
Abstract
Background:
Black patients with cancer are less likely to receive supportive care than non-Hispanic White patients. Studies examining supportive care use patterns specifically among Black patients are limited.
Objectives:
To describe supportive care receipt and explore its sociodemographic, clinical, and communication-related correlates in Black patients with advanced lung cancer.
Design:
Observational exploratory pilot study.
Setting:
Black patients with advanced lung cancer (N = 30) were recruited from thoracic oncology clinics in the United States.
Measurements:
Participants self-reported sociodemographic, clinical, and communication-related factors. Supportive care receipt (palliative medicine, chaplain, or mental health services) was abstracted from electronic medical records. Point-biserial correlations or Fisher’s exact tests (as appropriate) assessed relationships between key variables and supportive care receipt. Significance was set at 0.05, and results were interpreted with caution due to the exploratory focus.
Results:
Only six participants (20%) received supportive care during the three-month study. Supportive care receipt was more common in participants who were younger (r = −0.48, p = 0.007, 95% CI: [−0.82, −0.14]) or had experienced medical discrimination in the past 2 years (50% v. 9%, Fisher’s exact test, odds ratio (OR) = 8.98, p = 0.03, 95% confidence interval CI: [1.25, 88.17]). Those with poorer general quality of life (QOL) (r = −0.41, p = 0.025, 95% CI: [−0.76, −0.06]) or poorer lung cancer-specific QOL (r = −0.55, p = 0.002, 95% CI: [−0.88, −0.23]) also had higher rates of supportive care receipt.
Conclusion:
Among Black patients with advanced lung cancer, supportive care receipt varied by sociodemographic, clinical, and communication-related factors, suggesting future research avenues.
Background
Despite higher symptom burden, Black patients with cancer are less likely to receive supportive care (e.g., palliative care, spiritual support, and mental health services) than non-Hispanic White patients.1–7 Factors underlying these disparities include differential access to supportive care, mistrust, discrimination, and cultural differences.8,9
Although disparities between racial groups in supportive care receipt are well-documented, less is known about patterns within the substantially heterogeneous Black community. 10 Factors affecting supportive care use in Black patients may or may not reflect findings from predominantly White samples. Accordingly, expert guidelines recommend prioritizing palliative care research among minoritized populations. 11 Determining factors associated with supportive care receipt among Black patients with cancer could inform tailored intervention approaches for increasing supportive care receipt specifically for this subgroup to reduce symptom management inequities.
Prior studies suggest factors affecting supportive care receipt. For example, palliative care use varies by gender, age, and socioeconomic status.12,13 Because supportive care is especially relevant for those with higher disease burden, complex comorbidities, and more severe symptoms,11,14,15 clinical factors may also play a role. In addition, patient-centered communication—prioritizing patient involvement and building patient-clinician relationships 16 —could promote symptom discussions, while communication barriers and prior experiences of discrimination in medical settings can complicate such discussions.9,17–20 Yet, supportive care studies often over-represent White patients 21 and rarely focus on minority health;21–23 thus, there is a need to determine factors linked to supportive care use among Black patients specifically.
Advanced lung cancer is a unique clinical context to examine supportive care receipt among Black patients. Lung cancer survivorship is growing, 24 yet 64% of patients have advanced disease at diagnosis. 25 Compared to other cancers, those with lung cancer experience higher symptom burden, greater distress, and quality of life (QOL) challenges.26,27 However, supportive care is underutilized in lung cancer care, especially among Black patients.2–4,28
In summary, supportive care services are critical components of advanced lung cancer care,11,14,29 but Black patients are less likely to receive them than non-Hispanic White patients despite higher symptom burden.1–5 Determining factors associated with supportive care receipt specifically among Black patients can guide intervention approaches. In this exploratory pilot study, we described rates of supportive care receipt in Black patients with advanced lung cancer and examined whether receipt varied by sociodemographic, clinical, and communication-related factors in order to inform future larger research studies.
Methods
This exploratory pilot study included patient surveys and electronic medical record (EMR) abstraction between March 2022 and May 2023. The Georgetown-MedStar Joint Oncology Institutional Review Board approved the study (Protocol #00004381).
Participants and procedures
As previously described, 30 study team members recruited participants (n = 30) from three thoracic oncology clinics, confirmed eligibility, and obtained written informed consent. Participants were ages ≥18, Black or African American, English-speaking, and receiving care for advanced (Stages III-IV; extensive) lung cancer. Patients receiving hospice care or demonstrating severe cognitive impairment were excluded.
Participants completed surveys at baseline (T0), following a routine oncology appointment (T1), and one month later (T2). Trained staff abstracted EMR data.
Measures
Based on the social-ecological model,31,32 shared decision-making frameworks,33,34 and prior literature, 35 we examined patient-level (sociodemographic and clinical characteristics) and interpersonal factors (patient–clinician communication factors) expected to potentially impact supportive care receipt.
Sociodemographic characteristics
At T0, participants reported their age, gender, education, employment status, insurance status, and involvement of a support person in their care (yes/no). Single-item questions assessed financial toxicity, health literacy, and religious coping.
Clinical characteristics
Because QOL challenges, anxiety, and depressive symptoms signal a need for supportive care, participants reported these factors at T0 Functional Assessment of Cancer Therapy-General 7-item version; (FACT-G7), 36 Functional Assessment of Cancer Therapy-Lung; (FACT-L), 37 Generalized Anxiety Disorder 2-item scale; (GAD-2), 38 Patient Health Questionnaire 2-item scale; PHQ-2 39 ) Upon examining their distributions, FACT-G7 and FACT-L scores were used as continuous variables, while GAD-2 and PHQ-2 scores were recoded into binary variables (representing any/no symptoms). Time since diagnosis, treatment(s) received, comorbidities, and performance status were abstracted from the EMR.
Communication variables
At T0, participants reported patient-oncologist relationship quality (The Human Connection scale 40 ). At T1, participants reported perceived shared decision-making in a routine oncology appointment (CollaboRATE scale 41 ). Because prior discrimination experiences may impact communication,18,42 participants reported experiences of discrimination in medical settings within the past two years based on race, language spoken, gender, age, appearance, smoking history, or lung cancer status (adapted from the Commonwealth Fund Health Quality Survey 43 ); responses were dichotomized as any/none.
Supportive care receipt
Trained research staff abstracted EMR data on supportive care receipt (palliative care, chaplain, or mental health services) between study enrollment and T2 (M = 78 days, SD = 50 days). Length of study enrollment was not significantly related to supportive care receipt (p = 0.14).
Statistical analysis
Analyses were conducted with IBM SPSS (v29) and R (v4.5.2, exact2x2 package). To identify areas of focus for future studies, we examined descriptives and bivariate relationships between supportive care receipt and sociodemographic, clinical, and communication-related variables using point-biserial correlations and Fisher’s exact tests with corresponding 95% confidence intervals, 44 as appropriate. All tests were two-tailed; significance was set at α ≤ 0.05. Due to the exploratory nature of the study and multiple statistical comparisons, we interpreted analyses with extreme caution.
Results
Sample descriptives
Table 1 summarizes participant characteristics by supportive care receipt.
Participant Sociodemographic, Clinical, and Communication-Related Characteristics, by Receipt of Supportive Care Services
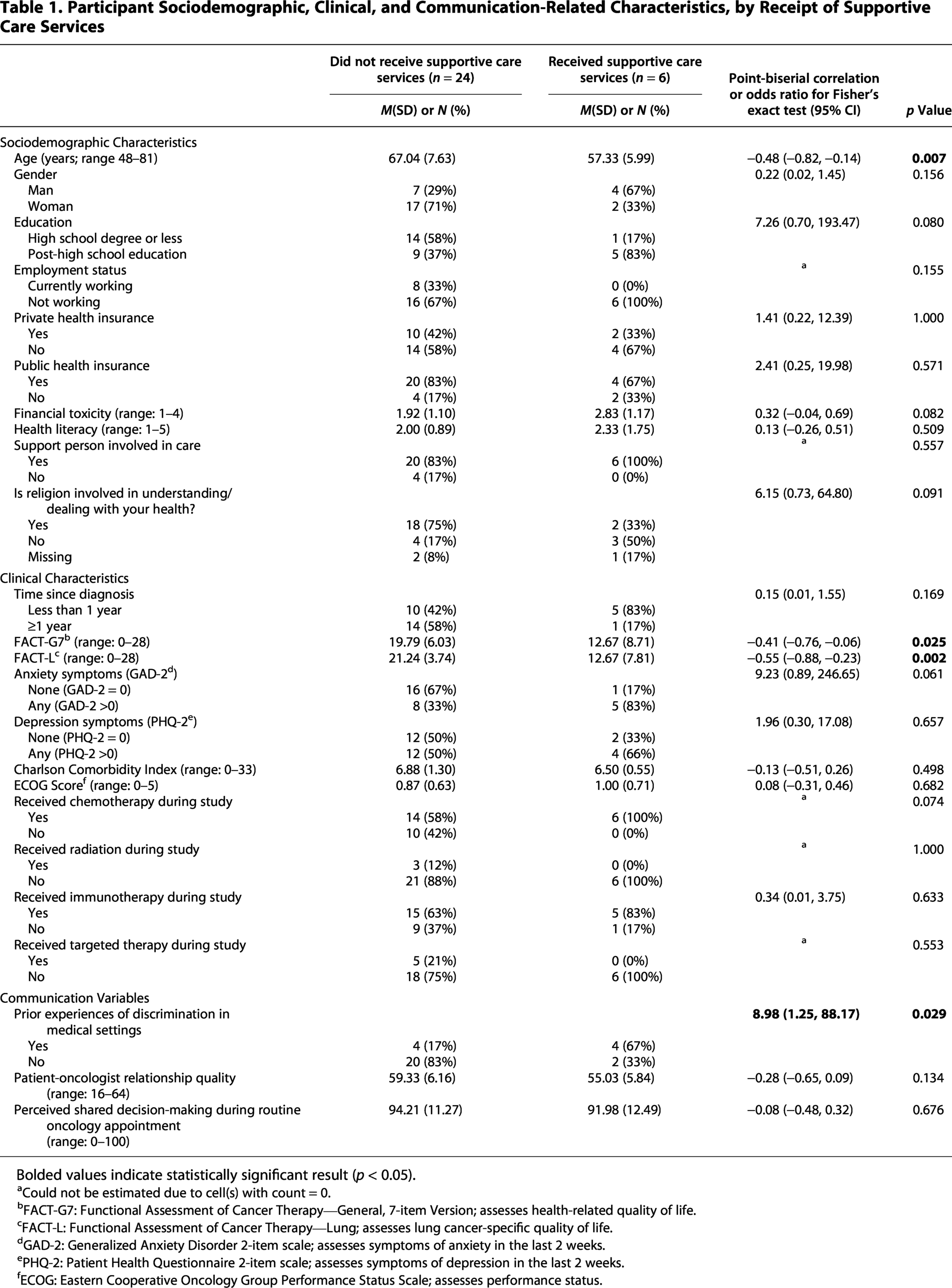
Bolded values indicate statistically significant result (p < 0.05).
Could not be estimated due to cell(s) with count = 0.
FACT-G7: Functional Assessment of Cancer Therapy—General, 7-item Version; assesses health-related quality of life.
FACT-L: Functional Assessment of Cancer Therapy—Lung; assesses lung cancer-specific quality of life.
GAD-2: Generalized Anxiety Disorder 2-item scale; assesses symptoms of anxiety in the last 2 weeks.
PHQ-2: Patient Health Questionnaire 2-item scale; assesses symptoms of depression in the last 2 weeks.
ECOG: Eastern Cooperative Oncology Group Performance Status Scale; assesses performance status.
Frequency of supportive care receipt
Six participants (20%) received supportive care services during the study (Table 2); some received multiple services.
Receipt of Supportive Care Services

Factors related to supportive care receipt
Sociodemographic characteristics
Younger participants received supportive care services more frequently than older participants (r = −0.48, p = 0.007, 95% CI: [−0.82, −0.14], Fig. 1A). Supportive care receipt was not significantly associated with other sociodemographic characteristics (p-values ≥ 0.08; Table 1).

Boxplots demonstrating receipt of supportive care services by
Clinical characteristics
Supportive care receipt was higher among participants with poorer general QOL (r = −0.41, p = 0.025, 95% CI: [−0.76, −0.06], Fig. 1B) and poorer lung-cancer specific QOL (r = −0.55, p = 0.002, 95% CI: [−0.88, −0.23], Fig. 1C). Supportive care receipt was not significantly associated with other clinical characteristics (p-values ≥ 0.06; Table 1).
Communication variables
Participants who experienced prior medical discrimination had higher rates of supportive care receipt compared to those without these experiences (50% vs. 9%; Fisher’s exact test; OR = 8.98, p = 0.03, 95% CI: [1.25, 88.17]; Fig. 2). Supportive care receipt was not significantly associated with other communication factors (p-values > 0.13; Table 1).

Proportion of participants reporting prior experiences of discrimination in medical settings by receipt of supportive care services.
Discussion
Despite disparities in supportive care use,1–5 little is known about factors associated with its receipt specifically among Black patients. We explored supportive care receipt among Black patients with advanced lung cancer. Consistent with prior literature,45,46 only 20% of participants received supportive care. Those who were younger, previously experienced medical discrimination, and had worse QOL were more likely to receive supportive care. These exploratory results offer pathways for future research.
While they must be interpreted with extreme caution, these findings can inform future clinical and research efforts to identify those who may be less likely to receive yet still benefit from supportive care. For example, older adults received supportive care at lower rates than younger patients. Older Black adults may benefit from tailored interventions promoting supportive care. 47 In contrast, patients experiencing worse QOL were more likely to receive supportive care, which aligns with clinical guidelines. 11 However, we could not determine the timing of supportive care relative to symptom onset, an area for future work given the benefits of early palliative care integration.29,48 Furthermore, those with lower symptom burden may still benefit from supportive care. 14
Interestingly, those who experienced prior medical discrimination were more likely to receive supportive care, an unexpected finding. It is possible that people with prior discrimination experiences may have higher symptom burden, self-advocate more in clinical visits, and/or prompt different referral patterns from clinicians.18,49 Future work examining links between communication and supportive care receipt in larger samples is needed.
Strengths and limitations
Study strengths include its focus on Black patients and multidimensional data from participant reports and EMRs. However, due to the exploratory nature of the study, the small convenience sample precluded adjusted analyses, restricted statistical power to detecting large effect sizes, and limited generalizability to the broader population of Black patients with advanced lung cancer (e.g., those of various ancestries, those treated in community settings). As expected due to the study’s exploratory nature, post-hoc power analysis indicated that the study was underpowered to detect small and medium effects; additional relationships may be revealed in larger studies. Because we studied supportive care use specifically in Black patients to understand their experiences, 50 we cannot draw conclusions about whether these findings are unique to Black patients. Multi-method studies examining supportive care receipt prospectively from diagnosis and including clinician factors (which influence referral patterns 51 ) are needed.
Conclusion
Only 20% of Black patients with advanced lung cancer received supportive care services during this three-month exploratory pilot study. Exploratory findings indicated that those who were younger, experienced prior medical discrimination, and had worse QOL had higher rates of supportive care receipt. Future research should explore these relationships prospectively in larger samples to confirm findings and inform interventions promoting supportive care receipt.
Authors’ Contributions
Conceptualization: All authors. Methodology: H.M.D.-V. and C.C.C. Funding acquisition: H.M.D.-V., C.K., and C.C.C. Supervision: H.M.D.-V. and C.C.C. Project administration: A.K., J.D.R., H.M.D.-V., and C.C.C. Formal analysis: A.K., C.C.C. Investigation: A.K., J.D.R., O.M.B., J.D.R., H.K., E.T., and A.S. Resources: C.K., I.V., J.W., and M.G. Data curation: A.K. and C.C.C. Visualization: A.K. and C.C.C. Writing—original draft: H.M.D.-V., A.K., B.M., O.M.B., and C.C.C. Writing—review and editing: All authors.
Footnotes
Acknowledgments
The study team expresses their appreciation to the patients who participated in this study, to the members of the Project TLC Community Advisory Board, to Dr. Lora Kasselman and Dr. Valeriy Korostyshevskiy for statistical consultation, and to Dr. Lisa Carter-Bawa for feedback on the draft manuscript.
Data Availability Statement
Author Disclosure Statement
C.C.C. has received grant funding from Pfizer. M.G. has received consulting fees from Guardant, honoraria for speakers bureau activity from BMS and Merck MSD, and stock in COTA Healthcare. C.K. has received consulting fees from Daiichi Sankyo, Regeneron, Sanofi, Takeda, J&J, Pinetree, Boehringer Ingelheim, BMS, Bicycle, Bayer, Onviv, Bio-Thera, and his institution has received research funding from AstraZeneca, Novartis, Regeneron, Janssen, Genentech, Lyell, Daiichi Sankyo, Gilead, Macrogenics, Boehringer Ingelheim, Black Diamond Therapeutics, ORIC. All other authors have no conflicts of interest to disclose.
Funding Information
This research was supported by a Developmental Funds Award from the Lombardi Comprehensive Cancer Center (LCCC) Cancer Center Support Grant (P30CA051008; PI: Weiner) and by the National Cancer Institute (T32CA261787, PI: O’Neill; K08CA270402, PI: Conley). This research was also supported by the LCCC Survey, Recruitment, and Biospecimen Collection Shared Resource (SRBSR), which is partially supported by NIH/NCI grant P30CA051008 (PI: Weiner).