
Abstract
Patients who sustain a mild traumatic brain injury (mTBI) experience a variety of clinical trajectories. Recent efforts to identify mTBI subtypes have begun to describe observed phenotypic variability. Clinical applicability of these subtypes is limited due to critical variations in each subtype’s defining characteristics and limited inclusion of objective data. Here, we review mTBI literature that describes subtypes at various timepoints following injury. We describe five predominately symptom-based subtypes (cognitive, somatosensory, vestibular-ocular, headache, and neuropsychiatric [affective/behavioral]). Each of these subgroups has been reported at separate timepoints postinjury, with the majority of studies describing symptom clusters in the acute and subacute recovery period. Analysis of each subgroup indicates significant overlap and ambiguity within the currently described symptom-based subtypes of mTBI. Additionally, inconsistent terminology within symptom description and subtyping nomenclature limit the ability to compare among one another. We suggest that improved understanding of possible biological processes that contribute to certain clinical trajectories may be identified by incorporating objective assessments, biomarkers, neuroimaging, and genetic analysis into future mTBI subtyping analysis. In doing so, advancements toward individualized symptom management, recovery, and improved care for our mTBI community are possible.
Introduction
Many brain-injured individuals require personalized care from a multidisciplinary team to address patient-specific symptoms. These symptoms may occur after a single mild traumatic brain injury (mTBI) experienced through sport, assault, motor vehicle collisions (MVC), or falls. 1 While sport-related concussions (SRC) are estimated to make up at least 30% of all mTBIs, injuries that occur through sport, MVC’s, falls, and assaults are likely under-represented due to delayed presentation, self-management of symptoms, and under-recognition. 2 Other, less studied populations at risk for mTBI include those who experience intimate partner violence, child abuse, and abusive head trauma, which often result in repetitive mTBIs on a spectrum of severity and are also likely under-identified.3,4 mTBI pathophysiology influences symptom development that consists of unique biomechanical forces resulting in an acute neurometabolic cascade, altered neurotransmission, evolving neuroinflammation, and injury-dependent neuronal reorganization and connectivity.5–11 Variations in adaptive and maladaptive neuromodulation result in cognitive, somatic, vestibular, ocular, affective, and/or behavioral symptoms that impact a patient’s daily life.12–28
Although diverse mTBI-induced symptoms result in a heterogeneous patient population, commonalities exist among patient symptoms and their evolution throughout recovery. As with many other neurological conditions, stratifying patients by commonly experienced symptoms, pathophysiology, and underlying risk factors enables better understanding of patient heterogeneity and guides individualized treatment. Historically, the idea that heterogeneous conditions may have subtypes was conceptualized within the field of psychiatry in an initial effort to better understand schizophrenia. 29 It was posited that underlying genetic factors, in addition to environmental components, may result in separate clinical trajectories. This concept, later defined as endophenotypes, was expanded to describe that the basis of complex disease may be the result of “… neurophysiological, biochemical, endocrinological, neuroanatomical, cognitive and neuropsychological (including configured self-report data) in nature.” 30 The strictest definition of endophenotypes implies that a disease has a genetic underpinning. However, many often use the term for various complex disease subtypes without an identified genetic basis for the observed phenotypic variability. Efforts to better define heterogeneous diseases with a similar clinical presentation resulted in the establishment of endotyping.31,32 Initially discussed in pulmonary and oncology literature and utilized in personalized medicine, endotypes reflect a “subset of a disease, defined functionally and pathologically by a molecular mechanism or treatment response.”33–36 Endotyping allows subtyping of physiologically complex conditions through evaluation of differences in biomarkers, mechanisms or treatment response. In the context of respiratory conditions (i.e., asthma or ARDS), it has been suggested that certain phenotypes may be the result of multiple endotypes, although the defining characteristics of what constitutes an endotype require further consensus. One recent definition proposes that an endotype must have at least five of seven components consisting of clinical characteristics, biomarkers, physiology, genetics, histopathology, epidemiology, and treatment response, yet it is uncertain if this criteria will be adopted by other fields or diseases. 34 The concept of identifying endotypes thus provides an intriguing approach to assist in the subtyping of complex conditions that extend beyond a single biological underpinning.
Broader consensus on the application of subtyping within mTBI is needed to describe the observed phenotypic variability to help facilitate clinical advancements. Even though mTBI subtypes are apparent in clinical settings, a consistent framework or approach for classifying them has not been established. Current approaches to mTBI subtyping include terminology such as symptom cluster, subgroup, endotype, and endophenotypes. However, studies often use these terms interchangeably, without consistent definitions, and without an identifiable biological underpinning. Further, the makeup of many subtypes are defined by subjective, symptom-based assessments with few including objective biomarkers (i.e., physiological parameters [heart rate, blood pressure]), neurophysiological studies (electroencephalogram [EEG], magnetoencephalography [MEG]), neuroimaging (computed tomography [CT], magnetic resonance imaging [MRI]), serum molecules, and genetic markers. This results in inherent ambiguity, making it challenging to discern if similar symptoms at different time points are indicative of the same or separate pathophysiology, particularly for symptoms that may be attributed to multiple post-mTBI sequelae. Thus, the clinical impact of currently defined mTBI subtypes is limited by challenges in comparing groups across different cohorts. We suggest that the first step in improving mTBI subtypes is to adopt a unified classification system that allows for comparison among clinical cohorts to improve understanding of clinical trajectories and phenotypic variability. One possible structure is proposed in Table 1 and utilized throughout this review. Here, we propose nomenclature that classifies current mTBI subtypes with a clear hierarchy between the labels of symptom cluster/subgroup, endotype, and endophenotype. While this may be just one possible hierarchical structure for mTBI subtyping, the use of consistent terminology will hopefully begin a conversation that allows for improved understanding and comparison among mTBI subtypes.
Proposed mTBI Subtyping Hierarchy Classification
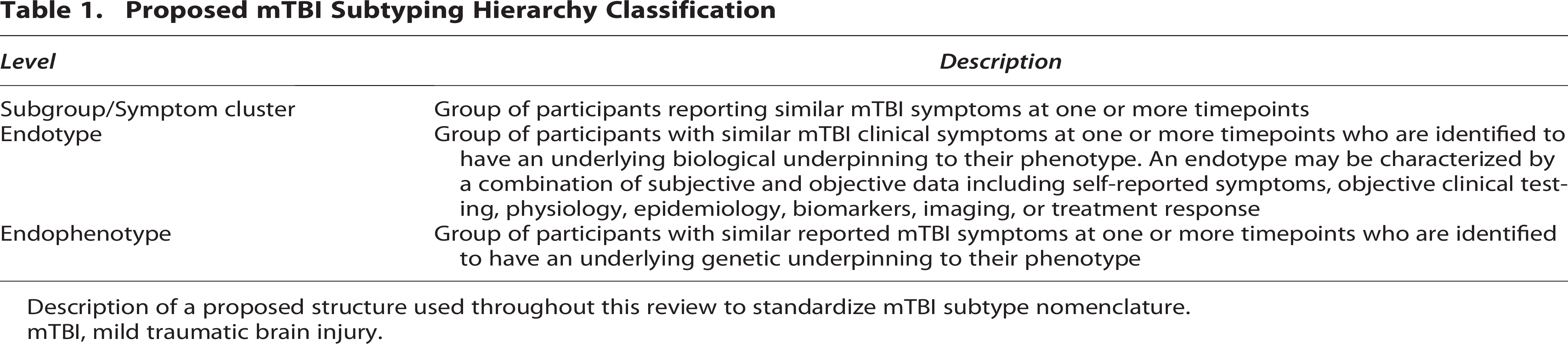
Description of a proposed structure used throughout this review to standardize mTBI subtype nomenclature.
mTBI, mild traumatic brain injury.
One potential goal of examining currently described mTBI subtypes is to better delineate expected clinical trajectories and ideal points for more precise therapeutic interventions. Recently, Pugh et al. reviewed the spectrum of subtypes among all severities of brain injury. 37 Their review identifies multiple ways in which TBI has been subcategorized including thorough analysis of symptom-based profiles, severity-based profiles, and analysis of additional diverse post-injury metrics. Throughout their analysis, it was determined that four to five subtypes were often identified, although comparison across studies was made difficult given variations among studies and inconsistent methodology. In an effort to better define common subtypes of mTBI, Lumba-Brown et al. and the Concussion Subtype Workgroup described five concussion subtypes (cognitive, ocular-motor, headache/migraine, vestibular, anxiety/mood) and two concussion associated conditions (sleep disturbances and cervical strain) through the use of a meta-analysis of primary literature in the acute timepoint (0–3 days postinjury [DPI]), which included analysis of subjective symptom-based assessments in addition to objective data (neuropsychological testing, Balance Error Scoring System [BESS], King-Devick [KD]). 38 Additional studies have described cognitive, somatic/somatosensory, vestibular-ocular, affective, and behavioral subtypes in mTBI populations.37–52 Yet, variations in subtype description and inconsistent methodology continue to limit the ability to fully characterize the spectrum of possible subtypes following mTBI. In an effort to better understand how mTBI subtypes emerge and evolve, we conducted a narrative literature review that analyzed clinical subtypes following mTBI.53,54 Studies were included if they characterized two or more subtypes based on clinical profiles at any time point (either at baseline or following mTBI) and published prior to the first quarter of 2022. Studies were excluded from analysis if they focused solely on a singular subtype/symptom. Historic classifications of TBI (mild, moderate, severe) are imprecise and characterization with the recently defined CBI-M criteria was not yet able to be accomplished. Studies were excluded if they were not specific to mTBI based on the primary article’s classification. Studies based on moderate and severe TBI were excluded to have increased specificity for time course of symptoms following injury. While patients who sustain more severe TBIs may also demonstrate a range of symptoms, symptom onset/resolution as well as underlying pathophysiology and adaptive/maladaptive processes may occur differently than “milder” injuries. Additional studies that did not subtype patients based on clinical phenotypes (i.e., mechanism, severity) or those that were based on commentaries, editorials, case report/series or reviews were excluded. Studies were classified as sport-related concussion (SRC) if at least 50% of the primary article’s population was related to sport. Individuals who sustain mTBI via sport versus non-SRC injuries (assault, falls, and MVC) may experience different mechanisms that affect outcomes, although a detailed analysis into possible subtypes was limited and beyond the scope of this review. Each study also needed to label or refer to each of their subgroups based on a predominant clinical symptom/phenotype. Following the review of the studies, each subtype was distributed under one of five commonly described subtypes (cognitive, somatosensory, vestibular-ocular, headache, and neuropsychiatric [affective/behavioral]) based on the primary article’s description. A summary of each population, post-mTBI assessments and methodology to identify specific subtypes is described in Table 2. Each of these five subtypes was primarily defined by self-reported, symptom-based assessments. Notably, the subjective nature of symptom-based subtyping resulted in ambiguity and overlap. An analysis between these five subtypes was conducted and it identified the frequent use of ambiguous terms to identify nonspecific symptoms. Together, this resulted in inclusion of the same or similar symptoms across multiple subgroups (Fig. 1, Table 3 [created using tool found at https://bioinformatics.psb.ugent.be/webtools/Venn/]). Violin plots summarizing time course of reported mTBI subtypes are depicted in Figure 2. Together, the lack of specificity in subtype description and characterization has made it challenging to describe consistent mTBI subgroups or clinical prognostication, resulting in limited clinical utility of symptom-based mTBI subgroups.
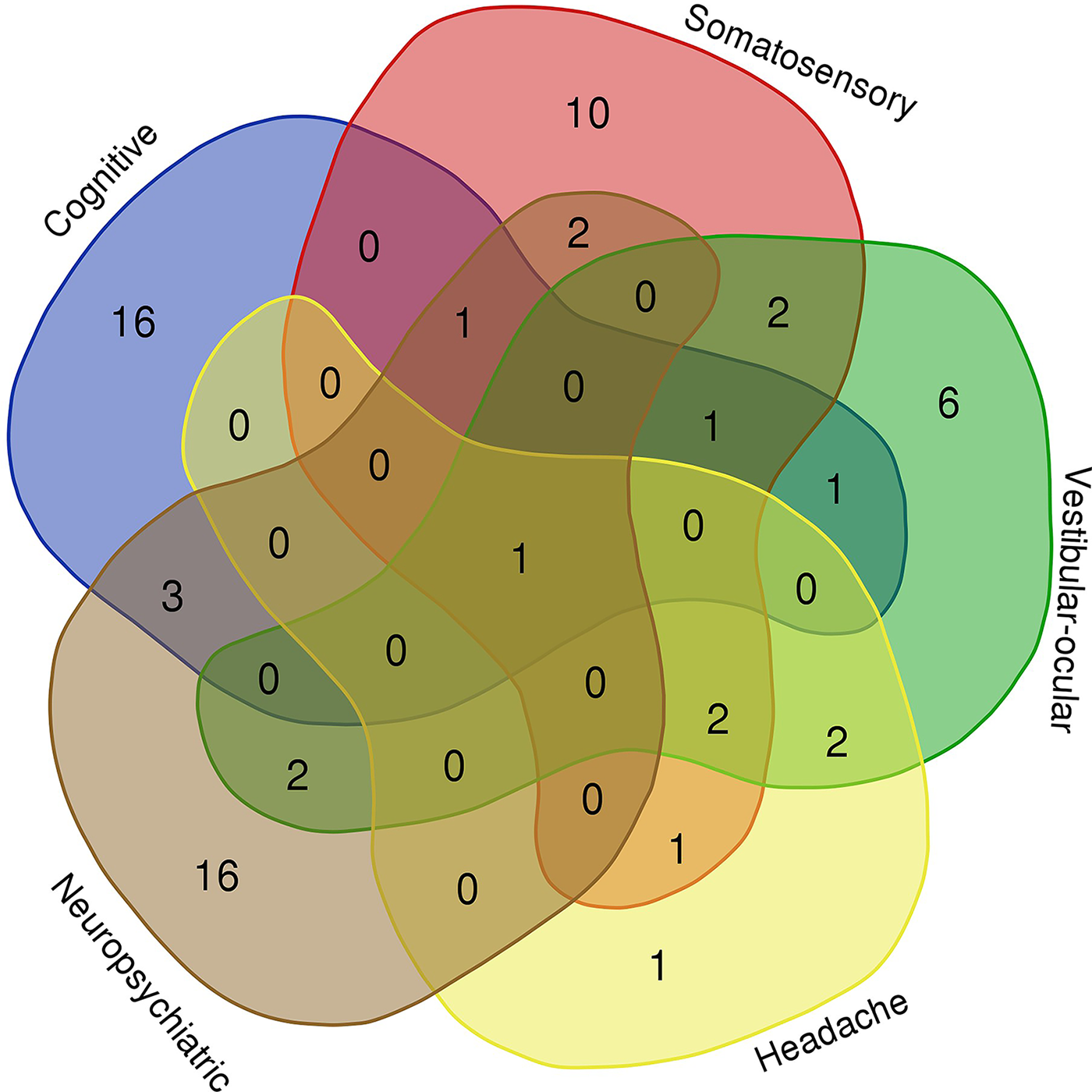
mTBI subtypes. Current literature has described five main mTBI subgroups (Cognitive, Somatosensory, Vestibular-ocular, Headache, Neuropsychiatric). Ambiguous definitions for each subgroup have led to inconsistent symptom profiles. This Venn diagram depicts the number of unique and overlapping symptoms between each subgroup of the studies listed in Table 2. mTBI, mild traumatic brain injury.
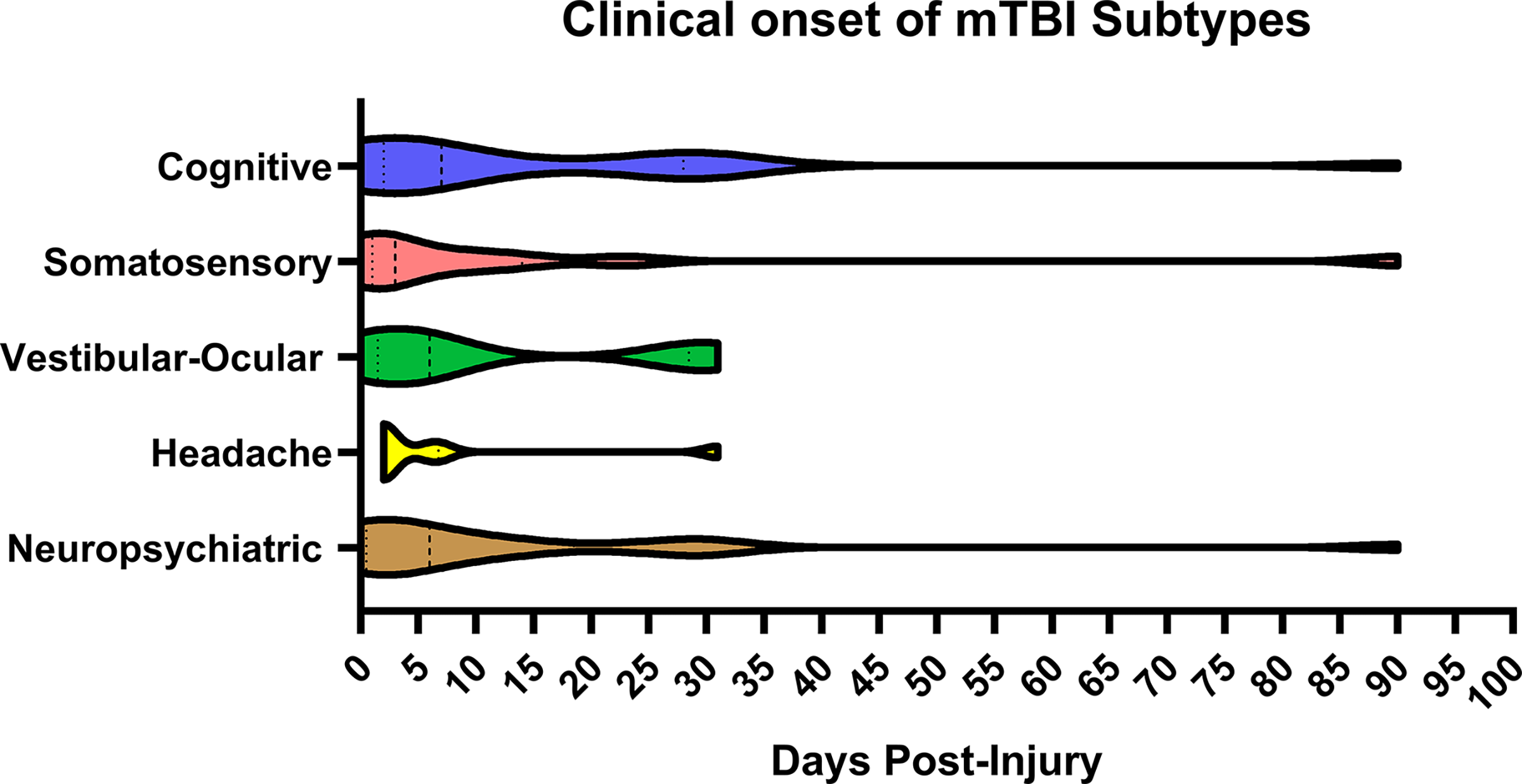
mTBI subtype time course. Violin plots depicting when each of the symptom-based subgroups were reported following injury based on the studies reviewed.
Literature Review of Studies Describing Mild TBI Subtypes
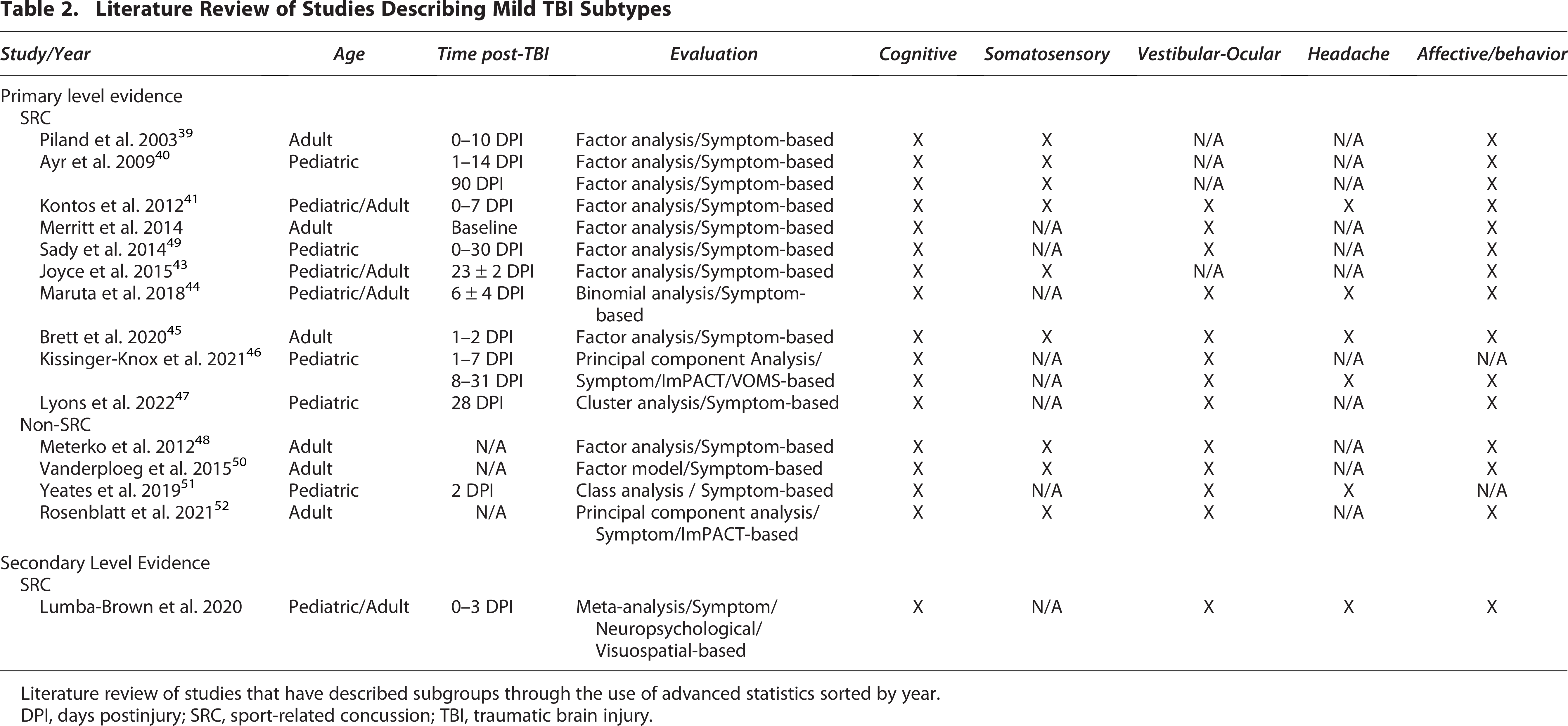
Literature review of studies that have described subgroups through the use of advanced statistics sorted by year.
DPI, days postinjury; SRC, sport-related concussion; TBI, traumatic brain injury.
mTBI Subtype Symptoms. Outline of Unique and Overlapping Symptoms between Each mTBI Subgroup Depicted in Figure 1. Co-Occurring Symptoms Listed under Right Column
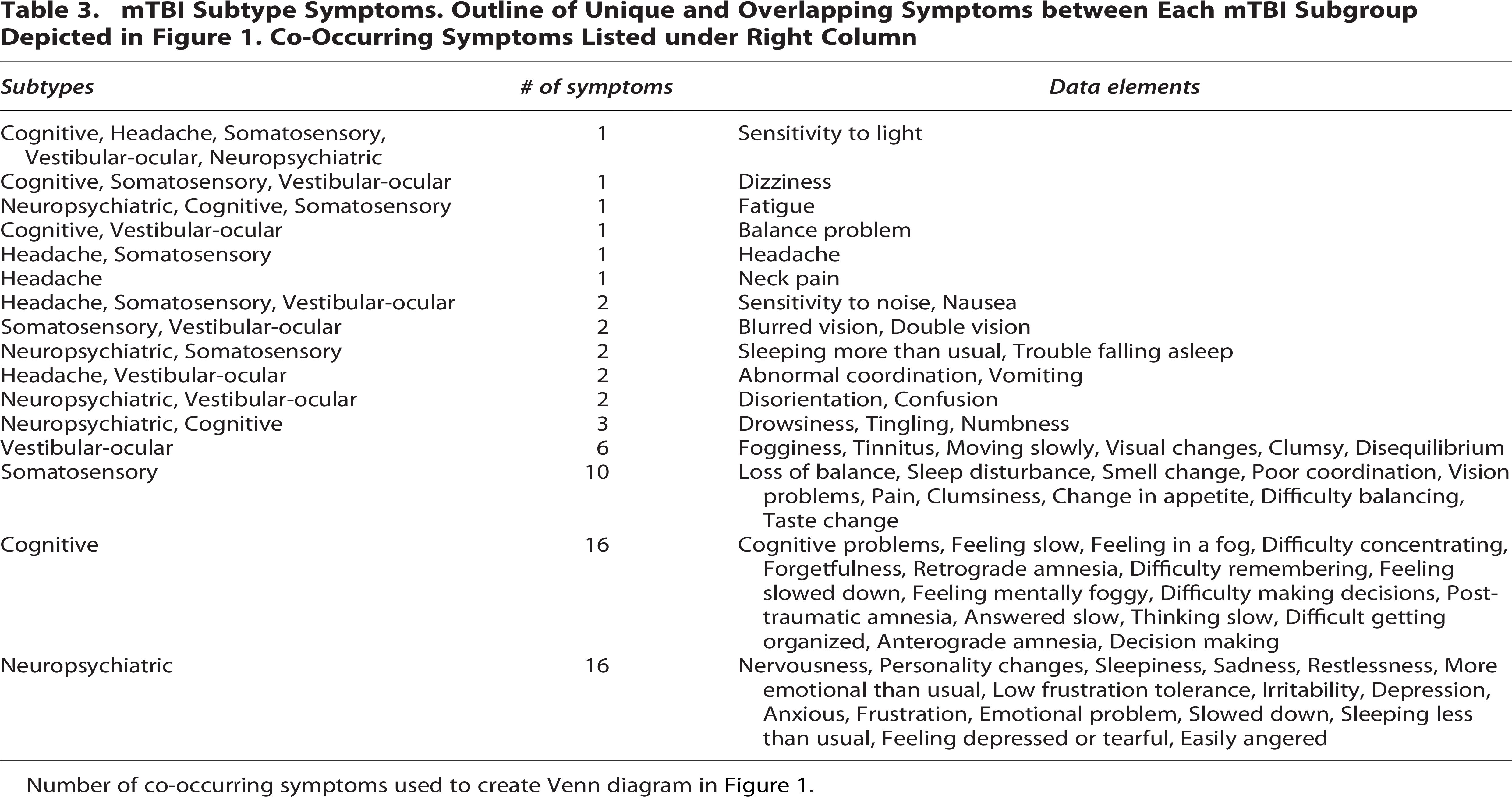
Number of co-occurring symptoms used to create Venn diagram in Figure 1.
The purpose of this review is to synthesize the commonalities and identify inconsistencies among current mTBI subgroup literature utilizing a well-defined taxonomy structure. Given that the majority of mTBI subgroups are currently symptom-based, the limited incorporation of objective biological data precludes categorizing many subtypes as endotypes/endophenotypes. It is possible that improved understanding of current symptom-based subgroups could provide a framework for future mTBI subtypes. Future inclusion of objective testing, including a broad spectrum of biomarkers, may be able to identify a biological underpinning for certain trajectories. As objective outcomes following mTBI become better defined, our objective is to initiate a process that will lead to consensus of clearly defined subtypes with consideration of injury mechanism as well as demographic factors such as age and sex. As a result, we aim to advance mTBI subtype classification and provide a foundation that allows for improved diagnostics, prognostics, and individualized interventions.
mTBI Subtypes
Cognitive
Cognition entails higher-order neurological processes that entail attention, executive function, memory, language, visuospatial skills, and processing of information. Cognitive symptoms following brain injury are one of the more prominent symptoms described by both pediatric and adult patients.38,44 In our review, every study described a cognitive subtype following mTBI, although the specific symptoms and assessments utilized by each study vary (Table 2).38–52 Given the variability in definitions, comparison of each cognitive subgroup’s symptoms was made to the other subgroups (Fig. 1) and described in detail in Table 3. Analysis of these comparisons found that the cognitive subgroup described in this review had the most unique symptom profile by encompassing the fewest overlap of symptoms with other defined mTBI subgroups. While this superficially suggests that cognitive subgroups lend themselves to comparison across studies, each cognitive group was defined using different testing modalities and different cognitive domains/symptoms. Thus, the cognitive subgroup may not be fully representative of the entire spectrum of cognitive symptoms after concussion.
Development of cognitive symptoms in mTBI is multifactorial. Certain pre-injury characteristics impact the development of cognitive symptoms including inherent cognitive ability and greater years of education.42,55 Following mTBI, cognitive symptoms are usually reported immediately or shortly following injury (Fig. 2).39–42,44–46,51 The underlying pathophysiology related to these acute symptoms is typically attributed to TBI-induced alterations to neurotransmission, biochemical processes, neuronal signaling, and energy deficit.8,9 Clinically, concussed patients have been described to experience their worst symptoms at 1 DPI, with improvement over the following 1–2 weeks. 39 However, patients may not recognize their symptoms until cognitive demands increase upon their return to school/work or experience stability in their symptoms. 45 As mTBI patients begin to recover, approximately half report at least moderate cognitive symptoms, with limited overlap of other symptom profiles into the subacute phase. 44 However, cognitive symptoms may also be related to non-specific concussion symptoms, as others have described an association with symptoms of headache, dizziness, mood, poor sleep, fatigue, and drowsiness.46,51 Within these associations, cognitive, migraine, and fatigue (CMF) symptoms have been shown to frequently cluster together. Together, CMF symptoms, as assessed by the Post-Concussion Symptom Scale (PCSS), have better specificity than the total PCSS score in differentiating concussed patients from noninjured controls in both pediatric and adult athletes. 56 The high prevalence of headache in the acute and subacute phase makes it an important consideration when evaluating cognitive concerns as symptoms may be secondary to severe or chronic pain. However, it is not clear if the CMF symptom combination represents a separate mTBI subtype or is influenced by the disruption of a biological mechanism. As time from injury lengthens, lingering cognitive symptoms can be noted in the later subacute to chronic phases of recovery. However, significant interactions with aspects of vestibular, ocular, fatigue, somatic, and emotional symptoms, as well as dysregulated sleep become more evident, raising questions about whether persisting cognitive symptoms arise from the evolution of acute symptoms or are secondary to comorbid conditions.39–41,43,46–48,50,51,57
Identification of those with mTBI-induced cognitive symptoms becomes important for the purposes of diagnosis, management, and prognostication. With regard to prognostication, patients who present with worse early cognitive-related symptoms are more likely to report lingering cognitive symptoms and/or a longer recovery period.56,58 Thus, the presence of cognitive symptoms post-mTBI is a large factor in delaying patients’ return to their typical life, particularly in children. Clinically, this has led to multiple interventions to help the recovery process. Non-pharmacologic therapies and progressive reintroduction into cognitively demanding activities remain the first-line approach, coupled with graduated exercise programs, and in some cases, cognitive rehabilitation.58,59 When symptoms persist, medications such as amantadine and medications used in attention-defecit/hyperactivity disorder (ADHD) may have some benefit in certain cases, although their use remains controversial.58,60–63 Overall, detailed examinations with quantitative assessments in conjunction with objective postinjury biomarkers are necessary to identify underlying biological processes that may be contributing to persisting cognitive symptoms.
Somatosensory
Somatosensory pathways involve complex neural networks to produce aspects of vision, hearing, touch, pain, smell, and taste. The neuroanatomy of these networks leaves certain pathways more vulnerable to the forces of brain injury and prone to disruption.16–21 Brain injury results in changes to these circuits that contribute to symptom development. Unlike evaluation of cognitive symptoms, clinical assessment of somatosensory symptoms remains challenging given the largely subjective nature and limited objective evaluations. Comparison of symptoms used in studies that identified a somatosensory subgroup indicated considerable overlap with each of the other four subgroups (Fig. 1, Table 3). This is particularly appreciated among symptoms that are often associated with headaches. Symptoms related to photophobia, phonophobia, and nausea were found to be categorized within the somatosensory, vestibular, and headache subgroups. The majority of reviewed studies did not identify headache and somatosensory subtypes, although seven did include headache symptoms within other subgroups.39–41,47–50 Clinically, the combination of headache, photophobia, phonophobia, and nausea is consistent with a headache/migraine phenotype. Additional symptoms categorized within somatosensory subtypes identified nonspecific, redundant, and possibly infrequently observed symptoms, hindering the ability to define a uniform somatosensory subtype (Fig. 2).
Evolution of mTBI-induced somatosensory symptoms are the result of multiple individual and injury-specific factors. Preinjury factors including prior education, co-occurring psychiatric conditions, and history of prior TBI may influence the initial development of symptoms.41,55 After injury, somatic symptoms have also been described as typically presenting in the acute phase. 39 Over the first 48 hours, certain symptoms, including sensitivities to light and sound, have been reported to worsen compared to their immediate initial presentation. 45 Delayed onset of specific somatic symptoms including nausea and numbness may occur up to at least 1 week postinjury in adolescent athletes; however, it is unclear how common these symptoms may be. 41 Further identification of broader somatic symptoms, including aspects of headache, dizziness, blurry vision, and decreased energy level have been reported up to 14 DPI. 40 Further, it remains unclear if the etiology of these somatic symptoms experienced in the acute and early subacute phase are experienced as a result of early maladaptive neurocircuitry recovery/reorganization, or are related to nonspecific comorbid symptoms.9,18,19,21,56,64 The persistence of headache, sensitivities to light/sound, nausea, blurry vision, and fatigue into the subacute and chronic phases of recovery have been noted in the pediatric and adult populations up to at least 90 DPI for some individuals, though this is not the norm.40,43 Certain populations may tend to report a longer duration of similar somatic symptoms, particularly in those who are at risk for co-occurring conditions.48,50 It thus remains unclear if each of these symptoms are best explained by a somatosensory subtype or are better characterized among headache and vestibular-ocular subgroups.
Identification and classification of the range of somatosensory symptoms following mTBI is important, although challenging, given the current breadth and overlap with other subgroups. This makes the definition of a somatosensory subgroup difficult and limits its current clinical applicability. It may be that certain symptoms are better described by inclusion in other subgroups such as vestibular-ocular, headache, and neuropsychiatric (affective, behavioral, sleep). There may be a limited, small subset of unique symptoms that suggest a somatic/somatosensory subgroup, though this needs improved delineation in order to aid prognostication and allow for interventions. While certain somatic symptoms such as pain and allodynia may have a distinct underlying neurobiology, the etiology of other symptoms remains less clear at this time.18,19,21,64,65 Current treatment typically focuses on symptom management through behavioral therapies including lifestyle modification and multidisciplinary interventions. While many of the symptoms unique to this subgroup are difficult to quantify, future studies may utilize objective testing (BESS, KD, sleep scores, vision testing) particularly when symptoms overlap in conjunction with to better define the underlying mechanisms in which patients experience these symptoms.
Fatigue
Brain injury subtypes have often included fatigue within the cognitive or somatosensory subgroups. Clinically, fatigue is a challenging symptom given the potential broad etiology and likely does not meet criteria as a separate subgroup or symptom cluster. Fatigue may be viewed as the result of cognitive, physical, and/or affective dysfunction after mTBI and is often reported in all phases of recovery.41,44,47,49,51 Contributing factors to the presentation of fatigue are patient-specific and multi-factorial. Acutely following brain injury, fatigue has been attributed to the increased neurocognitive demand and altered biochemical processes that occur following mTBI.66–68 Of the four studies that identified a separate fatigue subgroup, two reported symptoms in the acute and subacute periods lending credence to the biochemical and energy demand hypothesis.44,45,47,49 In the subacute to chronic phases, altered biochemical processes improve, making fatigue more attributable to alternative etiologies. Throughout the chronic phase of recovery, fatigue is one of the most prevalent symptoms and is related to cognitive and affective subgroups.47,49,66,67,69 The current practice of symptom-based, self-report questionnaires commonly used to investigate fatigue makes it impossible to identify the underlying mechanism. Ultimately, it is likely that fluctuating cognitive, physical, affective/psychiatric, sleep, pain, neuroendocrine, polytrauma, brain-body interactions, and behavioral/environmental factors contribute to produce the symptom of fatigue in patients.47,66,69–71 Fatigue may thus represent a nonspecific symptom that is indicative of one or more underlying disrupted biological mechanisms and would be better categorized based on additional objective testing and possible future endotypes (i.e., affective, autonomic, endocrine, metabolic, etc.). Current clinical evaluation of fatigue should involve consideration of additional medical conditions, such as endocrine abnormalities (GH, TSH, fT4, ACTH, cortisol), given the anatomical vulnerability in mTBI of the pituitary, as well as evaluation of co-occurring affective disorders, sleep dysregulation, or other psychosocial/environmental factors, which may be readily diagnosable and treatable.66,69,72 Future studies and more targeted inquiries aimed at identifying the underlying etiology of fatigue may be able to better delineate a biological basis of the symptom and thus improve individualized approaches to clinical management.
Vestibular–Ocular
Vestibular–ocular reflexes result from the synchronized coordination of cranial nerves and brainstem nuclei to produce features of vision, saccades, coordination, and balance. mTBI results in disruptions to this neurocircuitry and may contribute to the presence of vestibular–ocular symptoms including nausea, vomiting, abnormal coordination, ataxia, dizziness, and disorientation. Compared with other subtypes, the neuroanatomy that regulates these processes is better understood and may help localize symptoms following brain injury to the brainstem.73,74 Despite their interconnectedness, both the vestibular and ocular neuroanatomical pathways are anatomically distinct and may experience isolated symptoms depending on the injured neurocircuitry. Thus, many symptoms within this subtype are likely more specific to a vestibular, ocular or combined vestibular-ocular pathology and should be classified as such rather than being included in other subgroups.
Presentation of vestibular-ocular symptoms often occurs immediately following mTBI (Fig. 2). Visible signs such as the fencing response, slowed eye tracking, and motor incoordination identify those patients who have a high likelihood for having experienced a brain injury.74–76 However, up to 50% of concussed patients may not demonstrate an observable sign. 76 It is unclear whether the demonstration of immediate vestibular–ocular symptoms predicts the development of symptoms at later timepoints. 75 Within the acute phase, vestibular–ocular symptoms are prevalent. 38 Further characterization of adult acute vestibular–ocular symptoms including dizziness, blurred vision, and balance problems indicate that these symptoms are worse immediately following injury and improve within the first 48 hours. 45 This raises the question of whether acute vestibular–ocular symptoms are age-dependent, related to a specific underlying neuropathology, more representative of general mTBI symptoms, or secondary to other subtypes. Vestibular and oculomotor symptoms may continue into the subacute period with differing reports on how prevalent symptoms may be.44,46 Additionally, persisting vestibular–ocular symptoms may be separate from those observed acutely, indicating possible separate pathophysiology. For example, children often report that vestibular symptoms are experienced in the context of profound physical, emotional, migraine, and cognitive symptoms and that vision is their least affected sense.46,47,49 However, objective testing has described that one (or more) visual diagnoses may be present following mTBI including accommodative disorders, convergence insufficiency, or saccadic dysfunction. 77 The etiology of visual symptoms are likely injury dependent and may involve dysfunction of complex neurocircuitry involved in visual processing that is distinct from those noted more acutely. Clinically, it also suggests that a complete visual examination may be helpful even in the absence of reported symptoms. 77 When considering prognostication, acute physical symptoms including difficulties with dizziness, balance, clumsiness, and vision were more predictive of persisting symptoms at 4 weeks while acute cognitive symptoms were more likely to predict persisting symptoms at 12 weeks in children. 51 Persistence (i.e., 6+ months) of vestibular symptoms have been associated with dysfunction in the inferior vestibular nerve, possibly providing an underlying pathophysiology in which symptoms may be related to the initial injury. 78 The implication of these results is limited, as the adult subjects reported co-occurring anxiety and depression, making it difficult to determine if their vestibular symptoms were influenced by an aspect of functional neurological pathophysiology as well. Altogether, these studies indicate that the vestibular–ocular subgroup is most prevalent during the acute phase and aids in the initial diagnosis of mTBI. As patients recover, persisting symptoms at the subacute and chronic phases may represent a combination of injured neurocircuitry that is exacerbated by co-occurring symptoms.
Clinically, vestibular–ocular symptoms are multifactorial and related to numerous anatomical pathways, which makes it challenging to identify underlying pathophysiology and apply specific interventions. Multiple objective evaluations of a patient’s symptoms are recommended as each assess different aspects of the vestibular–ocular reflexes (vestibulospinal vs. dynamic vestibular–ocular). 79 Caution is needed when utilizing subjective questionnaires as nonspecific questions related to vision abnormalities, especially in children, have shown not to correlate well with objective data. 44 Adults may be able to better differentiate between physical and vestibular symptoms of dizziness, balance, and coordination, making this a possible age-dependent challenge.44,50 Expansion of the use of current diagnostic testing with technology (e.g., objective eye tracking) is needed to better understand how vestibular–ocular symptoms are related to primary versus secondary pathophysiology.80–82 As this relationship becomes better understood, improvements may be made in potential pharmacologic and nonpharmacologic interventions. Until this becomes better defined, current management remains related to therapy (e.g., vestibular rehabilitation).58,61,83
Headache
Headache and migraine-type symptoms are among the most reported symptoms among children and adults post-mTBI. 38 Migraine exists at a prevalence between 6% and 18% in uninjured men and women, respectively, and increases the risk for headache symptoms post-mTBI. 84 The pathophysiology of each headache subtype is variable, with migraine occurring due to alterations in blood flow, biochemical changes, or cortical spreading depression.84,85 Post-mTBI headache and its associated symptoms have often been considered their own subgroup. 86 However, of the 15 studies reviewed (Table 2), 10 did not identify a separate headache subgroup in their analysis, often including cephalgia and associated symptoms in other subgroups. Seven of the reviewed investigations evaluated for headache symptoms, but attributed them with somatosensory, vestibular/vestibular–ocular, and physical subgroups.39–41,47–50 This unclear categorization of headache makes it difficult to compare symptoms, assess natural evolution, and evaluate effectiveness of treatments. Overall, the prevalence of headache and associated symptoms following mTBI indicates the need for a distinct subgroup.
Development of headache symptoms following mTBI are variable and multifactorial. Pre-injury migraine has been associated with prolonged recovery, but has not been found to affect total return-to-play (RTP) times in adolescents following SRC.60,87,88 Acutely post-mTBI, headache and migraine-like symptoms were the most prevalent symptoms in pediatric patients and the second most prevalent among adults within 3 days of mTBI. 38 Evolution of symptoms during the acute to early subacute period remains less clear, and may be age-dependent. Collegiate athletes reported a decline in headache symptoms at 48 hours postinjury when compared with their immediate symptoms. 45 However, both pediatric and adult patients reporting headache symptoms were more than twice their preinjury baseline at 6 DPI for those exhibiting mild symptoms (defined by reporting headache and at least one other symptom of noise sensitivity, light sensitivity, nausea, or vomiting). 44 Additionally, both pediatric and adult post-traumatic headache have been shown to co-occur with symptoms of nausea, fatigue, drowsiness, dizziness, balance issues, and cognitive complaints with pediatrics often having more migrainous features and adults more tension-type features.41,51 This raises the question if early headache is secondary to the metabolic cascade, energy crisis, ocular strain, fatigue, mood fluctuations, and/or cognitive symptoms experienced. 48 Regardless of etiology, acute headache symptoms have been associated with longer symptom duration.45,88–94 In the subacute and chronic phases, few of the reviewed studies described a headache or migraine-type subgroup beyond 7 DPI. Kissinger-Kox et al. 46 identified a vestibular–ocular migraine subgroup in children that was described from 8 to 31 DPI. However, this subgroup uses the previously described cognitive–migraine–fatigue and somatic symptom scale, complicating interpretation. Yeates et al. describe how pediatric (age 8–18) headache symptoms reported by their parents in the acute period predicted 52.7% of the clinical phenotypes. These phenotypes, subcategorized by age and sex, predicted persisting postconcussive symptoms in 8–70% of children at 4 weeks and 4–49% at 12 weeks, in conjunction with other premorbid factors and symptoms at initial clinical presentation. 51 Throughout all stages of recovery, dysregulated sleep and aspects of cognitive, vestibular, ocular, and somatic symptoms are described within the headache subgroup, which likely impacts the development of symptoms. When compared with one another, only one symptom (neck pain) is specific to the headache subgroup and may contribute to multiple headache phenotypes (i.e., migraine, tension, cervicogenic, occipital neuralgia) (Fig. 1, Table 3). This highlights the bidirectional influence multiple symptoms may have on the development of post-traumatic headache, as well as how the presence of headache may worsen other domains.
Clinically, cephalgia following mTBI is a subjective, patient-specific symptom that is challenging to quantify, evaluate, and manage. Our review indicates that headaches and related symptoms are common in all phases of mTBI recovery and involve complex relationships with other subgroups. Yet, there is a notable discrepancy that exists among the prevalence of post-traumatic headache in the reviewed studies and what is observed clinically. Improved subjective and objective assessments are needed to appropriately characterize this subtype and identify the underlying etiology to effectively manage. Additional consideration may be given to separate subtypes within post-traumatic headache (i.e., migraine, vestibular, tension, cervicogenic, musculoskeletal). 86 Currently, treatment consists of therapies commonly used in primary headache disorders and include behavioral modifications, sleep optimization, tricyclic antidepressants, triptans, local nerve blocks, botulinum injections, topiramate, valproate, and newer CGRP receptor medications.95–97 In the athletic community, an early graded return to activity and exercise may provide additional benefit.60,98–100 Yet, treatment of post-traumatic headache often utilizes provider gestalt, often leading to trial of multiple medications and polypharmacy. Improved characterization of post-traumatic headache in conjunction with the identification of physiological biomarkers may provide the ability to identify opportunities for targeted, more personalized interventions.
Neuropsychiatric
Affective
Affective symptoms comprise a range of domains, including aspects of anxiety, depression, and emotional lability. Current understanding of the neurocircuitry that produces these emotions continues to evolve but likely involves complex interactions within cortical and limbic circuitry.101,102 Symptom assessment requires the use of comprehensive questionnaires (i.e., GAD-7, PHQ-8,) that evaluate the complexity of affective symptoms rather than single symptom questions. Our review of mTBI subtype literature found commonalities among frequently reported affective and behavioral symptoms. Review of these similarities identified that the affective and behavioral subgroups were the second most specific by having limited overlap of symptoms when compared with other subgroups (Fig. 1, Table 3). Inclusion of these specific symptoms in a subgroup provides the ability to characterize the extent in which brain-injured individuals experience dysregulated mood and behavioral symptoms throughout recovery (Fig. 2).
Pre-existing affective conditions within the general population obscure the true incidence of mTBI-induced affective symptoms. The prevalence of individuals that experience intermittent affective symptoms (not qualifying for a disorder) is unclear, but approximately 21% of adults and 14% of adolescents will experience a mood disorder in their lifetime. 103 Similar to other post-mTBI symptoms, it is likely that the presence of affective symptoms or a mood disorder prior to injury may result in worse symptoms following mTBI. In the acute phase, robust evidence has been presented for the presence of an affective subgroup in adult and pediatric populations. 38 Within the first 48 hours of injury, anxious, depressive, and emotional symptoms have been reported to increase in many adult athletes. 45 Moderate anxiety/mood symptoms may remain evident in the early subacute period.41,44 However, in this period, pediatric emotional symptoms have been reported to be less prominent compared with cognitive and somatic symptoms, and found to be interrelated to one another. 40 A delayed onset of adult emotional symptoms has additionally been described, as concussed patients have reported worse symptoms after 14 days of injury compared with earlier postinjury. 43 Within pediatrics, premorbid anxiety has also been identified as a risk factor for persisting postconcussive symptoms up until 12 weeks following injury. 51 The etiology for these delayed symptoms is likely multifactorial, and may be representative of a separate underlying pathophysiology. Translational studies have identified mTBI-induced alterations in limbic system neurocircuitry as a potential mechanism.23,25,102,104–106 Together, these studies provide evidence that mTBI may result in a range of affective symptoms, with the potential for delayed onset, that should be comprehensively evaluated for among children and adults. Future investigation into whether symptom variety and time of presentation are representative of different underlying biological mechanisms as affective subtypes are identified is needed.
Behavioral
Related to the development of affective symptoms following mTBI are alterations in behavior. While this entails a broad scope of interpersonal interactions, sleep-wake disruptions and agitation are often the most described. Given interactions between sleep and other subtypes of mTBI, this specific symptom has been described as an associated condition rather than its own subgroup in the acute setting. 38 Our review of mTBI subgroup studies found all but 2 of the 15 studies described affective and behavioral changes following TBI (Table 2).38–52 Of these, at least three reported sleep as a separate component, provoking inquiry about a separate categorization of these changes.41,42,44 Investigation into possible etiologies for these behavioral changes through the use of preclinical studies have reported alterations among the complex networks involved in social interactions, endocrine disruptions, and a neuroinflammatory response, all of which provide potential mechanisms for these symptoms and may represent possible future endotypes of sleep disorders following mTBI.107,108 Clinically, sleep-wake disorders are prevalent following brain injury, but remain one of the less studied conditions.109–111 In the general population, older adolescents may experience worse sleep hygiene compared with younger teenagers. 41 Following mTBI, studies describe a small, but significant change in sleep within the first 7 DPI in both pediatric and adult populations.41,44 As expected, there is also an association between behavioral, somatic, and emotional factors in these acute and subacute periods.40,46 As recovery progresses, there is limited data, but some report that symptoms may be less prevalent at 3 months in children. 40 Together, this raises the question of whether lingering sleep-related symptoms are the result of persistent dysregulation experienced acutely following injury, related to delayed clinical onset, or influenced by separate mTBI subtypes.
Overall, affective symptoms and behavioral changes following mTBI are less studied and require improved characterization to ensure a patient’s symptoms are identified and addressed. Current understanding suggests that neuropsychiatric symptoms are likely multifactorial and influenced by individual factors such as the presence of pre-injury affective symptoms, professional identity, and individual resilience.112–115 Given these multifactorial interactions, the designation of a neuropsychiatric subgroup is likely a more inclusive description of the affective, behavioral, and sleep disruptions observed in some brain-injured patients. 39 Further improvements to the characterization of these symptoms may be made through the expanded use of additional validated questionnaires that screen for anxiety, depression, fatigue, PTSD, and sleep disturbances. Special consideration of the unique, subjective, and individualized nature of neuropsychiatric symptoms, particularly in the pediatric population, is required, as symptom reports are often not correlated between parents and patients compared with other subtypes.40,49 Clinically, current treatment of neuropsychiatric symptoms includes consideration of psychological interventions, optimization of sleep-related behavior, SSRI/SNRI’s, melatonin, or stimulants.58,60,61,116 However, the effectiveness of these treatments are variable and often difficult to predict. As the neuropsychiatric subgroup becomes better characterized, opportunities for improved counseling, prognostication, and individual interventions may be made possible.
Sex Differences
mTBI subtype characterization allows for improved characterization of a heterogeneous injury. Multiple factors including age, sex, injury mechanism (i.e., sport, blast, MVC, or abuse), and pathophysiology of brain-injured patients likely contribute to variations in symptom presentation. The mTBI literature provides conflicting reports of symptom trajectory among pediatric/adult, male/female and athletic/nonathletic patients. Among these differences, sex is often viewed as a co-factor, with reports of women presenting with an increased severity of symptoms and longer recovery.46,56,117,118 The underlying source of these differences is less clear and may be related to physical, physiological (i.e., hormonal differences), or societal factors.119–121 Sex-dependent, post-injury pathophysiology may also contribute to observed differences, including those in neural network activity, cellular transmission, molecular pathways, and neuroinflammatory cascades. 122 It has also been recently described that the majority of concussion literature and consensus statements have been based on research in male athletes, raising questions as to the relevance of current diagnostic and management techniques to females with brain injury. 123 Together, this likely provides an incomplete characterization of the clinical course for male and female brain injuries.
In the context of mTBI symptoms and subtype characterization, sex differences are also less studied and under-reported. Among the studies reviewed here, sex differences were described among vestibular, somatosensory, headache, and neuropsychiatric symptoms. Females were described to have worse vestibular-ocular reflexes (smooth pursuits, convergence, and visual motion sensitivity tests) up to at least 1 week following injury and worse with co-occurring migraines.44,124 Somatosensory symptoms also differed, with male athletes reporting increased sensitivity to light, whereas females reported being more sensitive to noise. 124 Finally, in the domain of neuropsychiatric symptoms, women experienced worse sleep symptoms at 1 week following injury and worse anxiety symptoms 2–3 weeks post-injury.43,44 When evaluated with the timeline for typical mTBI recovery, adolescent female symptoms were reported to worsen more often within 1 week postinjury, while males trended toward improvement. 87 When assessing health care utilization in concussed patients, one study reported that women have a higher proportion of visits at chronic timepoints following injury compared with men, who access care for preseason baselines or acute injury visits. 125 Despite these reports, robust studies have reported that these differences may not be present at all ages or timepoints, or impact overall recovery duration.126–128
Ultimately, it remains unclear if mTBI subtypes differ based on sex. The possible pathophysiology behind sex differences is likely multifactorial and currently in the initial stages of being characterized at the clinical and preclinical levels. Consideration of underlying biological differences including variations in hormones, musculature, increased prevalence of certain pre-injury conditions (i.e., migraine, anxiety, depression), and societal expectations are needed.129,130 It is possible that a combination of certain biological sex differences within a specific symptom cluster may help delineate additional endotypes. Future studies will need to analyze data separately for males and females, as well as consider transgender and nonbinary individuals who may use exogenous hormones. 129 Integrating objective biomarkers in conjunction with sex-specific differences will be essential to accurately characterize mTBI subtypes and ensure equitable care across individuals.
Improvements to Clinical Subgroups of mTBI
The variety of mTBI-induced symptoms that each patient experiences result in a heterogeneous patient population. Symptoms are the result of multiple pathophysiologic processes and are likely influenced by numerous individual factors including preinjury history, injury mechanism, sex, age, family, sociodemographic, and other unidentified variables. Care for mTBI recovery utilizes an individualized approach from a multidisciplinary team to provide optimal recovery. Individual recovery trajectories are also highly heterogeneous. Although some individuals recover within 1-month, patients injured through nonsporting mechanism in particular may experience a protracted course, sometimes reporting symptoms months to years following the initial injury.60,131–138 Current guidelines recommend prioritizing the most disabling symptoms in order to improve quality of life and attempt to improve interrelated symptoms.139,140 However, the heterogeneity of injury has likely contributed to the limited number of pharmacologic interventions. 116 Thus, identifying mechanisms that contribute to commonly experienced symptoms can improve prognostication and facilitate personalized interventions.
Multiple attempts to better define the heterogenicity of mTBI have been made. Most of these utilize symptom-based typology to define commonly experienced clinical trajectories (i.e., cognitive, somatosensory, vestibular–ocular, headache, and neuropsychiatric) that may be identified at most timepoints following mTBI. The clinical utility of symptom-based subgroups is limited as critical variations exist amongst the definitions of each group. Additionally, it is challenging to know if similar symptoms developed at different timepoints represent the same pathophysiology thus representing the same or separate mTBI subtypes. Improved understanding of mTBI heterogenicity would benefit from more clearly defined subtypes. Incorporating objective evaluations indicative of underlying pathophysiology may offer enhanced understanding of the mechanisms contributing to mTBI symptoms and evolution. Inclusion of advanced mTBI evaluations (i.e., Vestibular Ocular Motor Screening, BESS, KD, etc.), and expanded neuropsychological tests have been proposed to improve subjectivity and ambiguity within mTBI subtyping. As an initial step, symptom-based subgroup studies have begun to correlate their groups to advanced mTBI evaluation and expanded neuropsychological tests, yet this needs further validation before any one test is related to a specific symptom group.39,45,46 Beyond these assessments, serum biomarkers, advanced neuroimaging, and genetics have been studied and may be relevant to mTBI subtyping. Multiple biomarkers (i.e., Glial Fibrillary Acid Protein), Neurofilament Light polypeptide (NF-L), Tau, S100 calcium-binding protein B (s100-B), and Ubiquitin C-terminal hydrolase L1 (UCH-L1)) have been identified to help diagnosis and project recovery trajectories of mTBI.75,141 Brett et al. in conjunction with the CARE consortium have provided an analysis of how these biomarkers may apply to certain symptom-based mTBI subtypes (cognitive, fatigue, somatosensory, vestibular-ocular, headache, and emotional). 45 Further, advanced neuroimaging, including aspects of MRI, fMRI, DTI, magnetic resonance spectroscopy, and cerebral blood flow, have also been studied, but are likely limited to research populations at this time.142,143 Evaluation of genetic analysis has also been proposed, with initial studies investigating how single gene polymorphisms may relate to specific mTBI outcomes. So far, single gene polymorphisms have identified associations between APOE and injury severity as well as additional aspects of how clinical outcomes are related to differences in calcium channel mutations (CACNA1A), adenosine receptors (A1AR), dopamine receptors (DRD2, COMT, ANKK1), and other biomolecules (BDNF, Tau, NEFH, PARP1).144–149 Together, inclusion of expanded neuropsychological testing, neuroimaging, and genetic analysis may allow for the creation of risk profiles for a subset of the mTBI population but are unlikely to predict a specific clinical trajectory for any subtype alone. Given this, a shift to endotyping of mTBI as a means of subtype classification has been proposed to incorporate multivariable mTBI evaluations into clinical profiles. So far, this approach has led to the proposal of autonomic, headache, neuroinflammatory, neurovascular, and post-traumatic epilepsy endotypes.150–157 Initially described within post-traumatic epilepsy, Diaz-Arrastia et al. described how neurophysiologic techniques (EEG) and neuroimaging (MRI) may be used to describe select individuals who develop seizures following injury. 152 Additional applications have been applied to the neurovascular consequences of TBI, exploring how molecular biomarkers, imaging abnormalities, and genetic risk factors influence TBI outcomes.151,157 Biomarkers have also begun to be studied in the context of post-traumatic headache; however, improved clarity is needed before this is able to be utilized clinically. 86 Finally, autonomic dysfunction following mTBI has also recently been proposed, given observation of nonspecific symptoms of headache, fatigue, dizziness, nausea, balance issues, cognitive impairments, emotional lability, and sleep disruptions in association with vital sign variability, and pupil changes.153–156 It is also possible that incorporating objective assessments and biomarkers may refine existing symptom-based typology, providing deeper insights into commonly experienced clinical presentations. It is also possible that additional endotypes exist that align with those identified in symptom-based typology. As mTBI endotypes become better understood, future discussions in mTBI subclassification require consideration of evidence-based consensus of the variables included in each subgroup in order to provide comparisons between various research cohorts and improved clinical applicability.
Practical measures to advance mTBI subgroup classification require clear definitions of each group at each timepoint of recovery. Initial consensus has been described in the acute (0–3 DPI) period using a meta-analysis of predominately SRC. 38 However, the symptoms and advanced mTBI testing included in these subgroups differ from those included in the currently described mTBI subgroup literature in the subacute and chronic phases of recovery. It is also not clear if certain brain injury-induced signs and symptoms are representative of the same subgroup over time or if different symptoms at different timepoints are indicative of separate pathophysiology. Expanded evaluations utilizing objective assessments, biomarkers, neuroimaging, and genetic analysis would likely improve mTBI subclassification, which is supported by the new CBI-M TBI classification system proposed by a recent National Institute of Neurological Disorders and Stroke working group. 158 Future studies identifying alterations to physiologic parameters (heart rate, blood pressure), neurophysiological studies (i.e., EEG, MEG), advanced mTBI testing, structural and functional brain imaging, and changes in serum molecules, and genetic testing are needed to identify a composite analysis that will eventually aid in mTBI subclassification. Additional consideration will also need to be given to injury mechanism (sport vs. assault, blast, MVC, fall, etc.) and other sociodemographic factors such as age, sex, and race/ethnicity are needed to adequately characterize the symptom profile of all patients who experience mTBI. As mTBI studies begin to include these concepts, it remains critical to establish systematic criteria that clearly defines mTBI subtypes at each timepoint of recovery to be able to compare clinical trajectories and response to potential interventions.
Ultimately, it is likely that the most specific subclassification of mTBI will be completed through integration of objective and subjective postinjury data. As mTBI subtypes move away from isolated symptom-based topology, efforts that focus on combining the clinical presentation with objective neuropsychological testing, biomarkers, neuroimaging, and genetics will provide the most accurate categorization of commonly observed trajectories following mTBI. 159 As this is accomplished, clinical application of mTBI subtypes provides the opportunity to create a mTBI classification framework to improve clinical prognostication, and allow earlier interventions to assist in the recovery of brain-injured patients. In doing so, advancements toward individualized symptom management, recovery, and improved care for our mTBI population may be made possible.
Transparency, Rigor, and Reproducibility Statement
This review’s protocol was not registered, as this review was not conducted as part of a formal systematic review. Studies were included if they characterized two or more subtypes based on clinical profiles at any time point (either at baseline or following mTBI) and published prior to the first quarter of 2022. Studies were excluded from analysis if they focused solely on a singular subtype/symptom or if the study population was not specific to mTBI. Additional studies that did not subtype patients based on clinical phenotypes (i.e., based on mechanism or severity) or those that were based on commentaries, editorials, case reports/series or reviews were excluded. Each study also needed to label or refer to each of their subgroups based on a predominant clinical symptom/phenotype.
Authors’ Contributions
J.A.B.: Conceptualization, methodology, investigation, and writing—original. N.D.: Writing—review and editing. S.M.M.: Writing—review and editing. C.L.M.: Conceptualization and writing—review and editing. C.C.G.: Conceptualization and writing—review and editing. C.M.C.: Conceptualization and writing—review and editing. M.S.: Conceptualization, methodology, writing—review and editing, and supervision.
Footnotes
Acknowledgments
The authors would like to thank the Texas Institute for Brain Injury Repair, Peter O’Donnel Jr. Brain Institute, and ConTex organization for their continued support.
Author Disclosure Statement
The authors declare that there is no conflict of interest with respect to the research, authorship, and/or publication of this article.
Funding Information
This work was partially supported by the