
Abstract
Background:
It is unclear whether loneliness among cancer patients with minor children increased during the coronavirus disease 2019 (COVID-19) pandemic.
Objectives:
This study aimed to investigate the prevalence of severe loneliness among cancer patients with minor children during the COVID-19 pandemic in comparison with the pre-pandemic sample.
Design:
An online cross-sectional survey was conducted from December 2022 to January 2023.
Setting/Subjects:
Adult cancer patients whose youngest child was under 18 years of age and who were members of an online peer-support group in Japan were eligible.
Measurements:
Loneliness was measured using the University of California, Los Angeles Loneliness Scale (UCLA-LS). Associations between variables and severe loneliness (UCLA-LS score ≥50), as well as the prevalence of severe loneliness, were compared with those in a study conducted in 2019 using multivariable logistic regression.
Results:
A total of 233 patients of all types were included (83.3% female; mean age [standard deviation], 45.4 [5.8] years). The most common primary cancer type was breast (44.6%). The prevalence of severe loneliness was 37.3%. Factors associated with severe loneliness were Lubben Social Network Scale score (adjusted odds ratio [aOR], 0.77; 95% confidence interval [CI], 0.71–0.85; p < 0.001) and Kessler Psychological Distress Scale score (aOR, 1.21; 95% CI, 1.11–1.32; p < 0.001). The prevalence of severe loneliness was not significantly different from the prevalence in the pre-pandemic sample (aOR, 1.20; 95% CI, 0.73–1.96; p = 0.474).
Conclusions:
The COVID-19 pandemic did not affect the prevalence of severe loneliness among cancer patients with minor children. Understanding their characteristics may help to identify protective factors against increased loneliness in future pandemics.
Introduction
The coronavirus disease 2019 (COVID-19) pandemic has created significant social, economic, and medical challenges for many people worldwide. As a result of the pandemic, many countries around the world have enforced physical distancing orders 1 that have resulted in fewer social contacts, which in turn might have increased the risk for loneliness, social isolation, and depression.2,3 Loneliness is defined as a distressing emotional experience that arises when an individual perceives their social relationships as insufficient in either quantity or quality to meet their social needs.4,5 Loneliness is known to be a significant public health problem. 6 Loneliness has also been shown to affect physical health, psychological distress, and quality of life among cancer patients.7,8 Palliative care is defined as an approach that improves the quality of life of patients and their families who are facing problems associated with life-threatening illness, whether physical, psychological, social, or spiritual. 9 In this context, loneliness is included in a psychosocial problem, requiring interventions. A recent systematic review reported increases in loneliness during the COVID-19 pandemic across gender and age groups. 10 However, most of the eligible studies were conducted with the general population.
Cancer patients are particularly vulnerable to Severe Acute Respiratory Syndrome Coronavirus 2 infection. They are more likely to develop severe COVID-19 symptoms due to a systemic immunosuppressive state resulting from both tumor progression and the effects of anti-cancer therapies.11,12 A recent study reported that adolescents and young adults with cancer had worsening psychological distress and anxiety during the pandemic. 13 Some previous studies have reported that cancer patients experienced loneliness during the pandemic.14–17 In these studies, however, loneliness was evaluated with a single item or a few items, with unvalidated items, or only after the pandemic. Thus, it remains unclear whether loneliness among cancer patients has increased since the pandemic.
The number of cancer patients with minor children is increasing in many countries. In Japan, it is estimated that approximately 56,000 people with children under the age of 18 years are newly diagnosed with cancer each year. 18 A cancer diagnosis and its treatment can negatively affect both patients and their families, often leading to concerns about maintaining parental roles, disruptions to daily family routines, and challenges in communicating the illness to their children. 19 Despite these difficulties, these patients have not received adequate support. Our previous study revealed that cancer patients with minor children are at heightened risk for loneliness. 20
Therefore, we hypothesized that these patients experienced increased loneliness during the pandemic. The primary objective of the current study was to examine the prevalence of severe loneliness among cancer patients with minor children during the COVID-19 pandemic. Secondary objectives were to investigate correlates of severe loneliness, including COVID-19–associated factors, and to compare the prevalence of severe loneliness determined by our study with that in a previous study that examined loneliness in the same sample during a pre‐pandemic period (previous study). 20
Methods
Study design
This was an observational and cross-sectional study.
Place of data collection with duration
The survey took place between December 3, 2022, and January 31, 2023, using a web-based platform hosted by Medilead (http://www.medi-l.com).
Patient selection
Inclusion criteria were as follows: (1) histopathological or clinical diagnosis of cancer, (2) age of 18 years or older, (3) having minor children (children aged under 18 years), and (4) membership in the Cancer Parents online peer support group (https://cancer-parents.com/). The exclusion criterion was an inability to understand the Japanese questionnaires.
Cancer Parents is one of Japan’s largest online peer support communities for adult cancer patients. Members can connect with peers, post and read diaries, and exchange messages with each other. On December 3, 2022, we sent an email invitation containing a study description and the website address for the questionnaires to all 4374 Cancer Parents members.
To investigate factors associated with severe loneliness, we planned a multivariate logistic regression. The sample size requirement for logistic regression should be at least 10 cases per predictor. 21 In order to consider 15–20 explanatory factors extracted from a review of previous studies15,17,19,20,22,23 and discussions with coauthors, the sample size required is 200.
Survey procedures
An email invitation containing a study description and the questionnaires’ website address was sent to all Cancer Parents members at once. The survey was conducted online, and participants were invited to complete it at their convenience using their own devices. A reminder email was sent one month after the request email was sent to ensure a wide range of responses. The participants anonymously accessed and answered the questionnaires. The questionnaire form was developed based on the prior literature.13,16,17,22 The participants provided informed consent online by selecting checkboxes before completing the survey questionnaire. They then completed a series of questionnaires assessing sociodemographic and clinical characteristics, loneliness, social networks, and psychological distress. As a token of appreciation, respondents received a 500-yen Amazon gift card (approximately 3.3 United States dollars).
The statement of ethical approval
This study was conducted in accordance with the Declaration of Helsinki and was approved by the institutional review board of the National Cancer Center, Japan (approval number, 2022-222).
Study participants, procedure, and measurements from our previous study
Detailed methods have been previously reported. 20 Shortly, we conducted an online cross‐sectional survey from April 27 to May 13, 2019. This study aimed to investigate the association between loneliness and the frequency of using online peer support groups among cancer patients with minor children. The inclusion criteria were as follows: (1) diagnosis of cancer, (2) age of 20 years or older, (3) having minor children (children aged under 18 years), and (4) membership in Cancer Parents. Sociodemographic and clinical characteristics, loneliness, social networks, and psychological distress were assessed using the same questionnaires as the current survey, except for questions related to COVID-19.
Measurements
Sociodemographic characteristics
The survey collected information on a variety of sociodemographic variables: age, gender, relationship status, household composition, education level, employment status, the impact of COVID‐19 on employment, feelings of financial distress, the negative impact of the pandemic on financial status, and household income in 2022.
Clinical characteristics
The survey also collected information on cancer‐ and health‐related variables: primary cancer site, cancer stage, time since cancer diagnosis, ongoing cancer treatments, and self‐reported preexisting chronic physical and mental health illness.
Frequency of using the online peer support group
Since there was no specific measurement tool available to evaluate the experiences of an online peer support group, we developed a questionnaire based on a previous study. 24 In our previous study, we revealed that the frequent use of online peer support groups was associated with less loneliness among cancer patients with minor children. 20 Therefore, we used this questionnaire again to investigate whether there was any correlation. Participants were asked the following question: “How often do you log in to the Cancer Parents online peer support group?” The response options were at least once a day, at least once a week, at least once a month, and less than once a month. Those who selected “at least once a day” or “at least once a week” were classified as “weekly active users,” based on a previous study. 20
Loneliness
Loneliness was assessed using the Japanese version of the University of California, Los Angeles Loneliness Scale version 3 (UCLA-LS), a 20-item, 4-point Likert-type scale. 23 This is designed to be self-administered and is one of the most used questionnaires to assess loneliness. 10 Total scores range from 20 to 80, with higher scores indicating greater loneliness. 25 A score of ≥50 was defined as the presence of severe loneliness in this study. 26 The Japanese version has demonstrated high reliability (Cronbach’s alpha, 0.92). 23
Social networks
Social networks were assessed using the Japanese version of the abbreviated Lubben Social Network Scale (LSNS-6), a 6-item, 6-point Likert-type scale. 27 The LSNS-6 evaluates both family and friendship ties. Total scores range from 0 to 30, with higher scores indicating a larger social network. A score of <12 delineates being at risk for social isolation. 28 The Japanese version has shown adequate reliability (Cronbach’s alpha, 0.82). 27
Psychological distress
Psychological distress was assessed using the Japanese version of the Kessler Psychological Distress scale (K6), a 6-item, 5-point Likert-type scale. 29 Participants reported how often they have experienced symptoms such as feeling hopeless or that nothing could cheer them up over the past 30 days. Total scores range from 0 to 24, with higher scores indicating greater psychological distress. A score of ≥5 indicates the presence of moderate to severe psychological distress.30,31 The original version has demonstrated strong reliability (Cronbach’s alpha is 0.89), 32 and the Japanese version has been validated. 29
Fear of COVID-19
The Fear of COVID-19 Scale (FCV-19S) was developed with the aim of evaluating fear of COVID-19. 33 The FCV-19S is a 6-item, 5-point Likert-type scale. Total score ranges from 7 to 35, with higher scores indicating greater fear of COVID-19. A total score of ≥21 indicates difficulties in daily living due to fear of COVID-19. 34 The Japanese version of FCV-19S was used to measure the participants’ fear of COVID-19. It has shown adequate reliability (Cronbach’s alpha, 0.87). 35
Statistical methods
First, we conducted descriptive analyses of the current survey (Dataset 1). Next, we conducted univariate analyses of associations between severe loneliness and categorical and continuous sociodemographic and clinical variables using the chi‐square test and simple logistic regression. Odds ratios (ORs) and associated 95% confidence intervals (CIs) were computed using unconditional maximum likelihood estimation (Wald’s method). In addition, we used multivariate logistic regression to identify factors associated with severe loneliness. The participants with missing data on the variables included in the multivariate logistic regression model were not included in the analysis. Variables with a p-value < 0.05 in the univariate analysis or identified as relevant in a literature review were evaluated in the model.15,17,19,20,22,23
Second, we merged data from the current survey and the previous study (Dataset 2). The merged dataset contained 567 participants from both studies and a time period variable (pre‐pandemic vs. pandemic). 13 Severe loneliness among current survey participants and previous study participants was compared after adjusting for variables listed in Table 3 using multiple logistic regression.
A two-sided p-value of less than 0.05 was considered statistically significant. All analyses were conducted using JMP statistical software, version 13.2 (SAS Institute, Cary, North Carolina, United States of America).
Results
Participants’ characteristics
A total of 237 participants completed the questionnaires. Of these, four were excluded because their youngest child was aged 18 years or older. Thus, data from 233 participants were analyzed (Fig. 1). Thirteen participants had missing family income in 2021.

Flow diagram of sample recruitment, data collection, and data analysis.
Table 1 presents the characteristics of study participants. The mean age was 45.4 years (standard deviation [SD], 5.8), and the median number of children was 2 (interquartile range [IQR], 1 to 2). The majority of participants were female (83.3%), married or partnered (91.4%), living with children (97.4%), and employed or self-employed (77.3%). Breast (44.6%), colorectal (11.6%), and gynecological (8.2%) cancers were the three most common. More than half of the participants (55.4%) were receiving active cancer treatment; 39.9% of the participants had metastatic or recurrent cancer.
Characteristics of the Study Participants
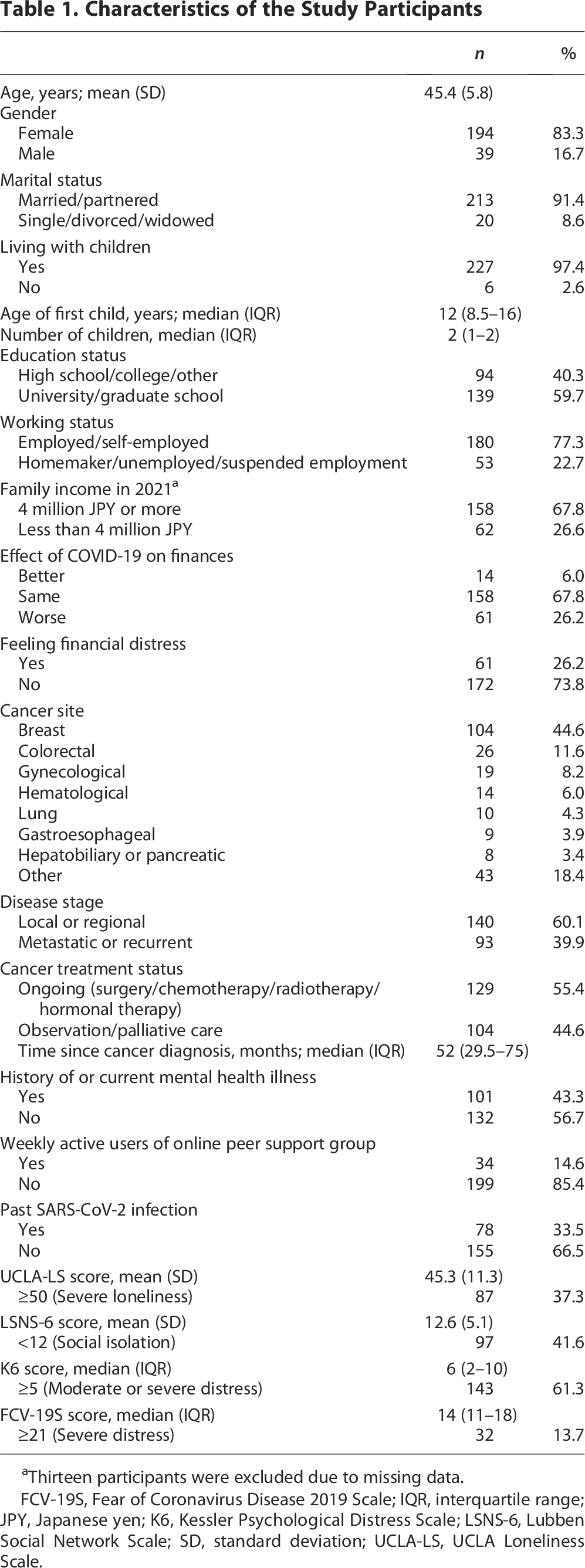
Thirteen participants were excluded due to missing data.
FCV-19S, Fear of Coronavirus Disease 2019 Scale; IQR, interquartile range; JPY, Japanese yen; K6, Kessler Psychological Distress Scale; LSNS-6, Lubben Social Network Scale; SD, standard deviation; UCLA-LS, UCLA Loneliness Scale.
Prevalence of severe loneliness and associated factors
The prevalence of severe loneliness (UCLA-LS score ≥50) was 37.3% (87/223). Table 2 shows the factors associated with severe loneliness. The univariate analysis demonstrated that lower family income in 2021, feeling financial distress, being weekly active users of the online peer support group, higher K6 and FCV-19S scores, and lower LSNS-6 scores are associated with severe loneliness (p < 0.05, respectively). The multivariable analysis included 220 participants due to variable selection; 13 participants were excluded due to missing data. The multivariate analysis demonstrated that severe loneliness is significantly associated with higher K6 score (adjusted odds ratio [aOR], 1.21, 95% CI; 1.11–1.32; p < 0.001) and lower LSNS-6 score (aOR, 0.77; 95% CI, 0.71–0.85; p < 0.001).
Factors Associated with Severe Loneliness (UCLA-LS Score ≥50)

Thirteen participants were excluded due to missing data.
CI, confidence interval; OR, odds ratio.
Comparison of severe loneliness with the previous study
In the previous study, the prevalence of severe loneliness (UCLA-LS score ≥50) was 34.1% (114/334) (Table 3). After adjusting for age, gender, marital status, living with children, financial distress, disease stage, time since diagnosis, weekly active users of the online peer support group, location, and LSNS-6 and K6 scores, time period was not significantly associated with severe loneliness (aOR, 1.20; 95% CI, 0.73–1.96; p = 0.474).
Characteristics of the Current and Previous Study Participants

Discussion
This is the first study to compare the prevalence of severe loneliness among cancer patients before and during the COVID-19 pandemic as measured using a validated scale. The important finding of the present study was that, contrary to our hypothesis, the prevalence of severe loneliness among cancer patients with minor children was not higher than during the pre-pandemic period. We have four possible explanations. First, the previous study revealed that those who lived alone or were single were particularly at risk for increased loneliness during the pandemic. 10 Most of our participants lived with their families, including their children, which might have protected them against increased loneliness. Second, the previous study reported that those who frequently used the Internet to communicate were less lonely during the pandemic. 36 Because our participants are members of an online peer support group, they might be skilled at communicating via the Internet and thus might not have experienced more loneliness. Third, the previous study reported that intolerance of uncertainty is a risk factor for severe loneliness. 37 Intolerance of uncertainty is a characteristic originally conceptualized as cognitive, emotional, and behavioral responses to uncertain situations and events. 38 Compared with the early stages of the pandemic, there might have been less uncertainty at the time of the survey, which was conducted in the late stages of the pandemic. Fourth, a recent large-scale longitudinal cohort study found that cancer survivors experienced a decrease in loneliness scores compared with noncancer patients. 39 The authors attributed the greater loneliness among cancer patients to the fear of COVID-19 infection and disrupted health care access. They noted that about half of their participants were long-term survivors not on active treatment, which may explain the findings. In our study, the median time since cancer diagnosis was 52 months, and about half were not receiving active treatment, suggesting that a similar pattern may apply.
Consistent with prior literature,8,40–42 severe loneliness was associated with higher levels of psychological distress in our study sample. Previous studies reported that severe loneliness was associated with more severe depressive symptoms in elderly patients with various cancers. The results of our study support this finding and indicate that the association also applies to younger cancer patients.
As in a previous study, 43 severe loneliness was associated with a smaller social network in our study sample. Social isolation and loneliness have been known to be positively associated with mortality and negatively associated with quality of life in elderly cancer patients. 43 Our findings suggest efforts to reduce isolation and loneliness may also be necessary for younger cancer patients.
It is necessary to identify cancer patients who having higher levels of psychological distress and/or a smaller social network. These patients should receive adequate social and psychological support, which will help alleviate their loneliness and its associated burdens. A meta‐analysis of interventions to reduce loneliness identified four primary intervention strategies: (1) improving social skills, (2) enhancing social support, (3) increasing opportunities for social contact, and (4) addressing maladaptive social cognition.44,45 Therefore, health care providers should promote measures that alleviate loneliness. For example, they can help these patients enhance their social support and connect with peer support groups and other resources.
The current study also demonstrated that severe loneliness is not significantly associated with fear of COVID-19 in cancer patients. A previous study conducted during the first wave of the pandemic and the lockdown period in European countries reported an association between fear of COVID-19 and loneliness in healthy individuals during the pandemic. 46 The results might have differed from those of our study, which was conducted in the late stages of the pandemic when there were no strict restrictions on daily life.
We found that 37% of cancer patients with minor children reported severe loneliness, which seems to be equal to or lower than the prevalence reported in previous studies of cancer patients conducted during the pandemic, ranging from 39% to 53%.15,17,47 However, in these studies, loneliness was evaluated with different scales or cutoff values. Thus, it is not possible to make direct comparisons between this study and previous studies. It would be desirable for a validated cutoff value to be determined. Palliative care seeks to improve the quality of life of patients and families facing physical, psychological, social, or spiritual challenges from life-threatening illness. 9 Given its high prevalence of loneliness, our study results support the expansion of the assessment of loneliness in palliative care practice.
Strengths and limitations
A strength of the current study is that we compared loneliness among cancer patients before and during the COVID-19 pandemic using a validated scale. Another strength is that this is the first study to investigate loneliness among cancer patients with minor children during the COVID-19 pandemic. While previous studies have mainly focused on elderly adults or the adolescent and young adult generation,14–17,47 this study targeted the generation in between.
However, the study also had limitations. First, since this study did not have a longitudinal design, differences in study participants and other unmeasured time‐related factors might have contributed to the results. Second, the participants were recruited from a single online peer support group, which might limit the generalizability. Third, since this study involved a self-administered questionnaire, there might be inaccuracies in sociodemographic and clinical information. Fourth, although it was difficult to enumerate all members who fulfilled the inclusion criteria, the response rate was low, leading to response bias. Fifth, the content validity of the items in our questionnaire regarding the frequency of using the online peer support group was not confirmed.
Conclusion
We found no significant differences in the prevalence of severe loneliness among cancer patients with minor children before and during the pandemic. However, our findings suggest that living with their family and having adequate Internet communication skills may help mitigate loneliness during this period. Cancer patients who have higher levels of psychological distress and/or a smaller social network appear to be at high risk for loneliness. This indicates a need for health care providers to proactively connect these patients to peer support and other resources to alleviate loneliness.
Authors’ Contributions
All authors contributed to the study conception and design. Material preparation and data collection were performed by T.T., S.Y., and J.T. Analyses were performed by K.K., T.K., and T.M. The first draft of the article was written by K.K., and all authors commented on previous versions of the article. All authors read and approved the final article.
Footnotes
Acknowledgments
The authors thank all the participants of our survey. The authors also thank Masako Ikeda, Rumiko Osawa, and Sachiko Nagatsuma of the National Cancer Center Hospital East for their secretarial support.
Author Disclosure Statement
Dr. K.K. received grants from Grant-in-Aid for Rare Cancer Research and payment for lecture from Daiichi Sankyo Co., Ltd. and EA Pharma CO., Ltd. Dr. T.Y. received grants or contracts from AC MEDICAL INC., A2 Healthcare Corporation, ClinChoice, Japan Tobacco Inc., Japan Media Corporation, Medidata Solutions, Inc., ONO PHARMACEUTICAL CO., LTD., Medrio, Inc., NIPRO CORPORATION, Intellim Corporation, Welby Inc., 3H Medi Solution Inc., Baseconnect Inc., Nobori Ltd., Puravida Technologies LLC., Hemp Kitchen Inc., Kyowa Kirin Co., Ltd., TSUMURA & CO., DAIICHI SANKYO COMPANY, LIMITED., Otsuka Pharmaceutical Co., Ltd., Solasia Pharma K.K., Cordis and NTT DOCOMO, INC. Dr. T.Y. also received consulting fees from Public Health Research Foundation, EPS Corporation, Japan Tobacco Inc., Medidata Solutions, Inc., ONO PHARMACEUTICAL CO., LTD., Kowa Company, Ltd., CHUGAI PHARMACEUTICAL CO., LTD., DAIICHI SANKYO COMPANY, LIMITED., Eisai Co., Ltd., 3H Clinical Trial Inc., Intellim Corporation, AstraZeneca, SONIRE Therapeutics Inc., SEIKAGAKU CORPORATION, Merck & Co., Inc., Mebix, Inc. and Nippon Boehringer Ingelheim Co., Ltd. Dr. T.Y. participated on a data safety monitoring board or advisory board of Incyte Biosciences Japan. The other authors have no conflicts of interest to disclose.
Funding Information
This study was supported by the Sasakawa Health Foundation (grant number 2022 A-102) and Takeda Science Foundation.
Data Availability
Due to the sensitive nature of the questions asked in this study, survey respondents were assured that raw data would not be shared.