
Abstract
Background:
Extremely premature infants (<28 weeks gestational age) have a greater risk of mortality and, when they survive, higher rates of significant neurological disability and need for medical care. As a result, extremely premature infants and their families often benefit from early involvement of palliative care.
Objectives:
To identify possible associations between palliative care consultation and length of life, code status, and manner of death of extremely premature versus nonextremely premature neonates.
Methods:
A retrospective, cohort study of premature infants with a terminal admission at two academic medical centers in the southeastern United States. The primary hypothesis was that extreme prematurity was associated with receipt of a palliative care consultation. Secondary hypotheses examined the association between extreme prematurity with (1) time from admission to death and (2) code status and manner of death.
Results:
Extreme prematurity was associated with a lower likelihood of a palliative care consultation (p < 0.001) than for older neonates. When consultations occurred, they were often within the final days or hours of life. Females had a 43% higher likelihood of a palliative care consultation than males when controlling for other factors (p < 0.001). Extremely premature infants had lower odds of having an allow natural death versus full code status than older infants (p = 0.008).
Conclusions:
Infants born extremely premature were less likely to receive palliative care consultation during a terminal admission than older preterm infants. Considering the higher burden of comorbidities and later nature of consultation, extremely premature infants may benefit from earlier and more frequent integration of palliative care.
Key Message
Infants born with extreme prematurity (<28 weeks gestational age) have a high risk of morbidity and mortality, yet they were less likely to receive a palliative care consultation during their terminal admission. This finding supports the need for early integration of palliative care resources for this high-risk population.
Introduction
Premature infants have a high risk of morbidity and mortality, with approximately 65% of infant deaths in the United States occurring in infants born preterm (<37 weeks gestational age). 1 In 2022, the mortality rate was 175.18 deaths per 1000 live births for preterm infants (<32 weeks gestational age) versus 2.18 deaths per 1000 live births for at-term infants (37–41 weeks gestational age). 1 Prematurity is the leading cause of death in neonates, higher than genetic anomalies or other incurable conditions.1–5 Furthermore, extreme prematurity (<28 weeks gestational age) has an even higher burden of morbidity and mortality, especially in neonates born in the periviable period of 20–25 weeks gestational age.6,7 Extremely premature infants now have better survival rates with advances in medical care that have (1) enabled prenatal detection of serious genetic and anatomical defects, 8 (2) slowed or stalled overall morbidity,5,9–11 and (3) established protocols for resuscitation of neonates as young as 22 weeks gestational age in some centers. 9 Despite these improvements, this population has ongoing medical and psychosocial complexities that begin during their neonatal intensive care unit (NICU) admission and may benefit from specialty palliative care early during their hospitalization. Yet formalized palliative care is often offered late, or not at all, in a premature neonate’s course.8,9,12
For terminally ill neonates, palliative care focuses on both the infant and their family. This care may combine curative medical or surgical care with that focused on improving quality of life. Moreover, this care relies on an interdisciplinary team of physicians, advanced practice providers, social workers, chaplains, and grief and bereavement specialists to reduce both physical and psychosocial hardship.2,8,13 According to the World Health Organization, pediatric palliative care is the “active total care of the child’s body, mind, and spirit, and also involves giving support to the family. It begins when illness is diagnosed and continues regardless of whether or not a child receives treatment directed at the disease.” 14 Based on this definition, palliative care should begin at birth for many premature infants. Although prenatal discussions with the palliative care teams are a potential option for families, deliveries of extremely premature infants are often unexpected and abrupt, giving less time to plan and coordinate palliative care consultation. With these logistic constraints, palliative care for neonates is less commonly combined with immediate goal-oriented, potentially curative therapy. 15
A great number of neonates at end-of-life receive overall care from neonatologists who may lack specific, additional training in palliative care. 2 This trend suggests that families and clinicians may benefit from the involvement of palliative care specialists in the care of these infants. However, a survey of critical care team members identified several barriers to formalized palliative care consultations in the NICU. These barriers included a lack of familiarity with palliative care involvement, absence of specific protocols, and perceived hesitancy or comfort from families. 15 Additionally, survey respondents (neonatologists and palliative care physicians) across Level IV NICUs across North America describe variability in resources for neonatal palliative care as well as variability in diagnoses that would typically trigger palliative care consultation. 16 Despite these limitations, experts continue to suggest early palliative care consultation as a multidisciplinary approach to support parents; assist with complex, shared decision making; and align care of the critically ill neonate with family goals.4,17–23 Palliative care consultation is associated with improved patient-centered outcomes in children with serious illness, but the magnitude of these effects has not been extensively studied in premature neonates receiving care in the NICU.
In this study, we aimed to identify trends in palliative care use in extremely premature infants along with associations between palliative care consultation and the patient’s length of life, code status, and manner of death.
Methods
Study design
In this retrospective cohort study, we evaluated the involvement of palliative care teams during the terminal admission of patients to the NICU at two academic institutions in the southeastern United States. Data were obtained from hospital records of all premature neonates who were born at <37 weeks gestational age and died before discharge from the NICU between February 1, 2020, and February 28, 2023. Infants were excluded if they were born at full term (≥37 weeks gestational age) or were delivered and died in the delivery suite. The study was deemed exempt from requiring patient or proxy consent by the institutional review boards at the Medical University of South Carolina (MUSC) and Atrium Health Levine Children’s Hospital (AHLCH).
Patient characteristics
We obtained data on patient demographics, including gestational age at admission, birthweight, sex, parent-reported race and ethnicity, whether or not English was the primary language, and insurance status (private, public, uninsured, or unknown). We abstracted data related to the provision of palliative care during the patient’s hospitalization. These data included the occurrence of prenatal palliative care consultation, occurrence of palliative care consultation during the terminal admission, time from admission to palliative care consultation, time from admission to death, and time from palliative care consultation to death. While standardized consult criteria (i.e., trigger consults) are generally not utilized at one of the institutions for prenatal consultation, palliative consultation is frequently requested for fetal concern of serious or life-threatening abnormalities. In contrast, at the other institution, there are standard criteria for palliative prenatal constitutions including severe genetic anomalies (i.e., Trisomy 13, 18), anhydramnios, single ventricle or complex CHD, anencephaly or severe neurologic defect, giant omphalocele, and severe congenital diaphragmatic hernia. These consults are done jointly with the neonatologists.
We also collected health-related information about the patient. This information included the presence of congenital heart disease; severity of congenital heart disease (none, acyanotic, cyanotic); presence of chromosomal abnormalities; presence of syndrome(s); presence of other major comorbidities including bronchopulmonary dysplasia and/or other major pulmonary disease, intraventricular hemorrhage and/or other major neurologic insults, and metabolic disorders. Finally, we abstracted data surrounding manner of death and resuscitation preferences, specifically the patient’s recorded code statuses at admission and at death.
Statistical analysis
Descriptive statistics by center were calculated for all patient characteristics. All analyses were conducted in SAS version 9.4 (SAS Institute, Inc) and R version 4.2.1 (R Foundation for Statistical Computing).
Evaluation of time to palliative care consultation
We examined the association between extreme prematurity and time to palliative care consultation using a competing risk approach. 24 An initial univariate model was fit to examine the association of extreme prematurity with time to consultation. A multivariable model was also fit to examine the impact of extreme prematurity on time to palliative care consultation controlling for other relevant factors. All factors with a univariate association of p < 0.2 were considered in the multivariable model, and backward selection was used to identify the final model while retaining all predictors with p < 0.1. Death was treated as a competing risk for occurrence of a consultation, and all models included a clustering effect for the medical center (MUSC or AHLCH) to account for potential dependence within site.
Relationship between extreme prematurity and time to death
We examined the relationship between extreme prematurity and time from admission to death using a frailty model that included a random center effect to account for clustering within center (MUSC or AHLCH). We initially considered univariate associations and then fit a multivariable model that considered all variables with a univariate association of p < 0.2. However, because gestational age was our primary covariate of interest, this variable was considered and retained in the model regardless of statistical significance. Backward selection was used to identify additional covariates, retaining all predictors with p < 0.1.
Relationship between manner of death or code status and extreme prematurity
We examined the relationship between extremely prematurity and a code status at the time of death (defined as full, limited, or allow natural death [aka do not resuscitate]) using a generalized logistic regression model. We also examined the association between extreme prematurity with manner of death (defined as escalation, resuscitation, or transition to comfort-based care) using a generalized logistic regression model.
Results
Of the 236 included patients, 108 (45.8%) were females, and 128 (54.2%) were males (54.2%). Within the cohort, 107 (45.3%) patients were Black, 86 (36.4%) were White, 36 (15.3%) were of another race, and 7 (3.0%) were of an unknown race. The median (interquartile range) gestational age of patients was 28.4 (24.7–40.4) weeks, with 116 (49.2%) infants identified as extremely premature (Table 1).
Patient Characteristics (N = 236)
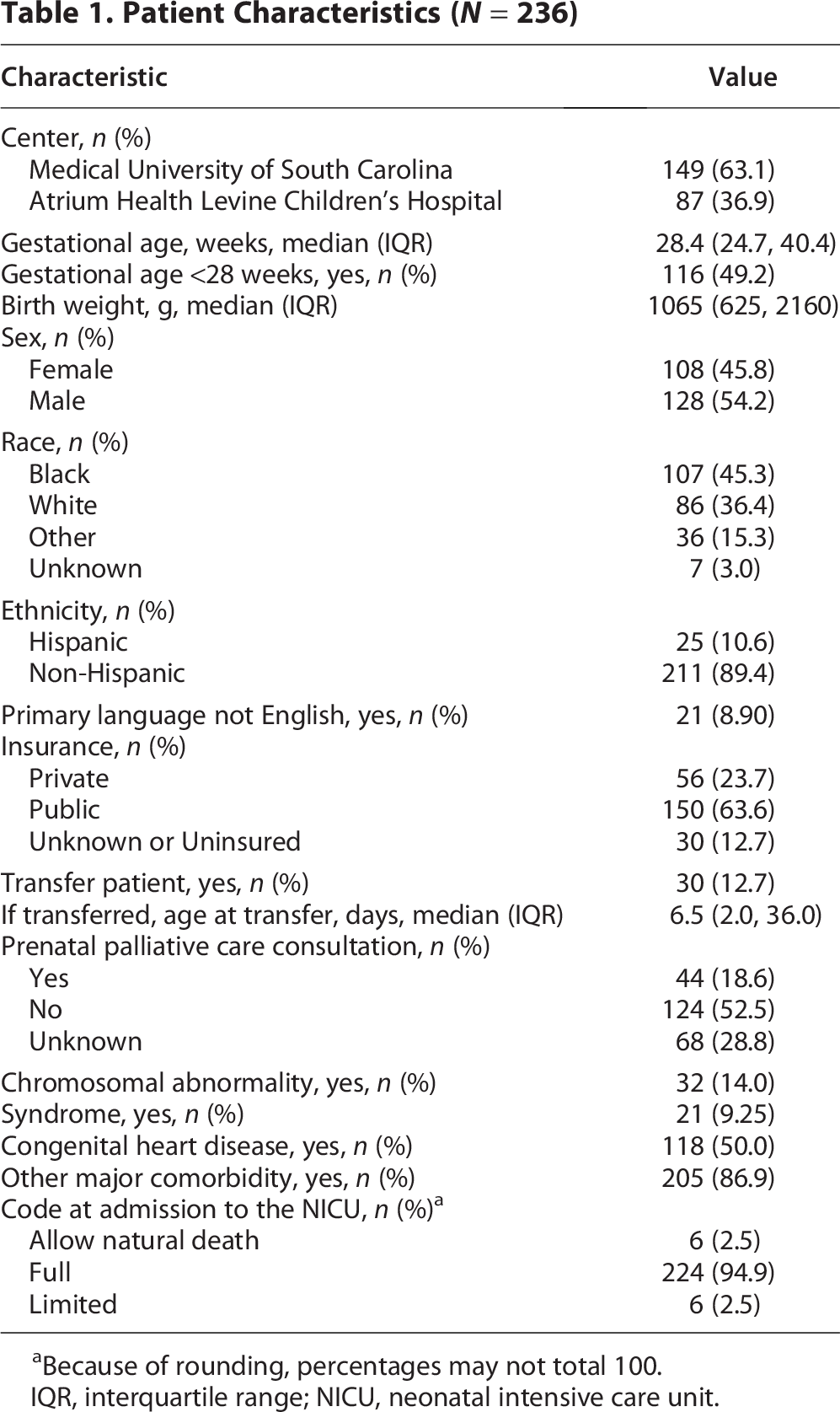
Because of rounding, percentages may not total 100.
IQR, interquartile range; NICU, neonatal intensive care unit.
Evaluation of time from admission to palliative care consultation
Fifty-five (47.4%) extremely premature infants received a palliative care consultation during their terminal admission vs. 81 (67.5%) infants born at 28 weeks gestational age or later. In univariate models, time from admission to palliative care consultation was significantly associated with several patient characteristics. Extreme prematurity was associated with a reduced likelihood of a palliative care consultation (hazard ratio [HR], 0.55; 95% CI, 0.40–0.77) p < 0.001). Sex, race, occurrence of a prenatal palliative care consultation, chromosomal abnormalities, presence of a syndrome, congenital heart disease, and presence of other major comorbidities were associated with having an earlier palliative care consultation (Table 2). There were no differences between cyanotic and acyanotic lesions, so the groups were combined under the category of congenital heart disease.
Univariate and Multivariable Competing Risk Regression Models for Clustered Data Examining Time from Admission to Palliative Care Consultation a

Death was treated as a competing risk.
HR, hazard ratio.
In the multivariable model including extreme prematurity, we retained sex, race, prenatal palliative care consultation status, and presence of other major comorbidities as additional covariates. Extreme prematurity was associated with a 23% lower likelihood of a palliative care consultation when adjusting for sex, race, prenatal consultation, and the presence of other major comorbidities (HR, 0.77; 95% CI, 0.65–0.93; p = 0.006). Females had a 41% higher likelihood of a palliative care consultation than males when controlling for other factors (HR, 1.41; 95% CI, 1.24–1.60; p < 0.001). Black infants had a 17% greater likelihood of having a palliative care consultation than infants of other or unknown race, though this difference was not statistically significant (p = 0.055). No significant differences in the likelihood of having a palliative care consultation were found between White infants versus Black infants or between White infants versus infants of other/unknown races. Families who received a prenatal palliative care consultation were more than twice as likely to have a palliative care consultation after delivery when adjusting for other factors (HR, 2.55; 95% CI, 1.37–54.77; p = 0.003). Also, patients with other major comorbidities were twice as likely to have a palliative care consultation than those without other major comorbidities (HR, 2.10; 95% CI, 1.99–2.21; p < 0.001) (Table 2).
Relationship between extreme prematurity and time to death
In univariate models, time from admission to death was not associated with extreme prematurity (p = 0.785). However, time to death was associated with the presence of congenital heart disease, presence of other major comorbidities, and insurance status (Table 3).
Univariate and Multivariable Cox Regression Models of Time from Admission to Death
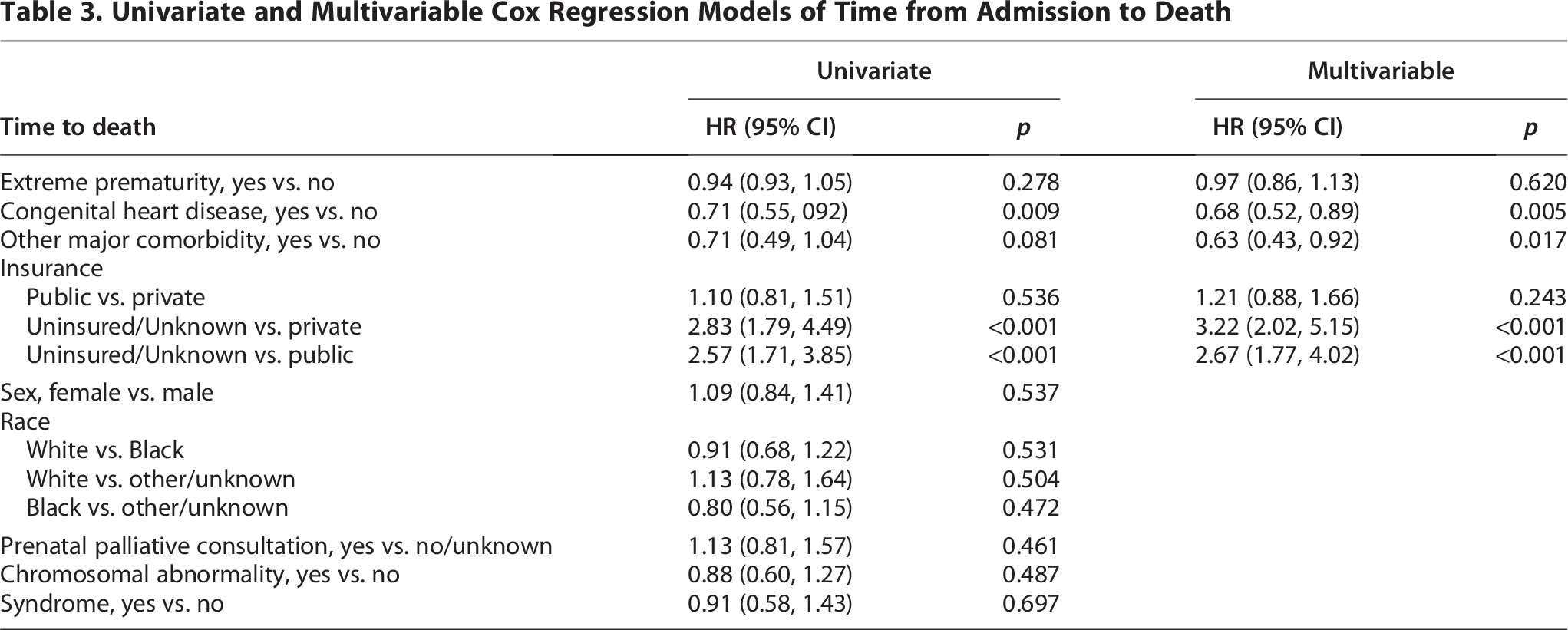
The multivariable model included extreme prematurity, congenital heart disease status (cyanotic and acyanotic lesions remained combined), presence of other major comorbidities, and insurance status. All variables, except gestational age, remained significant in the multivariable model controlling for other variables. Similar to the univariate results, there was no significant difference in time to death between extremely premature infants and infants born at 28 weeks gestational age or later after controlling for other covariates (HR, 0.96; 95% CI, 0.74–1.25; p = 0.778). Having a congenital heart condition was associated with a >30% lower hazard of death when controlling for gestational age and insurance status (HR, 0.67; 95% CI, 0.451–0.88; p = 0.009). Also, having other major comorbidities was associated with a >30% lower hazard of death when controlling for gestational age, congenital heart disease, and insurance status (HR, 0.43; 95% CI, 0.43–0.92; p = 0.018). Additionally, infants who were uninsured or had unknown insurance status had >2.5-fold increase in the hazard of death compared to infants with private (HR, 3.22; 95% CI, 2.02–5.15; p < 0.001) or public insurance (HR, 2.67; 95% CI, 1.77–4.02; p < 0.001) after controlling for other covariates (Table 3).
To provide a visual comparison of how increasing gestational age affects these outcomes, we created Kaplan–Meier curves for the time to palliative care consultation and time to death of premature infants by gestational age <28 weeks and ≥28 weeks (Fig. 1).
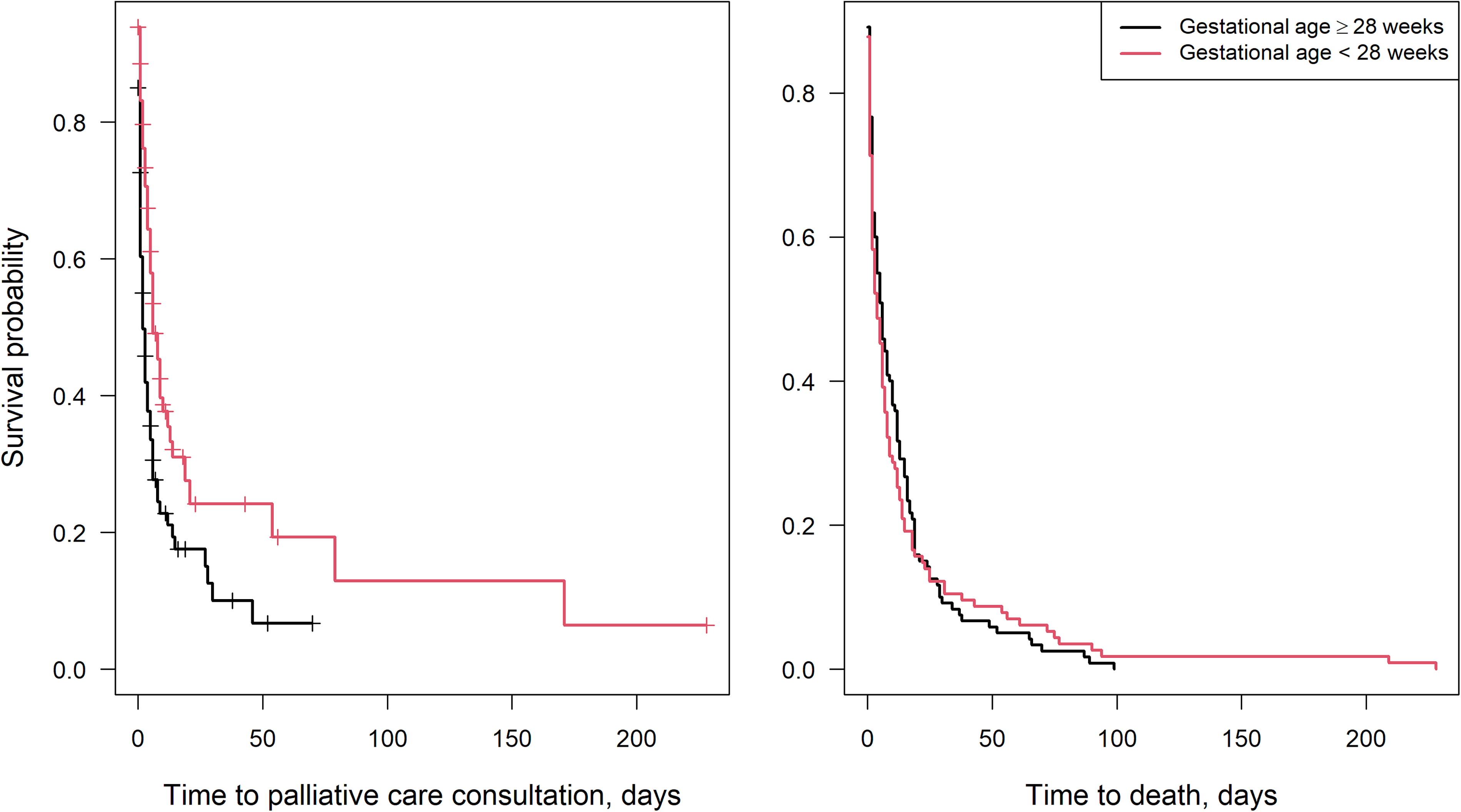
Kaplan–Meier curves of time to palliative care consultation and time to death of premature infants by gestational ages <28 weeks and ≥28 weeks.
Code status at the time of death and manner of death
We compared the odds of the code status at death in extremely premature infants born at <28 weeks gestational age versus premature infants born at 28 weeks gestational age or later. We found that extremely premature infants had significantly higher odds of a full code versus allow natural death status than older neonates (odds ratio [OR], 2.44; 95% CI, 1.27–4.76; p = 0.008).
We also compared the odds of different manners of death. Compared to older premature neonates, extremely premature infants had significantly higher odds of resuscitation versus transition to comfort-based care (OR, 3.39; 95% CI, 1.45–7.91; p = 0.005) or no escalation of care (OR, 9.37; 95% CI, 2.91–30.2; p < 0.001) (Table 4).
Manners of Death Between Infants Who Were Extremely Premature versus Premature at ≥28 Weeks
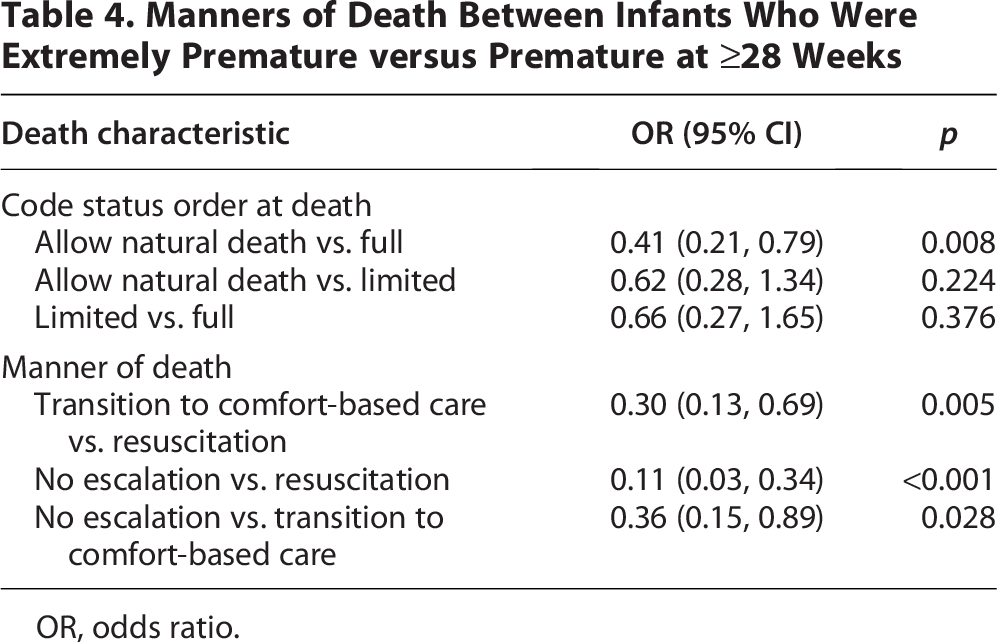
OR, odds ratio.
Discussion
Hospital-based palliative care has existed in the United States for more than three decades. 9 Yet, our findings from this retrospective, multicenter study align with previous work suggesting that formalized palliative care is often lacking or offered late in a neonate’s course.8,9,12 We found that extremely premature infants born at <28 weeks gestational age were less likely to receive a palliative care consultation during a terminal admission than were older preterm infants. When palliative care was used, extremely premature infants received consultation later in the terminal admission, often within the last hours to days of life, than older preterm infants. Extremely premature infants were more likely to receive full resuscitation attempts at the time of death and more likely to have a full code status at the time of death than older preterm infants, which aligns with the findings of other retrospective analyses. 25 These findings suggest a potential opportunity to intensify involvement of palliative care specialists in the care of extremely premature infants and the potential impact an increase in specialty involvement and/or crossover palliative care principles by neonatologists may have for this patient population.
To address the heterogeneity in palliative care consultation for premature neonates, standardized care practices could be implemented. For example, in some institutions, palliative care involvement is automatically triggered for neonates who are at the margins of viability, have an antenatal or postnatal diagnosis of a life-threatening condition, or have deteriorated despite all appropriate medical efforts.3,8,13,15 Introduction of triggers for palliative care consultation was shown by Nguyen et al. 26 to increase consult rate and awareness of services, providing clear guidelines for providers to complement their existing knowledge from intensive care training. 26 Also, given the high predicted mortality in certain infant populations in the NICU, involvement of a palliative care team early in the patient’s course could help establish a known and trusted source of support for families whose infants experience complications or who do not survive. 27 This approach could improve inconsistencies across care teams and work shifts that are related to the current model of using palliative care “as needed.” 28
Importantly, given the relative shortage of palliative care physicians, additional or strengthening of existing training for neonatologists in palliative care practices could help bridge potential care gaps. For example, the neonatology team can provide primary palliative care concepts such as pain management, and begin discussions surrounding prognosis, goals of treatment and code status. 29 Fellowship-trained palliative care physicians can assist with more complex medical cases or conflict management, whether between care teams and the family or among multidisciplinary or subspecialty teams. 29 Given the ever-increasing medical complexity of this patient population, the expansion of primary palliative care, as managed by the neonatologists, could benefit patients and their families. 16 These standardized practices could help facilitate specialized palliative care consultation earlier, alongside primary palliative and curative care, and across what can be a long, unpredictable NICU course. 3
An important challenge with palliative care is ensuring equitable, consistent use of palliative care consultation. Our findings uncovered potential disparities in receipt of palliative care services across sex, race, ethnicity, and insurance status, similar to that found in other studies. 30 For example, in our cohort, we uncovered differences in timing of palliative care delivery between male and female neonates in a multivariable model. In other studies, palliative care consultation was delayed or referred less often among various subsets of pediatric populations, which revealed racial, ethnic, and socioeconomic inequities.30–32 To address these disparities, a standardized approach for palliative care consultation, as well as other multilevel interventions, could be implemented in the NICU and tailored to existing resources.
The benefits of integrating palliative care services in the NICU are multifold. First, early palliative care integration helps to build a solid foundation with the patient’s family and may facilitate difficult discussions across multiple specialties and subspecialties. 33 Second, consultation and co-management by a palliative care team may reduce potential harms to neonates and decision-making distress for caregivers.3,8 Third, palliative care is a potential longitudinal resource for care coordination in the rising number of preterm infants and their families who survive to discharge 7 or for those families of neonates who die. 16 Finally, in a survey of NICU professionals, nearly all respondents reported that their medical team and families would benefit from a dedicated, formal palliative care team. 27 However, given the relative shortage of specialized palliative care physicians, encouraging education and coordinated training for primary neonatologists with specialized palliative care physicians could facilitate wider access to care. 16 These compounding benefits suggest a crucial need to integrate palliative care access across the care continuum of a neonates’ hospital admission, whether by expanding primary palliative care by the primary neonatology team or by earlier consultation of specialized palliative care.
To establish and expand a neonatal palliative care service, several strategies can be explored.34,35 For example, prenatal education and counseling, when feasible, can help families understand where palliative care and intensive care approaches overlap and where they diverge, including considerations as the gestational age decreases. 11 The generalist plus specialist concept for primary palliative care prior to consultation for specialty palliative care 29 can expand overall access to primary palliative care by neonatologists while targeting more complex cases for the specialty-trained palliative care physician. To this end, process frameworks could screen all admitted patients for appropriateness of palliative care consultation. 36 Appropriate assessment could include diagnosis-specific triggers based upon neonatology and palliative care discussions and preferences at each individualized center. 16 This screening would address commonly reported barriers to palliative care use, including prognostic uncertainty, team or family acceptance of prognosis, lack of education, and lack of consistent care models.4,13,15 In addition, the approach of using trigger criteria has sustained success in improving access to palliative care in neonates admitted to the NICU with severe, life-threatening conditions.33,37
The results of this study should be interpreted in the context of several limitations. First, our retrospective approach of describing the use of palliative care consultation may not capture all instances of team involvement (e.g., “curbsides”), late documentation of consultations, or consultations that took place before admission (outside institution or prenatally). Second, we did not describe efforts from the primary NICU team to provide goal-concordant care through prognosis conversations, family meetings, code status discussions, or goals of care documentation. Third, we did not capture neonates who received palliative care consultation, survived, and were discharged from the hospital. Fourth, while we did attempt to control for severity of comorbid disease by accounting for major comorbidities, congenital heart disease, chromosomal abnormalities and syndromes, this may not fully capture the severity of illness or the suddenness versus expectedness of the terminal event when comparing the relationship between gestational age, deaths and palliative care consultation. Fifth, the two high-volume NICU centers in this study showed important differences. For example, AHLCH had less-frequent use of palliative care consultation and a lower median gestational age of infants. However, both centers had a balanced total proportion of extremely premature infants and, even after adjusting for center, the trends remained significant. Although these centers have several differences, both are in the same geographic region and may not represent all NICUs across the United States.
Conclusions
In this study, we found that extremely premature infants were less likely to receive a palliative care consultation during their terminal admission than older preterm infants. When extremely premature infants did receive a consultation, this consultation occurred later during their care. Moreover, extremely premature infants were less likely to have limited resuscitation than a full code at the time of death. Although more work is needed to develop an intervention that increases awareness and use of palliative care for extremely premature infants, our study highlights the urgent need for greater integration of palliative care for these high-risk infants. Moreover, there is an opportunity for future research in the palliative care utilization and patterns in the neonatal population, especially within diagnosis-specific trigger criteria and within gestational age ranges (i.e., 22–24 weeks vs. 25–28 weeks).
Footnotes
Acknowledgments
The authors thank Crystal Herron, PhD, ELS(D), of Redwood Ink, LLC, for editing of the article.
Author Disclosure Statement
None of the authors have any conflicts of interest to disclose.
Funding Information
This publication was supported, in part, by the