
Abstract
With growing concern about the long-term effects of head injuries in contact sports, understanding differences in head impact exposure (HIE) across age groups is critical. Youth athletes may face heightened risks due to developmental vulnerability, yet the relationship between level of play and HIE remains unclear. This systematic review compares HIE characteristics between youth (≤14 years) and collegiate football players using accelerometer-based sensors. PubMed, Embase, and Scopus were searched (2015–2025) for studies quantifying HIE with impacts defined as acceleration events exceeding a 10–15 g threshold. Variables included cohort age, study period, sensor type, impact frequency during practice and competition, and median and 90th–95th percentile linear and rotational acceleration. Twenty-nine studies met the inclusion criteria, representing 1742 youth athletes (aged 6–14) and 3850 collegiate athletes (aged 17–23). Collegiate players sustained more cumulative seasonal impacts than youth in practice (472.1 vs. 113.0) and overall (449.0 vs. 228.0). However, impacts per individual game (youth: 10.0; collegiate: 9.8), median linear accelerations (youth: 18.6 g; college: 20.7 g), and upper-tail linear accelerations (youth 95th percentile: 46.4 g; collegiate 90th–95th percentile: 47.7 g) were similar between groups. By contrast, youth athletes exhibited higher seasonal median (1144.9 vs. 964.0 rad/s2) and upper-tail rotational accelerations (youth 95th percentile: 2929.7; collegiate 90th percentile: 2072.2 rad/s2). These findings indicate that while collegiate athletes sustain greater cumulative exposure, youth may sustain impacts of comparable or greater magnitude. Accelerometer-based data provide critical insights into age-related differences in HIE, with implications for understanding concussion pathophysiology and informing safety strategies.
Keywords
Introduction
Head injuries have become a growing concern in sports, particularly in high-contact activities where collisions frequently occur.1,2 American tackle football stands out due to its widespread participation and elevated risk for traumatic brain injury (TBI). In a national surveillance study of U.S. high school athletic teams, football accounted for over 40% of all reported concussions, more than all other sports evaluated, including soccer and wrestling. 3 Additionally, football is a leading contributor to sports- and recreation-related TBIs treated in emergency departments among children and adolescents. 4 While some contact sports injuries result in clinically diagnosed concussions, many head impacts go unrecognized or unreported, especially those that do not produce overt symptoms in the acute setting.5,6 Traditionally, concussion diagnoses have relied on symptom reporting and documentation by athletic trainers, limiting the ability to fully capture the scope of brain trauma. 7 Even in the absence of concussion, repeated non-concussive impacts have been associated with white-matter abnormalities, disrupted neural connectivity, and impaired cognition.8–11 These findings have prompted increased attention to the cumulative effects of both concussive and subconcussive trauma over time.12,13
Specifically, repetitive head impacts (RHI) refer to the cumulative burden of head contact events on a longitudinal basis, regardless of whether individual impacts result in acute symptoms or a diagnosis of concussion.14,15 Whereas TBI is defined by the occurrence of a discrete event, RHI represents a dose–response construct, encompassing both the frequency and magnitude of impact exposure over time.16,17 This distinction is pertinent to contact sports. Athletes may sustain numerous subconcussive blows throughout a season; however, current surveillance systems may underrepresent the full scope of exposure, often only capturing diagnosed concussions.18,19 In addition to characteristics of individual impacts, the cumulative amount of head injury exposure has emerged as a critical determinant of long-term risk for neurodegeneration.9,12,20
In fact, RHI are now recognized as a primary risk factor for chronic traumatic encephalopathy (CTE), a progressive neurodegenerative disease defined by perivascular accumulation of hyperphosphorylated tau in the depths of cortical sulci. At present, CTE remains a postmortem diagnosis.14,21,22 Large cohort studies of former American football players show that cumulative seasons of play and career length correlate with increased likelihood of developing CTE, underscoring that increased exposure amplifies risk.15,23,24 Importantly, this relationship holds even in the absence of a clinically diagnosed concussion, highlighting that it is the repetitive exposure itself, rather than isolated injuries, that may drive chronic neurodegeneration and disease pathogenesis.14,16 Recognition of RHI as a pertinent risk factor underscores the essential nature of systematic tracking of head impact exposure (HIE), specifically via devices that offer the most direct means of quantifying this cumulative burden.
To better assess HIE, researchers have implemented accelerometer-based devices, embedded in helmets or mouthguards. This offers objective biomechanical data on cumulative head injury burden via measuring frequency of impacts, linear and rotational peak acceleration magnitude, and direction of impacts sustained by each athlete.25–27 Consequently, accelerometers offer a more comprehensive evaluation of the full spectrum of head impacts, including both minor and concussive hits, endured in sports like football. This is particularly valuable in younger athletes, who may underreport symptoms or lack access to consistent medical evaluation.
The distinction between concussive and subconcussive injury is especially relevant in pediatric populations. Children have thinner cranial bones, less developed white matter, and ongoing synaptic remodeling, all of which may heighten vulnerability to biomechanical stress. Underdeveloped neck musculature and slower reflexes can exacerbate the effects of acceleration forces during impact.28–30 Moreover, the developing brain may be more susceptible to disruption, with some studies suggesting longer recovery periods and greater risk of lasting neurocognitive effects after head injury in youth athletes compared with adult counterparts.31–34 Neuroimaging studies further support this concern. In youth football players, diffusion tensor imaging and resting-state fMRI reveal white-matter microstructural changes and alterations in brain network efficiency after a single season of play, even in the absence of concussion.35–37 These findings underscore the pertinence of measuring cumulative HIE, not just symptomatic injury, when evaluating risk for chronic neurodegeneration in vulnerable populations like youth athletes.
While the literature on HIE has historically centered more on high school and collegiate athletes, recent years have seen a rise in studies investigating younger populations. Nevertheless, there is a profound paucity of studies that have conducted direct comparisons between youth and college-level players. Variability in physical development, play intensity, rules, and helmet fit might contribute to age-related differences in HIE, but these differences remain poorly characterized. Understanding how HIE evolves across developmental stages is critical to designing age-appropriate safety interventions.
This systematic review aims to address these gaps by synthesizing accelerometer studies of HIE in American football players across two levels of play: youth under 14 years and college. Given the substantial increase in accelerometer-based research involving youth athletes in recent years, we focused on literature from 2015 to 2025 as an updated synthesis of the contemporary HIE literature. This start date was prespecified to: (a) prioritize current sensor platforms and reporting conventions, (b) reflect more recent policy and practice-structure changes in youth football, and (c) maintain a feasible scope for a focused update. While foundational work on age-related HIE was published prior to 2015, these studies were outside the predefined time window for this update. By comparing impact frequency and magnitude of linear and rotational acceleration, this review seeks to clarify developmental risk profiles and support the development of age-specific guidelines for preventive measures against head injuries.
Methods
Search and screening strategy
A literature search was performed using the PubMed, Embase, and Scopus databases to identify relevant studies published between 2015 and 2025. The 2015 start date was selected to provide a focused synthesis of the contemporary accelerometer-based HIE literature. The following terms were applied using Boolean operators: (youth football OR collegiate football) AND (concussion OR head impact) AND (incidence OR exposure). Reference lists of included articles and forward citations were hand-searched to identify additional studies. Records were exported to a reference manager, de-duplicated using identifier and title/author matching, and screened in two stages. Two independent reviewers screened titles/abstracts to assess initial eligibility; disagreements were resolved by consensus, with adjudication by a third reviewer when necessary. Studies were selected for inclusion if they reported primary data on head impact frequency and/or acceleration magnitude in either youth (defined strictly as less than 14 years of age), collegiate (17–23 years of age), or both cohorts.
Eligible articles were required to be peer-reviewed, published in English, and use accelerometer-based methods to quantify head impacts. Exclusion criteria included studies that did not report accelerometer-derived biomechanical outcomes (i.e., impact counts or acceleration magnitudes), including those limited to concussion incidence, symptom reporting, or clinical surveillance. Additional exclusion criteria included studies evaluating other sports (e.g., flag football or Australian rules football), publications written in a language other than English, case reports, reviews, editorials, posters, conference abstracts, or studies published prior to 2015. Articles solely focused on the high school level were excluded. When multiple publications from the same dataset were identified, only the most complete or updated version was retained. Full-text review was conducted on all remaining articles to confirm adherence to the inclusion criteria. The review protocol was registered prospectively in the PROSPERO database (ID: CRD420250632766). Institutional Review Board approval was not required for this study.
Data extraction and outcomes of interest
Data extraction included the following demographic and study variables: participant count, age, sex, body mass, type of sensor, threshold for measured acceleration events, frequency of impacts per session or per season, median peak linear acceleration, 95th percentile peak linear acceleration, median peak rotational acceleration, 95th percentile peak rotational acceleration, and proportion of high-magnitude impacts. Extraction used a prespecified form piloted on a subset of studies. One reviewer extracted, while a second verified all fields. Where applicable, we also noted session classification (practice or competition) and sensor mount (helmet, mouthguard, skin patch) to aid contextual interpretation. In cases of disagreement between reviewers, a third reviewer was available to ensure consensus.
Because outcome definitions varied across studies (e.g., session type, percentile levels), we did not conduct a formal meta-analysis. Instead, sample-size–weighted averages were applied to describe central tendencies for impact frequency and peak linear and rotational accelerations at each level of play and setting (practice, competition, and overall season). We used sample-size weighting to summarize grouped outcomes because the included studies reported metrics from cohorts with substantially different sample sizes. This yields a descriptive estimate that reflects the average value across athletes represented in the included cohorts, rather than giving each study equal influence regardless of cohort size. This weighting approach does not imply that larger studies are inherently higher quality, but rather it is used to account for differences in cohort representation. Because head-impact kinematics tend to be right-skewed, such that many impacts are low magnitude with a smaller number of high-magnitude impacts,38,39 we summarized acceleration outcomes using medians (typical impact magnitude) and 95th percentiles (upper-tail exposure) when reported. Accordingly, “weighted average median” acceleration values represent sample-size–weighted summaries of study-reported medians across cohorts, rather than pooled impact-level estimates.
When studies reported 90th rather than 95th percentile values, we retained these data and flagged this decision as a potential source of downward bias for upper-tail estimates in the relevant age group. Accordingly, any pooled upper-tail estimates that include both 90th and 95th percentile inputs are labeled as “90th–95th percentile.” To minimize heterogeneity related to event-triggering settings, we extracted the linear acceleration trigger threshold for each cohort when reported, with most cohorts using thresholds in the 10–15 g range. Cohorts that capture only higher-magnitude events were not combined with 10–15 g cohorts when summarizing impact frequency or median and 95th percentile acceleration magnitudes. For cohorts in which the trigger threshold is not explicitly reported, studies were retained when they clearly describe an impact-detection approach and report standard head impact summary metrics, allowing inclusion for descriptive synthesis while acknowledging threshold-related uncertainty. Because impact-level data were not available across studies, we did not attempt to rescale impact frequency or acceleration percentiles to a single common threshold within the 10–15 g range. As such, pooled estimates reflect cohorts measured under commonly used 10–15 g settings and should be interpreted as descripted summaries rather than threshold-standardized values.
Sensor type (i.e., helmet-embedded telemetry, instrumented mouthguard, or skin patch) was recorded for each cohort, but all device classes were analyzed collectively in our report. Season-aggregated and session-specific data were reported separately. If one study followed the same team across multiple seasons, each season was treated as an independent cohort, with data extracted separately for each year and acknowledging possible participant carryover. When studies provided both overall and subgroup data, such as linemen versus skill players, these were included as distinct entries if they met the inclusion criteria. For impact frequency, we extracted the study-reported measure of central tendency, prioritizing mean values when reported, while using medians when means were not available. We consequently computed sample-size–weighted averages of these cohort-level summaries. No transformations were performed to convert between medians and means. Therefore, impact frequency estimates represent weighted summaries of reported central tendency measures.
If percentile distributions were presented in ranges, the closest available value to the 95th percentile was extracted. Finally, when studies included multiple comparator groups, we extracted only data relevant to youth or collegiate football. For example, if youth and high school athletes were included in the same study, only the youth subset was retained. Likewise, if football exposure was reported alongside other contact sports, only the American football data were extracted for analysis.
Risk of bias assessment
Methodological quality and risk of bias for each included study were evaluated using the Methodological Index for Non-Randomized Studies (MINORS) tool. This scoring system assigns values of 0 (not reported), 1 (reported but insufficient), or 2 (reported and sufficient) across key methodological domains. Two reviewers rated each item independently with consensus resolution. For comparative studies, the highest possible score is 24. Scores were interpreted as follows: <16 indicating high risk of bias, 16–20 indicating moderate risk, and 21–24 indicating low risk. For noncomparative studies, which have a maximum score of 16, thresholds were defined as <8 for high risk, 8–12 for moderate risk, and 13–16 for low risk of bias. Risk-of-bias considerations informed narrative synthesis and sensitivity notes but were not used as quantitative weights.
Results
Search results, study characteristics, and demographic data
Initial search results identified 1219 total articles. After removing duplicates, 842 unique articles remained. Of these, 29 were identified for inclusion in the study. The large reduction from 842 screened records reflects the application of our predetermined eligibility criteria, with many studies excluded because they lacked accelerometer-derived biomechanical data. This article selection process is summarized in Figure 1.

PRISMA flow diagram illustrating study selection for the systematic review of youth and collegiate head impact exposure (HIE). PRISMA, Preferred Reporting Items for Systematic Reviews and Meta-analyses.
The 29 studies included in this review all had a prospective study design, and all were published between 2015 and 2025. Twenty-six were comparative cohort studies with a Level of Evidence of two, and three were observational cohort studies with a Level of Evidence of three. Additional information regarding the included studies is explained in Table 1. Across 29 studies that reported sample size, a total of 5592 participants were identified, consisting of 1742 youth and 3850 collegiate athletes, all of whom were male. Nineteen studies focused on youth cohorts, eight studies centered on college-level athletes, and two studies had data for both age groups. 18 out of 29 studies reported the mean age, yielding a pooled total mean age of 11.9 years for 14 youth-level cohort studies (715 athletes represented), and 19.1 years for 4 college-level cohort studies (1223 athletes represented). The overall age range for all youth and collegiate studies was 6–14 and 17–23 years of age, respectively. Fourteen studies reported body mass for youth participants, resulting in a pooled total mean body mass of 50.83 kg (545 athletes represented). Body mass was reported in one collegiate study, in which 502 participants had a mean body mass of 105 kg. 40
Study Characteristics and Methodological Assessment
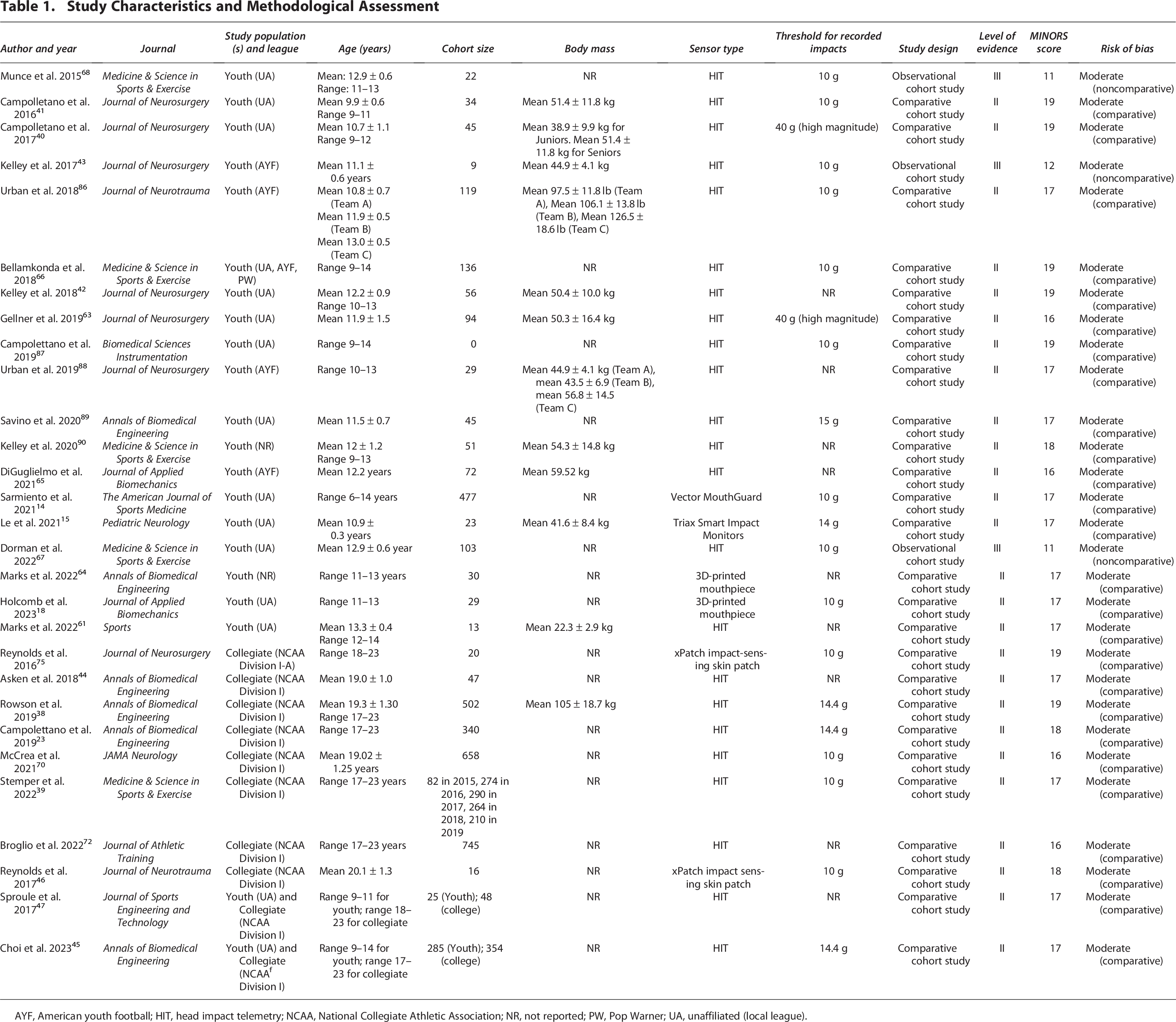
AYF, American youth football; HIT, head impact telemetry; NCAA, National Collegiate Athletic Association; NR, not reported; PW, Pop Warner; UA, unaffiliated (local league).
For acceleration sensors, 23 studies implemented a head impact telemetry (HIT) system installed in helmets, 1 study used a Vector Mouthguard, 2 studies used 3D-printed mouthpieces, 2 studies used xPatch impact-sensing skin patches placed over the mastoid process, and 2 studies implemented Smart Impact Monitors placed on headbands or skullcaps. Thirteen studies set a minimum threshold of 10 g in magnitude for all measured acceleration events. One study implemented 14 g, three studies used 14.4 g, and one study utilized 15 g for their thresholds. Two studies assessed higher-magnitude impacts and consequently focused on impacts that exceeded 40 g. These studies were not grouped with those reporting 10–15 g thresholds but were instead retained for descriptive comparisons between age groups. Eight studies did not report their threshold for recorded impacts. These cohorts were included in pooled summaries according to the threshold-handling criteria described in the Methods section.
The units for measuring impact frequency varied across the included studies. From 25 studies quantifying frequency in units of contextual time, 15 studies reported the average amount of impacts per athlete across a season. Five studies included measurements of impacts per athlete per practice session, in addition to eight studies recording impacts per athlete per game. Five studies quantified impact frequency in units of discrete time, such as impacts per athlete per hour.
Outcome measures related to linear and rotational acceleration were reported in 19 and 18 studies, respectively. Additionally, nine studies included data on exposure to high-magnitude impacts such as those that exceed 40 g. Eighteen studies reported HIE during in-season games, 18 reported HIE during practice sessions, and 17 reported metrics across both session types combined. One study measured 90th percentile values, rather than 95th percentile, for linear and rotational acceleration in collegiate athletes. 41 For our comparison, we included these values with data pertaining to the 95th percentile.
Risk of bias assessment
The 26 comparative studies had an average MINORS score of 17.5 (standard deviation 1.07, range 16–19), while the 3 noncomparative studies had an average MINORS score of 11.33 (standard deviation 0.58, range 11–12). All 29 studies had a moderate risk of bias according to their respective guidelines.
Impact frequency
Thirteen total studies reported the frequency of impacts across a whole season. Of these, four articles, including two youth (N = 79) and two collegiate cohorts (N = 356), measured the occurrence of impacts throughout all practice sessions within a season. When accounting for sample sizes per study, there was a weighted average of 121.8 total impacts throughout all practices for youth, and 472.1 total practice impacts for college players. Four studies, encompassing three youth (N = 108) and one collegiate (N = 20) contained data on impact frequency throughout all games within a season. Youth players had a weighted average of 143.2 total impacts across seasonal games. The one college cohort reported an average of 24.4 game-related impacts per season. Eleven studies measured the number of total impacts sustained throughout a whole season, regardless of session type. This consisted of 10 youth (N = 485) and 4 collegiate cohorts (N = 2138). Youth athletes had a weighted average of 228.9 impacts per season, and college-level athletes had a weighted average of 449.0 impacts per season.
Six studies representing eight youth cohorts (N = 1074) and one collegiate cohort (N = 354) contained data on impact exposure during individual practice sessions. Youth athletes endured a weighted average of 6.80 impacts per practice session, while the one collegiate cohort had an average of 8.20 impacts per session. For competition, 11 youth (N = 1198) and 3 collegiate (N = 1115) cohorts from 11 total studies had a weighted average of 10.0 impacts and 9.8 impacts per game, respectively. Furthermore, 10 youth cohorts (N = 167), 6 of which consisted of 103 participants tracked over 6 seasons, from 3 studies had a weighted average of 6.3 impacts per session, whether competition or practice. No included study contained equivalent data for collegiate players.
The weighted averages for impact frequency per season and per session in youth and college-level cohorts, including in the practice, competition, and combined settings, are summarized in Table 2. These values for youth, collegiate, and combined age cohorts, across overall season and individual session, are also represented in Figures 2 and 3, respectively.

Bar chart showing the weighted mean number of head impacts sustained across a full season, stratified by cohort (youth, collegiate) and session type (practice, game, overall). Standard error bars represent the standard error of the weighted mean, calculated from aggregated study-level data. Sample sizes per cohort and activity are indicated in parentheses.

Weighted mean frequency of head impacts per session, grouped by cohort (youth, collegiate) and activity type (practice, game, overall). Standard error bars represent the standard error of the weighted mean, and sample sizes per cohort are reported in parentheses. *Indicates a cohort for which one study group is represented.
Weighted Averages for Impact Frequency in Youth and Collegiate Cohorts

One cohort represented.
Five studies reported frequency of impacts in units of discrete time. Three youth cohorts (79 participants) from two studies reported an average range of 6.2–21.6 impacts per hour during games. For four youth cohorts (N = 79) from two studies, the average frequency in practice ranged from 2.5 to 23.1 impacts per hour.42,43 In two youth cohorts (N = 65), average occurrence in practice ranged from 0.1 to 0.5 impacts per player per minute, depending on the type of drill.44,45 One collegiate cohort (N = 47) found time-based frequency to depend on playing position, with linemen and non-linemen sustaining 0.12 and 0.06 hits per player per minute, respectively. 46
Linear acceleration
A total of eight studies reported linear acceleration data during games, encompassing six youth cohorts (N = 956) and three college cohorts (N = 390). Among youth cohorts, the median peak linear acceleration during games ranged from 18.3 to 32.5 g, with 95th percentile values ranging from 45.6 to 63.0 g. When accounting for pooled sample sizes, the weighted average for median and 95th percentile values for youth players was 19.1 g and 48.8 g, respectively. For college-level cohorts, the median peak linear acceleration during games ranged from 28.2 to 29.5 g, while one study reported 61.9 g as the 95th percentile linear acceleration in games. 47 The weighted average median linear acceleration for collegiate-level games was 28.8 g.
Ten studies reported linear acceleration magnitudes during practice sessions, consisting of seven youth cohorts (N = 971) and eight collegiate cohorts (N = 1537). Five out of eight college-level cohorts were taken from different seasons within the same study, with unspecified overlap in players between seasons. 41 At the youth level, median linear acceleration during practices ranged from 14.5 to 25.0 g, while 95th percentile magnitudes ranged from 32.7 to 56.4 g. The weighted average for median and 95th percentile linear acceleration for youth during practice was 18.1 g and 47.3 g, respectively. At the college level, median linear acceleration ranged from 20.0 to 25.7 g. The 90th–95th percentile values for collegiate cohorts ranged from 44.0 to 62.3 g. The weighted average for median and 90th–95th percentile linear acceleration for college was 20.5 g and 49.6 g, respectively.
For linear acceleration values recorded across a season including both practice and competition, 12 studies were included, yielding 19 youth (N = 987) and 6 collegiate (N = 1168) cohorts. For youth athletes during combined session types, median linear acceleration ranged from 9.5 to 25.5 g, and 95th percentile linear acceleration ranged from 27.0 to 57.3 g. The weighted youth average for median and 95th percentile was 18.5 g and 46.4 g, respectively. For college, median linear acceleration ranged from 20.0 to 21.0 g, and 90th–95th percentile ranged from 45.0 to 60.1 g. The weighted average for collegiate athletes was 20.7 g and 47.7 g for median and 90th–95th percentile linear acceleration, respectively.
The weighted average values for median and upper-tail linear acceleration magnitude in youth and college-level cohorts, across all session types, are summarized in Table 3. These averages are also represented in Figure 4.
Weighted Averages for Median and Upper-Tail Percentile Linear Acceleration in Youth and Collegiate Cohorts

One cohort represented.
95th percentile only.

Bar chart depicting the weighted mean peak linear acceleration (in gram) experienced during head impacts, stratified by cohort (youth and collegiate) and percentile tier (50th and 90th–95th across practice, competition, and combined settings). Percentile tiers were derived from study data. Error bars denote the standard error of the weighted mean, and sample sizes are reported in parentheses. *Indicates a cohort for which one study group is represented.
Rotational acceleration
From six studies that measured rotational acceleration during games, five youth (N = 479) and two collegiate (N = 370) cohorts are represented. For youth players, the median and 95th percentile rotational acceleration ranged from 889.2 to 2509.0 rad/s2, and from 2217.0 to 4782.3 rad/s2, respectively. The weighted average for median rotational acceleration in youth was 1502.2 rad/s2, and the weighted average for the 95th percentile was 2685.3 rad/s2. For college athletes, the median rotational acceleration in the competition setting was only reported by one study, which was determined to be 5297.6 rad/s2. 48 The 95th percentile rotational acceleration in college-level games was only reported by Choi et al., which was calculated to be 4422.0 rad/s2. 47
For rotational acceleration in the practice setting, nine studies were included and consisted of six youth cohorts (N = 550) and seven collegiate cohorts (N = 1521). The median and 95th percentile values for youth athletes ranged from 904.4 to 1628.6 rad/s2, and from 2081.0 to 3709.6 rad/s2, respectively. The weighted average for the median rotational acceleration was 1173.9 rad/s2, and the weighted average for the 95th percentile was 2475.0 rad/s2. At the college level, median and 90th–95th percentile ranged from 950.0 to 1563.2 rad/s2, and from 1967.0 to 4052.0 rad/s2. The weighted average for median and 90th–95th percentile rotational acceleration in college practice was 989.1 rad/s2 and 2535.6 rad/s2, respectively.
For combined sessions during the overall season, 16 youth cohorts (N = 548) and 5 collegiate cohorts (N = 1120) are represented across 10 studies. The five college-level cohorts were extracted from the same study that assessed HIE over five seasons, which strictly reported 90th percentile values. 41 At the youth level, median and 95th percentile rotational acceleration ranged from 666.4 to 1691.8 rad/s2, and from 1863.3 to 4107.0 rad/s2, respectively. The weighted median and 95th percentile were 1144.9 and 2929.7 rad/s2, respectively. The median rotational acceleration for college athletes ranged from 922.0 to 974.0 rad/s2, while the 90th percentile ranged from 1968.0 to 2110.0 rad/s2. The weighted average for median and 90th percentile rotational acceleration in the collegiate cohorts was 964.0 rad/s2 and 2072.2 rad/s2, respectively.
The weighted average values for median and 90th–95th percentile rotational acceleration magnitude in youth and college-level cohorts, across all session types, are summarized in Table 4. These measures are represented in Figure 5.
Weighted Averages for Median and Upper-Tail Percentile Rotational Acceleration in Youth and Collegiate Cohorts
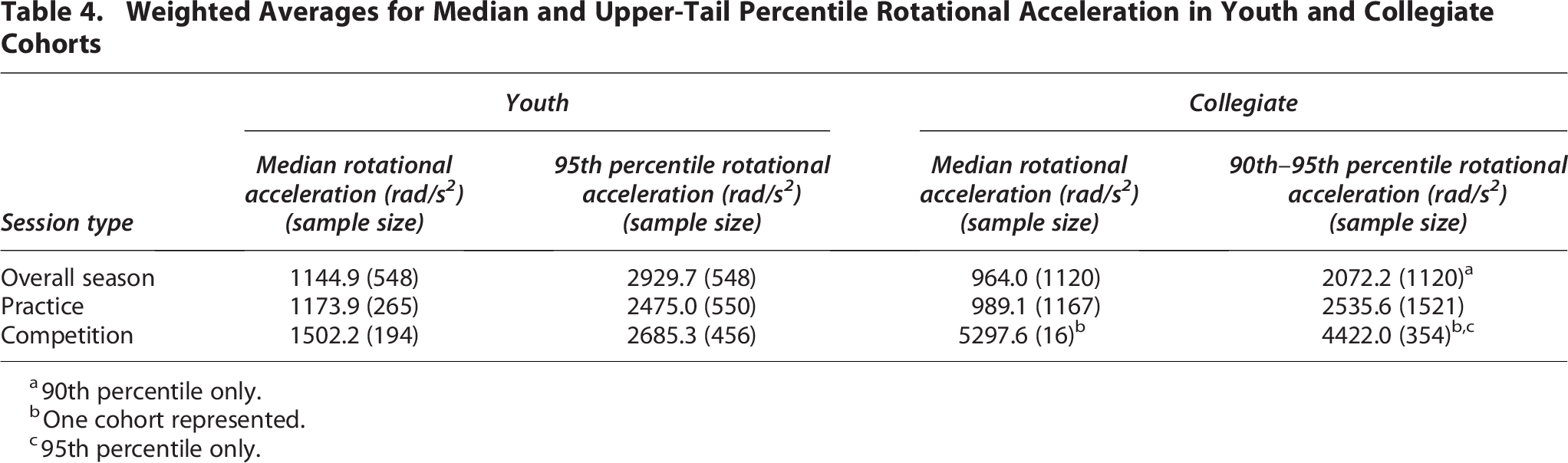
90th percentile only.
One cohort represented.
95th percentile only.

Weighted mean peak rotational acceleration (in rad/s²) across head impacts, stratified by cohort (youth and collegiate) and percentile tier (50th and 90th–95th percentile across practice, games, and combined settings). The 50th and 90th–95th percentiles reflect median and higher-impact thresholds, respectively. Standard error bars indicate variability across studies contributing to each cohort. Sample sizes are reported for each cohort. *Indicates a cohort for which one study group is represented.
Discussion
Impact frequency
This review aimed to assess age-related trends in HIE that may help inform safety precautions and guidelines in tackle football, particularly for pediatric populations more vulnerable to chronic effects from head trauma. Our results demonstrate that differences in head impact frequency between youth and collegiate athletes are shaped by both session type and unit of analysis. At the seasonal level, collegiate athletes sustained substantially more impacts than youth athletes, with 472.1 versus 113.0 during practices, and 449.04 versus 228.04 across all sessions. However, per-session data revealed more complexity. Collegiate players averaged more impacts per practice session (8.2 vs. 6.7), but youth players exhibited a comparable frequency of impacts per game (10.0 vs. 9.8). The age-based similarity in exposure during a single game is robust based on pooled sample sizes (1198 youth participants and 1115 collegiate participants), suggesting this is not merely a sampling artifact. Of note, impact frequency was summarized on a per-athlete basis and was not normalized to participation time. Because participation time varies substantially by level of play, reflecting differences in roster size and substitution patterns,49,50 per-game impact counts may appear similar or lower in collegiate athletes despite markedly higher cumulative seasonal exposure. Thus, accounting for participation time may partially reconcile these apparent discrepancies. Additionally, the collegiate season-level competition value (24.2 impacts) and session-level practice value (8.2 impacts) were each derived from a single cohort due to limited data and should therefore be interpreted with caution.
Our findings highlight that collegiate players experience greater cumulative impacts throughout a season. This aligns with the results from Sproule et al., in which 25,332 total impacts were recorded for 48 collegiate athletes across a season (527.8 average impacts per athlete per season), while the 25 youth players endured a total of 3842 impacts (153.7 average impacts per athlete per season). 51 However, there is a higher per-game impact rate observed in youth athletes. This could reflect structural differences in play, such as fewer substitutions, less player rotation, and more continuous field time per athlete.49,52 Our finding on competition-based exposure deviates from the comparison study by Choi et al., in which youth athletes sustained a lower average number of impacts than collegiate players per game (7.3 impacts vs. 16.8 impacts). 47 When further narrowing down frequency measures to units of discrete time (e.g., impacts per athlete per minute), age-based discrepancies in impact occurrence actually became somewhat neutralized. This points toward the notion that although both age groups may endure impacts at a similar time-based rate, systemic factors such as increased play time, longer seasons, or more practice exposure could contribute to the observed differences in cumulative impact exposure across a whole season. This also indicates that session structure and activity type may modulate age-related differences in determining session-level HIE.
Importantly, the cumulative impact count alone is unlikely to fully capture the RHI burden. As defined conceptually, RHI reflects a dose construct incorporating both frequency and magnitude of impacts over time. 53 While total counts indicate exposure volume, they do not account for the distribution of impact severities, such as the composition of low-level and high-magnitude impacts. Accordingly, complementary metrics may improve characterization of HIE, including upper-tail kinematics (e.g., 95th percentile linear and rotational acceleration), counts above clinically meaningful thresholds (e.g., greater than 40 g), and impact locations that may differentially contribute to tissue strain. From a practical standpoint, reporting both cumulative counts and severity distributions provides a more complete description of RHI than either metric alone.
Impact severity
Even though our pooled data suggests that college-level athletes sustain impacts at a notably higher frequency during practice and combined sessions, the collegiate group displayed a more marginal increase in linear acceleration magnitude during practice (20.5 g vs. 18.1 g for median; 49.6 g vs. 47.3 g for 95th percentile) and overall season (20.7 g vs. 18.6 g for median). In fact, youth athletes had a similar 95th percentile magnitude (46.6 g) for the overall season than the 90th–95th percentile for college-level players (47.7 g), highlighting magnitudes to be generally comparable across both age groups. As noted, we emphasize 95th percentile values as they represent the upper tail of impacts sustained by athletes, which are more likely to drive acute symptomology or disproportionate brain tissue strain compared with the median impact. As such, upper-tail measures complement averages and medians by characterizing whether one group experiences a larger high-magnitude exposure profile even when central tendencies appear similar.
Interestingly, despite age-based comparability during practice and overall season, collegiate athletes exhibited a larger increase in competition-based measures (19.1 g vs. 28.8 g for median; 48.8 g vs. 61.9 g for 95th percentile). This is consistent with prior age-based comparisons that reported collegiate cohorts to have modestly higher upper-end values for magnitude, in addition to consistently increased measures in games than in practice.47,51 These findings may reflect the more controlled and instructional nature of youth practices, where contact is often moderated, in contrast to the higher-intensity, performance-driven context of collegiate competition. Despite some similarities in practice-related exposures, elevated magnitudes observed in college games could also stem from factors including greater player mass, speed, and collision forces.45,54
We report rotational acceleration magnitudes to be larger in the aggregated youth cohort during the overall season (1144.9 vs. 964.0 rad/s2 for median; 2929.7 vs. 2072.2 rad/s2 for 90th percentile). Notably, aggregate collegiate values for games at the 50th and 95th percentile rotational acceleration were unexpectedly inverted, where the 50th percentile cohort presented with a higher weighted mean than the 95th percentile cohort. However, this disparity likely reflects the relatively small sample size of the 50th percentile groups, in addition to limited and nonoverlapping datasets.
During practice, youth athletes exhibited a larger median magnitude (1173.9 vs. 989.1 rad/s2), but collegiate players seemingly displayed more variability in rotational impact magnitudes based on their higher upper-tail percentile. One potential explanation is that younger athletes are less capable of bracing and absorbing forces due to decreased neck musculature, thereby enabling greater rotational displacement during unanticipated impacts. 13 This is consistent with literature emphasizing the role of anticipatory postural adjustments in mitigating head kinematics during contact sports.55,56 It is possible that this observed age-related pattern is reversed during games, with Choi et al. reporting a significantly higher rotational magnitude in their college cohort compared with youth that is more pronounced in competition. 47 However, considering the limited pooled data on competition-based rotational acceleration at the college level, we cannot definitively conclude any trends in that setting at this time.
The observed age-group patterns in rotational acceleration are salient, given the hypothesized causal link between angular kinematics, diffuse axonal injury, and small-vessel stress.57,58 Rotational impacts preferentially strain long, myelinated axons and bridging veins. 59 Specifically, in developing brains, reduced myelin density and lower neck stiffness likely exacerbate angular displacement and shear for a given impact, as children’s weaker neck musculature and immature white-matter structure permit greater inertial head motion under load.60,61 Current imaging evidence in athletic cohorts has associated repetitive subconcussive exposure with white-matter microstructural alterations and perivascular space enlargement, even without diagnosed concussion.35,62 Although our synthesis is biomechanical rather than clinical–radiological, the relative elevation of seasonal median rotational values in youth than in collegiate players, despite lower cumulative hit counts, strengthens the rationale for interventions that specifically target angular kinematics. This may include technique coaching, neck-strengthening programs, or equipment that limits off-axis motion.63,64
Modifying factors in age-based HIE differences
It is also relevant to consider additional variables that may differ between levels of play and thus contribute to these age-related trends in HIE. For instance, Marks et al. reported levels of self-confidence and perceived support from coaching to negatively correlate with measured impact frequency in youth football players, but not in high school participants. 65 This suggests that coaching style could differentially influence HIE depending on athlete age; however, this notion will need to be assessed via further research. It is plausible that subtle aspects of team culture, such as the degree of encouragement for aggressive play or reinforcement of safe technique, could further magnify these effects. In particular, youth athletes may be more impressionable, making their exposure profiles partly dependent on how adults set expectations for play. Positional roles and positional demands also likely evolve with the level of play. Linemen have been shown to sustain frequent and often high-magnitude impacts due to repetitive line engagements, particularly at the collegiate level.46,66 Meanwhile, some youth studies report backs and receivers to experience greater rotational acceleration than linemen, suggesting positional exposure profiles differ by age.67,68
Body mass index (BMI) may be another relevant factor, considering that the youth cohort in our pooled data had a substantially lower weighted average body mass (50.8 kg) compared to collegiate players (105 kg). Prior research indicates that lighter players tend to experience higher peak accelerations, while higher BMI is associated with more frequent but lower-magnitude impacts.65,69 Differences in impact location could also reflect biomechanical or behavioral variability by age, with youth athletes more commonly enduring impacts to the back and sides of the helmet,45,70–72 as well as college athletes experiencing a greater proportion of top-of-the-head impacts.47,51 This could be attributed to level-based differences in tackling technique or neuromuscular maturity. It is also reasonable to consider that differences in coaching emphasis on head placement, combined with developmental changes in reaction time and anticipatory movement, might influence where impacts are absorbed across levels of play.
Overall seasonal structure can play a role, as the collegiate preseason often involves longer or more intensive training periods than youth football. 73 This aligns with findings that concussion risk and impact frequency are disproportionately high during the preseason in collegiate cohorts. Specifically, McCrea et al. reported 48.5% of diagnosed concussions to occur during the preseason, despite the preseason comprising only 20% of the total season duration.41,74 Interestingly, we found that across both age groups, there was a notably higher frequency of total seasonal impacts during practice than during competition, likely reflecting the greater number of practices relative to games over the course of a season. Collectively, these observations underscore that developmental, structural, and contextual factors, such as position, body composition, impact location, and season phase, likely interact with age to shape HIE patterns in football.
Our results demonstrate that session type may interact with age to modulate HIE, corroborating other age-related comparison studies.47,51,65 HIE trends in practice and competition are considerably varied in the literature. Impact frequencies and magnitudes have been reportedly larger during practice for youth,52,67,75 high school, 76 and college football.39,77 However, other studies demonstrate increased impacts and severity during competition for youth45,71 and college.74,78 Here, we report larger magnitudes during competition than during practice for both youth and collegiate athletes, with the college group exhibiting a greater degree of increase between the two settings. This differential pattern may reflect the autonomy of game dynamics, where speed, strength, and decision-making are less constrained than in structured drills. It is likely that age-based variations in practice exposure are attributed to distinct practice structures across levels of play. For instance, Campolettano et al. reported that compared with other drill types during youth practice, tackling drills without a blocker yielded the highest number of impacts exceeding 40 g. 43 Kelley et al. found that during practice, open-field tackling and install drills contributed to 43% of impacts above 60 g in youth athletes. 45
Finally, it is important to note that youth tackle football is not a homogenous exposure group across the 6–14-year range. Prior accelerometer studies suggest that HIE differs significantly between younger athletes (i.e., aged 6–9 years) and older youth (i.e., aged 12–14 years), with older cohorts generally demonstrating higher median and 95th percentile linear acceleration magnitudes and a shift toward more frequent higher-magnitude impacts, consistent with age-related increases in player size and contact intensity.75,79,80 For instance, comparisons across youth levels of play suggest that differences in body size and velocity of collisions between players, in addition to practice drill composition and contact intensity, can shift the distribution of impacts toward higher magnitudes in older youth athletes.42,67 Furthermore, even within similar youth age groups, HIE can vary substantially across teams due to differences in practice structure, drill selection, and coaching-related factors.70,81
Implications for chronic neurodegeneration
As discussed, accelerometers are a vital tool in measuring cumulative HIE, since they capture lower-magnitude impacts that do not manifest in clinical diagnosis of concussion.7,82 There is a vast amount of evidence that accumulation of RHI can contribute to degeneration and neurocognitive symptoms long after initial trauma exposure, including memory impairments, neurobehavioral dysregulation, and sleep disruption.12,83 Consequently, HIE metrics offer critical insight into quantifying neurodegenerative risk in RHI-exposed populations. This has particularly important implications for pediatric athletes, who are more vulnerable to brain injury due to developmental factors and yet, as demonstrated by our pooled data, can experience impact magnitudes comparable to collegiate players. These findings advocate for the implementation of more age-appropriate safety guidelines during practice and competition, as they raise concerns about youth athletes enduring biomechanical loads substantial enough to trigger early biological processes associated with chronic neuropathological change.
One such condition of concern is CTE, for which RHI exposure is recognized as the only definitive risk factor to date. 22 Notably, CTE pathology has been documented at autopsy in RHI-exposed individuals without concussion diagnosis, reinforcing the idea that cumulative biomechanical load could drive disease onset. 84 As such, efforts to characterize cumulative HIE via accelerometry can provide a more accurate and biologically relevant measure of exposure risk, especially when assessing long-term outcomes in youth athletes. In fact, through implementing accelerometer data, Daneshvar et al. reported that a model incorporating cumulative head impacts and linear and rotational magnitudes was the strongest predictor of CTE pathology in football-exposed brain donors, as opposed to just years of play. 23 The effects of age of first exposure, including in the context of CTE, contribute an additional component to understanding neurodegenerative risk in youth-level athletes. Although it was not found to correlate with the severity of postmortem CTE pathology, Alosco et al. reported that early exposure to tackle football, especially below age 12, significantly correlated with earlier onset of cognitive impairment and mood symptoms in life. 31
A noteworthy consideration of the literature is individual variation in concussion thresholds, such that a given high acceleration magnitude may manifest in a clinical concussion for some players but not others. In fact, the results from Rowson et al. suggest prior TBI exposure to be a pertinent risk factor for subsequent HIE and lower concussion threshold in collegiate cohorts. By implementing a subject-specific approach, in which the magnitude at which each concussed athlete sustained a concussion was used as their individualized threshold, the authors found that concussed players experienced, on average, 10.2 more high-magnitude impacts, and 17.4 more impacts equal to or greater than their concussive threshold, compared with physically matched nonconcussed controls. 40 Stemper et al. further demonstrated that higher HIE during preseason was significantly associated with higher concussion incidence during preseason, as well as throughout the whole season. 41 This relationship between HIE and concussion incidence remains relatively unstudied in youth populations, making it unclear how age may interact with this relationship. However, the observed association at the collegiate level suggests that cumulative HIE contributes to a lower threshold for concussion, potentially placing youth athletes with earlier age of exposure at greater risk for concussion and neurodegeneration.
Limitations
One limitation in our review is the methodological heterogeneity in the included articles. While 23 out of 29 studies implemented HIT systems fitted inside helmets, the remaining studies utilized alternative sensors such as mouthpieces or skin patches placed over the mastoid process. The varied locations of sensor placement could create minor discrepancies in the measurement of head kinematics, particularly with respect to rotational acceleration and impact direction. Further, because the included studies did not report device-specific calibration error in a harmonized way, we did not apply quantitative corrections for any sensor-type measurement errors. Pooled estimates should therefore be interpreted as descriptive summaries across sensor systems. This limitation is enhanced by the ongoing controversy regarding accelerometer methodology. Helmet-based systems, while widely used, can be influenced by helmet motion relative to the skull, particularly for impacts at peripheral locations.82,85 For instance, mouthguard-mounted sensors, which are rigidly coupled to dentition, have shown high fidelity for estimating skull kinematics 86 and have been adopted in some sports settings such as rugby.87,88 This variation, spanning helmet, skin patch, and mouthguard sensors, adds a degree of caution to interpreting pooled HIE estimates. Rather than a single standardized sensor system, the field may benefit from clear performance benchmarks (e.g., acceptable error bounds, repeatability, reporting conventions) to enable more consistent cross-study comparisons, guiding continued refinement and validation. Moreover, although trigger thresholds of approximately 10 g are commonly used in on-field HIE monitoring to exclude nonimpact head motions, 89 eight included cohorts did not explicitly report their threshold, which limits direct evaluation of how low-magnitude signals may influence pooled estimates. In addition, variation in trigger thresholds within the standard 10–15 g range may influence estimated HIE metrics, particularly for lower-magnitude events.
Inconsistencies in outcome metrics also challenge interpretation. Although many studies report season-long aggregates for impact frequency, others use per-session or time-based units, complicating pooled analysis and our ability to make direct comparisons between groups. Inconsistencies in setting (i.e., game or practice) create further limitations in controlling for this variable. Despite an initially large dataset from included studies, narrowing down outcome measures based on setting ultimately led to only one collegiate cohort represented for impact frequency in cumulative games per season and in individual practice sessions, in addition to one college cohort for rotational acceleration during competition only. Notably, several collegiate HIE datasets published prior to 2015 report that games involve approximately twice as many impacts as practices, with upper percentile magnitudes tending to be higher in games39,90,91; however, these were outside our prespecified window and thus not included in our synthesis. Incorporating these earlier cohorts in a subsequent expanded synthesis would increase precision and reduce reliance on single-study estimates for select severity outcomes. In addition, because a small subset of cohorts reported impact frequency as medians rather than means, pooled frequency values should be interpreted as descripted weighted summaries of reported tendency measures, rather than strictly mean-based estimates.
Furthermore, the aggregated youth-level data were derived from heterogeneous leagues, including programs like Pop Warner that have formal practice restrictions, as well as leagues without structured contact-limiting policies. This variability introduces differences in coaching practices, rule enforcement, and exposure profiles that may influence impact metrics. Consequently, while our findings corroborate evidence from Pop Warner studies supporting the effectiveness of practice-based reforms in reducing cumulative head impacts, they may also reflect data from “rogue” or nonaffiliated leagues without safeguards or medical supervision. This variation highlights the need for standardized, widely adopted policies across youth football organizations to ensure consistent reductions in HIE.
Likewise, one study measured 90th percentile measures for rotational and linear acceleration, instead of 95th percentile. 41 For our purposes, we pooled both 90th percentile and 95th percentile measures together where applicable. Considering that this study contributed data from five cohorts to the overall collegiate group, representing 1120 out of 3850 participants, this may have contributed to a slight underestimation of upper-end magnitudes in college participants. This points toward another limitation, in which some studies contributed multiple cohorts to our pool due to reporting data from multiple seasons, as was the case with Stemper et al. 41 Each season was treated as its own cohort; however, the precise degree of overlap in subjects between seasons was not reported in those original articles. This may have led to some overrepresentation of data from certain participants, albeit from different years, in the overall pooled group. Moreover, anthropometric variables (i.e., BMI, playing position, or season structure), which are potentially significant modifiers of HIE, are not always included in studies, limiting our ability to fully capture the nuances of HIE in the context of age.
Future directions and recommendations
Considering the limited direct comparisons between youth and collegiate football players, future accelerometer-based investigations may benefit from including large cohorts for both age groups, with measurement of potential covariables such as BMI. This would help derive more concrete findings on age-related differences in HIE, allowing for better risk determination in younger athletes. Further research should also prioritize standardization of measurement protocols in order to limit heterogeneity across the HIE literature and enable efficient comparisons between groups. Due to the significant role of cumulative head impact burden in promoting chronic neurodegeneration, studies can aim to incorporate biomechanical, behavioral, and neurobiological covariates into creating risk and exposure models. Longitudinal studies that link accelerometer data with clinical outcomes (i.e., neurocognitive testing, imaging, and biomarkers) are essential in elucidating causal pathways between repetitive HIE and brain injury pathology. Building on foundational work that demonstrates associations between HIE and changes in diffusion imaging or blood-based markers,92–94 future investigations should continue to employ multimodal designs to define dose-dependent relationships, clinically interpretable exposure thresholds, and risk stratification.
Future efforts to enhance player safety in youth football may increasingly focus on modifying season or session structure, providing a practical avenue for reducing cumulative impacts without fundamentally altering gameplay. For example, in 2013, Pop Warner football was among the first youth leagues to implement formal rule modifications aimed at reducing head contact during practice, based on preliminary accelerometer studies demonstrating significant proportions of high-magnitude impacts occurring in youth practice. This included eliminating head-on blocking and tackle drills starting at greater than 3 yards, restricting contact to one-third of total practice time, and removing the kickoff play. 52 Subsequent research has proven the effectiveness of these changes. Cobb et al. observed a 37–46% reduction in head impacts for teams that adopted Pop Warner’s practice structure, with competition thus becoming the dominant source of season-long impacts. 75 However, Young et al. demonstrated that after these modifications, practices remained the primary source of HIE for youth athletes, reinforcing the need for limiting contact in the practice setting. 52
Our review highlights the disproportionate contribution of practice toward cumulative HIE, as both age cohorts tended to sustain a substantially higher number of impacts during practice than in competition. Importantly, this strengthens the evidence base supporting practice-focused rule modifications as a practical and effective means of reducing repetitive trauma risk in controlled settings. Moreover, despite gains from practice reforms, competition remains a persistent and less modifiable source of exposure. However, prior work has demonstrated total impact burden to be significantly influenced by factors such as preseason structure that can be optimized without compromising the core gameplay experience. 41 This likely aligns with our reported discrepancy in age-related HIE metrics between a per-season and per-session basis, as discussed. Therefore, our results not only reinforce the significance of Pop Warner’s model for practice reform, but they also point toward the reliability of additional structural changes, such as reconfiguring preseason schedules, that can further reduce risk across youth leagues, including those that lack standardized safety regulations.
That said, complementary strategies are necessary to address the seemingly unavoidable exposure during competition at all levels of play. Although the National Football League has incorporated high-profile reforms, such as the Dynamic Kickoff rule that has reportedly reduced concussion rates for kickoffs by 43%, total concussion incidence has remained relatively stagnant over recent years.95,96 This underscores the limitations of rule-based interventions during competition. In parallel, increasing access to affordable helmet options, such as youth-specific or position-tailored designs, remains pertinent, particularly in resource-limited leagues. Together, these approaches complement one another, offering a multifaceted strategy to better safeguard athletes at all levels of play, including youths.
Conclusion
This systematic review highlights key differences in HIE between youth and collegiate American football players, emphasizing that developmental stage, practice structure, and session type all influence the distribution of impacts. Although collegiate athletes tend to sustain a greater number of impacts over the course of a season, youth athletes demonstrated per-session impact frequencies and rotational magnitudes that were comparable with, and in some cases greater than, their collegiate counterparts. These findings suggest that cumulative exposure cannot be understood solely in terms of age or level of play, but rather it reflects the interaction between training demands, game intensity, and developmental biomechanics.
An important takeaway is that youth athletes cannot be assumed to experience lower biomechanical loads merely because of their younger age or smaller body size. On the contrary, higher per-game rotational accelerations in youth players raise concern given the heightened vulnerability of the developing brain, with thinner cranial bones, less robust cervical musculature, and ongoing white-matter maturation. These developmental factors may amplify the biological consequences of impacts that approximate collegiate exposure in a mechanical context. The convergence of biomechanical and neurodevelopmental risk highlights the need for targeted safeguards in youth football.
The results also underscore the disproportionate contribution of practice to seasonal head impact burden. Across both levels, practice sessions accounted for the majority of exposures, and in youth athletes, contact density during drills appeared to drive elevated per-session accelerations. This finding carries important translational weight. Whereas competition-related exposure may be less amenable to modification without altering the foundation of the sport, practice structure is highly adjustable. Policies limiting contact intensity in youth drills, adopting progressive skill acquisition models, and instituting mandated recovery times are practical, evidence-informed avenues for reducing cumulative exposure, all while preserving participation opportunities. Collegiate programs, by contrast, may require more nuanced adjustments that involve balancing high cumulative load with the necessity of preparing athletes for competitive play.
Methodological challenges also emerge from this synthesis. Variability in sensor platforms, trigger thresholds, and reporting conventions limits comparability across studies. This likely contributed to the heterogeneity in pooled values. Establishing standardized reporting criteria, such as uniform threshold definitions, consistent reporting of both median and upper-tail accelerations, and explicit disclosure of participant carryover between seasons, would enable more reliable meta-analyses and facilitate replication across cohorts in the future. Such harmonization would also allow researchers to better clarify the contributions of team-level factors, such as coaching philosophy and contact culture, from individual-level susceptibility, such as BMI.
Future research should extend beyond descriptive biomechanical profiles to include integration with imaging, biomarkers, and longitudinal neurocognitive outcomes, building on prior multimodal work. Linking accelerometer-derived exposure metrics to downstream structural and functional changes will be critical for defining dose–response relationships and establishing acceleration magnitude thresholds that hold clinical significance. Prospective designs that follow youth athletes across developmental stages into higher levels of play may further elucidate how early-life exposures shape long-term neurological trajectories. Expanding cross-sport comparisons may also contextualize football exposure within the broader landscape of youth contact sports, informing whether observed risks are unique to football or represent generalizable features of RHI.
Ultimately, this review demonstrates that both youth and collegiate athletes sustain meaningful HIE, but the character of that exposure differs in ways that have distinct developmental and policy implications. The evidence supports a shift from focusing solely on diagnosed concussions to considering the cumulative distribution of impacts, including those that are subconcussive and clinically silent. Age-specific interventions, improved methodological rigor, and integration of biomechanical data with clinical outcomes are essential next steps in mitigating risk and safeguarding neurological health in American tackle football. By applying biomechanical findings toward a developmental framework and aligning them with feasible policy strategies, this review provides a foundation for advancing both research and practice in HIE surveillance.
Transparency, rigor, and reproducibility statement
This systematic review was prospectively registered in PROSPERO (CRD420250632766) prior to initiation of full-text screening, thus ensuring that the analytic plan, inclusion criteria, and outcomes of interest were specified. As this study synthesized published data only, Institutional Review Board approval was not required. Screening and reporting procedures are presented in a Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA) flow diagram (Fig. 1), which shows that 1219 records were initially identified, 842 records remained after removal of duplicates, and 29 studies ultimately satisfied eligibility requirements for inclusion.
Electronic searches were conducted in PubMed, Embase, and Scopus for publications between January 2015 and July 2025. Boolean combinations of controlled vocabulary and keywords were developed in consultation with a medical librarian and adapted for each database to maximize sensitivity. Two reviewers independently screened all titles and abstracts, followed by full-text evaluation of potentially eligible studies. Discrepancies were resolved by consensus, with a third reviewer available for adjudication if needed. Eligible studies were peer-reviewed, published in English, and employed accelerometer-based sensors to quantify head impacts in youth (<14 years) or collegiate (17–23 years) American football athletes. Studies focused on other sports, high school-only cohorts, non-English publications, conference abstracts, or reports lacking primary data were excluded. Where multiple publications relied on overlapping datasets, the most complete or updated report was prioritized to avoid duplication.
Data extraction was performed using a prespecified template that captured study design, sample size, athlete characteristics, sensor type and placement, linear acceleration threshold, and duration of monitoring. Outcomes extracted included the number of impacts per practice, per competition, and per season; seasonal totals; and both median and 95th percentile peak values for linear and rotational acceleration. In cases where studies reported subgroup analyses (e.g., linemen compared with other positions), each subgroup was treated as an independent cohort. For multi-season datasets, each season was considered separately as an independent cohort, while acknowledging the potential for carryover of some participants between years. When studies provided both median and mean frequencies, means were prioritized for consistency across datasets. Reports that presented 90th rather than 95th percentile accelerations were retained, but these were noted as a possible source of downward bias in upper-tail estimates. Because of variability in sensor models, reporting thresholds, and outcome definitions, a formal meta-analysis was not feasible. Instead, sample-size–weighted averages were calculated to summarize central tendencies, stratified by level of play and by session type (i.e., practice or competition). Device type was recorded for each cohort, and pooled analyses incorporated data from all device classes with recognition of this heterogeneity.
Risk of bias was assessed using the MINORS. Two reviewers independently scored each study across domains, with totals interpreted according to prespecified thresholds for high, moderate, or low risk. Reproducibility is supported by preregistration, explicitly defined eligibility criteria, dual independent screening, standardized data extraction procedures, and transparent analytic decisions. Supplementary materials provide the PRISMA diagram, study-level data tables, and risk-of-bias scores to enable independent verification. Together, these measures enhance transparency and ensure that the findings of this review are reproducible by other investigators.
Authors’ Contributions
G.S.B.: Conceptualization, formal analysis, writing (original draft), writing (review and editing), and screening. C.L.: Conceptualization, formal analysis, and writing (original draft). J.S.: Writing (original draft). S.A.: Screening. C.V.B.: Writing (review and editing). J.E.B.: Conceptualization, writing (review and editing). All authors have read and approved the final version of the article.
Footnotes
Author Disclosure Statement
J.E.B. is Chairman of the Medical Advisory Committee for Pop Warner Little Scholars.
Funding Information
No funding was received for this article.