording, and response format.
Results:
The PubMed search returned 92 articles, 22 of which were included in the final dataset after exclusions. Only four studies utilized externally validated questionnaires, although several additional studies were based on validated items. Survey length, wording, and response formatting varied across the studies. These 22 studies contained responses from 3,796 patients and 2,388 eye care professionals, but the lack of standardization between the surveys makes high power conclusions impossible.
Discussion:
The results of this review demonstrate a need to develop a standardized and validated survey instrument specifically for assessing teleophthalmology to identify barriers to widespread implementation.
Introduction
Telemedicine has become an increasingly prevalent means of health care delivery, the adoption and utilization of which has been accelerated by the COVID-19 pandemic. Medicare and Medicaid data show that weekly telehealth visits increased from approximately 13,000 before the COVID-19 pandemic to more than 1.7 million in April 2020, 1 and in 2020, telemedicine constituted approximately $55.9 billion on the global market. 2 Telehealth services may be synchronously provided via phone or computer, with the patient and provider linked in real time, or asynchronously with data sent to a remote provider who interprets and completes the visit at a later time. Telemedicine can benefit those with transportation difficulties, chronic illnesses, vision impairment, and other barriers to attending in-person appointments and can expand provider reach so that those in underserved areas can see specialized physicians on time. From the provider’s perspective, telehealth benefits include increased schedule flexibility, patient compliance, increased independence, and reduced expenditure on clinic supplies. Overall, studies report that patient3–6 and provider7,8 satisfaction are reported to be generally high with telemedicine.
Despite the recent boom in telehealth services and potential benefits, ophthalmology is likely one of the fields utilizing telecare the least. 9 A thorough ophthalmical examination generally requires some combination of testing visual acuity and intraocular pressures, as well as a physical eye examination using a slit lamp microscope and indirect ophthalmoscopy. Ancillary tests, such as visual fields, optical coherence tomography, gonioscopy, fundus photography, and optical coherence tomography, are common adjuncts. Techniques for obtaining equivalent information virtually have been attempted with varying success, including smartphone apps for the slit lamp examination and home devices for performing ancillary tests.10–12
While many groups have successfully provided tele-eye care using these methods, there does not seem to be an overall consensus on the long-term utility and feasibility of incorporating remote care into ophthalmology practices. In this systematic review, we analyze published literature on telemedicine and eye care, specifically including studies that assess patient and provider opinions on this care delivery method. Our aim is to understand how the adoption of teleophthalmology is being studied and whether definitive conclusions regarding patient and provider perspectives on telecare can be drawn from published literature.
Materials and Methods
We performed a systematic search in PubMed to identify studies assessing patient and provider perspectives on teleophthalmology. The search phrase began with the medical subject heading (MeSH) “telemedicine” followed by Boolean Operator AND to link to “ophthalmolog.” The use of “telemedicine” as a MeSH term allowed us to retrieve all related articles using variations of this term, including “telehealth,” “eHealth,” “virtual medicine,” and “telecare,” among others. The complete list of entry terms included in the “telemedicine” MeSH search can be found on the National Library of Medicine website. 13
To specifically target studies analyzing direct provider or patient feedback, we included a search of the title or abstract fields for “questionnaire*,” “poll*,” or “surve*.” The entire search phrase used was as follows: (Telemedicine[MeSH Terms]) AND (ophthalmolog*[Title/Abstract]) AND (surve*[Title/Abstract] OR poll*[Title/Abstract] OR questionnaire*[Title/Abstract]). We included all articles published before June 1, 2023, without additional filters. This initial PubMed search yielded 92 articles.
The abstract and methods sections of each article were screened for relevance by author #1 (T.E.F.). “Teleophthalmology” was interpreted broadly by the authors as including any means of remotely delivering eye care using electronic transfer of medical information, including synchronous and asynchronous approaches. Only articles that directly surveyed patients’ or eye care providers’ viewpoints on teleophthalmology were included. The most common reason for exclusion was that the article did not directly assess patient or provider experiences with teleophthalmology (28 articles). The second most common reason for exclusion was that the article assessed a specific application or internet platform rather than teleophthalmology as a general method for care (12 articles). Seven publications were excluded because they surveyed providers from specialties other than ophthalmology, such as emergency providers or general practitioners. We did encounter studies that surveyed eye care professionals other than ophthalmologists, including optometrists and ophthalmical assistants, and decided to include them due to relevance. Six studies were reviews without primary data, three specifically assessed the delivery of newborn eye screens, three were not available in English, two were not relevant to teleophthalmology, and one was a duplicate of an included article. Some articles met multiple of these criteria for exclusion. At the completion of the abstract/methods screen, 62 articles were excluded, with 30 articles remaining in the dataset.
The full text of each selected article was downloaded, and the complete questionnaire was extracted when available. Questionnaires not available in the article’s main body or supplemental materials were requested directly from the authors. Four requests could not be fulfilled as the articles were published several years prior and the authors no longer had access to the original surveys; these articles were excluded as we could not access the specific questions. Four authors did not reply to requests, and thus, these articles were also excluded. After these exclusions, the final dataset included 22 articles. A flow chart demonstrating the article selection process is included in Figure 1. The second author (G.D.L.) independently reviewed the final list of included articles and did not remove or add any additional articles.

Systematic review article exclusion and inclusion process.
The questions used in the original articles were extracted. It was noted whether the questionnaires were validated or nonvalidated, the subject of each question (patient or provider), and the style of the response options (Likert, yes/no, rating scale, multiple choice, open ended). Questions about the demographic characteristics of the respondents were removed such as, “what is your gender?” or “what is your age?”, as these were not relevant to the study objectives. Provider questions asking specific features of their practice which could not be generalized and were not the focus of this study, such as how many years the provider has practiced or the setting of their clinic, were also removed.
Table 1 demonstrates patient-reported questions related to teleophthalmology from each included publication, whereas Table 2 provides corresponding information from the provider’s perspective (Tables 1 and 2). Questions consisting of a single prompt with the ability to mark multiple responses, such as “Which platform do you use? Select all that apply,” were counted as one single question. Questions with a single prompt heading but multiple subquestions with their own answer choices were recorded as separate questions. As an example, Rhodes et al. contained a question reading “Did you know that it is possible to…” with 4 subquestions reading: “(a) obtain a remote medical opinion or diagnosis from a physician via telemedicine technology?”, “(b) receive a medical intervention or treatment supervised remotely by a specialist via telemedicine technology?”, “(c) obtain telephone advice from a health care professional on the appropriate type of service to use?”, and “(d) remotely monitor individual health status via telemedicine technology?” with yes/no answers available for each. 19 This was counted as 4 separate questions, since each one addressed a unique idea and required a distinct answer. All articles and included questions were cross-checked for accuracy.
Studies Assessing Patient Perspectives on Teleophthalmology, Including the Study First Author, Subspeciality Where Applicable, Year, Validation Status, Sample Size, and Journal
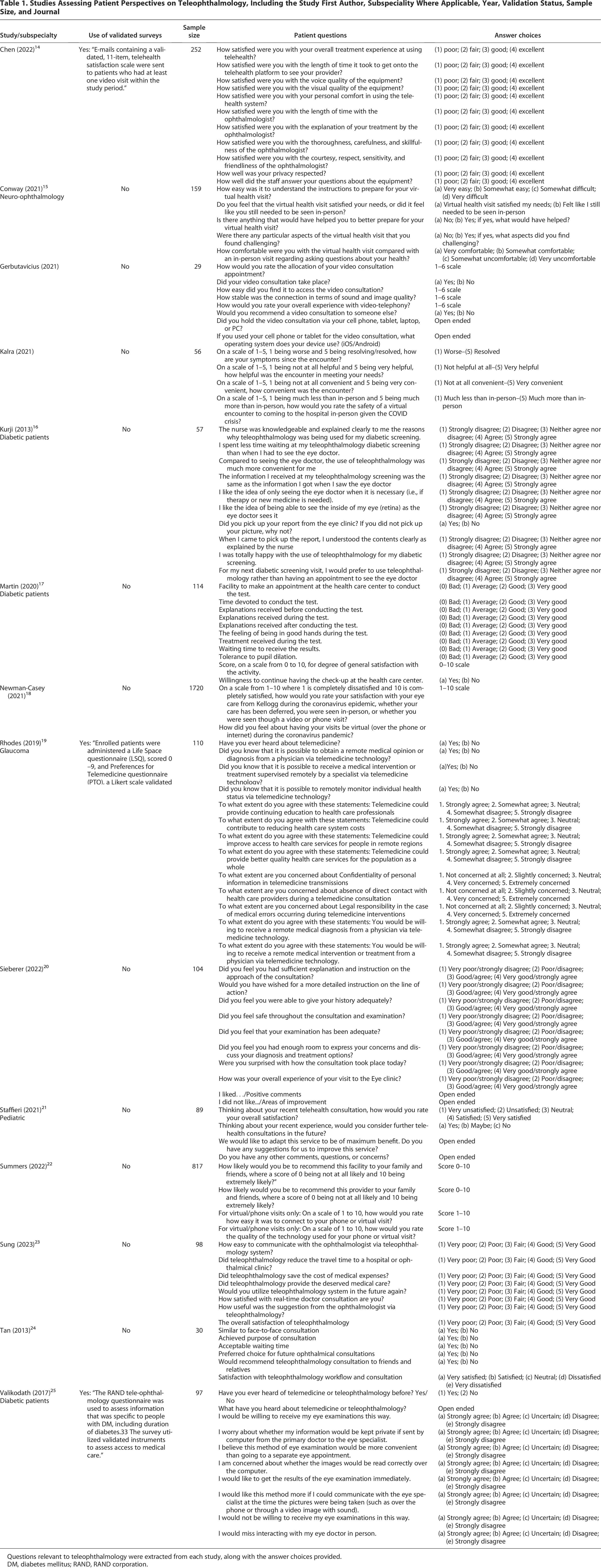
Questions relevant to teleophthalmology were extracted from each study, along with the answer choices provided.
DM, diabetes mellitus; RAND, RAND corporation.
Studies Assessing Provider Perspectives on Teleophthalmology, with the Publication Information, Sample Size, and Relevant Questions with Answer Choices Extracted

AAO, American Academy of Ophthalmology; AMA, American Medical Association; AMD, age-related macular degeneration; ASRS, American Society of retina specialists; CNV, choroidal neovascularization; DR, diabetic retinopathy; EHR, electronic health record; EMR, electronic medical record; ERGs, electronic retinal grading system; HIPAA, Health Insurance Portability and Accountability Act; IIH, idiopathic intracranial hypertension; MR, magnetic resonance; MeSH, medical subject heading; OCT, optical coherence tomography; OHSU, Oregon Health and Science University; OKN, optokinetic nystagmus; OPD, outpatient department; PAS, patient administration system; ROP, retinopathy of prematurity; VOR, vestibulo ocular reflex.
Results
Survey subjects
The final dataset used included 22 studies. Four (18.2%) surveyed both providers and patients, 8 (36.4%) surveyed the opinions of providers only, 9 (40.9%) surveyed patients only, and 1 (4.5%) surveyed the parents of pediatric patients regarding a pediatric teleophthalmology visit. Most of the studies directed at providers surveyed ophthalmologists, but some included optometrists or ophthalmology staff members. Four studies elicited the opinions of specific subspecialists within ophthalmology, including 2 surveys of neuro-ophthalmologists (365 total respondents),15,30 1 of oculoplastic surgeons (70 respondents), 27 and 1 of vitreoretinal surgeons (214 respondents). 31 In total, these 22 studies included 3,732 patient/parent participants and 2,388 provider respondents (Tables 1 and 2). We note that one study did not specifically report the total number of patient survey participants, but we used the N values listed for specific questions to estimate the total responses. 22
Validated questionnaires
Among the 22 included studies, four (18.2%) specifically note that they utilized externally validated questionnaires.14,19,25,26 Three of the studies utilizing validated surveys were performed in the United States and assessed patient perspectives,14,19,25 and one was performed in India and assessed provider perspectives. 26 The authors of one additional publication note that their patient-directed survey was internally validated by use on 10 study subjects, but did not undergo external validation. 24
One of the validated patient studies utilized the Preferences for Telemedicine Questionnaire, 19 a 14-item survey that includes 5 yes/no questions assessing telemedicine knowledge followed by 9 questions assessing telemedicine beliefs, concerns, and predispositions on a 5-point Likert scale. 32 Another used a modification of the RAND teleophthalmology questionnaire to assess the attitudes of diabetic patients regarding remote screening for diabetic retinopathy. 25 The third study 14 utilized a questionnaire adapted from the Telehealth Satisfaction Scale, a 10-item survey with responses on a 4-point Likert scale initially developed to assess specialist access via telehealth among First Nation peoples 33 and validated in the memory clinic setting. 33 In total, these 3 patient-directed studies utilizing validated questionnaires contained 103 questions after excluding demographics and patient data questions. After removal of the patient data and demographics questions, the validated surveys contained 11, 14 22, 19 and 69 25 question prompts, whereas the nonvalidated surveys ranged in length from 4 to 10 questions. A total of 459 patients responded to these 3 surveys.
The only provider-directed survey noting validation, Agarwal et al., surveyed 1,026 providers using a 25-item questionnaire, which was prevalidated by 4 independent ophthalmologists and pilot tested via use with 20 providers. 26 This study was performed in India and contained the largest group of provider respondents of the included publications. The main focus of the Agarwal et al. study was to assess the financial impact of the COVID-19 pandemic on ophthalmology practices in India, and only one question in the survey directly addressed attitudes toward teleophthalmology. This question read “What is your experience regarding utility of teleophthalmology in your practice during lockdown period and after (Multiple options can be marked), with 6 answer options reading “No experience with teleophthalmology,” “It did not match my expectation and not many of my patients were benefitted,” “It benefitted my patients, and I am satisfied,” “It was billed similar to my outpatient department (OPD) face-to-face consultation charges,” “It was billed lower than my usual consultation charges,” and “It was not billed.” 26
Nonvalidated questionnaires
The remaining 18 studies included in the final dataset (81.8%) used nonvalidated surveys constructed by the authors, with significant variation in question style and response format. The authors of three of these studies did note that their questions had been adapted from separate validated surveys, but had not been validated for use in the setting of teleophthalmology.18,22,34 These surveys demonstrated significant variety in question wording, response wording, and response style (Likert, yes/no, numerical score, open ended, multiple choice).
Patient surveys
We identified several themes among the patient-directed survey questions, including preexisting knowledge of telemedicine, satisfaction with remote care, willingness to use teleophthalmology in the future, and feelings of safety during the examination (Table 1). Five questions asked about confidentiality, and two asked whether the patient felt safe during their teleophthalmology encounter, one of these specifically in the setting of COVID-19. Seven patient questions asked about the timing of the visits: two regarding the amount of time spent during the encounter with testing or with the ophthalmologist, three regarding waiting time, one asked satisfaction with the time it took to obtain results, and one asked whether the teleophthalmology encounter reduced the time required to travel to a clinic. Three specifically asked about the convenience of receiving eye care remotely compared with in-person, and five asked whether the patient would recommend a teleophthalmology visit to others. Two questions asked about cost, both on a 5-point Likert scale:
Provider surveys
Twelve publications included questionnaires directed at providers (Table 2). Common themes included provider utilization of telemedicine, home monitoring, or any remote care, including remote imaging interpretation, especially in the context of the COVID-19 pandemic. Twenty-three questions included reference to cost, overhead, or reimbursement for telehealth visits. Several questions assessed the providers’ views on the adequacy and reliability of the examinations, such as “Were you able to complete an examination as part of the virtual health visit that provided enough information for medical decision-making?,” 15 “Did you feel you were able to carry out examination adequately?,” 20 and “I trust the results/findings from telehealth visits.” 22
Only one provider question specifically included the term “satisfaction,” stating “Score, on a scale from 0 to 10, your degree of general satisfaction with the activity.”
17
Fourteen questions asked whether the provider planned to continue telemedicine visits, remote image reading, or home monitoring activities in the future, whereas 13 questions asked about barriers encountered in providing remote eye care visits. Prompts assessing the providers’ opinions on the utility of teleophthalmology for patients and their ocular health outcomes included:
“Do you think that online video calls/examination applications are beneficial to the health service received by the patient?,”
35
“In your opinion, is telemedicine an effective tool for oculoplastic consultations?,”
27
“In its current form, I find telemedicine visits to be an acceptable form of evaluation for retina patients in the right clinical scenario,”
28
“I think telehealth visits will improve outcomes for our patients,”
22
and “I think telehealth visits have advantages for patients.”
22
Discussion
Telemedicine has been slow to catch hold in ophthalmology despite its successful implementation in other health care fields. This discussion is especially prudent in the context of a growing shortage of ophthalmology providers in the United States, 36 particularly in rural areas, 29 and in the wake of the global COVID-19 pandemic. Telemedicine has the opportunity to address these challenges but, in our opinion, has not been utilized to its potential. This review seeks to address a gap in knowledge regarding the patient and provider experience with teleophthalmology.
Overall, patients surveyed in these studies seem to be generally satisfied with remote eye care/teleophthalmology, and the majority indicated that they would like to continue to receive remote visits for eye care and would recommend the service to others. For example, 95% of 386 patients in India agreed with the statements “I would use the mobile clinic again,” and “I would recommend the mobile clinic to others.” 37 In a separate study out of Spain, 99.1% of 114 patients responded Good or Very Good when asked about “the feeling of being in good hands during the test.” 17
There was variation in provider responses regarding satisfaction. When asked in the study by Conway et al., “Were you able to complete an examination as part of the virtual health visit that provided enough information for medical decision-making?,” 137/157 (87.3%) providers replied “Yes.” 15 However, in a separate study conducted by Mercer et al., only 28/63 (45%) responded with Modest/Large when asked about their perception of the “role for teleophthalmology in future practice.” 38 The Agarwal et al. study from India asked providers, “What is your experience regarding the utility of teleophthalmology in your practice during the lockdown period and after?,” and 326/780 (41.7%) responded with the option “It benefited my patients, and I am satisfied.” 26
While these data are intriguing, it is challenging to summarize given the variability in question and answer design across the studies. Many extracted questions addressed the same underlying theme, but with different wording, highlighting a lack of standardization. For example, consider the following questions asked of patients from 4 different studies:
“Do you feel that the virtual health visit satisfied your needs, or did it feel like you still needed to be seen in-person?,”
15
“Score, on a scale from 0 to 10, for degree of general satisfaction with the activity,”
17
“Thinking about your recent telehealth consultation, how would you rate your overall satisfaction?,”
21
“Did you feel that your examination has been adequate?”
20
All four items address general satisfaction with tele-eye care from the patient’s perspective; however, the variation in wording and answer styles makes the data impossible to compile for increased statistical power. Response choices among the extracted questions included Likert scales, binary yes/no, multiple choice, numerical scales, and open ended.
The predominant use of author-developed surveys rather than validated questionnaires for assessing teleophthalmology is consistent with the trend found in other reviews of telemedicine surveys.39–41 Recent literature provides support for the development of a validated and standardized tool with which to assess telemedicine encounters. Such a tool could enhance the accuracy of evaluating patient-centered aspects of audiovisual telemedicine interactions and contribute to the development and harmonization of standardized assessment frameworks across telehealth platforms and medical domains.42,43 However, it is important to acknowledge that such an instrument may not fully reflect the unique characteristics of specific programs, geographic regions, or population groups. Using validated surveys is especially beneficial in increasing the power of pooling studies with limited participants; in this case, the largest patient cohort was 1,079, 44 whereas the largest provider cohort was 1,026. 26 Some of these studies addressed subspecialized areas within ophthalmology: of the 22 studies examined, 2 addressed neuro-ophthalmology15,30 with a total of 365 providers surveyed, 2 were specific to glaucoma with 1,189 patients total,19,44 7 addressed diabetic retinopathy/retina,16,17,25,28,31,34,45 1 oculoplastics with 70 providers, 27 and 1 pediatric ophthalmology with 89 parents surveyed. 21 Given the small number of studies and participants in each of these subgroups, utilizing validated surveys with the ability to pool cohorts would be even more beneficial for identifying trends. Some subspecialties within ophthalmology may be more amenable to virtual care than others, such as oculoplastics, where remote visits may be a reliable method for assessing eyelid position and orbital abnormalities. In contrast, neuro-ophthalmologists may find it challenging to obtain a reliable pupil and extraocular movement examination virtually, but these studies are small overall and have low power.
Another consideration is that these 22 studies utilized differing methods of delivering remote eye care. For example, some telemedicine protocols required patients to present in-person to an office for ocular imaging, followed by asynchronous evaluation by offsite ophthalmologists. Other studies used live video visits or telephone encounters without any direct patient contact. Some included studies did not directly state how the visits were performed within their methods or did not provide a detailed description of the setup. The lack of standardization in the care delivery methods makes the results difficult to combine and interpret. While some patients/providers may strongly favor video visits, their answers may differ when trying phone visits instead, but with the current published studies, these differences are difficult to determine. Additional factors such as network reliability and platform usability may be important in patient and provider experience with teleophthalmology, but were not discussed in many of these studies.
We note several limitations to this study. Demographic data about the providers and patients could provide useful insight, but variation in the way these data were collected between studies made it difficult to pool and report. In addition, a rating of study quality could be useful for future studies. However, assessing study quality based on design is challenging because it involves multiple nuanced factors such as sample size, methodology, and bias control. These elements vary by context and cannot be easily captured in a single score, making expert judgment essential.
Telemedicine has not become a mainstream practice in ophthalmology, although it is difficult to pinpoint the exact reasons. Studies assessing teleophthalmology have increased since the onset of the COVID-19 pandemic, with 18 of the 22 studies included in this review published in 2020 or later. Despite a growing interest in remote delivery of medical care postpandemic, further investigation into teleophthalmology is needed before it can become widely implemented, and generalized conclusions are only possible if small studies can be pooled to have higher power. Here, we review the landscape of published studies assessing patient or provider opinions on teleophthalmology through direct surveys, identifying trends where evident. The development of standardized guidelines and evaluation metrics specific to teleophthalmology would be a worthwhile goal for national and international ophthalmological organizations, to draw evidence-based conclusions about the utility of teleophthalmology and promote its implementation.
Footnotes
Authorship Contribution Statement
T.E.F. analyzed the data and prepared the article. G.D.L. conceptualized the project and contributed to article preparation. All authors read and approved the final article.
Availability of Data
Additional data available from the corresponding author upon reasonable request.