
Abstract
Background:
Medical Assistance in Dying (MAiD) and palliative care are often portrayed as oppositional practices due to the belief that the former hastens death while the latter focuses on life-affirming approaches to symptom management. As Canada’s MAiD program expands, the shared focus on end-of-life care raises the question of whether this divide in provision should proceed or if integration of MAiD with palliative care is possible from the perspective of clinicians.
Objective:
The objective of this study is to explore Ontario palliative care physicians’ perspectives on the potential integration of MAiD within palliative care services.
Design:
This study utilizes a qualitative descriptive study design.
Setting/Subjects:
Seventeen palliative care physicians practicing across Ontario were interviewed from February to May 2025. Six abstained from involvement with MAiD, seven acted as assessors and providers, and four acted as assessors only.
Measurement:
Virtual semi-structured interviews and thematic analysis to identify dominant patterns and beliefs.
Results:
Our data analysis spanned four main themes: (1) ethical interpretations of the act of MAiD as determinants of inclusion or exclusion, (2) integration versus separation of MAiD and palliative care, (3) MAiD as patient-centered care, and (4) potential negative consequences of MAiD integration.
Conclusion:
Participants offered varying opinions on the ethical appropriateness of offering MAiD through palliative care, yet all acknowledged the importance of respect for patient choice and provision of a full range of medical treatments for high-quality patient care. Findings highlight the need for nuanced policy and supportive professional environments as palliative care clinicians navigate this ethically complex terrain.
Key Message
Palliative care physicians hold diverging perspectives about integrating MAiD within their clinical scope, which are shaped by ethical and practical considerations. Despite differences in opinion, a shared commitment exists in working toward coordinated care. Our findings highlight the need for nuanced policies and institutional supports to promote comprehensive end-of-life care.
Introduction
Palliative care physicians serve an essential role in supporting individuals at the end-of-life, often engaging in practices that aim to uphold patient autonomy and relieve distressing symptoms, such as pain management, withdrawal of life-sustaining treatment (WLT), and palliative sedation. Increasingly, palliative care physicians are also navigating requests for medical assistance in dying (hereafter referred to as MAiD). 1 The role of palliative care physicians in discussing and providing MAiD for patients is contested.2–4 MAiD and palliative care are often depicted as oppositional practices with distinctive goals across both academic literature and social commentary.5–7 According to the Canadian Hospice Palliative Care Association, the former hastens death, while the latter “intends neither to hasten nor postpone death.” 8
The legalization of MAiD in Canada following the 2016 Carter versus Canada decision and subsequent passage of Bill C-14 brought forth the question of the relationship between MAiD and palliative care.8,9 There is no standard model guiding this relationship; some Canadian hospitals offer MAiD independently of palliative care services, while others integrate MAiD within the provisional scope of palliative care.10–12 Much of the ongoing debate has taken place in political, legal, and bioethical spheres, with emphasis on questions of philosophical compatibility between practices.2,13,14 However, these debates often fail to systematically engage with the perspectives of frontline clinicians who participate in one or both practices. The goal of this study is to articulate the beliefs of palliative care physicians about alignment of MAiD with their medical practices to foster a balanced discourse concerning the appropriate provisional scope of palliative care services.
Methods
Study design
Our study applied a qualitative descriptive methodology. 15 This approach is suitable for the exploration of palliative care physicians’ ethical and professional experiences navigating the interface of palliative care and MAiD by engaging in a low-inference interpretation of the data to ensure that highlighted perspectives remain true to participants’ own words. 15 The University of Waterloo Research Ethics Board (REB #45975) approved this study.
Participants and recruitment
Physicians were recruited across Ontario by approaching existing network contacts and through a recruitment advertisement published in the Ontario Medical Association’s monthly palliative medicine email newsletter. Purposive snowball sampling was then used to ensure the study sample represented the diversity of perspectives on the relationship between MAiD and palliative care. Inclusion criteria were physicians with experience in palliative and end-of-life care, including the provision of MAiD, palliative sedation, and/or WLT.
Data collection
Data collection occurred between February and May 2025. Data pertaining to participant characteristics were collected via a Qualtrics survey. The interview guide was codeveloped through discussion between A.S. and M.M. with the goal of eliciting participant opinions about whether MAiD should be integrated with palliative care and potential challenges that may arise (see the Supplemental File for the interview guide). Semi-structured interviews were led by M.M. and co-facilitated on an alternating basis by A.B. and E.M., ranging in length from 45 to 90 minutes. All interviews were conducted online via Microsoft Teams. Written and verbal consent were obtained for audio-recording. Automated transcriptions were generated through Microsoft Teams and were subsequently cleaned and anonymized by A.B.
Data sufficiency was validated by the theory of informational power. 16 We anticipated a smaller sample size due to the specific goals of this study, the distinctive nature of participant experiences, and the extensive and rich variety of participant discussions. Furthermore, as this study was not guided by a particular theoretical framework, data collection was terminated when significant repetitions in key ideas occurred among participants.
Data analysis
Interview transcriptions were coded and thematically analyzed 17 using NVivo (v15). Two analysts (M.M. and A.B.) independently reviewed themes, and areas of convergence and divergence were discussed until consensus was reached. A reflexive journal was maintained by M.M. throughout the data collection process to document personal reactions to participant experiences. Through documentation of preconceptions and potential biases, the research team sought to validate the trustworthiness of the data interpretation.18–20
Results
We conducted 17 interviews with palliative care physicians. Eleven were MAiD-involved physicians (seven assessed and provided MAiD, four exclusively assessed), and six abstained from MAiD. Eight physicians viewed MAiD as already part of palliative care’s provisional scope (MAiD-inclusionists), while the remaining nine found them to be distinctive practices (MAiD-exclusionists). Primary medical specialties represented included family medicine and internal medicine (e.g., oncology), with the majority of participants (82%) dedicating over 75% of their clinical practice to palliative care. All physicians resided in the province of Ontario, and all but one participant practiced medicine in urban locations (see Table 1 for a full representation of demographic characteristics and Table 2 for descriptions of themes and full-text participant quotations).
Demographic Characteristics of Participants (n = 17)

Description of Themes and Illustrative Participant Quotations
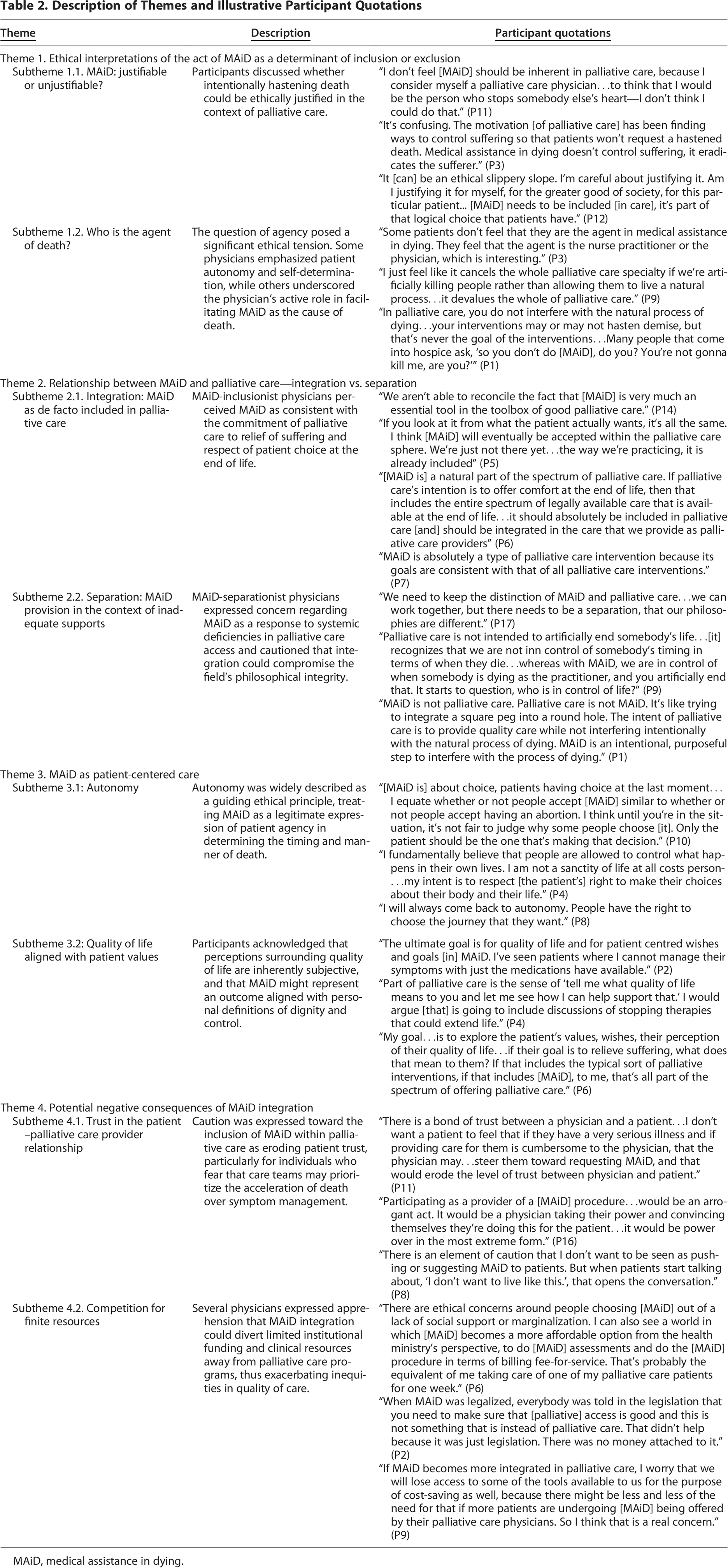
MAiD, medical assistance in dying.
Theme 1: Ethical interpretations of the act of MAiD as a determinant of inclusion or exclusion
Physicians discussed the ethical distinction between performing procedures with the sole intention to relieve suffering and procedures intending to hasten death. MAiD-involved participants perceived the procedure as an expansion of compassionate patient-centered care after all other options had been explored, while MAiD-abstaining physicians viewed the deliberate hastening of death as incompatible with their clinical ethos.
Subtheme 1.1. MAiD: justifiable or unjustifiable?
For MAiD-abstaining physicians, the direct physician involvement in causing death was a significant barrier to MAiD’s inclusion in palliative care, regardless of how compelling the patient’s reasoning may have been to precipitate the request. The act of being the one to “stop somebody else’s heart” (P11) was viewed as a profound transgression of the medical role and an unacceptable method to achieve relief of suffering. As one participant stated, “medical assistance [in] dying doesn’t control suffering…it eradicates the sufferer” (P3). Comparatively, for MAiD-involved physicians, if the patient’s medical condition was deemed irremediable, the physician’s role in facilitating MAiD became an acceptable extension of compassionate care given the foreseeability of death: “it’s almost like mercy” (P7). For these participants, the ethical duty to relieve suffering justified the use of MAiD to hasten death.
Subtheme 1.2. Who is the agent of death?
The locus of agency was a key subtheme. In MAiD, the physician becomes a direct agent of an act that causes death. This act was a crucial point of ethical consideration, with five participants noting that physicians should not be in control of the timing of patients’ deaths. One participant explained that in “palliative care, you do not interfere with the natural process of dying…your interventions may or may not hasten demise, but that’s never the goal of the interventions” (P1). For these participants, supporting a natural death allowed them to clearly affirm to themselves and others that their intentions did not involve causing death. Interestingly, patients who choose MAiD may prefer to attribute agency to the provider, paradoxically making MAiD more acceptable from their vantage point by alleviating their own sense of responsibility: “agency has come up in conversations that I’ve had with patients…they don’t feel that they are the agent, in MAiD. They feel the agent is the [clinician]” (P3). One physician who acts as a MAiD assessor only described discomfort with provision in the following manner: “that’s where palliative care providers’ concern about [MAiD] comes in, in the intention for the life to end. Maybe that’s why I haven’t been able to give an injection yet. I don’t know how I would cope with that…actively doing something that ends someone’s life is a hard thing to come around to” (P17).
Theme 2: Relationship between MAiD and palliative care—integration versus separation
MAiD-inclusionist participants argued that integration of MAiD within palliative care enables continuity of care and coordination of services involved in providing end-of-life care. Contrarily, MAiD-exclusionists argued for a division between MAiD and practices like WLT and palliative sedation.
Subtheme 2.1. Integration: MAiD as de facto included in palliative care
Eight MAiD-involved physicians felt that MAiD is already part of the palliative care provisional scope regardless of any efforts to maintain separation. As depicted by one participant, “MAiD is…basically already included [in palliative care], it’s just society that says it’s separate…it’s a giant elephant in the room” (P5). Another participant described the integration of MAiD and palliative care as follows: “We aren’t able to reconcile the fact that [MAiD] is very much an essential tool in the toolbox of good palliative care” (P14). These accounts suggest that, from the perspective of clinicians who actively provide MAiD, it is not simply an adjacent service but a central component of comprehensive end-of-life care. Though this perspective is not universal, it was echoed by several participants who emphasized that integrating MAiD within palliative practice was important for ensuring a holistic approach to patient needs.
Subtheme 2.2. Separation: MAiD provision in the context of inadequate supports
Two MAiD-abstaining participants rejected the alignment of MAiD with palliative care due to the belief that requests for the former are a result of unmet palliative needs. Concerns were raised that MAiD has been offered in cases where a specific palliative care service was suited to meet the need: “we have people banging at the door…’I’m at home suffering, what can I get?’, ‘well, the MAiD team is willing to come to my house, guess that’s what I’ll do.’ It’s very sad” (P1). The adequacy of current services was also called into question: “…you need to make sure everybody has good access to [palliative] care, but we still hear stories about that not happening. Community care, home care, and good living options…continue to be underfunded” (P2).
Furthermore, 10 participants comprising both MAiD inclusionists and exclusionists shared a deep concern about the impact of MAiD’s expansion on the sole basis of mental health, fearing that the readily available nature of the procedure may preclude governmental systems from doing more to support them. The majority of participants emphasized the importance of access to comprehensive psychosocial care prior to initiating MAiD conversations: “[a patient] was basically asking to die because the social system was not giving them a quality of life…I can’t actually address that with [my] practice…the fact the patient wants to die because society doesn’t help them” (P5). Referring specifically to the proposed MAID expansion with mental illness as the sole underlying medical condition, one physician contended “if we’re talking about [MAiD] for mental health, what is the alternative? That’s good mental health care, [which] is not accessible. Not OHIP covered. People can’t afford to see a therapist every week, and you can see a psychiatrist after a two year wait list…there’s so much inequity around mental health care” (P6).
Theme 3: MAiD as patient-centered care
Six participants described how witnessing firsthand the unrelieved suffering of patients bolstered their support for MAiD, particularly when patients articulated an autonomous, clear, cogent wish to die.
Subtheme 3.1. Autonomy
Autonomy was a key bioethical consideration that underpinned several participants’ considerations of the merits of integrating practices: “it’s always really about patient autonomy” (P8), “it’s all about what the patient wants…that guides my practice” (P5), and “it’s never [about] what I want for the patient and whether it’s [MAiD] or it’s palliative care…it’s the same, it’s the patient’s goals” (P12). These participants suggested that maximizing the range of options given to patients serves to uphold autonomy to the greatest extent.
Subtheme 3.2. Quality of life aligned with patient values
Four participants reflected that MAiD aligns with the tenets of palliative care due to the intent of upholding a quality of life viewed as acceptable according to a patient’s values. One participant said that both practices “are similar in terms of the ultimate goal for quality of life, for patient centred wishes” (P2). Similarly, a second participant found that the goals are the same across MAiD and palliative care provisions, which is “to explore the person’s…perception of their quality of life, what they wish could be better, what’s too difficult…offering them the options that exist based on those conversations” (P6). MAiD-inclusionist participants emphasized that when patients expressed sentiments such as “I can’t do what I want to do, I can’t do the things that bring me value…this is not acceptable to me” (P4), MAiD served as a means to honor the patient’s values.
Theme 4: Potential negative consequences of MAiD integration
Physicians experienced a range of emotional and professional challenges when considering the implications of integrating MAiD with palliative care.
Subtheme 4.1. Trust in the patient–palliative care provider relationship
Four MAiD-exclusionist participants were fearful that incorporating MAiD into palliative care would erode patient trust in the physician’s ability and desire to provide high-quality care. One MAiD-abstaining physician shared that he had experienced patients in hospice asking “so you don’t do MAiD, do you? You’re not gonna kill me, are you?” (P1). Highlighting the power disjuncture implicit in the patient–provider relationship, another participant stated “there is a bond of trust between a physician and patient. As long as a patient believes that I’m going to do everything in their best interest, the patient has trust in me…[MAiD] should be done by a completely separate profession…it should not be [done by] physician[s]” (P11).
Subtheme 4.2. Competition for finite resources
Concerns were raised by six participants regarding the potential of a diversion of palliative care resources should MAiD become widely accepted as part of the provisional umbrella. One issue was the impact on home palliative care: “it’s much more difficult to get home care for a patient who is at end-of-life than it is to get MAiD” (P3). Another participant worried that it may be easier and less resource-intensive for the health system to provide MAiD than to invest in comprehensive long-term palliative care services: “to do [MAiD] assessments and the procedure in terms of fee-for-service…that’s probably the [cost] equivalent of me taking care of one of my palliative patients for one week” (P6). This participant highlighted that MAiD assessments are well-compensated for the time required, whereas ongoing palliative care that is more time-intensive is financially undervalued. One participant felt that MAiD’s inclusion would cause palliative care “to shrink…and see more patients undergoing [MAiD] than living naturally…we would lose access to some of the tools available to us” (P9). This participant showed concern that the expansion of MAiD may divert resources away from standard palliative care practices, thus limiting clinicians’ abilities to use interventions that help patients live comfortably until death.
Discussion
The findings of this study reveal both philosophical and pragmatic challenges posed by the potential integrated delivery of MAiD and palliative care in Ontario, expanding on a growing corpus of provider-focused research.1,21,22 Physicians were divided as to the merits of full provisional integration between the practices, with MAiD-involved physicians responding more favorably to this concept than MAiD-abstaining physicians. Participants who provide MAiD viewed full integration of the practices as a necessary step toward prioritizing patients’ wishes and improving access to a full range of health services. Most MAiD-abstaining physicians stated a preference for a model of care that delivers MAiD and palliative care as integrated yet separate services, an approach that exists in nations such as Belgium.3,23 In the Belgian model, MAiD is legalized under strict eligibility criteria and offered alongside a robust palliative care system but coordinated by distinct teams to maintain clear provisional boundaries between the practices while enabling patient access to both. There was a shared recognition that as a legal practice, MAiD will likely remain a service offered within the Canadian health care system; as such, it is necessary for the services to connect even if they do not merge. Implementing mechanisms to enable separate provision with coordination where necessary between MAiD and palliative care requires nuanced policy frameworks and supportive professional environments that accommodate diverse clinician perspectives and safeguard high-quality patient care. 24
Eight participants felt that MAiD had already become an unspoken offering under the domain of palliative care, while four MAiD-exclusionist participants worried that this inclusion would heighten inequities in palliative care access. Questions have been raised about the accessibility and quality of palliative care in Canada, in particular, how long palliative care is received and how effective it is.25–27 Furthermore, concerns were expressed that the integration of MAiD with palliative care may erode the trust within the patient–provider relationship, an ethical concern that has been documented in bioethical literature given the vulnerability of patients in this relationship.28,29 Addressing these ethical tensions requires professional supports, clear guidelines, and policies that allow clinicians to navigate moral uncertainty while maintaining patient-centered care.6,30 Arguments in favor of MAiD’s inclusion under palliative care often appeal to principles such as autonomy, quality of life, and relief of suffering, as echoed in other studies.31–33
As reflected in the palliative care literature, participants identified inadequate funding as a key barrier that limits both the availability of palliative services and the coordination of patient care.34–36 Six participants who abstain from MAiD expressed worry that MAiD may divert material resources away from palliative care. Though some MAiD-providing participants were skeptical about the legitimacy of such claims, palliative care physicians generally acknowledge that insufficient funding is an impediment to providing the highest quality of palliative care.37,38 The alarm raised by numerous participants over MAiD as a proxy for relief of unaddressed social suffering remains a central discourse as the law continues to expand; participants raised concerns about a deficient ‘architecture of choice’ in view of the limited availability of meaningful alternatives such as robust palliative and social supports in addition to the implicit ableism in health and social systems.39–41 Future research should investigate these concerns from the perspective of the impacted populations and community-based palliative care physicians.
Limitations
Participants in this study were restricted to the province of Ontario due to recruitment strategies, which may impede the transferability of these findings to other provinces or nations with different bodies of governance. As well, our study focuses on the experiences of palliative care physicians. Future studies in this area should explore the perspectives of other clinicians, such as nurse practitioners.
Conclusion
This study explored the perspectives of palliative care physicians as to whether they believe MAiD should become integrated under the provisional scope of palliative care. While participants offered varying opinions reflecting their ethical perspectives and professional readiness to engage in MAiD, they agreed that respect for patient choice and provision of an extensive range of medical treatment are important in promoting a high standard of patient care. Their insights underscore the need for nuanced policy frameworks that accommodate professional diversity while also ensuring that patients do not experience fragmented care. Continued engagement and supportive professional infrastructure are essential in navigating this ethically charged terrain.
Ethics Approval and Consent to Participate
Ethical approval for this study was obtained from the University of Waterloo Research Ethics Board (#45975). Informed consent to participate was obtained from all subjects involved in the study.
Consent for Publication
This article contains no personally identifiable information on study participants.
Patient and Public Involvement
Patients or the public were not involved in the design of this research.
Authors’ Contributions
A.S. and M.M. contributed to conception and design of the study. M.M., A.B., and E.M. completed the study analysis. All authors drafted the article. All authors read, edited, and approved the final article.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This work was supported by a Social Sciences and Humanities Research Council Insight Grant 435-2022-0530.
Availability of Data and Materials
De-identified data are available from the corresponding author upon reasonable request.
Supplemental Material
Abbreviations
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.