
Abstract
Background:
Documentation of goals of care (GOC) discussions is a critical aspect of caring for individuals with serious illness. In this study, we evaluated the use of a standardized GOC template across three Canadian health care sites, utilizing both quantitative and exploratory qualitative approaches to determine whether the template was associated with more comprehensive documentation.
Methods:
This was a multisite retrospective study. The frequency of documentation of each component of a GOC discussion was compared between notes that used the template and those that did not using chi-square (χ2) tests. The potential association between the characteristics of patients (age, sex, primary diagnosis) and the use of the template was determined using a multivariate binary logistic regression analysis. Semi-structured interviews and focus groups with key informants were conducted as part of an exploratory descriptive qualitative analysis.
Results:
The GOC template was used to document conversations 50% of the time, while in the remaining 50% of charts, the template was deleted and replaced with a narrative note. Compared to narrative notes, GOC conversations documented within the template were statistically more likely to provide comprehensive documentation. The odds of the GOC template being used were not associated with the age, sex, or primary diagnosis of the patient. The pilot qualitative analysis highlighted themes of utility and usability.
Conclusion:
Uptake of a standardized GOC template at our institution was strongly associated with more complete GOC documentation. Although the template went through a participatory design process, the current study reveals significant deficits in both utility and usability.
Keywords
Background
Facilitating goals of care (GOC) discussions is a critical aspect of caring for individuals with serious illness. Exploring GOC is a complex process that involves communication between care providers, patients, and substitute decision makers, with the goal of ensuring that medical treatments are aligned with patients’ preferences.1,2 Beyond focusing exclusively on specific medical life support interventions, high-quality GOC discussions include an exploration of personal values and belief systems, and how these inform decision making. 2 In Canada, many provincial health policies advocate for a shared decision-making model in which clinicians collaborate with patients, substitute decision makers, and families to develop and document a care plan that is based on the identified GOC. 3
Thorough documentation of GOC is often regarded as a marker of good quality clinical care, although consensus on outcome measures is lacking. 4 GOC documentation can facilitate communication among multiple care providers within a patient’s circle of care, and support care coordination and planning. 5 Absent or incomplete GOC documentation may lead to adverse outcomes, in particular the provision of unwanted medical interventions that may result in avoidable physical and emotional trauma to individuals, families, and health care providers.6,7
Very few studies explore how GOC are documented, and most of these studies are limited to exploring resuscitation status only. 8 A recent study 9 explored the accuracy of GOC documentation in electronic medical records (EMRs). The authors noted that in the absence of a structured approach, important components, such as end-of-life preferences, were often incompletely documented. There is some evidence indicating that standardized documentation templates encourage thoroughness and efficiency of documentation 9 and documentation templates have been developed to support competencies in advanced communication skills.8,10 Previous studies found that problem-oriented templates were associated with improved note quality without significant change in charting time. 11 Therefore, understanding how GOC documentation supports communication best practices represents an important opportunity in advancing goal-concordant care.
A recent study 12 describes the successful implementation of a GOC note template for medical oncologists, including an association between early use of the GOC template and end-of-life outcomes, including fewer days admitted to acute care, lower likelihood of receiving chemotherapy in the last 14 days of life, and increased hospice referral. A prospective study 10 at a Canadian academic hospital explored completion rates of a “Goals of Care Discussion Form” for individuals admitted to a general medicine service. Although completion rates (63%) were higher than expected, authors noted that less than two-thirds of completed forms were uploaded into the hospital EMR. Both of these were single-site studies that engaged only a single medical service. In addition, they did not examine whether template usage was associated with more comprehensive GOC documentation and did not include qualitative components to learn the perspectives of end-users. The primary objective of our study was to evaluate the use of a GOC template across three health care sites and to determine whether template usage was associated with more comprehensive documentation. The secondary objective was to learn the perspectives of health care providers using the template.
Methods
Design, setting, and participants
This was a retrospective cohort study conducted across three affiliated but distinct hospital sites in Toronto, Canada. While the three sites function under one corporate entity, each varies in its primary scope of practice. The main hospital is a 250-bed tertiary level acute care hospital, the second site is a 60-bed orthopedic and rehabilitation hospital, and the third site is a 60-bed reactivation center dedicated to convalescent and long-term care.
A locally developed GOC template 13 was implemented into the hospital-wide EMR in 2022. Prior to implementation, content modifications were made (Supplementary Appendix A1) to the original template in order to meet the needs of our health system. The GOC template underwent a rigorous participatory design process at our institution, including beta testing, with broad stakeholder engagement. The goal was to develop a “standardized” product that could be used by clinicians from different medical disciplines, each serving patients with life-limiting illness. An online video guide for completing the GOC template was launched to support users. The website hosting the video does not monitor the number of views. Simulated communication workshops led by palliative care physicians were implemented to support communication skills development among hospital staff. Prior to study onset, a total of 117 staff members completed the simulation workshop, including staff and trainee physicians, nurse practitioners, and allied health professionals. Baseline data monitoring indicated that in 2022, there were 1721 GOC notes documented across all three sites, representing 5.1% of all new EMR notes created during that time period.
The resulting GOC documentation template (Supplementary Appendix A1) implemented across all three sites at our institution included a number of content domains (Table 1). Template completion required users to complete tick-boxes as well as populate free-text or narrative fields related to specific content domains.
Core Content Domains and Required Input Types within the Standardized Goals of Care Documentation Template

Legend: Each domain represents a required component of the structured GOC note. “Narrative” indicates free-text entry fields; “Tick-box” refers to checklist selections to ensure completeness and consistency.
CPR, cardiopulmonary resuscitation; GOC, goals of care.
Chart review
We conducted a retrospective chart review of notes documented under a dedicated “Goals of Care” note-type in the hospital EMR across all three sites. The first 100 consecutive GOC notes of 2023 (January 1–January 17) in hospitalized individuals were extracted from the hospital EMR. We chose a sampling period that began six months after the GOC note was initially introduced into the EMR (June 2022). Each GOC note was reviewed to determine (1) was the template used to document the conversation?; (2) if the template was used, what specific documentation elements (Table 1) were completed or left blank?, (3) if the template was not used, did the narrative GOC note include each of the specific conversation elements found in the template? Patient age, gender, and primary diagnosis were collected.
Two specialist palliative care physicians and three hospitalist physicians independently reviewed the patient charts. Each chart was reviewed by a single physician. Each of the five physicians, with a mean of 10 years in clinical practice, routinely cares for patients with advanced illness and is experienced in conducting GOC conversations. Prior to review, a scoring template was developed by the authors to systematically capture each domain of the GOC template (Table 1). The authors reviewed EMR notes to determine if the template was used or deleted, and captured which specific elements of the template or narrative notes were documented. If the template was deleted in favor of a narrative GOC note, authors reviewed the documentation to determine what specific elements of the conversation were captured. The first 10 GOC notes were reviewed jointly by the study authors to ensure the reliability of data interpretation and collection. The remaining notes were evaluated independently, with frequent discussion among the authors to clarify uncertainties and minimize inconsistency in scoring.
Key informant interviews
A semi-structured interview guide (Supplementary Appendix A2) was developed through discussion and consensus-building by the study team. The interview guide was not pilot-tested.
The evaluation used a convenience sample limited to ten informants who were representative of services that use the GOC note type, including Internal Medicine, Palliative Care, and Critical Care medicine. The sample size was deemed large enough to represent diverse perspectives and was feasible within the parameters of the exploratory study. Informants were chosen purposefully from the three medical services described above, with the intent of including both junior and senior clinicians. None of the informants were involved in developing or implementing the GOC template. Given that the study authors and informants work clinically in the same institution, all participants had pre-existing professional relationships with the interviewers. Participants were initially approached via email, which included an informed consent form with a description of the study goals. All agreed to participate and completed the study.
Two semi-structured interviews (n = 2) and two focus groups (n = 8) were conducted. One focus group was conducted with two palliative care physician participants, and a second focus group was conducted with six internal medicine staff and trainees. One interview was conducted with a critical care physician, and the second interview was conducted with a nurse practitioner. This was a small exploratory study with no access to a research assistant to conduct interviews and focus groups. Interviews and focus groups were conducted in the workplace and lasted approximately 40 minutes. Both focus groups were conducted in person, while both interviews were conducted virtually. Conversations were audio-recorded, and field notes were taken during and after each interview. Data were not returned to participants for comment or correction. Transcripts were verified by the principal investigator.
Analysis
Characteristics of patients and of GOC documentation were analyzed descriptively using counts and percentages. The frequency of documentation of each component of GOC was compared between notes that used the template and those that did not using χ2 tests. Finally, the potential association between the characteristics of patients (age, sex, primary diagnosis) and the use of the template was determined using a multivariate binary logistic regression analysis. In the regression analysis, missing data were handled using complete case analysis, considering that there were only 2 missing values in the entire dataset. Degrees of freedom in the logistic regression did not exceed 10% of the number of patients with the outcome. 14 Statistical analysis was performed using SAS Studio (Cary, NC, USA). STROBE guidelines were used for reporting of quantitative data.
Qualitative analysis was undertaken through the lens of an exploratory pilot study. All of the interview and focus group data were manually coded independently by the first author using descriptive analysis. Themes were derived from the data using a framework analysis. 15 Codes and categories were developed by considering each line, phrase or paragraph of the transcripts in an attempt to summarize what informants were describing. Key phrases were summarized using participants’ own words into in vivo codes. The codes from each interview or focus group were compared to identify similarities and differences. Each in vivo code initially formed a potential category, but as coding progressed, they were grouped together into broader themes. Data analysis was reviewed and validated among the wider research team.
Ethics considerations
The study was approved by the Sunnybrook Health Sciences Research Ethics Board (project identification number 6626).
Results
Chart review
100 GOC notes were extracted from the health system EMR. A total of 84 inpatient GOC notes were included, with 16 outpatient notes excluded from analysis. The median age of patients (Table 2) with a GOC note was 79.5 (IQR = 65–94) years. There were similar numbers of females (46/84, 55%) and males (38/84, 45%). The majority (67/84, 80%) of patients had a noncancer diagnosis, while patients with a primary oncologic diagnosis constituted 20% (17/84) of GOC notes.
Demographic and Clinical Characteristics of Patients with Documented Goals of Care Notes (n = 84)

Legend: Data presented as n (%) unless otherwise noted. Cancer subtypes and noncancer conditions illustrate diagnostic diversity.
IQR, interquartile range.
Among the 84 inpatient charts reviewed, the GOC template was used to document conversations 50% (42/84) of the time (Table 3). In the remaining 50% (42/84) of charts, the template was deleted by the clinician and replaced with a narrative note. The length of narrative notes varied from one sentence to several paragraphs. The 42 template notes were created by 23 unique clinicians (15 staff and 8 learners), while the 42 narrative notes were created by 28 unique clinicians (12 staff and 16 learners).
Utilization of the Goals of Care Template Across Sites, Services, and Clinician
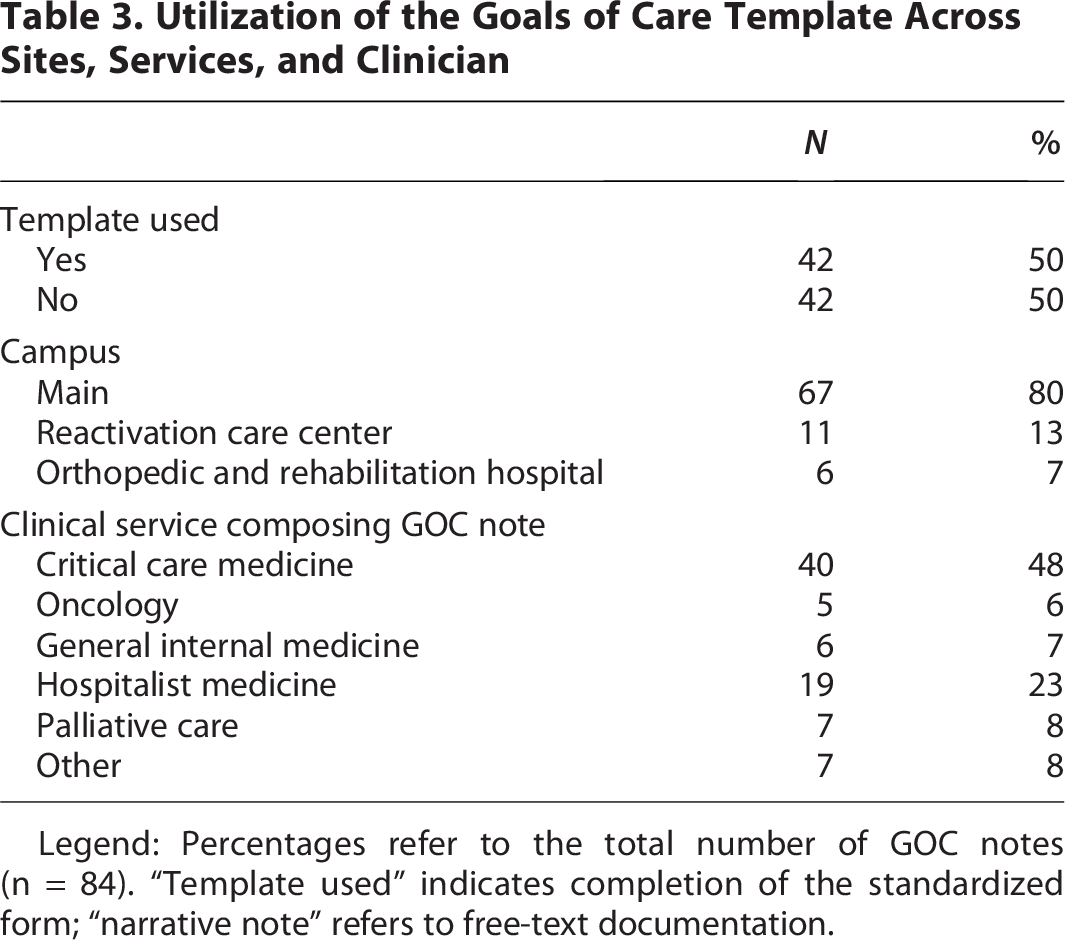
Legend: Percentages refer to the total number of GOC notes (n = 84). “Template used” indicates completion of the standardized form; “narrative note” refers to free-text documentation.
The majority (67/84, 80%) of GOC notes were documented for patient’s admitted to the hospital’s main campus. The clinician groups documenting the most GOC notes were Critical Care Medicine (40/84, 48%), Hospitalist Medicine (19/84, 22%), and Palliative Care (7/84, 8%). The majority of GOC notes were completed by either staff or trainee physicians (72/84, 86%), with 12 (14%) notes completed by nurse practitioners.
Variation in the completeness of GOC documentation (Table 4) was observed between notes using the template versus narrative formats.
Comparison of Documentation Completeness Between Template-Based and Narrative Goals of Care Notes

Legend: χ² tests used to compare proportions.
p < 0.05 considered statistically significant.
The logistic regression analysis was not statistically significant (likelihood ratio of χ2 = 1.43, p = 0.70; Table 5). That is, the odds of the GOC template being used was not associated with the age (OR = 0.98; 95% CI = 0.94–1.02), sex (OR = 0.81; 95% CI = 0.34–1.94), or primary diagnosis (OR = 1.37; 95% CI = 0.45, 4.17) of the patient.
Multivariate Logistic Regression of Patient-Level Factors Associated with Use of the Goals of Care Template

Legend: Model adjusted for age, sex, and primary diagnosis (cancer vs. noncancer).
CI, confidence interval; OR, odds ratio; SE, standard error.
Key informant interviews
Two semi-structured interviews and two focus groups were conducted with a total of ten participants, including two palliative care physicians, one critical care physician, one nurse practitioner, and six internal medicine physicians. While all interviewees were familiar with the standardized GOC template, none were aware of the online video and supplementary resources intended to support professional development for users of the template. The researchers identified two main themes from the interviews and focus groups: utility and usability (Table 6).
Thematic Summary of Clinicians’ Experiences with the Goals of Care Documentation Template: Utility and Usability Perspectives

Themes derived through framework analysis. Participant identifiers in brackets correspond to transcripts. Quotes illustrate representative experiences.
Discussion
Our study examined the uptake of a structured GOC documentation template in multiple inpatient settings. Critical Care, Hospitalist Medicine, and Palliative Care were the services that most commonly documented GOC at our institution. Clinician uptake of the standardized template was only moderate. Fifty percent of GOC notes utilized the documentation template while in 50% the template was deleted by clinicians in favor of writing free-form narrative notes. GOC were documented less frequently outside of the acute care setting, which may be reflective of the relative clinical stability of patients cared for outside of the main hospital campus in orthopedic and reactivation settings. We did not evaluate if patients at satellite sites had previous GOC documented while in the acute care setting.
Compared to narrative notes, GOC conversations documented within the template format were statistically more likely to document the patient’s capacity to participate in the discussion, the substitute decision maker, patient and family’s illness understanding, patient’s values and goals, code status and life support decisions, and preferred place of death. Our evaluation results are consistent with the findings of previous studies8,12 that found usage of a template resulted in higher documentation rates of patients’ goals and values when compared to free-form notes. However, our results may be applicable to a broader patient population given the inclusion of both cancer and noncancer diagnoses. A recent randomized study of hospitalized older adults with serious illness 16 demonstrated that implementation of a GOC communication guide was associated with significantly improved GOC documentation. However, it remains unclear if the quality of documentation is indicative of the quality of the GOC conversation, and ultimately, if it is associated with the provision of goal-concordant care.
Regression analysis revealed that patient age, sex, or primary diagnosis were not associated with completion of the GOC template. These results are reassuring in that they suggest that completeness of documentation does not seem to be dependent on patient-level factors. Whereas Curtis et al. 16 demonstrated a greater effect size of GOC documentation in patients from racial or ethnic minorities, we did not have access to race or ethnicity-based data in our current study. Our preliminary qualitative findings suggest that important drivers of usage may be related to users’ perceived expertise conducting GOC conversations and human factors limitations of the template.
Our exploratory descriptive analysis of users’ experiences with the template revealed themes of utility and usability. All 10 informants regarded themselves as experts in facilitating GOC conversations, such that the utility of the template in their own practices was low. Informants perceived the template to be better suited to trainees and those clinicians with limited competence in facilitating and documenting GOC discussions. Palliative care clinicians did not complete the template to elevate the quality of their clinical documentation, but rather to flag a patient’s code status to the broader clinical team. One staff clinician relayed:
“I’ve used it about a quarter of the time, more for documenting code status that may be helpful for ICU.”
Participants described the template as having poor usability, namely that it failed to accurately capture the iterative nature of GOC conversations. Given that the template is static and not a living document, many informants expressed dissatisfaction with the redundancy of completing the entire template each time they revisited GOC discussions. A critical care physician commented:
“I would have to complete the template multiple times to reflect the iterative nature of the GOC conversations I have.”
The Technology Acceptance Model (TAM) 17 is one model for addressing factors affecting users’ acceptance of novel technical systems, including how user acceptance is affected by the design features of the system. A recent systematic review of TAM 18 in health informatics concluded that clinical users are likely to accept a new technology, mainly if they recognize it as a tool to improve their work performance and build efficacy. This finding is consistent with the themes of limited utility and usability contributing to poor uptake at our institution. Specifically, future iterations of the GOC template must be perceived to add value to clinicians’ practices rather than posing barriers to an efficient workflow. Poor usability of EMRs has been associated with clinician stress, frustration, and burnout.19,20 Prior to implementing future versions of the template, using a “concurrent think-aloud” 21 approach may help to minimize human factor irritants. Another option for usability testing includes “near live clinical simulation,” 22 which is intended to mimic a real clinical encounter and may elicit key barriers and facilitators to provider workflow and adoption. 21
Limitations
Strengths of our study include its multiple methods design as well as the inclusion of both cancer and noncancer diagnoses. Limitations include a small sample size as well as possible selection bias given that cases were chosen consecutively rather than randomly. While the study evaluated the completeness of GOC notes, it did not explore the quality of documentation. The qualitative analysis was implemented as a pilot study and therefore lacked some elements of analytic rigor. For example, thematic analysis was limited to manual coding by a single investigator. The qualitative evaluation introduced investigator bias, given that study investigators conducted the interviews and focus groups. Informant responses may have been influenced by social desirability bias, given that evaluators had pre-existing professional relationships with informants. Future qualitative study will employ an objective interviewer.
Although the qualitative data analysis was exploratory, it will serve as a pilot for future evaluation.
Conclusion
Uptake of the GOC template was 50% over the study period, and its usage was strongly associated with more complete GOC documentation. Template usage was not associated with patient-level factors such as age, diagnosis, or sex. Although the template went through a participatory design process, the current study reveals significant deficits in both utility and usability. Usability evaluation should be employed prior to implementing future iterations of the GOC template. Future areas of interest may include a more robust qualitative study of low-propensity users and clinician trainees.
Authors’ Contributions
A.C. contributed to study design, data collection and analysis, interpretation of results, and was the lead writer of the article. M.B. contributed to data analysis and interpretation of results and was a major contributor in writing the article. V.B., S.T., and C.Z. contributed to study design, data collection and analysis, and interpretation of results. All the authors read and approved the final article.
Footnotes
Acknowledgments
The authors thank Ms. Ingrid Wirsig and Ms. Tania Johannsen for their thoughtful reviews of the article.
Author Disclosure Statement
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding Information
There are no sources of funding to declare.
Consent to Participate
Verbal informed consent was obtained from all study participants.
Availability of Data and Materials
The datasets used and analyzed during the current study are available from the corresponding author on reasonable request.
Supplemental Material
Abbreviations
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.