
Abstract
Background:
Bereavement is a known risk factor for depression; however, the prevalence of depression and its associated factors among family members who provided home care for terminally ill cancer patients remains unclear.
Objectives:
This study aimed to investigate the prevalence of probable depression and associated factors among bereaved family members of cancer patients who died at home in Japan.
Design:
A multicenter cross-sectional study within a prospective cohort using a self-administered questionnaire survey of bereaved family members.
Setting/Subjects:
Twenty facilities across Japan participated. Bereaved family members of adult cancer patients who died at home were surveyed.
Measurements:
Depression was assessed using the Japanese version of the Patient Health Questionnaire-9, with probable depression defined as a total score of ≥ 10.
Results:
Among 195 bereaved family members, 23 (11.8%; 95% CI: 7.3–16.3%) screened positive for probable depression. Factors significantly associated with depression included unpreparedness for death (OR 11.0; 95% CI 2.8–43.8), caregiver’s poor physical condition while providing care (OR 7.4; 95% CI 1.4–39.2), patient dyspnea within one week before death (OR 4.5; 95% CI 1.3–15.6), and use of antipsychotics at the start of home care (OR 6.3; 95% CI 1.2–32.2).
Conclusions:
A substantial minority of bereaved family members screened positive for probable depression after providing home care. In addition to effective symptom management, especially for dyspnea and addressing neuropsychiatric instability (as indicated by the need for antipsychotics), during home care, ensuring that family members are adequately informed about the patient’s condition and addressing their physical well-being may help reduce the risk of depression in bereaved family members.
Key Message
Approximately 12% of bereaved family members who had provided home cancer care screened positive for probable depression. Lack of preparedness for death and caregiver physical strain were strongly associated with depression, highlighting the need for proactive psychological and physical support from home palliative care teams.
Introduction
Bereavement is recognized as a significant risk factor for the onset of depressive symptoms. 1 A previous study reported that some bereaved family members who cared for cancer patients experience intense psychological distress and depression after the death of their loved one, 2 suggesting that this should be an important focus in palliative care.
In Japan, a study focusing on bereaved family members who provided care for cancer patients in palliative care units reported a depression prevalence of 13.6%. 3 The study reported that factors associated with depression included unpreparedness for death and the psychological burden experienced during caregiving.
A nationwide survey on home-based palliative care reported that 35% of family members supporting terminally ill patients experienced depressive mood. 4 This finding suggests that both the patient’s psychological symptoms and the caregiver’s own health status are contributing factors.
In Japan, the number of cancer patients wishing to spend their final days at home has recently increased, resulting in an annual increase in the home death rate. 5 This home-based care is primarily supported by a specialized system of home care clinics and hospitals, which are regulated to provide 24-hour, 7-day-a-week availability for emergency visits and end-of-life support. Within this clinical framework, “terminally ill” generally refers to patients with a life expectancy ranging from several weeks to approximately six months, for whom curative treatments are no longer feasible. These medical teams, typically comprising physicians and visiting nurses, coordinate care under the national Long-Term Care Insurance system to support both patients and their families in the domestic environment. While Japanese palliative care units (PCUs) serve as specialized inpatient facilities equivalent to inpatient hospices in other countries, home care focuses on providing equivalent specialized care at home. A study reported that the family caregiving burden in the home care setting is comparable to that in palliative care units. 6 However, the prevalence of probable depression among bereaved family members following care for a patient at home and the associated risk factors remain to be elucidated.
The aim of this study was to investigate the prevalence of probable depression among bereaved family members who cared for terminally ill cancer patients at home and identify associated factors.
Methods
This study analyzed data from the “COMparison of End-of-life trajectory in advanced cancer patient between inpatient HOspice and hoME; Multicenter cohort study on fundamental difference inpatient characteristics and influence of place of care” 7 (COME-HOME study), a multicenter observational study of home-based palliative care for advanced cancer patients. These data were combined with a self-administered questionnaire survey targeting bereaved family members.
The COME-HOME study was a prospective observational study that enrolled cancer patients who initiated home-based care between July 1 and December 31, 2017. The patient’s condition was recorded by attending physicians at the start of care and every three months thereafter. If a patient died at home, the circumstances of the death and the patient’s condition seven and three days before death were recorded retrospectively.
The questionnaire survey for bereaved families was conducted at participating facilities in the COME-HOME study that provided consent. The survey targeted all eligible bereaved family members of registered patients who met the criteria and died at home by September 30, 2018. Self-administered questionnaires were mailed to these families at least three months after the patient’s death.
Eligibility criteria included: (1) a bereaved family member (key person or guarantor for adult patients) of a patient who died at home, (2) patient age at death ≥18 years, and (3) bereaved family member age ≥18 years.
Exclusion criteria included: (1) inability to identify the bereaved family member; (2) treatment-related death or death in an ICU ward; (3) inability to complete the questionnaire due to medical conditions, such as dementia or mental disorder; (4) significant mental instability of the bereaved family member; or (5) judgment by the medical team that study participation was inappropriate because of strong dissatisfaction with the medical care or a severely strained relationship with the staff.
Assessment of depression: The questionnaire included the Japanese version of the Patient Health Questionnaire-9 (PHQ-9) 8 for depressive symptoms. The PHQ-9 is constructed based on diagnostic criteria for depression and has demonstrated superior discriminatory power compared with other screening scales. 9 Although the PHQ-9 is a screening tool rather than a diagnostic instrument, a total score of ≥ 10 was used as the cutoff to indicate probable depression, consistent with established criteria.
Measurements of associated factors: Physical and psychological conditions while providing care were assessed using the questions, “How was your physical condition while providing care?” and “How was your psychological condition while providing care?”, respectively. Participants responded on a 4-point Likert scale: “very good,” “fair,” “poor,” and “very poor.” For the statistical analysis, these were dichotomized into two groups: “good/fair” (comprising “very good” and “fair”) and “poor” (comprising “poor” and “very poor”).
Perceived social support was assessed using the question: “Is there someone around you who can listen to your concerns?” Participants responded using a 5-point scale: “extremely supportive,” “very supportive,” “supportive,” “not supportive,” and “not supportive at all.” These were categorized into three groups for analysis: “extremely/very supportive,” “supportive,” and “not supportive” (comprising “not supportive” and “not supportive at all”).
Preparedness for death was assessed using a single-item question: “Were you mentally prepared for the patient’s death?” Participants responded on a 4-point Likert scale: “well prepared,” “prepared,” “not prepared,” and “not prepared at all.” For the statistical analysis, these were dichotomized into two groups: “prepared” (comprising “well prepared” and “prepared”) and “unprepared” (comprising “not prepared” and “not prepared at all”).
Statistical analysis: First, univariate analyses were performed for patient-related and family-related factors to examine associations with depression in bereaved family members. Significance was defined as p < 0.05. Subsequently, multivariate logistic regression analysis was conducted. Explanatory variables included the age and sex of both the patient and bereaved family members, as well as factors identified as significant in the univariate analysis. Statistical analysis was performed using IBM SPSS Statistics version 29.0.2.
Results
The COME-HOME study was conducted at 45 medical institutions across Japan and enrolled 1,102 patients. During the observation period, 981 patients (89.1%) died, with 676 (68.9%) dying at home. Twenty facilities participated in the bereaved family survey. Questionnaires were sent to 357 eligible bereaved family members of 381 patients who died at home during the survey period at the facilities. Twenty-four were excluded for the following reasons: bereaved family members could not be identified (n = 7); bereaved family members were judged to be mentally unstable (n = 5); comprehensive judgment by the medical team that there was strong dissatisfaction with or misunderstanding of the medical care received (n = 5); and the patients had been excluded from the analytic cohort of the COME-HOME study (n = 7). Of the 357 individuals who were sent questionnaires, responses were obtained from 222 (62.2%). Of these, 195 individuals with evaluable PHQ-9 scores were included in the analysis (Fig. 1 and Table 1). The median time from the patient’s death to the bereavement survey was 1075.0 days (interquartile range [IQR]: 1027.5–1127.3 days; range: 841–1216 days).

Participation flow diagram.
Patient Characteristics
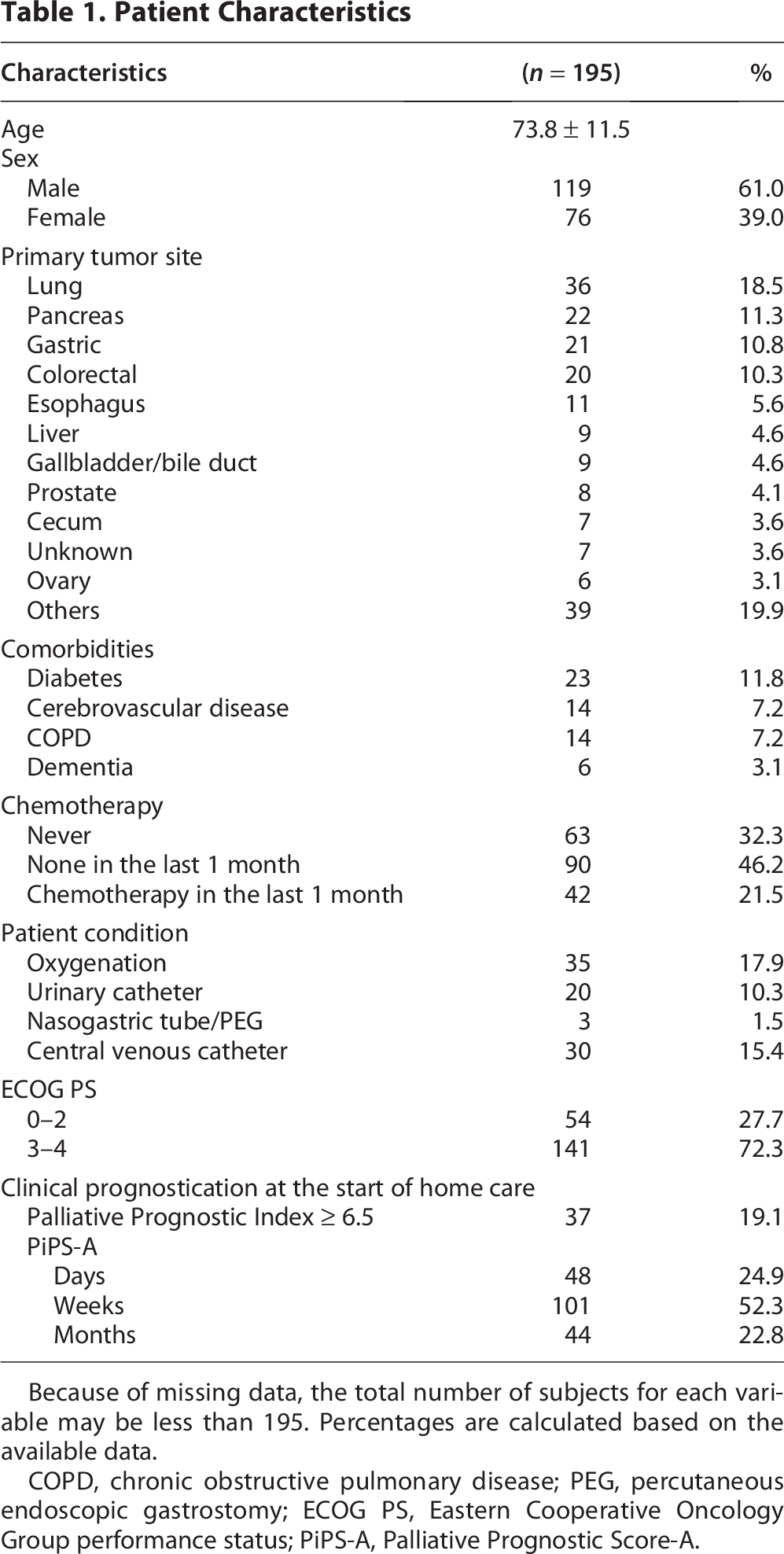
Because of missing data, the total number of subjects for each variable may be less than 195. Percentages are calculated based on the available data.
COPD, chronic obstructive pulmonary disease; PEG, percutaneous endoscopic gastrostomy; ECOG PS, Eastern Cooperative Oncology Group performance status; PiPS-A, Palliative Prognostic Score-A.
Twenty-three respondents screened positive for probable depression (11.8%). Table 2 shows the association between patient-related factors and depression in bereaved family members. Factors associated with depression included hyperactive delirium within 3 days before death, dyspnea within 1 week before death, antipsychotic use at the start of home care, and intermittent sedation.
Patient-Related Factors Associated with Depression in Bereaved Family Members

Because of missing data, the total number of subjects for each variable may be less than 195. Percentages are calculated based on the available data.
Table 3 shows the association between family-related factors and depression in bereaved family members. Factors associated with depression included being the spouse of the deceased, having a low household income, poor physical condition during caregiving, poor mental condition during caregiving, and unpreparedness for death.
Bereaved Caregiver Characteristics and Factors Associated with Depression

Because of missing data, the total number of subjects for each variable may be less than 195. Percentages are calculated based on the available data.
JPY, Japanese Yen
Table 4 shows the results of a logistic regression analysis that incorporated these factors as variables. “unpreparedness for death” (Odds ratio (OR): 11.0; 95% Confidence interval (CI): 2.8–43.8) exhibited the strongest association with depression in bereaved family members. Other associated factors included “poor physical condition during caregiving” (OR: 7.4; 95% CI: 1.4–39.2), “dyspnea within 1 week before death” (OR: 4.5; 95% CI: 1.3–15.6), and “antipsychotic use at the start of home care” (OR: 6.3; 95% CI: 1.2–32.2).
Logistic Regression Analysis

Discussion
This multicenter study investigated the prevalence of depression and associated factors among bereaved family members who cared for cancer patients at home until death. Probable depression was identified in approximately 12% of bereaved family members who provided home care.
This prevalence rate is slightly lower than the generally accepted range of 15% to 30% reported in the literature.3,10,11 Home care may facilitate a gradual acceptance of death through extended time spent with the patient and active engagement in caregiving. Nevertheless, the finding that approximately 12% of bereaved family members screened positive for probable depression underscores the continuous necessity of psychological support for bereaved family members during home care. Furthermore, the median time from the patient’s death to the survey was approximately 2.9 years (1075 days), which is considerably longer than in previous studies. This suggests that the observed prevalence reflects long-term, persistent depressive symptoms rather than temporary grief reactions immediately following bereavement.
The factor with the strongest association in this study was “unpreparedness for death”. Inadequate preparedness for death is linked to complicated and prolonged grief. 12 This result highlights the importance of communication during the terminal phase to foster understanding of the patient’s condition and encourage psychological preparation for loss. Because physician home visits are necessarily intermittent, it may be challenging to intervene with family members at the appropriate time. Accordingly, the daily involvement of visiting nurses may play a key role in delivering nurse-led interventions that support family members in achieving preparedness for death.
The prevalence of probable depression in our study (11.8%) was similar to that reported in a previous study of Japanese PCUs by Hatano et al. (13.6%). 7 While “unpreparedness for death” was the strongest predictor in both settings, its impact appeared substantially higher in the home care setting (OR 11.0) compared to the PCU setting (OR 4.5). This discrepancy suggests that the psychological impact of being mentally unprepared may be intensified at home, where family members are more directly involved in the patient’s end-of-life process. Furthermore, while Hatano et al. identified hyperactive delirium as a key patient-related factor, our findings highlighted dyspnea and the need for antipsychotics as significant associations. This may reflect the high levels of family distress and helplessness specific to witnessing respiratory distress in a home environment without 24-hour onsite medical presence. Additionally, the strong association with the caregiver’s own physical condition (OR 7.4) underscores the unique physical toll of home caregiving, which may be less prominent in institutional settings where professional nursing support is more readily available.
We found a significant association between depression and “poor physical condition during caregiving.” This finding suggests a need to address the physical aspects of caregiving burden. Visiting medical teams should continuously assess the health status of caregivers and, when appropriate, recommend the utilization of support services and respite care to mitigate psychological stress and potential social isolation. When caregiver burden becomes substantial, respite hospitalization may be worth considering within the framework of home-based care. In addition, when the patient’s remaining time is limited, sensitively sharing this information through a process of shared decision-making may help family members to anticipate the end of life and potentially facilitate broader involvement in caregiving, which may contribute to strengthening family support systems. 13
Regarding patient-related factors, the multivariable analysis showed that dyspnea within one week before death and antipsychotic use at the start of home care were significantly associated with probable depression, whereas hyperactive delirium was not. Dyspnea is a symptom that causes high levels of distress at the end of life, often leading to significant anxiety and feelings of helplessness in families.14,15 This finding suggests that effective management of dyspnea is necessary not only for the patient’s well-being but also for the psychological well-being of family members.
Furthermore, the association between antipsychotic use at the start of home care and probable depression may reflect underlying neuropsychiatric symptoms or overall clinical instability, rather than a direct effect of the medication itself. This suggests that an unstable mental state or significant symptom burden in the patient at the initiation of home care increases the psychological burden on bereaved family members. While hyperactive delirium was significant in the univariate analysis, its lack of independent association in the final model indicates that its impact may be mediated by other factors or better represented by the clinical need for antipsychotics.
Limitations
The limitations of this study are as follows: (1) Potential recall bias may be enhanced because the survey was conducted a median of approximately 2.9 years after the patient’s death; therefore, respondents’ perceptions of the patient’s symptoms and their own mental state during caregiving may have been influenced by the long time elapsed; (2) the possibility of characteristic differences between respondents and nonrespondents, given the 62.2% response rate; (3) the inability to infer causality due to the cross-sectional design. Specifically, several caregiver-related predictors, such as physical condition during caregiving, were assessed retrospectively. Therefore, it remains uncertain whether these factors preceded or co-occurred with probable depression. Future longitudinal and qualitative studies are needed to investigate the temporal aspects of psychological changes in bereaved family members; (4) the exclusion of family members who exhibited significant mental instability or those judged by the medical team to have strong dissatisfaction with medical care may have led to an underestimation of the prevalence of probable depression. These excluded individuals may have been at higher risk for psychological distress, and their exclusion could have introduced a selection bias; and (5) the relatively small number of participants who screened positive for probable depression (n = 23) may have led to overfitting in the multivariate logistic regression model. Although we selected explanatory variables based on univariate significance and pre-specified demographic factors to ensure comprehensive adjustment, the wide confidence intervals for some factors suggest potential instability in the estimates. Therefore, the results should be interpreted with caution, and further studies with larger sample sizes are warranted to confirm these associations.
Clinical Implications
This study investigated the prevalence of depression among bereaved family members providing home care and identified associated factors. Particularly, the strong associations between depression and “ unpreparedness for death “ and “the caregiver’s own health status” provide important practical implications for home visits and end-of-life care.
Conclusion
Approximately 12% of bereaved family members screened positive for probable depression after providing home care for cancer patients. Factors independently associated with probable depression included “unpreparedness for death,” “poor physical condition during caregiving,” “dyspnea within 1 week before death,” and “neuropsychiatric instability reflected by antipsychotic use at the start of home care.”
These results suggest that home palliative care teams should prioritize not only the management of physical symptoms, particularly dyspnea, but also providing comprehensive physical and psychological support to family members. Furthermore, facilitating clinical interactions that encourage mental preparation for the patient’s death is essential to reduce the risk of depressive symptoms in bereaved family members.
Authors’ Contributions
All the authors made substantial contributions to the conception and design of the work. All the authors facilitated the acquisition of data. T.M., J.H., and R.Y. conducted the statistical analyses. R.Y. and J.H. led the interpretation of data and drafted the work. T.M., J.H., and T.S. revised it critically. All the authors read and approved the final version of the article.
Ethical Considerations
The study protocol was approved by the Institutional Review Boards (IRBs) of all participating services. The main IRB (University of Tsukuba: No. 1153 and No. 1484) specifically approved the use of existing data for secondary analysis and their combination. This research was conducted in accordance with the Declaration of Helsinki (as revised in 2013). Informed consent was obtained in writing from all bereaved family members who completed the self-administered questionnaire.
Footnotes
Disclosure Statement
None of the authors have any financial or personal relationships to declare.
Funding Information
The COME-HOME study was supported in part by JSPS KAKENHI Grant Numbers 19K10551, 22H03305 and 25K02844. The sponsor played no role in the study design, collection, analysis, or interpretation of the data, writing of the report, or in the decision to submit the paper for publication.