
Abstract
Objectives:
This study aims to explore the response to anticipatory grief of family caregivers of terminally ill cancer patients in Bangladesh and to identify key factors influencing these grief dimensions.
Methods:
This study was conducted among 88 family caregivers of the terminally ill cancer patients from three palliative care units of tertiary-level hospitals in Bangladesh. Anticipatory grief dimensions were assessed by the Adult Attitude to Grief scale.
Results:
The majority of caregivers (75%) reported severe to high levels of emotional vulnerability, suggesting an increased risk of developing complicated grief in the future. Younger caregivers (≤35 years) were significantly more likely to feel overwhelmed by anticipatory grief. Additionally, caregivers with longer prognostic awareness demonstrated lower resilience and higher emotional vulnerability. However, caregivers’ sex and their relationship with the patient were not significantly associated with anticipatory grief dimensions.
Conclusion:
Family caregivers of terminally ill cancer patients receiving palliative care in Bangladesh experience high levels of anticipatory grief. Early identification of vulnerable caregivers and provision of psychosocial support may enhance resilience and reduce caregiver burden.
Introduction
Anticipatory grief reflects the emotional response that occurs prior to the actual loss of a loved one. 1 It encompasses processes such as mourning, coping, planning, and psychosocial reorganization, which are triggered by the awareness of impending loss. 2 Approximately one-third of family caregivers of patients with life-threatening illnesses experience anticipatory grief. 3 This experience is closely linked to post-death grief, particularly in palliative care settings. 2 Although anticipatory grief is a natural part of caregiving for terminally ill patients, its impact can be profound and debilitating, negatively affecting the physical and emotional well-being of caregivers. 3
Attitudes toward anticipatory grief reflect the tension between reflexive “overwhelming” distress and the instinctive drive to maintain “control,” with caregivers attempting to balance these competing reactions through “resilient” coping. 4 Another study conceptualizes anticipatory grief as a gradual, stage-based process comprising realization, caretaking, presence, meaning-making, and transition. 5 Responses to anticipatory grief are also mediated by the nature of stressors, interpersonal and intrapersonal resources, appraisal, and coping strategies, which collectively explain individual differences in adaptation. 1
However, in the real world, anticipatory grief is not determined by a single factor but rather results from the complex interplay of multiple variables. 3 Caregivers’ age, sex, relationship with the patient, perceived social support, prior bereavement experience, and coping style all play important roles in shaping anticipatory grief responses.3,6–9 In addition, the caregiving process itself, along with increasing caregiver burden over time, may influence caregivers’ capacity to engage in and process anticipatory grief. 5 At the same time, both caregiver burden and communication act as important mediators between preparation for death, coping style, and anticipatory grief responses. 3
Studies have found that high levels of pre-bereavement stress are associated with more prolonged grief experiences. Uncontrolled and unresolved anticipatory grief, particularly when combined with maladaptive coping styles, may progress to complicated grief disorder. 5 Evidence suggests that well-prepared caregivers tend to cope better; therefore, monitoring signs of emotional vulnerability and risk of complicated grief among caregivers is essential to mitigate adverse bereavement outcomes in the post-bereavement period. 10 Understanding caregivers’ attitudes toward anticipatory grief can help palliative care professionals manage this crisis more effectively, promote family recovery, and strengthen social and psychological resources.
The issue of grief management is a reality that palliative care professionals face every day. However, research on anticipatory grief among family caregivers in South Asian countries such as India, Pakistan, Bangladesh, and Nepal remains limited. 11 In Bangladesh, palliative care is still in its developmental stage and is largely concentrated in a few tertiary-level hospitals in the capital city, along with some scattered and isolated community-based initiatives in selective urban and sub-urban areas (WHO category 3a), leaving 99% of the population with limited or no access to palliative care services. These services are predominantly focused on cancer care and physical symptom management, while psychosocial and spiritual support remain mostly unaddressed. 12 Furthermore, an inadequately trained workforce, limited communication between patients and health care teams, low public awareness about end-of-life (EOL) care, and the absence of advanced care planning further complicate the situation. 13 Against this backdrop, Bangladesh may provide a distinct socio-cultural and health care context in which anticipatory grief experiences may differ substantially from those reported in Western, East Asian, and other high-income settings. In particular, strong socio-cultural and religious norms surrounding death and dying, family-centered caregiving structures, strong expectations of familial and ethical responsibility, and culturally influenced patterns of emotional expression and communication about illness and death may significantly shape how caregivers experience and process anticipatory grief that are distinct from other regions of the world. 11
Gathering evidence from such settings is therefore important for broadening the global understanding of caregiver grief across diverse cultural and health system contexts. This study aims to examine the anticipatory grief experiences and vulnerability to complicated grief among family caregivers of terminally ill cancer patients in Bangladesh and to identify key factors influencing these grief dimensions. This evidence may serve as baseline data for the development of contextually appropriate and culturally sensitive palliative care interventions in Bangladesh and similar settings globally.
Methods
Instrument
The Adult Attitude to Grief (AAG) scale is a self-administered instrument developed to evaluate how adults experience and cope with grief.
14
It assesses three core dimensions of grief through three distinct subscales:
Overwhelmed (items 2, 5, and 7): reflects the extent to which grief dominates an individual’s emotions and daily functioning. Controlled (items 4, 6, and 8): indicates the degree to which individuals regulate or suppress their grief. Resilient (items 1, 3, and 9): captures the ability to adapt positively and maintain functioning despite loss.
Scores for each subscale range from 0 to 12, and the three subscale scores are summed to produce a total vulnerability score ranging from 0 to 36. Higher scores refer to higher grief response. Higher vulnerability scores indicate a greater risk of developing complicated grief in the future and are categorized as low vulnerability (<20), high vulnerability (21–23), and severe vulnerability (>24). 4
Translation
The translation of the AAG scale from English to Bangla was conducted according to Beaton’s guidelines. 15 Two independent bilingual translators performed forward translations—familiar with the tool’s concepts, and another unaware of the tool’s objectives. A third independent reviewer then synthesized these two versions into a single reconciled version. This version was subsequently back-translated into English by two additional translators who were unaware of the original instrument. An expert committee, consisting of research team members, an English language expert, and a Bangla language expert, reviewed all translations alongside the original scale. Face and content validity was integrated into the translation process. No major language discrepancies were identified during translation. After reaching consensus, the pre-final Bangla version was prepared for pilot testing.
Pilot testing
The pre-final translated version of the AAG tool was pre-tested among 50 adult caregivers at the radiation oncology department of the National Institute of Cancer Research and Hospital (NICRH) prior to the main study (March 2025). All of them were proficient in reading and writing the Bangla language. Participants were interviewed both before and after completing the questionnaire to identify any unclear or confusing terms. Alternative wordings and explanatory phrases were iteratively tested until suitable replacements were found. Almost 98% of participants fully comprehended all nine items. Only 5% required clarification for items 3 and 4. For these, explanatory phrasing was used instead of a literal translation to ensure the concepts were easily understood. The Bangla version of AAG demonstrated good reliability, with Cronbach’s alpha values of 0.8 for the overwhelmed subscale, 0.7 for the controlled subscale, and 0.8 for the resilient subscale. The expert committee subsequently reviewed and approved the final Bangla version of the AAG for use in the study.
Study design and setting
This cross-sectional study was conducted in the palliative care units of three tertiary-level hospitals in Bangladesh: National Institute of Cancer Research and Hospital (NICRH), Bangladesh Cancer Society and Welfare Home (BCSWH), and Dhaka Medical College Hospital (DMCH). Among these institutions, NICRH and DMCH are leading government-owned tertiary referral centers providing oncology services along with limited hospital-based palliative care. In contrast, BCSWH is a private, non-governmental initiative focused on cancer support and palliative care, offering both hospital-based and home-based services for patients with advanced disease. Together, these three centers provided a diverse representation of both public and private palliative care settings in Bangladesh, thereby enhancing the variability and transferability of caregiver experiences captured in this study.
Data were collected over a four-month period from April to July 2025.
Study population
This study included adult family caregivers (aged ≥18 years) providing care to cancer patients with an estimated life expectancy of a few days to one month, as determined by palliative care specialists. Caregivers who provided care for at least five days per week, had attended at least one EOL care discussion with the palliative care team, were aware of the patient’s diagnosis, prognosis, and terminal stage, and had a clear mind at the time of data collection were included in the study. Occasional and paid caregivers, as well as those with poor reading ability, were excluded. Sampling was conducted using a census method, meaning all eligible caregivers attending the palliative care units during the study period were included.
During the data collection period, a total of 102 EOL meetings were conducted for 102 individual terminally ill patients across three study centers, and one primary caregiver from each meeting was selected for participation based on eligibility criteria. However, due to availability, 95 caregivers were ultimately approached, of whom 88 agreed to participate (response rate 92.6%). So, the final study sample comprised 88 participants.
Data collection procedure
Data were collected through a structured questionnaire. Socio-demographic and clinical information, included age, sex, relationship of the caregivers with their patients (spouse, children, parents/siblings), duration of prognostic awareness (time since learning about the terminal stage), and duration of illness, was collected from the hospital records. Caregivers’ response to anticipatory grief was assessed using the Bangla version of the AAG scale.
One primary family caregiver per patient was invited to participate in an interview following their most recent EOL care discussion with their palliative care team. Interviews were conducted at least 3–7 days after the discussion, or later depending on the participant’s emotional readiness (as reported by the participants themselves). EOL care discussions were conducted by the treating palliative care physicians as part of routine clinical care. Information about the study was provided to participants, and written informed consent was obtained by trained research assistants who were not involved in patient care. Participants were then asked to complete the questionnaire independently. Research assistants remained present to clarify any questions during completion. Interviews were conducted in a private setting to maintain confidentiality, with close attention to signs of distress. Members of the palliative care team were also available to provide emotional support if needed; however, they did not influence participants’ responses. If any participant became distressed, the interview was paused or terminated, and appropriate support was provided by the attending palliative care team member. Questionnaires that were not fully completed were considered invalid. Each interview lasted 30 minutes or less.
Data analysis
All statistical analyses were performed using IBM SPSS for Windows, version 26.0. AAG scores were calculated according to the AAG user manual. 9 Multivariable linear regression analyses were conducted to identify these factors affecting each subscale of anticipatory grief and overall vulnerability. All statistical significance was set at a 95% confidence interval, and p-values <0.05 were considered significant.
Ethical consideration
Ethical approval for the research (approval no: NICRH/IRB/2025/69; date: 02/03/2025) was granted by the Ethical Review Committee of the National Institute of Cancer Research and Hospital, Dhaka, Bangladesh. Written informed consent was taken from all participants prior to the study. The participants were also informed that participation in this study was voluntary and that refusal or withdrawal would not affect treatment or services. The research team operated separately from the clinical team and did not participate in any clinical decision-making regarding the study participants or their patients.
Results
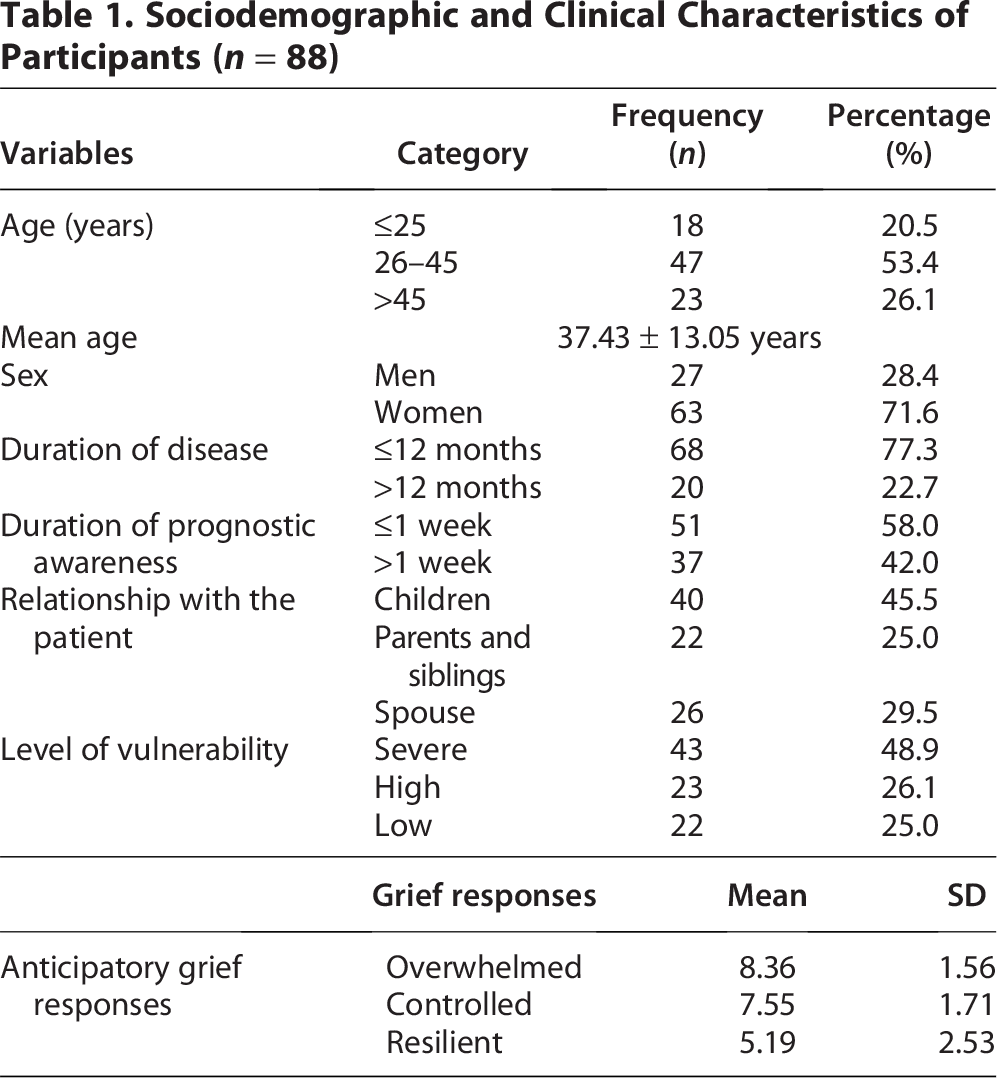
Among 88 participants, 71.6% were women and 28.4% were men, with a mean age of 37.43 ± 13.05 years. Children of the patients constituted the largest group of caregivers (45.5%), followed by spouses (29.5%) and parents or siblings (25.0%). More than half of the caregivers (58%) had learned that their patient was in the terminal stage within the previous week. Caregivers experienced high emotional distress, as reflected by the overwhelmed subscale (M = 8.36, SD = 1.56), indicating strong anticipatory grief reactions. The controlled subscale (M = 7.55, SD = 1.71) suggests moderate perceived emotional control, while the resilient subscale (M = 5.19, SD = 2.53) indicates lower resilience and limited adaptive coping. The majority of participants reported severe (48.9%) to high (26.1%) levels of vulnerability, indicating significant emotional distress and a potential increased risk of developing complicated grief in future (Table 1).
Sociodemographic and Clinical Characteristics of Participants (n = 88)
Multivariable linear regression showed that younger caregivers (≤35 years) were significantly more overwhelmed (B = 0.731, p = 0.034) with anticipatory grief. Caregivers with longer prognostic awareness (>1 week) had significantly lower resilience (B = −1.374, p = 0.010) and higher vulnerability (B = 1.479, 95% CI: 0.307 to 2.652, p = 0.014). Sex and caregivers’ relationship of with their patients showed no significant association with grief responses
Factors Influencing of Caregivers’ Response to Anticipatory Grief (n = 88)

Multivariable linear regression analyses were performed. All models are adjusted for sex, age category, prognosis awareness, and relationship with the patient.
Reference categories are: sex (women), prognosis awareness (≤1 week), age category (>35 years), and relationship with the patient (Spouse).
p < 0.05 considered as significant.
B, unstandardized regression coefficient; CI, confidence interval.
Discussion
Processing the impending loss of a loved one is a complex experience and represents a period of profound emotional vulnerability. 10 The majority (75%) of caregivers in our study showed strong grief responses and high vulnerability to developing complicated grief in future. This proportion is comparable to, and in some cases slightly higher than, previous reports, where about 47–71% of family caregivers of patients with end-stage dementia who showed high emotional vulnerability before death were at increased risk of developing post-bereavement depressive symptoms. 16 Similarly, another study found that around 18% of caregivers of terminally ill cancer patients with high pre-loss grief responses developed complicated grief in the post-loss period. 17 These findings suggest that the high level of pre-loss emotional vulnerability observed among our participants should not be considered a transient reaction but rather a persistent psychological risk that may continue into the bereavement period if left unaddressed. The elevated risk of developing complicated grief in this study may be explained by the limited access to palliative care and psychosocial support in resource-limited settings like Bangladesh. In such settings, family members often serve as the primary caregivers with minimal formal training or emotional support, which may intensify feelings of helplessness, loneliness, uncertainty, and psychological distress.18,19 This underscores the importance of early identification of vulnerable caregivers before the patient’s death and the implementation of timely psychosocial interventions to reduce the risk of adverse bereavement outcomes.
Age is an important factor affecting the response to anticipatory grief among our participants. Younger caregivers in our study were more overwhelmed by anticipatory grief. This finding is consistent with a previous study where caregivers aged <60 years experienced higher levels of pre-death grief. 20 Another study suggested that younger caregivers face greater psychological burden due to developmental life-stage conflicts and limited caregiving experience, making them more likely to feel overwhelmed and at higher risk of emotional distress even before the death of their patients. 21
Another factor affecting anticipatory grief dimensions, particularly resilience and vulnerability to developing complicated grief, found in this study was the duration of prognostic awareness among caregivers. Prognostic awareness of terminal illnesses typically evolves gradually over time, and caregivers often adopt adaptive coping strategies to manage the emotional burden of the impending death of their loved ones. 22 Previous studies suggested that, caregivers who are adequately informed about their patients’ terminal prognosis experience lower emotional distress and that a longer duration of prognostic awareness provides sufficient time to adapt psychologically and prepare for their patient’s death.23,24 However, in contrast to these findings, our study found that caregivers with longer prognostic awareness exhibited lower resilience and higher vulnerability, indicating diminished adaptive coping and increased susceptibility to adverse grief outcomes.
One possible explanation for this discrepancy may lie in contextual and cultural differences in caregiving experiences. Although not explored in the current study, in many Asian countries, including Bangladesh, discussions regarding prognosis and EOL care are often limited or partial due to socio-cultural barriers, such as the persistent taboo surrounding open conversations about death. 11 As a result, caregivers often become aware of patients’ prognosis through assumptions or informal interactions with physicians, rather than through structured or professionally guided communication. Additionally, in most resource-limited settings, structured or professional support to help caregivers process such information is often limited or unavailable. 25 Without adequate psychosocial and spiritual support, increasing awareness of patients’ progressive clinical deterioration may impose a sustained emotional burden on caregivers, rather than facilitating psychological preparedness for death. 26 As death becomes more imminent, this heightened prognostic awareness—without sufficient acceptance or psycho-spiritual support—may increase emotional vulnerability, trigger maladaptive coping responses, and heighten susceptibility to adverse grief outcomes.22,23,27,28 Moreover, prolonged and unresolved anticipatory grief may hinder the adjustment process and contribute to more severe post-bereavement grief reactions. 29 Evidence suggests that culturally sensitive and clear communication regarding prognosis, when combined with appropriate psychosocial support, can enhance acceptance, strengthen adaptive coping mechanisms, and reduce grief-related complications.6,10,30 These findings underscore the need to integrate culturally tailored communication approaches and structured psychosocial support systems into palliative care services in low-resource settings such as Bangladesh in order to reduce the risk of adverse grief outcomes among caregivers.
Limitations
Our study had some limitations. First, the cross-sectional design limits causal inferences and the ability to examine longitudinal changes in grief responses. Second, the self-reported nature of the data may have introduced bias. Additionally, factors such as caregivers’ mental health, coping strategies, and social support were not assessed, which may have influenced the findings. Also, apart from internal consistency, other psychometric properties of the AAG scale, such as construct validity, convergent validity, and test–retest reliability, were not formally assessed in this study.
Conclusion
Family caregivers of terminally ill cancer patients in Bangladesh experience high levels of anticipatory grief and emotional vulnerability, which increases their risk of developing complicated grief in the future. Early identification of vulnerable caregivers and interventions aimed at improving coping strategies and social support may reduce the psychological burden associated with anticipatory grief.
Authors’ Contributions
S.A.K. and J.B. envisioned and outlined the study. N.M.A., M.I.R., I.F., N.I., S.R.S., and R.J. were responsible for data collection, entry, and analysis, and prepared the initial draft of the article. S.A.K. and J.B. critically reviewed the article draft and provided expert opinion. W.W.M. re-analyzed data and prepared the article draft during revision. J.B. supervised and prepared the final article for submission.
Data Sharing Statement
All data relevant to the study are accessible in Mendely data, doi: 10.17632/km7nzgy7z5.1.
Footnotes
Author Disclosure Statement
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this article.
Funding Information
The authors of this study received no funding from any profit or nonprofit source.
Supplemental Material
Abbreviations Used
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.