
Abstract
Background:
Patients with cirrhosis who suffer cardiac arrest often undergo cardiopulmonary resuscitation (CPR). However, there is limited data on the effectiveness of CPR in achieving survival or liver transplantation in this population. This study aimed to describe rates of survival after CPR, liver transplantation, and palliative care utilization for hospitalized patients with cirrhosis.
Methods:
Hospitalized patients with International Classification of Diseases 10th revision codes for cardiac arrest and cirrhosis from October 2017 to December 2022 were included. Patients were excluded if CPR was not performed or if diagnoses were incorrectly coded. Primary outcome was post-CPR survival. Secondary outcomes included rates of transplantation and specialty palliative care utilization. Cox regression models and the log-rank test were used to compare survival in those with and without decompensated cirrhosis.
Results:
A total of 126 patients were included; 88 had decompensated cirrhosis and 38 had compensated cirrhosis. Overall median survival was < 1 day. Thirty-day survival for compensated and decompensated cirrhosis was 39% and 7.9%, respectively (p < 0.001). Decompensation was associated with a 2.5-fold increased risk of death within 30 days (95% CI: 1.6–3.0). Two patients reached transplant evaluation and were activated on the transplant wait-list. Specialty palliative care consultation occurred in 25 patients, with most occurring after the CPR event.
Discussion:
This study demonstrates that post-CPR trajectory differs with presence or absence of hepatic decompensation. Ability to reach liver transplant evaluation after CPR in patients with decompensated cirrhosis is significantly limited by poor survival. Further study is needed to inform goals of care discussions and implementation of primary and specialty palliative care in this population.
Key Message
Presence of decompensation significantly affects survival and trajectory after CPR in patients with cirrhosis. Palliative care utilization remains low in this population.
Introduction
Cirrhosis is a progressive disease with complications from liver dysfunction and portal hypertension. Once patients develop decompensated disease—characterized by hepatic encephalopathy (HE), ascites, jaundice, or variceal bleeding—prognosis drops significantly. 1 Patients with decompensated disease, often termed end-stage liver disease (ESLD), are at increased risk of multiorgan dysfunction, morbidity, and mortality. Therefore, there has been increasing impetus to evaluate the role of hospice and palliative medicine in this population, which led to publication of the first guidelines for palliative care management of patients with decompensated disease in 2022. 2 However, these guidelines along with multiple other publications note important gaps in knowledge and broad implementation of palliative care principles in this population; one important deficit is in advance care planning.2–4
Educated and evidence-based discussions on advanced care planning are limited, at least in part, by the dearth of cardiopulmonary resuscitation (CPR) outcomes data in patients with cirrhosis. Only a few prior studies have evaluated CPR in patients with ESLD. These largely population-based studies have found that patients with cirrhosis comprise a significant portion, up to 10%, of in-hospital CPR recipients.5–8 Moreover, these patients tend to have less chance of survival and less ability to discharge home compared with patients without ESLD. 5 The conversation surrounding code status and decision to pursue CPR becomes more complicated given the hope of reaching curative liver transplantation. To our knowledge, only two small retrospective studies have described outcomes of CPR as it relates to reaching liver transplant surgery (though no study has specifically described rates of transplant committee evaluation after CPR).9,10 Only two studies have evaluated palliative care utilization rates in this specific cohort of patients.8,9
In this study, we aim to describe a single transplant center’s experience on CPR survival outcomes in patients with cirrhosis. We secondarily aim to describe rates of transplant evaluation and surgery, as well as specialty palliative care utilization rates in this population.
Methods
We performed a retrospective chart review of all patients admitted to a tertiary referral transplant center from October 2017 to December 2022 who had International Classification of Diseases 10th revision (ICD-10) codes for both cirrhosis and cardiac arrest. Manual chart review was subsequently performed by three researchers to confirm diagnosis of cirrhosis by biopsy, elastography, and/or imaging findings. Exclusion criteria included: < 18 years of age, absence of cirrhosis by above criteria, CPR not performed, absence of medical data to define severity or history of liver disease, or history of liver transplantation prior to CPR event.
We collected data on demographics, medical comorbidities, liver-related variables (e.g., etiology of cirrhosis, hepatic decompensations, and status of transplant evaluation: deferred, declined, listed), admission diagnosis, cardiac arrest event details (e.g., location of cardiac arrest, initial arrest rhythm), most recent Model for End Stage Liver Disease-Sodium (MELD-Na) score prior to cardiac arrest, and post CPR course (e.g., survival status, transplant evaluation and decision, rates of palliative care utilization, and discharge location). Palliative care utilization was defined as either specialty palliative care consultation or hospice enrollment.
Cox regression models and the log-rank test were used to compare survival between those with compensated and decompensated cirrhosis.
All research was conducted in accordance with both the Declarations of Helsinki and Istanbul; all research was approved by the appropriate ethics and/or institutional review committee, and given methodology of study, it received a waiver of informed consent.
Results
Study population and baseline characteristics
A total of 247 distinct records were obtained on initial database ICD-10 query. Of those, 121 records were removed as they did not meet inclusion and exclusion criteria upon manual chart review. Therefore, a total of 126 patients were included in the study, of which 38 had compensated disease, and 88 had decompensated disease (Table 1). Most patients were male (65%) and Caucasian (87%) with a median age at time of CPR of 60 years. Median body mass index (BMI) was 31 kg/m2 and 44 patients (35%) met American Heart Association criteria for metabolic syndrome. Though individual comorbidities were not statistically different between the two groups, combination of any coronary artery disease (CAD), heart failure, chronic obstructive pulmonary disease (COPD), or chronic kidney disease (CKD)/end-stage renal disease (ESRD) were more common in patients with compensated disease than in decompensated disease (p < 0.01). A summary of this data is seen in Table 1.
Baseline Cirrhosis Demographics and Comorbid Conditions

CAD, coronary artery disease; CKD, chronic kidney disease; COPD, chronic obstructive pulmonary disease; ESRD, end-stage renal disease; n, number, percent is provided in parentheses.
Liver disease etiology and disease severity are described in Table 2. Most common etiologies of cirrhosis were metabolic dysfunction-associated steatohepatitis and alcohol associated liver disease, found in 40 patients (32%) and 38 patients (30%), respectively, with an additional 5 patients (4%) meeting criteria for combination of metabolic dysfunction and alcohol associated liver disease. The remainder of patients had hepatitis C (18%), followed by cryptogenic etiology of cirrhosis (12%), cardiac cirrhosis (7%), and genetic or autoimmune etiologies (<3%).
Liver Disease Etiology and Model for End-Stage Liver Disease Score

A1AT Alpha-1 antitrypsin; MASH, metabolic dysfunction associated steatohepatitis; MASLD, metabolic dysfunction associated steatotic liver disease; MELD, model for end-stage liver disease; n, number, percent provided in parentheses.
Compensated cirrhosis was present in 38 patients (30%), while 88 patients (70%) had decompensated disease. Of those patients with decompensated cirrhosis, ascites was the most common decompensation, present in 85 patients (97%), followed by HE in 38 patients (43%) and esophageal variceal hemorrhage in 14 patients (16%). Of the entire patient cohort, the most recent MELD-Na score prior to arrest was > 20 in 80 patients (63%) and > 30 in 42 patients (33%). Nineteen patients (15%) had prior transplant committee evaluation at our center—nine had been declined, four had been deferred, and six patients were waitlisted for transplant at the time of arrest. Prior to cardiac arrest and CPR event, 48 (55%) of all decompensated patients in the study were considered “not current candidate for transplant” either through formal decline by the transplant selection committee (9 patients) or documentation in the electronic medical record by the primary inpatient hepatology team (39 patients). A summary of this data is seen in Table 2.
Admission and CPR event
Admission and CPR event details are described in Table 3. Cardiac arrest was documented as an admission diagnosis in 36 patients (29%). Of the 90 patients who had in-hospital cardiac arrest, the most common admission diagnoses were acute kidney injury/hepatorenal syndrome, HE, infection, and ascites. Forty-one (33%) episodes of in-hospital cardiac arrest occurred in the intensive care unit while 49 (39%) occurred either on a floor unit or stepdown unit. Initial arrest rhythm was documented in all patients and found to be shockable in only 21 (17%) of all cases.
Cardiopulmonary Resuscitation Event Details and Primary Admission Diagnosis

AKI, acute kidney injury; CPR, cardiopulmonary resuscitation; LT, liver transplant; n, number, percent provided in parentheses; PEA, pulseless electrical activity; VT, ventricular tachycardia; Vfib, ventricular fibrillation.
Survival and transplantation outcomes
Survival outcomes are described in Table 4 and Figure 1. Median survival was < 1 day with overall 30-day survival of 17%. Patients with decompensated disease had worse 30-day survival of 7.9% compared with 39% in those with compensated disease (p < 0.001). Of all patients included, 52 (41%) died at arrest, 48 (38%) were transitioned to comfort-focused care or hospice, 10 patients (8%) were discharged to inpatient rehab or skilled nursing facility, and 15 patients (12%) were discharged home with or without home health. After adjusting for age, BMI, CAD, HF, CKD, and COPD, hepatic decompensation was associated with a 2.5-fold increased risk of death within 30 days (95% CI: 1.6–4.0).
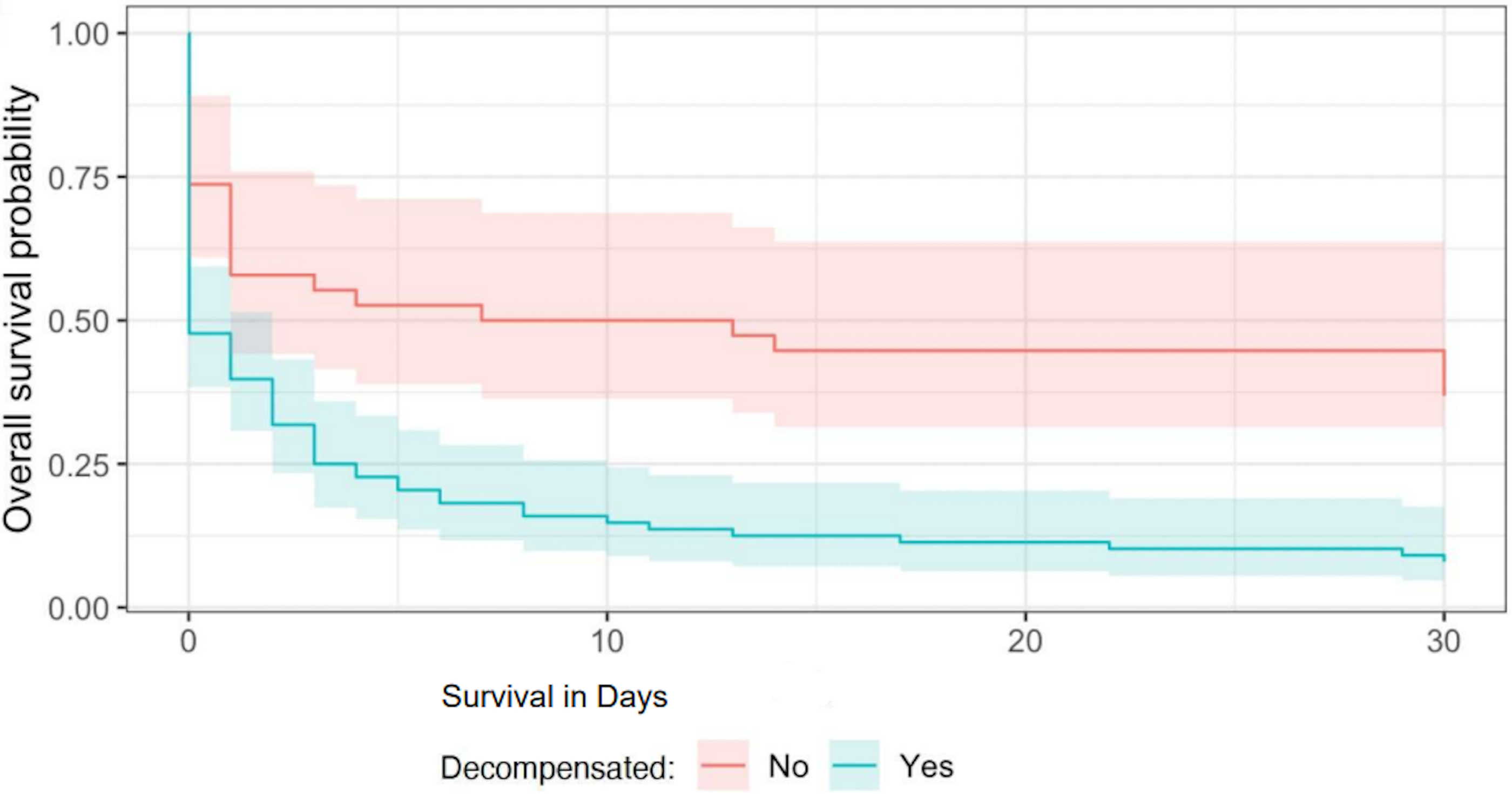
Thirty-day survival curves for compensated and decompensated cirrhosis after cardiopulmonary resuscitation. Median survival was < 1 day with overall 30-day survival of 17%. Patients with decompensated disease had worse 30-day survival of 7.9% compared with 39% in those with compensated disease (p < 0.001).
Cardiopulmonary Resuscitation Outcomes, Disposition, and Palliative Care Consultation

CPR, cardiopulmonary resuscitation; IPR, inpatient rehab; n, number, percentage provided in parentheses; SNF, skilled nursing facility.
Among the seven patients who had decompensated disease and survived > seven days, one patient was lost to follow-up and six patients were evaluated by the liver transplant selection committee after cardiac arrest. Of those evaluated, four were declined, and two were reactivated (as they had been listed prior to CPR event) and underwent liver transplantation within one-year follow-up.
Palliative care utilization
Prior to cardiac arrest, specialty palliative care consultation had occurred in nine patients (7%). After cardiac arrest, specialty palliative care consultation or hospice service initiation subsequently occurred in an additional 16 patients (13%) prior to discharge.
Discussion
In this study, we describe CPR outcomes in patients with cirrhosis at a single tertiary referral transplant center. We found that CPR is only successful 7.9% of the time in reaching 30-day survival in patients with decompensated cirrhosis compared with 39% of compensated patients. This is particularly notable, given that compensated patients in our cohort had significantly more comorbidities than decompensated patients. We found CPR was similarly unsuccessful at reaching liver transplant evaluation and transplant surgery, with only 2% of patients with decompensated cirrhosis reaching transplantation within one year of the CPR event.
Few other studies have evaluated in-hospital CPR outcomes in cirrhosis.5,6 In a large retrospective study, Ufere et al. used the National Inpatient Sample from 2006 to 2014 and found that 11% of ESLD patients survived to discharge after in-hospital CPR compared with 16% of those with metastatic cancer and 29% of those without ESLD. 5 These outcomes were more notable given that patients with ESLD were younger and had fewer comorbidities. A separate national registry study from Seoul University Hospital evaluated patient outcomes in out-of-hospital cardiac arrest and found that cirrhosis was associated with worse neurological recovery and survival to discharge compared with those without cirrhosis. 11 Smaller single-center retrospective studies have similarly found poor in-hospital post-CPR survival and neurological outcomes in patients with cirrhosis.7,10,12 Short-term survival post-CPR (e.g., 28-day survival, survival to discharge) in these studies ranged 10%–15%. In these studies, factors associated with poorer outcomes were higher MELD (>20) and Child–Pugh class C disease.7,9,10 Our findings are consistent with these prior studies. Particularly, we found that CPR in those patients with decompensated disease was similar to that found by Ufere and colleagues, whereas patients with compensated disease had similar survival to the non-ESLD patients.
To our knowledge only two retrospective studies have evaluated an outcome of reaching liver transplantation surgery.9,10 Roedl et al. included 47 patients with cirrhosis who underwent successful CPR, most of which (74%) had alcohol associated liver disease. Child–Pugh class C disease was associated with a 0% 28-day survival, and no patients in their study reached liver transplantation at one year follow-up. In a separate retrospective study, Stotts et al. evaluated 38 patients with ESLD and cardiac arrest and found that only 6 (16%) reached hospital discharge, and two reached listing for liver transplantation. Our study showed that only 2 of 88 patients (2.3%) with decompensated disease reached liver transplantation at one year follow-up of CPR event.
We should note that, though the transplantation rate was low, it should be contextualized to the patient population. For decompensated patients, rate was low primarily due to dismal 30-day survival of 7.9%. Of the seven decompensated patients that survived 30 days, one was lost to follow-up and six were evaluated by committee with two eventually reaching transplant. Interestingly, both of these patients were already listed prior to CPR event and subsequently reactivated after acute illness resolved. In contrast, the four patients who had their first transplant evaluation occurring after CPR were declined for transplant. For compensated patients, no transplantation evaluation occurred as would be expected.
Only two studies have described palliative care utilization rates in patients with cirrhosis undergoing CPR, with the most robust data coming from Dr. Margot Manning and Zachary Fricker.8,9 They performed a retrospective study of hospitalized patients with cirrhosis who underwent CPR. Their study included 96 patients with similar baseline characteristics to our population: 81% decompensated, Median MELD 28 and with 30-day survival of 21%. They found a similar 13.4% rate of specialty palliative care consultation with about half of those coming after the CPR event.
Though one may expect that the rate of palliative care consultation would be higher and the timing of consultation to be earlier for patients with decompensated cirrhosis, we should take caution in interpreting the meaning of this finding. Currently, there are no specific medical criteria for inpatient palliative care consultation for this patient population. Moreover, the decision to implement specialty palliative care consultation can rely on the complex dynamic of hospital system culture and provider teams’ training and comfort in providing primary palliative care interventions. Multiple barriers to palliative care implementation and documentation in both the inpatient and outpatient settings have been proposed and are under further study. 3
Moreover, though palliative care consultation has been shown to improve goals of care documentation and in specific populations is associated with change of code status from full code to “Do Not Resuscitate” (DNR), specialty palliative care consultation rate should not be used as the only metric to verify goals of care discussion. 13 In our study, of the patients who did not die at arrest, 66% were transitioned to comfort-focused care or hospice; presumably, some degree of a goals of care conversation was had in those patients despite only 13% of all patients receiving palliative care consultation. Even so, we show at the very least, the transition in goals of care occurs late in disease course with majority of palliative care or hospice referrals occurring after a cardiac arrest event or close to death.
Our findings have several limitations in addition to the inherent limitation and bias of a single-center, retrospective, unblinded descriptive study. A randomized prospective analysis of CPR outcomes was not possible. Our patient population was limited to those with ICD codes for cirrhosis and cardiac arrest, and thus, we may not have captured all patients who effectively had these two conditions but with different coding. Additionally, our patient population was predominantly white patients, which limits generalizability of this data. Survival data for our patient population was limited to those patients who remained within our single-center system; therefore, it is possible that those patients for which we did not have death-data and thus presumed to be alive have suffered progression of disease and death, causing us to overestimate survival. By the same token, it is possible that our transplantation outcome is underestimated, as those patients who survived may have reached transplant evaluation or surgery in seeking care elsewhere. However, the degree of under- or over-estimation of these outcomes is suspected to be low, given that it would come from the only 8% of decompensated patients that survived to 30 days. An obvious though important cohort of patients not covered by our study includes those patients that had previously selected to be DNR; thus survival, transplant, and palliative care utilization outcomes should only be compared with those patients that were full code and thus underwent CPR.
CPR is a commonly performed procedure in critically ill patients; however, its effectiveness on providing survival and a window for transplantation is not well-established in patients with cirrhosis. This potential window of transplantation has been shown to be important in health care providers’ ability to provide confident code status discussions with patients and families. 8 Despite the limitations of our study, our results highlight several important features of this patient population’s experience undergoing CPR. It underscores the difference in trajectory for patients with compensated versus decompensated disease undergoing CPR, reinforcing similar findings from recent studies. It contributes to a significant gap of knowledge being the largest study describing rate of transplant evaluation and transplant surgery for patients with cirrhosis undergoing CPR. Lastly, our study describes late utilization of inpatient palliative care consultation in decompensated patients undergoing CPR. We hope that our findings help further inform patient-centered discussions on the role of CPR in patients with cirrhosis.
Authors’ Contributions
C.R.T.: Conceptualization, methodology, software, investigation, resources, data curation, writing—original draft, review, and editing, visualization, and project administration. K.B.: Investigation and data curation. A.J.D.W.: Investigation and data curation. X.J.: Data curation, validation, formal analysis, and resources. J.C.S.: Data curation, validation, formal analysis, resources, and supervision. H.P.K.: Methodology, writing—original draft, review, and editing, visualization, project administration, and supervision.
Footnotes
Acknowledgments
Assistance with the study: none other than the others already written above.
Funding Information
None.
Disclosure Statement
Nothing to report.