
Abstract
Patients living with traumatic spinal cord injury (TSCI) often have multiple medical issues and chronic pain requiring potentially several prescription medications. Taking multiple medications can lead to adverse side effects and drug interactions. The main objective of this study is to measure polypharmacy among TSCI patients over a 20-year period and evaluate associated injury characteristics and clinical factors. This study is a retrospective analysis of a population-based cohort of patients with TSCI between 2001 and 2022. Utilizing linked health care data, patients with TSCI were identified. All community-dispensed medications were identified during the first 365 days after discharge. The cumulative polypharmacy method was utilized (average of ≥5 medications over four quarters of the year). Summary statistics were used to evaluate rates of polypharmacy. A multivariable logistic regression identified demographic and clinical characteristics associated with polypharmacy. A total of 3142 patients were identified, 964 (30.7%) patients had polypharmacy with ≥5 medications averaged per quarter in a 1-year period after discharge from the hospital. Factors associated with polypharmacy were age 65 and older (OR = 3.1, p < 0.001), female (OR = 1.5, p < 0.001), and a higher pre-existing comorbidity burden (OR = 3.8, p = 0.030). The study found that it is common for patients to experience polypharmacy in the first year after their injury. While polypharmacy is not inherently harmful, patients with polypharmacy should be identified and closely monitored for unnecessary medications, and policymakers should evaluate the role of regular medication reviews to avoid complications and poor outcomes.
Keywords
Introduction
Traumatic spinal cord injury (TSCI) is a life-changing event that can leave patients with permanent motor, sensory, and autonomic dysfunction. 1 TSCIs affect patients, their families, and caregivers and have significant implications for health care systems, including increased costs and utilization of health care services. 2 It has been shown that TSCI is most likely to occur among young adult males involved in motor vehicle collisions (MVCs), though rising rates of TSCI have been recently reported among the elderly population suffering low-energy falls.3,4
Upon initial presentation, patient care can be complex due to multiple injuries, pre-existing comorbidities, and higher injury severity. 5 During the time after hospital admission, patients living with TSCI are known to experience complex medical problems, especially in the first year after discharge. 6 The most common problems include genitourinary dysfunction, gastrointestinal irritability, cardiac issues, mental health conditions, and musculoskeletal injuries, often treated with prescription medications. 7 For TSCI, the most common classes of medications include: sedative-hypnotics, nonbarbiturates, anxiolytics, antispasmodics, 8 serotonergic systems agents (e.g., selective serotonin reuptake inhibitors and serotonin-norepinephrine reuptake inhibitors), 8 antihypertensives,9,10 narcotics, 11 anticonvulsants, 12 skeletal muscle relaxants, prokinetics, 13 and tricyclic antidepressants.
The concept of polypharmacy is defined as being treated with multiple medications simultaneously. In most current literature, the definition of polypharmacy has been defined as 5 or more concurrent medications, although definitions can vary.14,15 Methods to identify polypharmacy in previous literature are often based on a simple count of prescribed medications over a single calendar year. Polypharmacy can be appropriate, especially when the combination of the drugs is not causing harmful interactions or side effects and when each medication is necessary and prescribed for a clear indication. However, patients who experience polypharmacy are reported to have poorer medication adherence because of complicated drug regimens and face inappropriate prescription leading to disease progression, hospitalizations, and failure of treatment.16,17 Managing multiple medications often involves coordination between the primary care provider (PCP) and pharmacist who dispenses the medications. 18 Due to the complexity and spectrum of TSCI, the incidence of polypharmacy among TSCI patients has been reported to be nearly double the rate of control populations. Patients with polypharmacy are at risk for complications and poor outcomes, especially among high-risk and geriatric patients.19,20 Previous research has also noted that 92% of TSCI patients were on medications that put them at high risk for drug-related adverse events, ranging from mild reactions such as a rash to severe events like delirium and even early death.21,22 Older TSCI adults have been noted to suffer extensively from polypharmacy, exacerbating conditions such as disability, frailty, cognitive issues, and mobility.14,20 Thus, understanding the prevalence of polypharmacy among patients with TSCI and identifying those at highest risk is essential for guiding targeted interventions and improving medication safety.
There is a paucity of literature measuring the prevalence of prescribed medications, the rate of polypharmacy, and the factors associated with polypharmacy among TSCI patients. This study aims to measure dispensed medications among TSCI patients in British Columbia (BC), Canada, over a 20-year period to identify the prevalence of polypharmacy in the first year after discharge from acute care. Further, this study seeks to evaluate injury characteristics, temporal changes in polypharmacy, clinical and demographic factors associated with polypharmacy.
Materials and Methods
Study population and data source
This study was based on a retrospective analysis of a population-based cohort of patients with TSCI whose injuries occurred between January 2001 and December 2022. This population-based study took place in BC, which is a province in Canada that has over 5 million residents and represents about 13% of the Canadian population. Cohort members were identified through population-based analyses of linked population-level administrative datasets. This study utilized linked hospital discharge records, physician billing data, and provincial demographic statistics information. 23 For this study, TSCI patients were linked across several sources of data through Population Data BC, including the hospital discharge summaries in the Discharge Abstract Database (DAD), BC’s Vital Events and Statistics—Deaths, Medical Services Plan (MSP), PharmaNet, WorkSafeBC, the BC Trauma Registry, and the Rick Hansen Spinal Cord Injury Registry (RHSCIR).24–32 The protocol for linkage has been described elsewhere. 33 TSCI cohort members were identified using International Classification of Diseases (ICD) 10-CA codes in the DAD (See Supplementary Appendix). The codes were validated elsewhere and included all levels and severity of TSCI, including cervical, thoracic, lumbar, complete/incomplete injuries, and cauda equina syndrome. 34 Ethics approval was obtained from the University of British Columbia Research Ethics Board (REB#: H22-02696).
Clinical and demographic variables
Variables included in the analyses were extracted from the DAD from the hospitalization due to the injury and included age (categorized as <35, 35–64, ≥65), sex (male or female), Charlson Comorbidity index (0, 1, 2, ≥3), 35 urban or rural place of residence, surgical treatment (Yes or No), and length of acute hospital admission (in days). Clinical variables were extracted and validated through the DAD/RHSCIR and included the date of admission, date of injury, mechanism of injury, spinal column level (cervical, thoracic, lumbar, sacral/cauda equina), Injury Severity Score (ISS) (categorized as <25 or ≥25), 36 neurologic injury (complete vs. incomplete), functional impairment (paraplegia vs. tetraplegia), presence of traumatic brain injury, and mechanism of injury (MVC, falls, or other). Worker claims (Yes or No) were determined based on ICD-10 codes indicating a work-related claim through the WorkSafeBC dataset. Socioeconomic status (SES) at the time of injury was determined by using the Quintile of Adjusted Income per Person Equivalent (QAIPPE), which is a measure of neighborhood income per person equivalent, adjusted for household size, and based on census summary data from Statistics Canada, independent of this study. 37 In the QAIPPE, the first quintile represents the lowest SES, and the fifth quintile represents the highest SES. Whether the patient was treated at a specialized or nonspecialized center was identified in the DAD. 38 A specialized center was designated according to recommendations by Parent et al. 39
Prescription medication data and polypharmacy
All medications dispensed by outpatient pharmacies or community-based pharmacies are reported in PharmaNet, a population-based repository of dispensed prescription medications. 40 No inpatient medication is recorded in this repository. 40 Pharmanet includes information regarding each drug, including duration of supply and dispensing dates of all medications. All individual prescriptions were identified using unique Drug Identification Numbers (DIN). All DINs representing over-the-counter medications, supplements, herbal medications, vaccinations, and pharmacist medication reviews were excluded; medications only given as a one-time dose were also excluded. Each DIN was matched with a corresponding World Health Organization Anatomical Therapeutic Chemical (ATC) code and grouped into different classifications using the first four characters of the ATC. 41
The outcome of this study was the identification of individual-level polypharmacy within the first 365 days after being discharged from acute care for TSCI. Utilizing the cumulative polypharmacy method, the count of unique prescriptions for each participant was averaged over each quarter-year period in the first 365 days post-discharge.42,43 If patients were identified at any time point as receiving 5 or more medications using this average cumulative calculation, then they were considered to have experienced polypharmacy. Patients were further analyzed using a definition of 10 or more medications to represent a higher threshold of the number of dispensed therapies to be considered polypharmacy. 15
Statistical analysis
Demographic and clinical statistics were compared between those identified as having polypharmacy or those who did not meet criteria for polypharmacy with ANOVA for continuous variables and chi-square tests for categorical variables. A summary of the classes of drugs, based on ATC categories, was calculated for the top 10 prescribed classes of dispensed medications. The percentage of patients who experienced polypharmacy was visually assessed using a scatter plot for each individual year included in the 20-year study. The temporal trend was evaluated using simple linear regression methods.
Measuring associations of clinical and injury characteristics with polypharmacy was evaluated using a multivariable logistic regression model. Model fit was evaluated using the AIC and evaluation of the residuals. Missing data were addressed by applying multiple imputation methods with chained equations 44 and 30 imputations. Pooled standard errors for the covariates were calculated using Rubin’s rule for combining multiple imputations. 45 Statistical significance was set as two-tailed hypothesis testing when the p value was <5%.
Results
A total of 3142 TSCI patients were identified in the cohort, with 2151 (68.5%) male and an average age of 54 (SD 20.2) years. Of these 1108 (35.3%) patients were 65 years or older at the time of their injury. The average LOS for acute care prior to discharge was 60.6 (SD 103.3) days. Most patients had cervical spine injuries (56.9%) and incomplete neurology (83.9%), with a large proportion of injuries attributable to a fall mechanism (40.5%). Patients with ISS 25 or higher represented 22.5% of the cohort. See Table 1 for complete demographic and clinical variables.
Clinical and Demographic Data for Cohort of TSCI Patients from 2001 to 2022
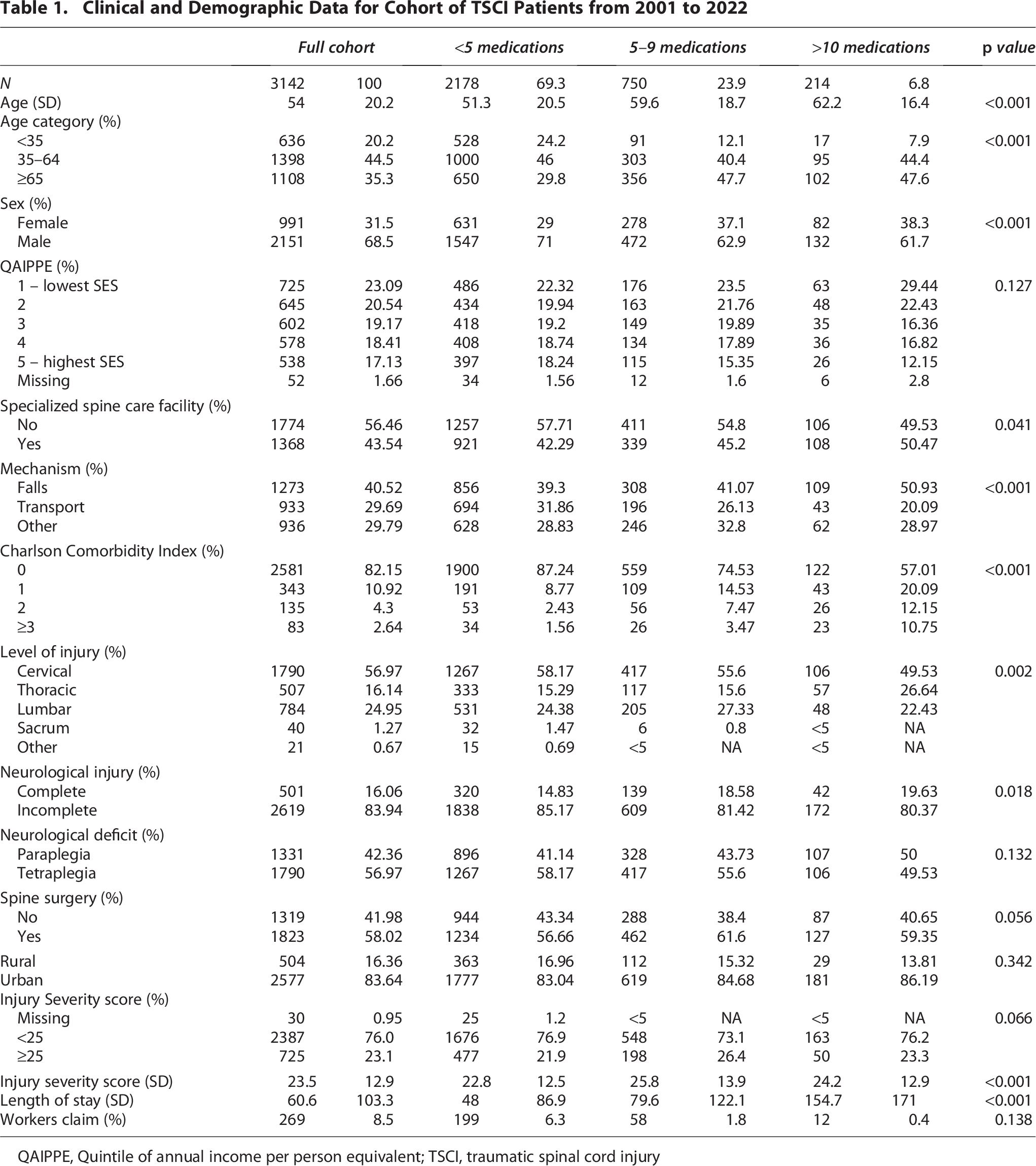
QAIPPE, Quintile of annual income per person equivalent; TSCI, traumatic spinal cord injury
Nine hundred and sixty-four (30.7%) patients had polypharmacy identified with 5 or more dispensed medications, and of those, 214 (6.8%) had polypharmacy when defined as 10 or more dispensed medications.
Over the course of 20 years of administrative data, there was an increase in the prevalence of polypharmacy within 1 year after hospital discharge. The proportion of TSCI patients with ≥ 5 dispensed concurrent medications increased from 23.4% in 2001 to 39.8% in 2022 (p < 0.001; see Fig. 1). Those prescribed ≥10 medications increased from 5.2% to 8.9% over the same time (p < 0.001; see Supplementary Fig. S1).

Rates of polypharmacy over the study period (2001–2022) for patients prescribed >5 medications and defined as polypharmacy vs. those with <5 medications defined as no polypharmacy.
Clinical and sociodemographic factors associated with a higher likelihood of polypharmacy were: those 65 and older (OR = 3.1, p < 0.001), female sex (OR = 1.5, p < 0.001), and higher pre-existing comorbidity burden (CCI = 2, OR = 2.9, p = 0.002, CCI > 3 OR = 3.8, p = 0.030). Further, the longer the length of stay in acute care, the more likely polypharmacy occurred (OR 1.02, p < 0.001). There were no association between polypharmacy and the mechanism of injury, level of injury, neurological status, workers’ compensation claim, or SES (see Table 2 for full model results).
Multivariable Logistic Regression for Patients Identified as Polypharmacy (≥5 Medications) and Various Clinical and Demographic Factors. Odds Ratio and 95% Confidence Intervals Presented

Bold text represents statistically significant values p < 0.05.
Traumatic brain injury.
Quintile of adjusted income per person equivalent.
Injury Severity Score.
CCI, Charlson Comorbidity Index.
When evaluating the ATCs’ most prescribed medications within the first year of discharge in the cohort, opioids (39.1%), antidepressants (30.6%), and gabapentinoids (30.5%) were the most prescribed. The top 10 prescribed medications for this cohort can be seen in Table 3.
Top 10 Prescribed Drug Classifications by ATC Code for TSCI Patients in First 365 Days after Discharge from Hospital

Discussion
This study calculated the prevalence of polypharmacy in a population of TSCI patients over a 20-year period. Overall, 30% of patients experienced polypharmacy of 5 or more medications dispensed concurrently one year after hospital discharge. This study is the first, to the best of our knowledge, to utilize the cumulative polypharmacy method with a unique population-based prescription medication database (PharmaNet). Patients at higher risk for polypharmacy were those who were females, 65 years of age or older at the time of their injury, presented with a higher comorbidity burden, and had a more severe injury. Further, opioids, antidepressants, and analgesic/gabapentinoid medications were the most prescribed in patients 1 year after discharge.
The prevalence of polypharmacy found in this study was lower than other research reported for patients with TSCI, with reported ranges between 31% and 87%.14,21,46 Variations in rates of polypharmacy have been an issue in current pharmaceutical literature due to variations in the definitions of polypharmacy as well as the methods used for calculation using administrative or clinical data. The operational definition of polypharmacy continues to vary in both the number of medications considered polypharmacy and the period over which this is evaluated.15,42 This analysis utilized a method for calculating polypharmacy described as a cumulative method, evaluating the number of unique medications dispensed in a given quarter and the average over a year. This method has been shown to reflect polypharmacy more accurately among patients when compared with other methods, such as the uninterrupted model or various count methods. 43 Lower rates of polypharmacy could be due to a stricter definition of polypharmacy applied in the cumulative method. Further variations seen within the literature are likely due to differing prescribing practices and patterns by clinicians for patients with TSCI. In the Canadian context, the lack of universal coverage for prescription drugs in Canada’s provincial public health care systems would also contribute to potential financial barriers to appropriate medications. 47
This study identified that patients who were 65 and older are at a higher risk of being prescribed multiple medications compared with younger patients. Existing literature identified that polypharmacy among elderly patients has a higher risk of drug-related interactions that can lead to a higher incidence of falls, cognitive impairment, delirium, and mortality.20,48 Together, our results strengthen previous reports calling for careful monitoring of prescriptions among elderly patients to help manage and reduce the likelihood of complications.14,49,50 This study also found significant associations between pre-existing comorbidity burden (CCI ≥ 3 OR = 3.8, p ≤ 0.001) with polypharmacy. In a scoping review of polypharmacy among patients with TSCI, pre-existing comorbidities are associated with a higher incidence of polypharmacy after injury. 46 Interestingly, this study found no associations between the level of injury or severity of neurological injury with polypharmacy. Previous studies indicated that patients with tetraplegia experience higher levels of longitudinal secondary complications, which may require more prescriptions, leading to polypharmacy, which may not have been fully revealed in the study during the first year after injury.51,52 Further research is needed to see if there are increased rates of polypharmacy using more specific neurological injury characteristics, such as motor scores and other functional measures, with long-term data. Despite efforts by numerous medical organizations to lower rates of polypharmacy and avoid potential drug–drug interactions, 20 this study found a trend of increasing proportion of patients with TSCI who have polypharmacy in the first year after injury. This could be due to several factors that are known to influence polypharmacy and are occurring in this cohort, including the shifting demographics in the incidence of TSCI in those who are over 65. 53
In the study, the most dispensed drugs for patients with TSCI were opioids (39.1%), antidepressants (30.6%), and gabapentinoids (30.5%). Pain medications are prescribed frequently in patients with TSCI, given that up to 60% of patients report severe or excruciating pain as a result of neuropathic, visceral, and musculoskeletal pain. 54 Opioids are often among the most prevalent drugs utilized for pain in patients with TSCI, with existing literature supporting the findings of this article, estimating between 30% and 40% of patients being prescribed opioids.55,56 Among the Canadian population, there has been a considerable decrease in the rate of opioid prescribing. 57 However, there is limited data on rates of opioid prescribing for patients with TSCI over time and whether this has decreased as well. Supplement pain medications, such as antidepressant medications, are prescribed not only for depressive symptoms but can also be used as adjuncts to help treat neuropathic pain along with gabapentinoids.58,59 When patients are placed on multiple different pain medications, as is often the case in polypharmacy, there is an increased risk of opioid overdose and mortality. 60 Other common medications prescribed included antacids, lipid-modifying agents, antihypertensives and muscle relaxants, which is consistent with the literature in this population. Patel et al. and Kitzman et al. found that the most common medications were dispensed due to pain, constipation, muscle spasms, hypertension, and depression.21,61
Implications for clinical practice and policy
The detailed analyses regarding the rates of polypharmacy allow policymakers to understand the scope of concurrent drug use among TSCI patients. There are several key points that must be addressed when developing treatment pathways for patients with TSCI. First, prior to discharge, consultation with pharmacists and PCPs should ensure that patients are on an appropriate medication regimen to manage their medical risks, as in some cases, multiple medications are necessary to treat complex situations. Efforts should be made to limit risks with polypharmacy before discharge, especially in elderly patients admitted to hospital with TSCI. Further, regular follow-up care with pharmacists from specialized TSCI referral centers would ensure continuity and medication management.
Second, polypharmacy rates are increasing, and this not only has potential health concerns but also economic implications for patients with the costs of certain medications prescribed. In BC, this coverage is provided by workers’ compensation, disability coverage, public drug insurance programs or individual personal drug insurance plans, which many patients will not have. 62 In fact, in this comprehensive cohort of individuals with TSCI, <10% of TSCI patients were associated with a workers’ compensation claim. In the Canadian context, some portion of patients will have to pay a component or all costs out-of-pocket, which is often not sustainable and impacts adherence to medications.63,64 There have been repeated calls in Canada for universal prescription drug coverage to help improve the Canadian health care system and ultimately reduce spending. 65 Policy makers must continue to make strides to improve access to essential medicines and ensure that all medications prescribed are necessary.
Finally, once TSCI patients are discharged into the community, there is a need for multidisciplinary teams with experience managing the myriad of conditions that they suffer from to judiciously ensure that they are on appropriate medications. Careful monitoring and periodic reassessment by PCPs and pharmacists must be done to avoid adverse drug-related events and to make sure their treatments are aligned with patients’ goals and ongoing medical needs. The management of complex medical conditions is becoming increasingly reliant on multidisciplinary teams, which, in TSCI, have improved outcomes and satisfaction with care. 66 Monitoring should happen in both patients discharged from specialized centers and nonspecialized centers, as polypharmacy risk does not differ between care setting discharge (OR = 1.1 p = 0.196) and is determined by patient characteristics. Investments in a team-based approach would help to manage polypharmacy in patients, decrease costs, optimize care, and improve outcomes.
Strengths and Limitations
This research has several limitations that are inherent to this study that should be noted. This study was completed using patients in a single province within Canada and potentially will not be representative of other regions in Canada. Drug information was obtained using an administrative dataset (Pharmanet) and is dependent on correctly entered DIN and ATC codes, in which there is the potential that medications were recorded in error. Further, even though medications were dispensed, there is no information on whether true adherence to medications was maintained as prescribed. Also, when utilizing the cumulative polypharmacy methods, it does not identify true polypharmacy of overlapping medications but a gross average of potential interactions. Further research would be required to look at the extent to which there are direct periods of time with overlapping medications and whether this influences both patient outcomes and the prevalence of polypharmacy in this population. Due to the limitations of administrative data, AIS grading was not included in the analysis, which is generally a clinical standard for TSCI research. Additionally, no inpatient medication was captured, potentially adding polypharmacy heterogeneity in patients who had varying LOS. Pre-injury medication was not measured, potentially confounding if the injury caused polypharmacy or was already present. Finally, this study looks at rates of polypharmacy 1 year after discharge from the hospital and cannot comment on polypharmacy at future dates.
Conclusion
TSCI is a devastating condition that leads to multiple medical complications. In this population-based cohort, roughly 30% of patients experienced polypharmacy. Older patients, females, and those who present with pre-existing medical comorbidities are more likely to have concurrent medication use in the first year after injury. Given the complexity of TSCI, patients should be carefully monitored in their first year for appropriate medications by a multidisciplinary team. Further research is needed to evaluate polypharmacy between 5 and 10 years to evaluate whether long-term complications from spinal cord injury lead to higher rates of polypharmacy as seen in other studies.
Transparency, Rigor, and Reproducibility Statement
Data utilized for this study were administrative data provided by Population Data BC for analysis. The information that was utilized came from a request of 2001 to 2022 administrative data. Population Data BC data use agreements prohibit sharing. Access to data provided by the Data Stewards is subject to approval but can be requested for research projects through the Data Stewards or their designated service providers. The following data sets were used in this study: (Consolidation file [includes demographics, registry, and census geodata], Hospital Separations, MSP, Vital Events and Statistics—Deaths, RHSCIR, BCTR, Vertebase/QISpine). You can find further information regarding these data sets by visiting the PopData project webpage at: (https://my.popdata.bc.ca/project_listings/15-119/collection_approval_dates). Due to the study’s retrospective nature, it was not pre-registered nor was the analysis. The sample size was determined by the number of patients diagnosed in hospital with TSCI. The study utilized validated ICD-10 code definitions for inclusion. After screening, 3622 patients were included. Investigators knowledgeable in the relevant topic assessed key inclusions and outcomes to report on. Statistical analysis was performed on SAS. Sample size and power calculations were not conducted, as the dataset obtained was exceptionally large, ensuring the study was adequately powered.
Inferences, opinions, and conclusions drawn in this publication are those of the author(s) and do not reflect the opinions or policies of the Data Steward(s).
Authors’ Contributions
M.B.: Conceptualization, methodology, writing—original draft, writing—review and editing, visualization, and supervision. A.B.: Writing—original draft, visualization, and writing—review and editing. V.K.N.: Conceptualization, project administration, writing—review and editing, and funding acquisition. N.R.K.: Writing—review and editing and project administration. B.K.K.: Writing—review and editing and supervision. S.T.W.: Writing—review and editing and supervision. G.L.: Software, formal analysis, data curation, and writing—review and editing. J.M.S.: Conceptualization, writing—original draft, writing—review and editing, and supervision.
Footnotes
Acknowledgments
The authors thank the following individuals for their contributions to the acquisition and preparation of data for this study: Jerome Buenaventura, Susan Jaglal, Shawna Cronin, Suzanne Humphreys, Jijie Xu, Melody Chen, Zeina Waheed, and Nader Fallah. They thank Allan Aludino, Leilani Reichl and the Spine Team and Mei Chong, Lori Korchinski, Jaimini Thakore, Recep Gezer, and the rest of the Trauma Services BC team for their assistance in data provisioning and support.
Author Disclosure Statement
B.K.K. is the Canada Research Chair in Spinal Cord Injury and Dvorak Chair in Spine Trauma at the University of British Columbia. The authors declare no competing interests related to this work.
Funding Information
This work was supported by funding from the Praxis Spinal Cord Institute, the Canadian Government, and the Government of British Columbia.
Supplemental Material
Abbreviations Used
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.