
Abstract
Traumatic pericallosal artery aneurysms (TPAAs) are a rare but potentially fatal subset of intracranial aneurysms, typically resulting from blunt or penetrating head trauma. Located along the distal anterior cerebral artery (DACA), their deep midline position and proximity to the falx render them vulnerable to shear injury, technically challenging to diagnose and treat. They often present as pseudoaneurysms with a high risk of delayed rupture. We conducted a systematic review of studies published between 1995 and April 2025 using PubMed and Google Scholar. Included studies described pericallosal or DACA traumatic aneurysms and reported clinical, radiological, and outcome data. Extracted variables included patient demographics, mechanism of injury, diagnostic modality and timing, aneurysm characteristics, treatment type, and outcomes. Statistical analysis assessed predictors of neurological prognosis using the Glasgow Outcome Scale. Fifty-eight patients from 44 studies met the inclusion criteria. Blunt trauma was the most common cause (62.1%). Aneurysms were more frequently right-sided (69%), and nearly half were diagnosed within 2 weeks postinjury. Endovascular (39.7%) and microsurgical (55.2%) treatments were both commonly employed, while conservative management was rare (3.4%). No significant outcome differences were found between treatment modalities. Poorer outcomes were significantly associated with aneurysm rupture (p < 0.01) and older age (p ≈ 0.02), while laterality and trauma mechanism were not. Pediatric patients demonstrated more favorable outcomes. In conclusion, TPAAs are rare but clinically urgent lesions. Early vascular imaging and timely intervention are essential. Prognosis depends more on rupture status and patient age than on treatment modality. Standardized outcome reporting is needed to guide management.
Introduction
Traumatic intracranial aneurysms, though accounting for less than 1% of all cerebral aneurysms, represent a critical diagnostic and therapeutic challenge in neurovascular care. 1 While the supraclinoid internal carotid artery is believed to be the most common location for these types of lesions, pericallosal or distal anterior cerebral artery (DACA) aneurysms are also known to present in rare circumstances. 2 While certain factors are associated with the development of TAs in specific regions, such as penetrating trauma or iatrogenic injury to a specific vessel, it has been hypothesized that DACAs, particularly the pericallosal branches, are injured due to their proximity to the inferior margin of the falx. 3 Their development is often precipitated by mechanical forces that either directly lacerate arterial walls or induce shearing injuries through rapid acceleration–deceleration movements. These aneurysms may manifest as true aneurysms or pseudoaneurysms, the latter lacking all three layers of the vessel wall and being more prone to delayed rupture.
The clinical significance of traumatic pericallosal aneurysms lies in their unpredictable natural history and potential for catastrophic subarachnoid or intraparenchymal hemorrhage. Their location makes both diagnosis and treatment technically demanding due to the deep midline anatomical position and close proximity to vital cerebral structures such as the corpus callosum and cingulate gyrus. Historically, the literature on these aneurysms has been limited to isolated case reports and small case series, thereby restricting a comprehensive understanding of their pathophysiology, presentation patterns, and optimal management protocols.1,2,4
Advances in neuroimaging and endovascular techniques have improved diagnostic accuracy and expanded therapeutic options. Nevertheless, surgical intervention remains crucial in complex or ruptured cases, especially where endovascular access is limited. Prognostic variability further complicates clinical decision-making, as outcomes are influenced by multiple factors, including the timing of diagnosis, aneurysm morphology, and the presence of concomitant brain injury. Given these complexities and the rarity of this condition, a systematic review of the literature was undertaken to consolidate existing knowledge and guide clinicians with the limited evidence of management having been previously employed.1,2,4
To our knowledge, this represents the largest dedicated synthesis of traumatic pericallosal artery aneurysms (TPAAs) to date, consolidating epidemiological and clinical characteristics while also identifying trauma-specific prognostic factors (rupture, age), exploring the impact of diagnostic delay, and proposing a practical framework for early digital subtraction angiography (DSA) and treatment selection.
Methods
Search strategy
A systematic search was undertaken between the last week of March and the first week of April 2025 using PubMed and Google Scholar. Given the low quantity of articles on the subject, the search was conducted broadly with the only the keyword (“pericallosal artery” OR “distal anterior cerebral artery”) AND “aneurysm”. Inclusion criteria included articles published after 1995, with no restriction in terms of language. Two reviewers undertook the abstract and title review, and a third reviewer served as tie-breaker for inclusion/exclusion for full-text review. Abstracts from conference presentations were excluded from formal systematic analysis. However, while reviews were not included for patient data extraction, two literature reviews previously published on the topic were surveyed for potential additional references.
Case data extraction
Demographic data including sex, age, and country of reporting were extracted. The mechanism or injury or type of accident was likewise noted. The following other criteria were likewise extracted when available: (1) aneurysm data such as type, size, rupture status, and laterality; (2) clinical and imaging presentation; (3) the time from injury to symptom development, TA identification, or timing of TA treatment; (4) the type of treatment (endovascular, surgical, combined, or conservative; and (5) clinical outcomes, and, when available, Glasgow Outcome Scale (GOS) score. When narrative outcomes were reported without a formal GOS score, two reviewers independently converted descriptions into GOS categories, resolving discrepancies by consensus with a senior author. Although interrater agreement was not formally quantified, consensus was achieved in all cases. Missing data were not imputed, and sensitivity analyses were performed by rerunning outcome comparisons after excluding cases with converted GOS scores, which yielded qualitatively similar results.
Inclusion criteria and anatomical definitions
For this review, we included aneurysms arising from the pericallosal artery proper as well as other DACA branches, including the callosomarginal and frontopolar arteries. Because many case reports and small series use the broader term “DACA aneurysm” interchangeably with “pericallosal aneurysm,” we applied inclusive criteria to capture all traumatic aneurysms occurring distal to the A2 segment. However, when available, we specified the exact branch involved to distinguish pericallosal aneurysms from other DACA lesions. This approach ensures completeness while preserving anatomical precision.
Statistical analysis
Descriptive statistics were generated for demographics and aneurysm characteristics. Group comparisons were performed using Chi-square or Fisher’s exact tests for categorical variables (e.g., laterality, rupture status, and age categories) and Wilcoxon rank-sum or Kruskal–Wallis tests for ordinal outcomes (e.g., GOS across treatment groups). Laterality prevalence was specifically tested against equal distribution using the chi-square test. Early (≤14 d) versus delayed (>14 d) diagnosis was compared with Fisher’s exact test. Ordinal logistic regression was applied to assess independent predictors of GOS. Statistical significance was defined as p < 0.05, and 95% confidence intervals (CIs) are reported where applicable.
A PRISMA diagram outlining the results of our systematic search is presented in Figure 1. The broad search identified 492 titles in PubMed and 816 in Google Scholar. Surveying the literature review identified an additional number of 4 cases in the literature. The complete list of cases and their data are presented in Table 1.

PRISMA diagram: Overview of search strategy.
Summary of Reported Cases of Traumatic Pericallosal and Related Distal Anterior Cerebral Artery Aneurysms

Each row represents a published case with available demographic, clinical, radiological, and outcome information. “Time interval (days)” refers to the delay between traumatic injury and aneurysm diagnosis. “Baseline GCS” indicates the reported Glasgow Coma Scale at presentation when available. “Treatment type” is categorized as conservative, endovascular, microsurgical, or combined. “Treatment” describes the specific technique used. “GOS” indicates the converted Glasgow Outcome Scale score, Where available (1 = death, 2–3 = poor, 4 = disabled, 5 = good recovery).
Results
Characteristics of included studies
This systematic review analyzed 44 studies focused on TPAAs.2–45 The included literature comprised 24 case reports (55%), 18 case series (41%), and 2 literature reviews (4%). The primary focus of the reviewed studies varied: 18 (41%) centered on traumatic aneurysms, 6 (14%) on endovascular treatment, 3 (7%) on surgical treatment, and 4 (9%) on complications. Additional topics included diagnosis, management, clinical series, and aneurysm regrowth, each addressed in one to two studies. Across all studies, 58 individual patients with pericallosal or DACA traumatic aneurysms were identified.
Clinical characteristics
Mechanism of Injury
Among the 58 patients, blunt trauma was the most common mechanism, observed in 36 cases (62.1%). Penetrating trauma accounted for 13 cases (22.4%), iatrogenic injuries for 6 cases (10.3%), and nonaccidental trauma in children (e.g., shaken baby syndrome) was reported in 3 cases (5.2%).
Presentation Patterns
Intracranial hemorrhage was the most frequent presentation, reported in 33 patients (56.9%). Subarachnoid and subdural hemorrhages were specifically identified. Headache was reported in 10 patients (17.2%), and altered consciousness (GCS < 14) was documented in 26 cases (44.8%). Consciousness was preserved in 21 patients (36.2%), and not reported in 11 (19%). Neurological deficits (e.g., hemiparesis, visual impairment) were noted in 8 cases (13.8%), seizures in 3 cases (5.2%), and incidental aneurysm discovery occurred in 4 cases (6.9%).
Diagnostic Features
DSA was used in 21 patients (36.2%), computed tomography (CT) in 25 (43.1%), MRI in 5 (8.6%), and conventional angiography in 3 (5.2%). Four cases (6.9%) did not specify imaging modality. Time from trauma to diagnosis was available in 54 patients. Of these, 23 (42.6%) were diagnosed within 14 days, 14 (25.9%) between 2 and 4 weeks, 7 (13.0%) between 1 month and 1 year, and 9 (16.7%) on the same day as trauma. One case (1.9%) was diagnosed 4 years postinjury.
Aneurysm size varied from < 1 mm to 23 mm; however, size was not reported in 22 cases (37.9%). Locations included pericallosal artery (n = 47, 81%), frontopolar (n = 1, 1.7%), DACA (n = 3, 5.2%), and callosomarginal artery (n = 7, 12.1%). Lateralization data indicated 40 right-sided (69%) and 18 left-sided (31%) aneurysms.
Exploratory analysis of diagnostic delay and outcome
In the subset of 45 patients with both diagnostic timing and outcome data, early diagnosis (≤14 days) was associated with good recovery (GOS 5) in 16/25 patients (64%), compared to 8/20 (40%) in the delayed diagnosis group. Poor outcomes were observed in 9/25 (36%) early diagnosed cases and 12/20 (60%) delayed cases(Fig. 2). Fisher’s exact test did not show a statistically significant association between diagnostic timing and outcome (OR 0.38, p = 0.14).

Outcomes by timing of traumatic pericallosal artery aneurysm (TPAA) diagnosis. Early diagnosis (≤14 days) was associated with a higher proportion of good outcomes (Glasgow Outcome Scale [GOS] 5), whereas delayed diagnosis (>14 days) showed more poor outcomes (GOS ≤ 4). Fisher’s exact OR (early diagnosis vs. delayed diagnosis) = 3.91, 95% CI 0.76–20.28; p = 0.17.
Treatment approaches
Of the 58 patients, 23 (39.7%) underwent only endovascular procedures, 32 (55.2%) had only microsurgical treatment, 1 (1.7%) received combined therapy, and 2 (3.4%) were managed conservatively.
Endovascular Techniques
Endovascular methods included coil embolization in 15 patients (65.2%), and both parent artery occlusion and onyx embolization in 8 patients each (34.8%). Five patients (21.7%) underwent both coiling and another endovascular technique. Only 9 patients (39.1%) had documented complete radiological occlusion. Short-term outcomes were reported for 22 patients (95.7% of those treated endovascularly): 17 (77.3%) had favorable clinical results, 2 (9.1%) had hemiparesis, 1 (4.5%) was in a vegetative state, and 2 (9.1%) died.
Follow-up based on the GOS showed: GOS 5 in 10 patients (43.5%), GOS 4 in 6 (26.1%), GOS 3 in 2 (8.7%), and GOS 2 in 1 (4.3%). Follow-up data were missing in 2 patients (8.7%).
Surgical Interventions
Among the 32 patients who underwent surgery, 20 (62.5%) were clipped, 10 (31.3%) treated with trapping or bypass, and 1 each (3.1%) underwent resection or wrapping. Procedural success was reported in 11 cases (34.4%). Favorable clinical outcomes were seen in 26 patients (81.3%). Severe deficits occurred in 2 (6.3%), and death in 2 others (6.3%), while outcomes were unreported in 2 (6.3%).
Follow-up GOS scores were available for 28 patients: GOS 5 in 22 (78.6%), GOS 4 in 4 (14.3%), GOS 3 in 1 (3.6%), and GOS 2 in 1 (3.6%).
Conservative Management
Two patients were managed conservatively (3.4%). No outcome data were reported, precluding further analysis.
Long-term outcomes
Follow-up durations varied from 3 months to 2.6 years. Of 53 patients with GOS data, 33 (62.3%) had a GOS of 5, 10 (18.9%) scored 4, 3 (5.7%) scored 3, 2 (3.8%) scored 2, and 5 (9.4%) died. Five cases (8.6%) lacked follow-up data.
Statistical comparison
Among the 58 patients analyzed, aneurysms were significantly more prevalent on the right side compared to the left (40 vs. 18 cases; 69% right side, 95%-CI 56%–79%, p = 0.0039) (Fig. 3). Patients were stratified into age categories as children (0–14 years), adults (15–64 years), and seniors (≥65 years). Functional outcomes were evaluated using the GOS and categorized into three levels: poor (GOS 1–2), disabled (GOS 3–4), and good (GOS 5), with a binary variable also created to identify Good outcomes (GOS = 5). No statistically significant differences in GOS were observed between treatment modalities (conservative median 3.0 (95% CI: 1.0–5.0), endovascular median 4.0 (95% CI: 4.0–5.0), microsurgical median 5.0 (95% CI: 5.0–5.0); p = 0.146) (Fig. 4), nor between grouped treatments or when comparing endovascular to microsurgical approaches (p > 0.1). Laterality was not associated with differences in outcome (Hodges–Lehmann median difference: 0.0, 95% CI: –4.0 to 4.0; p = 0.665), whereas age category was significantly associated with GOS [Children: median GOS 5.0 (95% CI: 5.0–5.0), Adults: median GOS 5.0 (95% CI: 4.0–5.0), Elderly: median GOS 3.0 (95% CI: 1.0–5.0; p = 0.024), with poorer outcomes observed in older groups (Fig. 5). Patients with nonruptured TPAAs achieved a good outcome (GOS = 5) in 86.4% of cases (95% CI 66%–97%), compared with only 19.4% (95% CI 7%–36%) among ruptured aneurysms. This difference was statistically significant (p = 0.0111). The mechanism of injury did not show a significant association with GOS (p = 0.8907), nor with the type of treatment administered (p = 0.9524). In multivariate regression analyses, rupture remained the most significant independent predictor of poor outcome (p < 0.01), while age had a marginal effect (p ≈ 0.05–0.07). Treatment modality and aneurysm side were not independently associated with outcome.
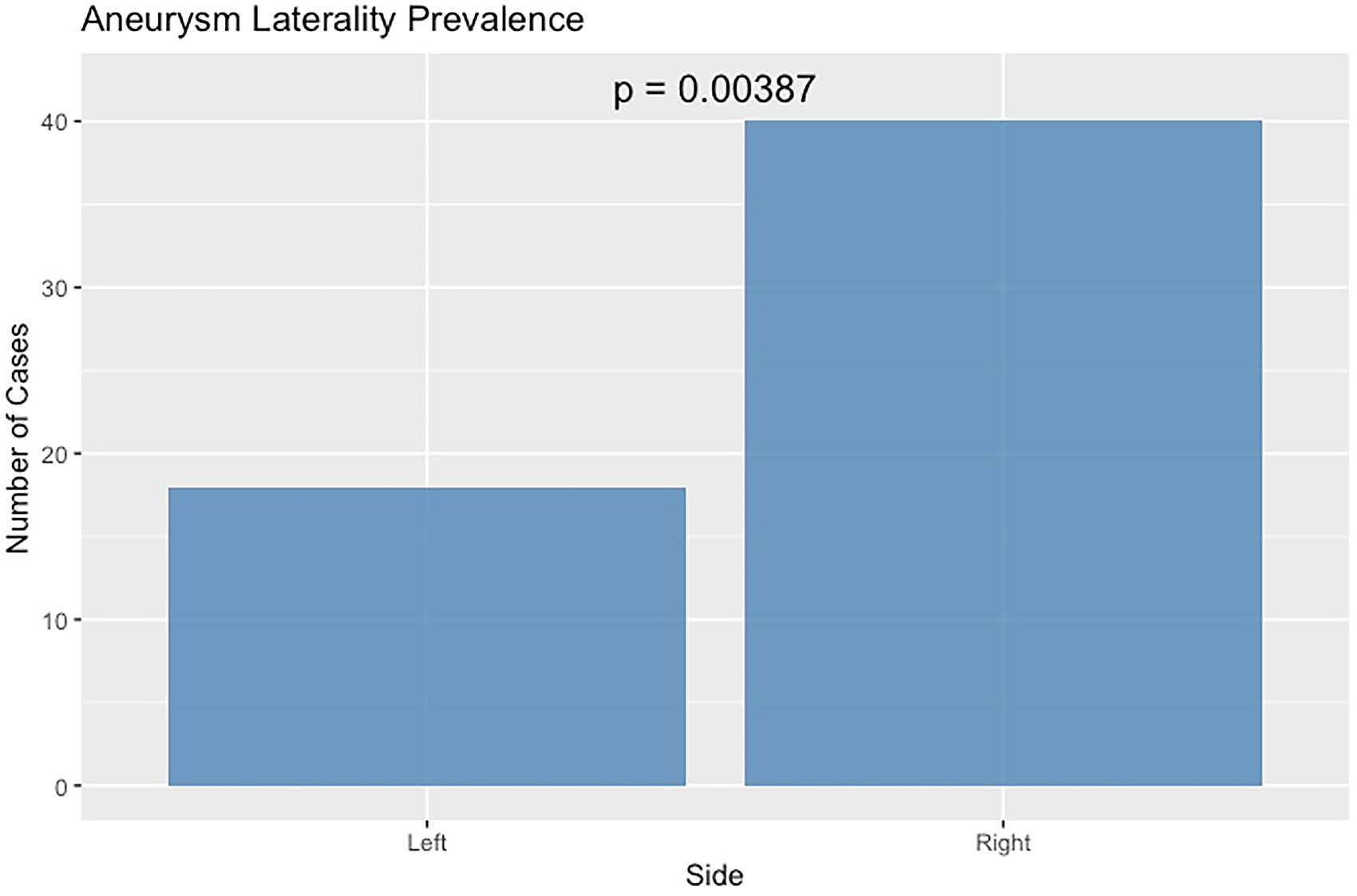
Aneurysm laterality prevalence showing a significant difference (chi-square test, p = 0.0039) with more right-sided than left-sided aneurysms.
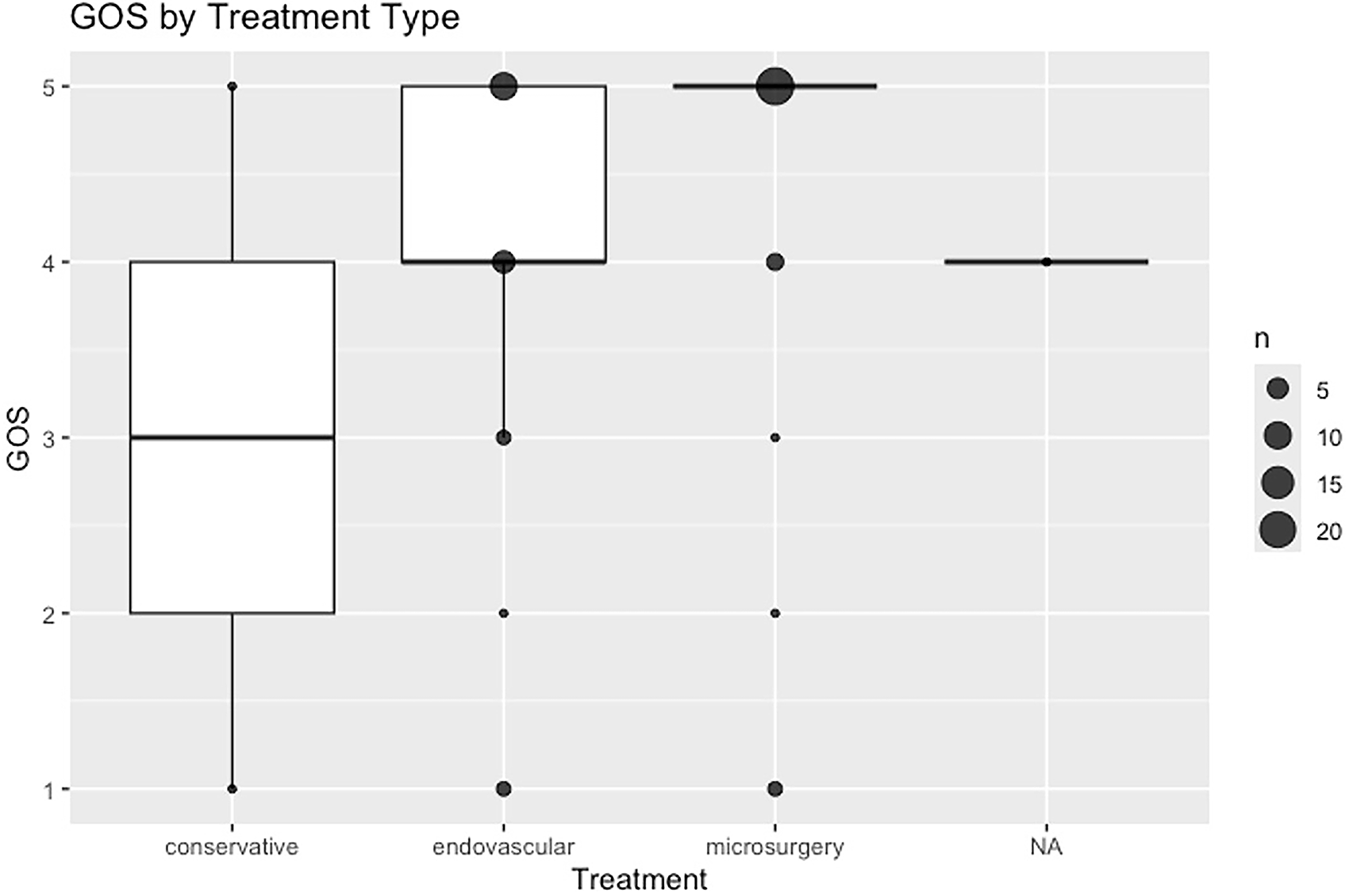
GOS by treatment type. No statistically significant difference was found between treatment groups (Kruskal–Wallis test, p = 0.1461).

GOS by age group, showing a statistically significant difference (Kruskal–Wallis test, p = 0.0243). Pediatric patients had more favorable outcomes.
Discussion
This systematic review consolidates the most extensive known case series of TPAAs, a rare but high-stakes clinical entity. Our findings build upon previous reports,2,18 confirming that blunt cranial trauma remains the predominant etiological factor, accounting for over 60% of cases. This supports existing hypotheses that shear forces generated during deceleration or rotational injuries result in focal arterial damage, particularly in pericallosal branches tethered near the falx cerebri. 3
Beyond confirming these earlier observations, our findings should be considered complementary to the recent evidence-based review by Badary et al., 46 which analyzed pericallosal artery aneurysms across all etiologies. While their work provided an essential overview of the broader spectrum of these aneurysms, our study narrows the focus to traumatic pericallosal and distal ACA aneurysms. This subgroup is characterized by distinct mechanisms of vessel injury, frequent pseudoaneurysm morphology, and clinical challenges such as delayed rupture and diagnostic latency. By concentrating on trauma-related cases, our review highlights prognostic determinants—particularly rupture status and patient age—specific to TPAAs. In this way, our analysis complements and extends the findings of Badary et al., 46 offering trauma-specific insights that may help clinicians identify high-risk patients and tailor management strategies in this rare but high-stakes condition.
Although illustrative case vignettes can be informative, the extreme rarity and diagnostic latency of TPAAs make identification of a single representative institutional case challenging. In lieu of an anecdotal example, the present systematic review allows reconstruction of a pattern-based clinical trajectory that effectively serves as a surrogate illustrative case. Across the reported patients, a consistent sequence emerges: moderate to severe head trauma—most often blunt—followed by interhemispheric or falcine hemorrhage on initial imaging, frequently without early vascular investigation, and subsequent delayed neurological deterioration or secondary hemorrhage leading to the diagnosis of a DACA pseudoaneurysm. This recurring pattern explains the high rate of delayed diagnosis and rupture observed in the literature and underscores that early recognition and vascular imaging, rather than treatment modality, represent the most actionable determinants of outcome. By synthesizing these shared clinical and radiological features, this review provides a practical framework for pattern recognition that may be more broadly applicable. This pattern also provides a useful framework for comparison with non-TPAAs.
When comparing TPAAs with non-TPAAs reported in the recent evidence-based review by Badary et al., 46 several important similarities and distinctions emerge. When all traumatic cases were considered, including pediatric and infant presentations, the mean age in our cohort was lower than that reported in nontraumatic series; however, this difference reflects a broader age distribution in traumatic cases rather than a distinct adult disease phenotype. In the nontraumatic population, pericallosal artery aneurysms predominantly affect middle-aged adults, with a reported mean age of approximately 50 years, whereas traumatic aneurysms span the entire age spectrum, including infants and children exposed to accidental or nonaccidental trauma. Despite these demographic differences, outcomes appear to be driven by similar prognostic determinants across both etiologies. In particular, rupture at presentation and advanced age consistently emerge as the strongest predictors of unfavorable outcome, regardless of whether the aneurysm is traumatic or nontraumatic. These observations suggest that trauma primarily influences the timing and mode of presentation, including diagnostic latency and delayed rupture risk, while ultimate clinical outcomes converge once hemorrhage occurs. This reinforces the importance of early recognition and vascular imaging in trauma patients, as etiology alone does not appear to mitigate the adverse impact of rupture and patient-related factors on prognosis.
Diagnostic delay
The diagnostic process for TPAAs remains fraught with delays and inconsistencies. More than one-third of aneurysms were diagnosed over two weeks post-trauma, with some identified months or even years later. This highlights the latent and insidious nature of traumatic pseudoaneurysms and reinforces the need for sustained vigilance in patients with delayed neurological deterioration. These delays have also been noted in earlier reports,31,47 underscoring the importance of developing standardized imaging protocols in the acute and subacute settings.
DSA remains the diagnostic gold standard due to its superior spatial resolution and dynamic capabilities, despite broader initial use of CT and CTA. MRI/MRA were underutilized in our cohort but may gain relevance, particularly in pediatric or iatrogenic trauma, where reducing radiation exposure is crucial.
In this exploratory analysis, no statistically significant association was found between diagnostic delay and outcome (p = 0.14). Nevertheless, the descriptive distribution indicates that many patients diagnosed beyond two weeks presented with rupture or neurological decline. Given the limited power of case-based literature, further studies are needed to clarify this association.
Treatment strategies
Treatment approaches varied, reflecting both the heterogeneity of aneurysms and institutional expertise. Endovascular therapy was employed in 23 cases, mostly using coiling or onyx embolization, and was associated with favorable outcomes (GOS 4–5) in over 77% of cases with available data. These findings reinforce the viability of minimally invasive approaches, especially for aneurysms in surgically challenging locations. 2 Conversely, microsurgical treatment was used in 32 patients and also yielded excellent results, with GOS 5 achieved in 78.6%. This slight advantage over endovascular approaches (22 vs. 10 patients with GOS 5) may reflect case selection bias, with younger or more stable patients receiving surgical intervention, or those with complex anatomy less amenable to endovascular techniques.
Treatment modality—whether surgical or endovascular—did not significantly influence GOS outcomes, and comparisons across grouped modalities also failed to show statistically significant differences. These results support the notion that both endovascular and microsurgical interventions can be equally effective when appropriately selected.
Conservative management was exceptionally rare in the published literature, reported in only two cases without detailed follow-up. As such, no reliable conclusions can be drawn regarding the safety or efficacy of noninterventional strategies. Given the high risk of delayed rupture observed in TPAAs, conservative management should likely be reserved for exceptional circumstances, such as medically unstable patients or incidental findings judged low risk by a multidisciplinary team.
Radiological outcomes
Angiographic follow-up was inconsistently reported across the included cases, with complete occlusion documented in only 9 endovascular and 11 surgical patients. This limited and selective reporting precludes a reliable comparison of the long-term durability of the two treatment modalities. Radiographic endpoints are critical in assessing aneurysm stability and recurrence, particularly for traumatic pseudoaneurysms, where regrowth or delayed rupture remains possible. Future publications should therefore systematically include angiographic follow-up in addition to clinical outcomes to enable more robust treatment comparisons.
Prognostic determinants
One of the most predictable findings was the impact of aneurysm rupture on outcome. Ruptured aneurysms were associated with significantly worse GOS scores and poorer functional categories. This held true in both univariate and multivariate models, where rupture was the strongest independent predictor of poor outcome. These results emphasize the clinical severity and urgency of ruptured TPAAs and the need for rapid intervention once rupture is suspected or confirmed.
Age was also found to influence prognosis. Patients were stratified into children (0–14), adults (15–64), and seniors (≥65), revealing a significant association between older age and worse outcomes. This trend persisted in multivariate analysis, with a marginal but noteworthy effect of age category on outcome. These findings align with prior evidence suggesting reduced neuroplasticity and increased comorbidity burden in elderly populations. 16 Although favorable outcomes in pediatric cases also support the notion of greater surgical resilience in younger brains.
Interestingly, neither the mechanism of trauma nor the type of treatment was significantly associated with outcome in multivariate models. This suggests that intrinsic aneurysm factors (e.g., rupture status) and patient-related characteristics (e.g., age) are more predictive of prognosis than the therapeutic modality itself and the underlying injury mechanism.
The statistically significant predominance of right-sided aneurysms in our review is intriguing but lacks clear anatomical justification, as no major asymmetry exists between hemispheric vascular structures. We therefore interpret this as a hypothesis-generating observation rather than evidence of pathophysiological predisposition.
Practical framework
In practice, early DSA should be pursued in any patient with interhemispheric hemorrhage or unexplained neurological deterioration following trauma, given the high risk of delayed recognition and rupture. Once a TPAA is identified, the choice of therapy is guided more by aneurysm characteristics and patient factors than by modality-specific superiority. Endovascular treatment is often suitable for anatomically accessible aneurysms, whereas microsurgical approaches remain essential for ruptured lesions, complex morphologies, or in younger, stable patients where long-term durability is prioritized. Multidisciplinary evaluation is therefore critical in determining the optimal management strategy.
To synthesize these observations into a practical guide, we propose a decision-making framework for the evaluation and management of TPAAs (Fig. 6). Any patient with traumatic interhemispheric hemorrhage or unexplained neurological deterioration should undergo early vascular imaging with CTA or DSA, as delayed recognition is frequently associated with rupture. Once an aneurysm is identified, management should be individualized following multidisciplinary discussion, taking into account rupture status, aneurysm morphology, and patient stability. Endovascular therapy is generally suited for anatomically accessible lesions, while microsurgery remains crucial for ruptured, complex, or anatomically challenging aneurysms, particularly in younger or stable patients where durability is prioritized. Conservative management has been reported only rarely and should be reserved for exceptional cases such as incidental findings deemed low risk. In all instances, close radiological follow-up is essential given the potential for regrowth or delayed rupture. This framework is intended as a synthesis of the available literature rather than a prescriptive guideline, and should be regarded as hypothesis-generating until supported by larger multicenter data.

Proposed diagnostic and management framework for traumatic pericallosal artery aneurysms.
Limitations
This review has important limitations. Most included studies were case reports or small series, making the data highly vulnerable to publication bias, with complications and deaths likely underreported, inflating good outcomes. Treatment comparisons are also subject to selection bias, as complex aneurysms were more often managed surgically while technically accessible lesions were treated endovascularly, limiting direct comparability. Follow-up was incomplete (45/58 patients), angiographic outcomes were inconsistently documented, and conservative management was reported in only two cases. In several instances, narrative outcomes were converted into GOS scores by consensus, introducing some subjectivity.
In addition, the observed right-sided predominance lacks an anatomical explanation and should be considered hypothesis-generating. Although delayed diagnosis was common and often associated with rupture, its impact on prognosis could not be formally analyzed. These constraints underscore the need for standardized reporting and multicenter data collection.
Conclusion
TPAAs, while rare, demand heightened clinical awareness due to their high morbidity and potential for delayed catastrophic rupture. This systematic review affirms that early detection through vascular imaging—particularly in patients with unexplained neurological deterioration following trauma—is essential. Both endovascular and surgical approaches can be effective, and the choice of treatment should be individualized based on aneurysm characteristics, clinical status, and institutional expertise. Our findings indicate that prognosis is less influenced by the treatment modality itself and more strongly associated with rupture status and patient age. These variables should be considered in clinical decision-making and prognostic evaluation. Future research should focus on standardized data collection, consistent outcome assessment, and comparative effectiveness studies to refine management strategies for this complex and understudied vascular pathology.
Authors’ Contributions
Conception and design: A.S., J.H., and A.N. Acquisition of data: A.S., J.H., and Y.A.-K. Analysis and interpretation of data: A.S. and J.H. Drafting the article: A.S. Critically revising the article: J.H., A.N., K.S., P.B., A.B., J.Y., and J.R. Reviewed submitted version of the article: J.H., P.B., and K.S. Approved the final version of the article on behalf of all authors: A.S. Review supervision: A.N.
Footnotes
Author Disclosure Statement
The authors report no conflicts of interest concerning the materials or methods used in this study or the findings specified in this article.
Funding Information
The authors received no specific funding for this work.
Ethics Approval
This study is a systematic review of previously published data and does not involve new studies with human participants or animals performed by any of the authors. Ethical approval was not required.
Ethics Standards
This systematic review was conducted in accordance with the principles outlined in the Declaration of Helsinki.