
Abstract
This scoping review examines current empirical, peer-reviewed literature regarding the unhoused population and professionals who serve them, including what interventions have been tested so far. The study followed a PRISMA-ScR checklist protocol, conducting a systematic review sharply focused only on unhoused populations and palliative care-related needs. Of an initial screening of 157 articles, 79 were selected as part of the final review. Evidence of what is needed to support this population, and some promising interventions exist, but there remains a very limited number and scope. A substantial need is apparent for (1) expanded evaluation of interventions, (2) systematic assessment of cost implications, and (3) multi-site, interdisciplinary studies that link housing, health, and palliative care outcomes.
Introduction
Background and rationale
The general literature suggests that somewhere between 75,000 and 135,000 unhoused people in the United States have palliative or end-of-life needs. Most visible are unhoused older adults, but younger adults with advanced, symptomatic illness are included.1,2 Palliative care and end-of-life needs for unhoused individuals are a social problem that has persisted for hundreds of years. However, only within the past decade have we begun to understand the complexity of this significant social problem and promise palliative care interventions could have. This scoping review targeted studies examining prevalence and costs, needs, and interventions or programming in previous research on unhoused individuals who have needs for palliative care. The purpose of this scoping review is to describe a full landscape of the intersection of palliative care and end-of-life needs for unhoused individuals to assist researchers in determining foci for future research areas.
The financial and societal costs of “business-as-usual”
People who are unhoused have higher rates of serious illness and premature death than housed peers, and they often die in acute, crisis-driven settings with little symptom management or care that meets their wishes. This pattern produces avoidable and unreimbursed spending such as ambulances, 3 ED use, ICU days,4,5 and prolonged admissions. There is unnecessary harm including unmanaged pain, 6 community inequities, 7 deaths in public spaces with complicated circumstances or shelters, and moral distress for staff 8 that surround this social problem. Studies in general populations show that palliative and end-of-life care have the potential to reduce high-cost, low-value utilization. Emerging work with the unhoused shows potential for specialized models that can redirect care toward meeting end-of-life wishes while lowering total costs. Based on general average costs, if a city prevents just 20 individual end-stage crises from becoming an ambulance for a one-day ER visit that alone could potentially save $100k–$150k 9 before counting any avoided ICU days, repeated cycles, or the nonhealth costs, which can be in the millions of dollars for 20 individuals.
Objective
To complete a systematic scoping review of published literature on unhoused individuals facing serious life-limiting and/or terminal illness. The main purpose of the review is to examine current literature for what so far has been examined through empirical observation within this population including what interventions have been studied to address the problem. The results will guide future researchers and practitioners.
Design
The scoping review followed a PRISMA-ScR checklist, and the protocol was developed by the authors after examining prior reviews on the topic, examining gaps, partially documented in a white paper of the same topic. 10 The unique contribution of our scoping review is an accounting of all primary articles explicitly examining the intersection of homelessness, palliative or end-of-life care, and costs of care. This strategy allows for a broader scope of empirical research done to date. It includes reports on interventions and cost estimates but also reports on qualitative and quantitative studies.
Eligibility criteria and information sources
Databases searched for peer-reviewed empirical studies were Academic OneFile Plus, PsychINFO, PubMed, and Web of Science. The search was conducted using the Auraria Library database membership access. Inclusion criteria for sources included having at least one word from two lists, one indicating unhoused related populations and the other life-limiting illness. Search terms to identify unhoused included homeless, unhoused, housing insecure, homelessness, unstably housed, and affordable housing. Search terms to identify palliative and end-of-life include hospice, palliative, serious illness, life-limiting illness, terminal illness, serious health condition, serious health problems, or challenges. Additionally, articles must have been written in the English language and published as a peer-reviewed article between 1977 and 2025.
Data charting and data items
All articles and summaries of the studies were examined. Data were entered into an Excel spreadsheet, and additional aspects of the dataset were examined after each phase. An iterative process of three phases of review took place between the two researchers (authors). Studies examining costs related to unhoused individuals needing palliative or end-of-life care were also included. Six articles were excluded due to inaccessibility. These articles were unavailable via the Auraria Library Interlibrary Loan (ILLiad) program.
Results
Selection and characteristics of sources of evidence
The data charting process was iterative, using a series of Excel files to review an initial group of 157 articles. Once all duplicates were removed, the articles were examined for specific characteristics. Included articles reported information on unhoused or formerly unhoused individuals or professionals serving unhoused individuals as the unit of analysis. Additionally, articles must report on qualitative or quantitative approaches to an intervention, assessment or program. The final scoping review included 79 articles, including 11 review articles to provide transparency of the types of reviews done to date. Since the inclusion criteria for articles included publication in English, multiple countries are represented in the findings. The countries in which the studies detailed in the articles were performed were primarily in the United States (23), Canada (27), and the United Kingdom (32). Eight articles focused on studies in the Netherlands, and Australia, Brazil, India, and New Zealand had one article each.
Consideration of previous reviews
If excluding review articles, there are 68 primary articles. An examination of the 11 review articles revealed that 24 primary studies were identified as overlapping between articles cited within prior reviews and those identified through our scoping review, leaving 44 unique articles in our scoping review. All 11 review articles contributed at least one study that was independently identified in the original review, although the number of overlapping articles varied substantially by review. Review 11 (Rodericks-Schulwach, Gokani, & Martin) is the dominant contributor, citing nearly all (22 of 24) primary overlapping studies. An example of insight our review provides is that the Rodericks-Schulwach, Gokani, & Martin review only identified 8 interventions, while ours identified 18 (Table 1). Review 12 (James, Flemming, Hodson, et al.) contributes a secondary cluster of 11 overlapping articles in their review. Other reviews, e.g.,13,14 contribute only one or two overlapping articles.
Multiple countries were represented in the 266 review articles, primarily in the United States (127), Canada (55), and the United Kingdom (41), the Netherlands (10), Australia (5), Sweden (4), Republic of Ireland (3), and India (2). Seven articles focused on studies in China, Colombia, Ethiopia, Iran, Tunisia, Germany, and Korea one article each. Twelve articles did not specify country. Within the reviews,11,12,15–17 only seven articles among the reviews focused on unhoused veterans (see Table 2).
Interventions Impacting Palliative and End-of-Life Care for People Experiencing Homelessness
Articles Focused on Unhoused Veterans

Human subjects data collection
Most of the 68 primary articles (54) involved direct data collection with human participants, including individuals experiencing homelessness, service providers, or both.
Financial and resource costs
Evidence supports the idea that the unhoused population with serious health issues utilize acute care at high rates. Our review of articles, both within our review of 79 articles and those within the review studies (n = 117 unique primary articles), found that only three studies examined the financial costs associated with the lack of palliative care for unhoused individuals. Within the original review of 79 articles, only four focused on unhoused veterans.12,16–18
Results of Individual Sources of Evidence
Summary of article types
After reviewing all 79 selected articles, we categorized them into five distinct categories, (a) original intervention studies, (b) retrospective service evaluations and secondary data analysis, (c) scoping reviews, (d) systematic reviews, (e) distinction between original review and 11 review studies, and (f) an “other” category that consists of a variety of qualitative, quantitative, mixed methods, studies and policy analyses. The breakdown of categories is as follows:
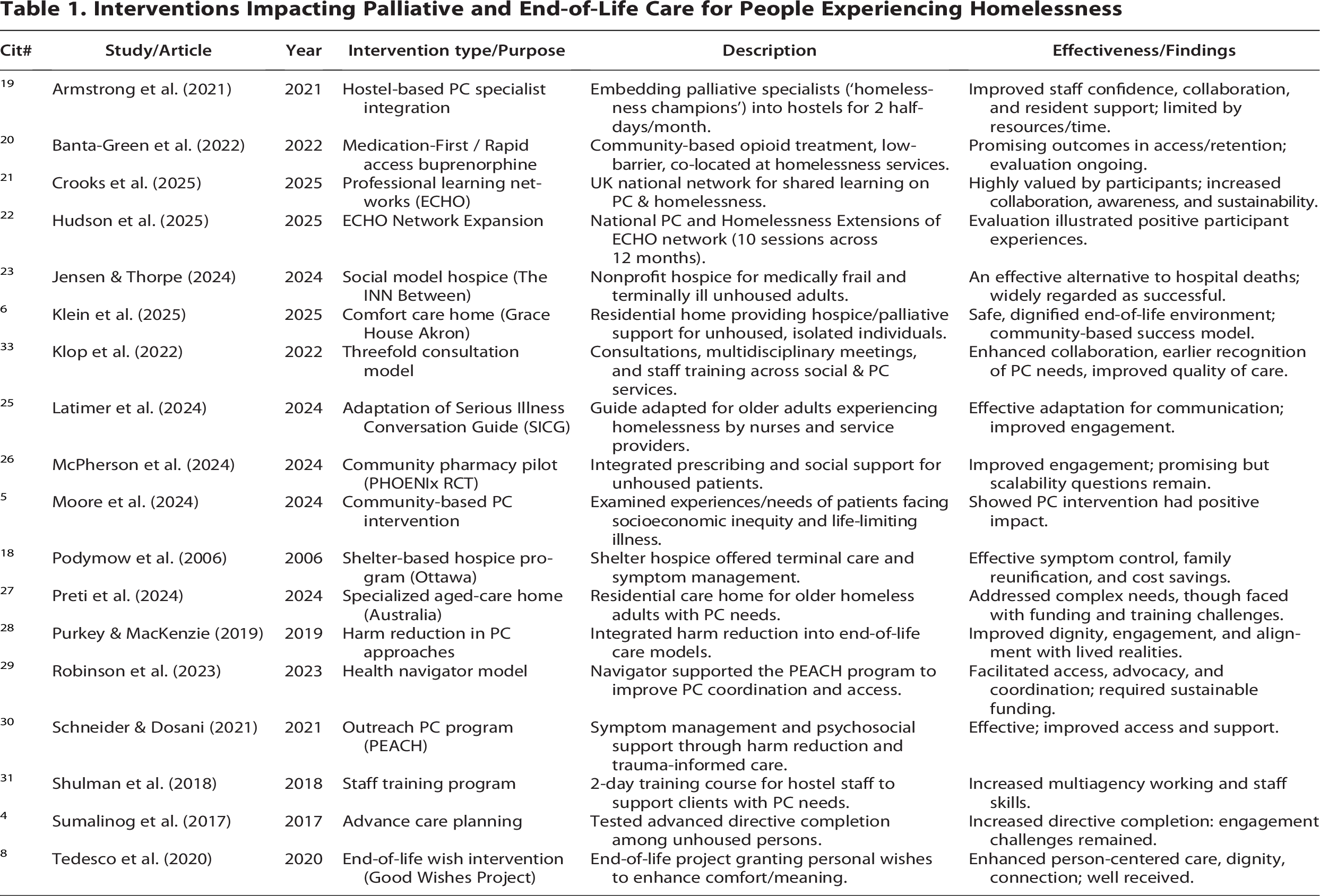
Eighteen original intervention studies4,–6,8,18,19–23,24–29,30,31 Retrospective service evaluations and secondary data analyses16,24,37,38,60,79,81–85 Review articles: Six scoping reviews11,12,14–16,32 and five systematic reviews4,13,17,33,34 Within the scoping and systematic review articles (c and d above), 24 primary articles overlapped with our review1,2,18,28,29,35,36,37,38,33,39,40–43,44–52 and Other (i.e., not an intervention/program, not retrospective service evaluations, and not secondary data analyses) (47 total)1,2,6,27,28,35,37,39–43,44–48,50–52,53,54–63,64,65–67,68–74,74,75–80
Critical appraisal of individual sources of evidence
This typology highlights a reliance on qualitative inquiry and literature synthesis, with fewer intervention studies testing new models of care. The trend in increased studies involving new original research with human subjects is promising and indicates a growing evidence base grounded in lived experience. However, significant gaps remain in quantitative outcomes research and longitudinal follow-up.
Synthesis of results
Five major themes emerged during the review process:
Barriers to Accessing Palliative and Health Services, Need for Training, Collaboration, and Networks, Complex Health and Social Needs, Innovative Community-Based Models, Centering Human Dignity, Autonomy, and Lived Experience,
Barriers to accessing palliative and health services
Stigma, discrimination, and assumptions about capacity continue to create barriers to access care. Structural barriers include uncompromising health systems, a deficiency of stable housing, and exclusion from typical palliative care models. Hostel staff and frontline providers often become “de facto” caregivers, highlighting gaps in formal service provision. Several studies emphasize that health disparities between housed and unhoused populations could be understood as a “cliff,” indicating abrupt and profound differences in morbidity, mortality, and access to care.
Need for training, collaboration, and networks
A recurrent theme is the necessity of targeted training, professional collaboration, and learning networks to support providers working with this population. Training hostel staff, fostering professional learning networks (e.g., UK ECHO initiatives), and building multi-professional partnerships are repeatedly emphasized. By engaging in providing these supports to staff, it addresses the isolation professionals can feel when working with this population, which can be isolated in and of itself. These efforts improve staff confidence, interagency collaboration, and early recognition of palliative needs. Cross-sector and multi-disciplinary involvement is seen as essential for sustainability and system-level change.
Complex health and social needs
People experiencing homelessness continue to present with high rates of multi-morbidity, frailty at younger ages, and co-occurring substance use and mental illness. Symptom burden extends beyond physical, encompassing psychosocial, existential, and spiritual suffering. As such, solutions to address these intersecting needs require multidisciplinary, flexible, and person-centered care approaches.
Innovative and community-based models of care
A substantial body of literature highlights innovative, community-rooted approaches that adapt palliative care to the realities of homelessness. Community and outreach-based interventions—including mobile palliative care teams, street medicine programs, harm reduction-oriented clinics, and health navigators—offer low-barrier entry points for unsheltered individuals. Many of these articles examined approaches such as hostel-based palliative specialists, harm-reduction approaches, social model hospices (e.g., The INN Between), comfort care homes (Grace House Akron), health navigators, and mobile outreach. Programs such as the PEACH model in Canada and Medication-First opioid treatment demonstrate that low-barrier, community-rooted interventions can increase engagement and dignity at the end-of-life.
Centering human dignity, autonomy, and lived experience
A cross-cutting theme throughout literature is the ethical imperative to center dignity, autonomy, and lived experience in palliative and end-of-life care for this population. Studies found highlight the value of trauma-informed, trust-building approaches that respect autonomy and recognize coping mechanisms. Co-production of research with people with lived experience is increasingly prioritized (e.g., TIFFIN recommendations), though still underutilized. Interventions like Good Wishes Projects and Death Cafés underscore the importance of honoring dignity, personal meaning, and opportunities for reflection at the end-of-life. Literature continues to support the pressing need to reduce systemic barriers, adapt care models, and embed dignity, autonomy, and collaboration into palliative services for people experiencing homelessness.
Interventions and promising approaches
Shelter and hostel-based models of palliative care approaches such as the Ottawa Inner City Health Project 18 demonstrated effective symptom management, family reunification, and cost savings. It was also reported that embedding palliative care specialists in hostels improved staff confidence, interprofessional collaboration, and access to external services.
The community and outreach-based interventions such as mobile and street medicine teams provide flexible, low-barrier access, especially for unsheltered adults. The use of health navigators enhances care coordination, addresses social determinants, and advocates for patients, showing promise in the Toronto PEACH program.29,30 Community-based clinics 20 provide harm reduction—oriented care and serve as gateways into health systems.
The specialized residential facilities such as social model hospices (e.g., The INN Between) 23 and comfort care homes (e.g., Grace House) 6 offer dignified, home-like environments for unhoused individuals at end-of-life. Or the specialized homes for older people in Australia 27 highlight the potential of tailored environments for older people experiencing homelessness. Several studies addressing needs in training and workforce development were also among the more relevant studies. For example, one training course for hostel and shelter staff in palliative care increased confidence and improved conceptualization of care needs. 31 Another example of multi-professional partnerships and ECHO networks expands shared learning and collaboration across providers.21,22
Advance care planning and psychosocial supports were also among the studies identified. Interventions such as advance directive programs and death cafés give voice to individuals’ wishes and address existential needs. 21 Another example, The Good Wishes Project personalizes end-of-life experiences, fostering dignity and connection. 8
Table 1 explains the details of interventions for readers to compare and review.
In summary, intervention categories with potential impact from this review include:
Shelter- and hostel-based palliative care models—feasible, cost-saving, and acceptable to patients and staff. Mobile and outreach teams—essential for unsheltered individuals. Health navigators and case management—improve coordination, advocacy, and access. Specialized facilities (social model hospices, comfort care homes, supportive housing with PC integration)—provide stability and dignity. Training, multi-professional partnerships, and trauma-informed approaches—address systemic barriers and workforce challenges.
Conclusions
Based on this scoping review, while a growth in the evidence base has occurred in the last decade, research on palliative care for unhoused individuals is still emerging, with significantly more contributions from descriptive and qualitative work than evaluative studies. Evidence of promising interventions exists, but a stark gap exists in the number and scope. Particularly, studies focused on unhoused veterans; the knowledge base is severely lacking for that important population. Scaling promising approaches, embedding trauma-informed and harm reduction principles, and enacting supportive policies are one approach to ensure equitable palliative care access. Housing itself can serve as a form of palliation, reinforcing the need for integrated housing and health care solutions.
Regarding practice, policy, and research recommendations, several exist on each level. Interdisciplinary practice teams trained in working with the unhoused could create more effective approaches when seriously ill unhoused individuals enter health care systems. Future policies can direct funding to this area of practice and programming as a means for cost savings in health care systems. Future research opportunities are abundant for this topic. While the diversity of strategies is a strength for future researchers to learn from, it is important to consider that studies were not concentrated in one country, and further scrutiny of what social policies in one country allowed approaches to be successful or supported is warranted. A close examination of qualitative literature to develop new creative interventions, as well as building on promising interventions and programs within this review, tested across multiple settings, is recommended.
In summary, evidence found in this scoping review reinforces the complexity of addressing palliative care needs for the unhoused population. Findings support a considerable need for (1) expanded evaluation of interventions that have shown promise (examples listed in intervention categories 1–4 above) and other creative interventions that incorporate training, multi-professional partnerships, and/or trauma-informed approaches (intervention category 5 above), (2) systematic assessment of cost implications, and (3) multi-site, interdisciplinary studies that link housing, health, and palliative care outcomes.
Limitations
This study is not without limitations. The library access was a barrier to using six articles that could have contributed. These articles’ titles and abstracts indicated four articles were qualitative, one was regarding an intervention covered in a different article found, and one was a review of outpatient primary care settings. There were also limited resources in terms of time and funding for graduate research assistants to examine articles. The fact that there is a lack of quantitative and longitudinal studies is a limitation in and of itself, so additional research is needed.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This project was not funded by an external source.